
Excellent Functional Outcome and Quality of Life after Primary Cementless Total Hip Arthroplasty (THA) Using an Enhanced Recovery Setup


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
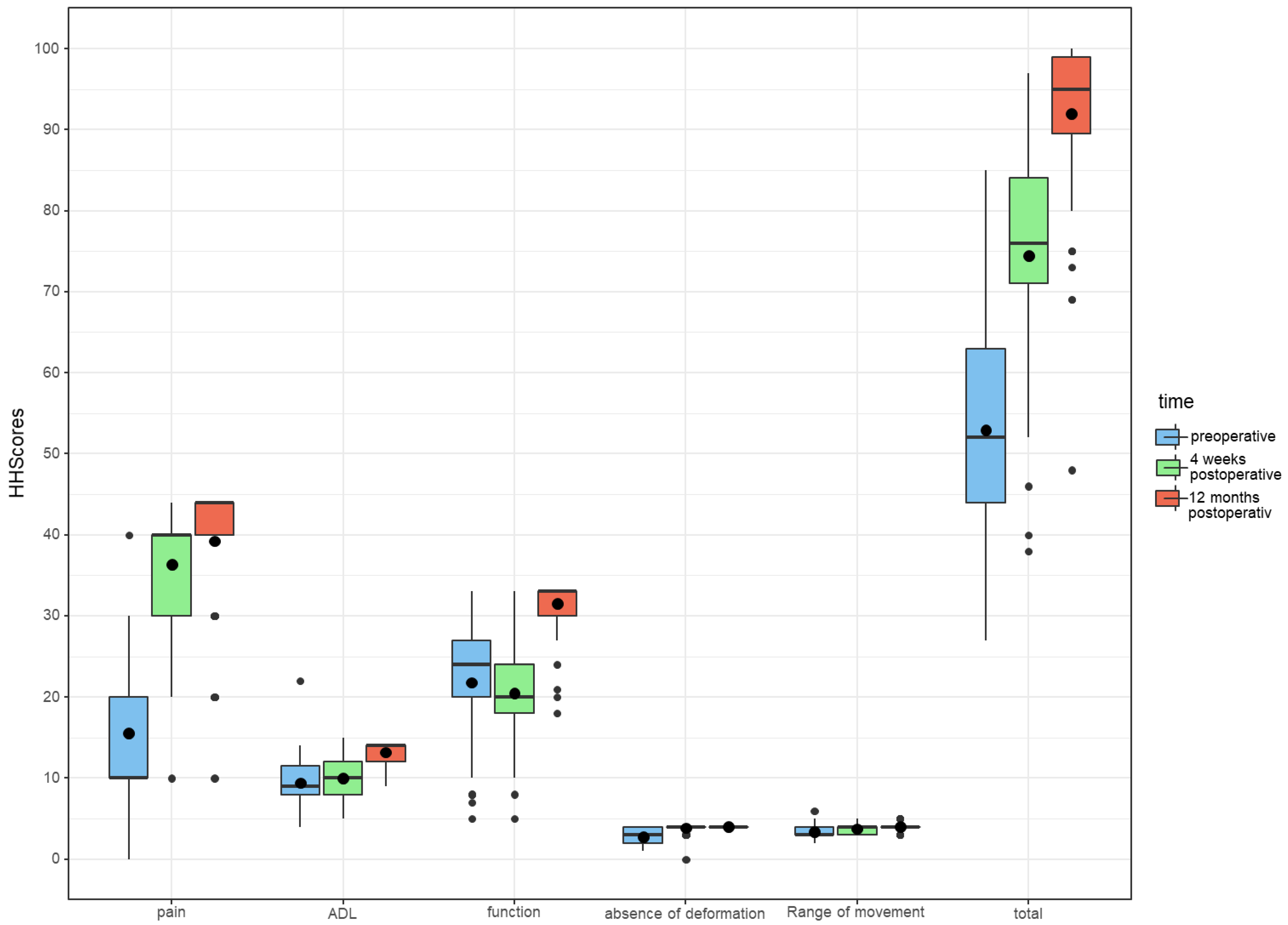
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barbieri, A.; Vanhaecht, K.; van Herck, P.; Sermeus, W.; Faggiano, F.; Marchisio, S.; Panella, M. Effects of clinical pathways in the joint replacement: A meta-analysis. BMC Med. 2009, 7, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, R.A.; Sanders, S.A.; Thill, E.S.; Sporer, S.M.; Della Valle, C. Newer anesthesia and rehabilitation protocols enable outpatient hip replacement in selected patients. Clin. Orthop. Relat. Res. 2009, 467, 1424–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowsey, M.M.; Kilgour, M.L.; Santamaria, N.M.; Choong, P.F. Clinical pathways in hip and knee arthroplasty: A prospective randomised controlled study. Med. J. Aust. 1999, 170, 59–62. [Google Scholar] [CrossRef]
- Husted, H.; Holm, G.; Jacobsen, S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: Fast-track experience in 712 patients. Acta Orthop. 2008, 79, 168–173. [Google Scholar] [CrossRef]
- Husted, H.; Jensen, C.M.; Solgaard, S.; Kehlet, H. Reduced length of stay following hip and knee arthroplasty in Denmark 2000–2009: From research to implementation. Arch. Orthop. Trauma Surg. 2012, 132, 101–104. [Google Scholar] [CrossRef]
- Husted, H.; Lunn, T.H.; Troelsen, A.; Gaarn-Larsen, L.; Kristensen, B.B.; Kehlet, H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011, 82, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Wilmore, D.W.; Kehlet, H. Management of patients in fast track surgery. BMJ 2001, 322, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Den Hartog, Y.M.; Mathijssen, N.M.C.; Vehmeijer, S.B.W. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop. 2013, 84, 444–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehlet, H. Fast-track hip and knee arthroplasty. Lancet 2013, 381, 1600–1602. [Google Scholar] [CrossRef]
