
Left Atrial Ejection Fraction Assessed by Prior Cardiac CT Predicts Recurrence of Atrial Fibrillation after Pulmonary Vein Isolation

 , , ,
, , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Demographic and Clinical Data