- Khan, S.K.; Malviya, A.; Muller, S.D.; Carluke, I.; Partington, P.F.; Emmerson, K.P.; Mike, R.R. CrossMark LogoCrossMark Reduced short-term complications and mortality following Enhanced Recovery primary hip and knee arthroplasty: Results from 6,000 consecutive procedures. Acta Orthop. 2014, 85, 26–31. [Google Scholar] [CrossRef]
- Stambough, J.B.; Nunley, R.M.; Curry, M.C.; Steger-May, K.; Clohisy, J.C. Rapid recovery protocols for primary total hip arthroplasty can safely reduce length of stay without increasing readmissions. J. Arthroplasty 2015, 30, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, C.C.; Kehlet, H. Role of patient characteristics for fast-track hip and knee arthroplasty. Br. J. Anaesth. 2013, 110, 972–980. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, C.C.; Madsbad, S.; Kehlet, H. Postoperative morbidity and mortality in type-2 diabetics after fast-track primary total hip and knee arthroplasty. Anesth. Analg. 2015, 120, 230–238. [Google Scholar] [CrossRef]
- Larsen, K.; Hansen, T.B.; Thomsen, P.B.; Christiansen, T.; Søballe, K. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J. Bone Joint Surg. Am. 2009, 91, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Dahl, J.B. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet 2003, 362, 1921–1928. [Google Scholar] [CrossRef]
- Kehlet, H.; Wilmore, D.W. Evidence-based surgical care and the evolution of fast-track surgery. Ann. Surg. 2008, 248, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Husted, H.; Otte, K.S.; Kristensen, B.B.; Orsnes, T.; Kehlet, H. Readmissions after fast-track hip and knee arthroplasty. Arch. Orthop. Trauma Surg. 2010, 130, 1185–1191. [Google Scholar] [CrossRef]
- Husted, H.; Otte, K.S.; Kristensen, B.B.; Ørsnes, T.; Wong, C.; Kehlet, H. Low risk of thromboembolic complications after fast-track hip and knee arthroplasty. Acta Orthop. 2010, 81, 599–605. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Traitement de la Douleur Cancéreuse; Organisation mondiale de la Santé: Genève, Switzerland, 1987; Available online: https://apps.who.int/iris/handle/10665/41712 (accessed on 3 November 2020).
- Menendez, M.E.; Neuhaus, V.; van Dijk, C.N.; Ring, D. The Elixhauser comorbidity method outperforms the Charlson index in predicting inpatient death after orthopaedic surgery. Clin. Orthop. Relat. Res. 2014, 472, 2878–2886. [Google Scholar] [CrossRef] [Green Version]
- Söderman, P.; Malchau, H. Is the Harris hip score system useful to study the outcome of total hip replacement? Clin. Orthop. Relat. Res. 2001, 384, 189–197. [Google Scholar] [CrossRef]
- Smith, M.V.; Klein, S.E.; Clohisy, J.C.; Baca, G.R.; Brophy, R.H.; Wright, R.W. Lower extremity-specific measures of disability and outcomes in orthopaedic surgery. J. Bone Joint. Surg. Am. 2012, 94, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Hoeksma, H.L.; van den Ende, C.H.M.; Ronday, H.K.; Heering, A.; Breedveld, F.C. Comparison of the responsiveness of the Harris Hip Score with generic measures for hip function in osteoarthritis of the hip. Ann. Rheum. Dis. 2003, 62, 935–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, K.; Hansen, T.B.; Søballe, K.; Kehlet, H. Patient-reported outcome after fast-track hip arthroplasty: A prospective cohort study. Health Qual. Life Outcomes 2010, 8, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutzner, K.P.; Meyer, A.; Bausch, M.; Schneider, M.; Rehbein, P.; Drees, P.; Pfeil, J. Outcome of an “Enhanced Recovery” Program in Contemporary Total Hip Arthroplasty in Germany. Z. Orthop. Unfall. 2020, 158, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Maempel, J.F.; Clement, N.D.; Ballantyne, J.A.; Dunstan, E. Enhanced recovery programmes after total hip arthroplasty can result in reduced length of hospital stay without compromising functional outcome. Bone Joint J. 2016, 98, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Loth, F.L.; Giesinger, J.M.; Giesinger, K.; MacDonald, D.J.; Simpson, A.H.R.W.; Howie, C.R.; Hamilton, D.F. Impact of Comorbidities on Outcome After Total Hip Arthroplasty. J. Arthroplasty 2017, 32, 2755–2761. [Google Scholar] [CrossRef] [PubMed]
- Mariconda, M.; Galasso, O.; Costa, G.G.; Recano, P.; Cerbasi, S. Quality of life and functionality after total hip arthroplasty: A long-term follow-up study. BMC Musculoskelet. Disord. 2011, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Szende, A.; Janssen, B.; Cabases, J. (Eds.) Self-Reported Population Health: An International Perspective Based on EQ-5D; Springer Nature: London, UK, 2014. [Google Scholar]
- Mercurio, M.; Gasparini, G.; Carbone, E.A.; Galasso, O.; Segura-Garcia, C. Personality traits predict residual pain after total hip and knee arthroplasty. Int. Orthop. 2020, 44, 1263–1270. [Google Scholar] [CrossRef]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.; Dieppe, P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012, 2, e000435. [Google Scholar] [CrossRef]
- Hassett, A.L.; Marshall, E.; Bailey, A.M.; Moser, S.; Clauw, D.J.; Hooten, W.M.; Urquhart, A.; Brummett, C.M. Changes in Anxiety and Depression Are Mediated by Changes in Pain Severity in Patients Undergoing Lower-Extremity Total Joint Arthroplasty. Reg. Anesth. Pain. Med. 2018, 43, 14–18. [Google Scholar] [CrossRef]
- Burns, L.C.; Ritvo, S.E.; Ferguson, M.K.; Clarke, H.; Seltzer, Z.; Katz, J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: A systematic review. J. Pain. Res. 2015, 8, 21–32. [Google Scholar] [PubMed] [Green Version]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization; Organisation for Economic Co-operation and Development; The World Bank. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Bansback, N.; Trenaman, L.; MacDonald, K.V.; Hawker, G.; Johnson, J.A.; Stacey, D.; Marshall, D.A. An individualized patient-reported outcome measure (PROM) based patient decision aid and surgeon report for patients considering total knee arthroplasty: Protocol for a pragmatic randomized controlled trial. BMC. Musculoskelet. Disord. 2019, 20, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Preoperative checklist | Important information is already requested and documented during consultation:
|
| Preoperative preparations | Information and preparation day approx. one week before surgery, detailed multidisciplinary lecture (anesthesia, surgery, physiotherapy) gait training with crutches |
| Surgery | Application of NSAID before surgerySpinal anesthesia Pre- and intraoperativelocal infiltration analgesia (LIA) and tranexamic acid (TXA)Anterolateral approach (Microhip)No wound drains |
| Intensive physiotherapeutic care | First mobilization 2–3h after surgery with full weight bearingPhysiotherapeutic treatment 2×/day with gait training and exercises Instruction to exercise circuit |
| Pain management | Recommendations within the WHO analgesic ladder |
| Discharge criteria | Absence of wound problemsSatisfactory pain control Knowledge of restrictions and being able to walk safely at ground level and stairs |
| n (total) | 109 | |
| Gender | Male | 70 (64.2%) |
| Female | 39 (35.8%) | |
| Age (in years) | 62.1 (±10.5) | |
| Side of operation | Right | n = 57 (52.3%) |
| Left | n = 52 (47.7%) | |
| Body Mass index (kg/m2) | 28.1 (±4.45) | |
| ASA | 1 | n = 30 (27.5%) |
| 2 | n = 72 (66.1%) | |
| 3 | n = 7 (6.4%) | |
| 4 | n = 0 (0%) | |
| ECM | 0 | n = 41 (37.6%) |
| 1 | n = 40 (36.7%) | |
| 2 | n = 20 (18.3%) | |
| >3 | n = 8 (7.3%) | |
| Coronary heart disease | n = 14 (12.8%) | |
| Arterial hypertension | n = 40 (36.7%) | |
| Diabetes mellitus type II | n = 9 (8.3%) |
| Preoperative | Follow Up: 4 Weeks | Follow Up 12 Months | |
|---|---|---|---|
| Harris Hip score | 52.95 ± 12.98 | 74.47 ± 12.92 | 91.99 ± 9.40 |
| WOMAC total score | 53.07 ± 15.73 | 8.52 ± 11.81 | |
| WOMAC subscale pain | 11.36 ± 3.60 | 1.51 ± 2.52 | |
| WOMAC subscale function | 35.79 ± 12.28 | 5.72 ± 8.19 | |
| WOMAC subscale stiffness | 4.69 ± 1.74 | 1.08 ± 1.34 | |
| EQ-5D | 0.61 ± 0.19 | 0.94 ± 0.10 | |
| EQ-VAS | 53.25 ± 19.97 | 76.36 ± 24.03 |
| HADS Score | ≤7 Points | 8–10 Points | ≥11 Points |
|---|---|---|---|
| HADS-A | 79.3% | 11.5% | 9.2% |
| HADS-D | 87.4% | 11.5% | 1.1% |
| PROM | Follow Up 4 Weeks | Follow Up 12 Months |
|---|---|---|
| Was the operation successful in your eyes? | Yes = 100% | Yes = 96.9% |
| No = 0% | No = 3.1% | |
| Would you perform the surgery (THA) again? | Yes = 98.9% | Yes = 97.9% |
| No = 1.1% | No = 2.1% | |
| How do you feel compared to before surgery? | Much better = 69.4% | Much better = 84.4% |
| Better = 27.6% | Better = 12.5% | |
| Equal = 3.0% | Equal = 2.1% | |
| Bad = 0% | Bad = 1.0% | |
| Evaluate your sleep in the last 3 nights? | Very good = 14.4% | Very good = 43.3% |
| Good = 49.5% | Good = 45.4% | |
| Moderate = 24.7% | Moderate = 7.2% | |
| Bad = 9.3% | Bad = 3.1% | |
| Very bad = 2.1% | Very bad = 1.0% | |
| Judge your current appetite? | Very good = 45.4% | Very good = 68.0% |
| Good = 50.5% | Good = 30.9% | |
| Moderate = 4.1% | Moderate = 1.0% | |
| How do you currently manage your personal hygiene? | Very good = 44.8% | Very good = 75.5% |
| Good = 47.9% | Good = 24.5% | |
| Moderate = 7.3% | Moderate = 0% | |
| How do you manage going to toilet? | Very good = 59.8% | Very good = 85.7% |
| Good = 37.1% | Good = 14.3% | |
| Moderate = 3.1% | Moderate = 0% | |
| How do you rate yourself when walking in the plane? | Very good = 27.8% | Very good = 61.2% |
| Good = 58.8% | Good = 33.7% | |
| Moderate = 13.4% | Moderate = 3.1% | |
| Bad = 0% | Bad =2.0% | |
| How do you rate yourself when climbing stairs? | Very good = 25.8% | Very good = 58.2% |
| Good = 55.7% | Good = 34.7% | |
| Moderate = 16.5% | Moderate = 4.1% | |
| Bad = 2.1% | Bad = 3.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leiss, F.; Götz, J.S.; Maderbacher, G.; Meyer, M.; Reinhard, J.; Zeman, F.; Grifka, J.; Greimel, F. Excellent Functional Outcome and Quality of Life after Primary Cementless Total Hip Arthroplasty (THA) Using an Enhanced Recovery Setup. J. Clin. Med. 2021, 10, 621. https://doi.org/10.3390/jcm10040621
Leiss F, Götz JS, Maderbacher G, Meyer M, Reinhard J, Zeman F, Grifka J, Greimel F. Excellent Functional Outcome and Quality of Life after Primary Cementless Total Hip Arthroplasty (THA) Using an Enhanced Recovery Setup. Journal of Clinical Medicine. 2021; 10(4):621. https://doi.org/10.3390/jcm10040621
Chicago/Turabian StyleLeiss, Franziska, Julia Sabrina Götz, Günther Maderbacher, Matthias Meyer, Jan Reinhard, Florian Zeman, Joachim Grifka, and Felix Greimel. 2021. "Excellent Functional Outcome and Quality of Life after Primary Cementless Total Hip Arthroplasty (THA) Using an Enhanced Recovery Setup" Journal of Clinical Medicine 10, no. 4: 621. https://doi.org/10.3390/jcm10040621
APA StyleLeiss, F., Götz, J. S., Maderbacher, G., Meyer, M., Reinhard, J., Zeman, F., Grifka, J., & Greimel, F. (2021). Excellent Functional Outcome and Quality of Life after Primary Cementless Total Hip Arthroplasty (THA) Using an Enhanced Recovery Setup. Journal of Clinical Medicine, 10(4), 621. https://doi.org/10.3390/jcm10040621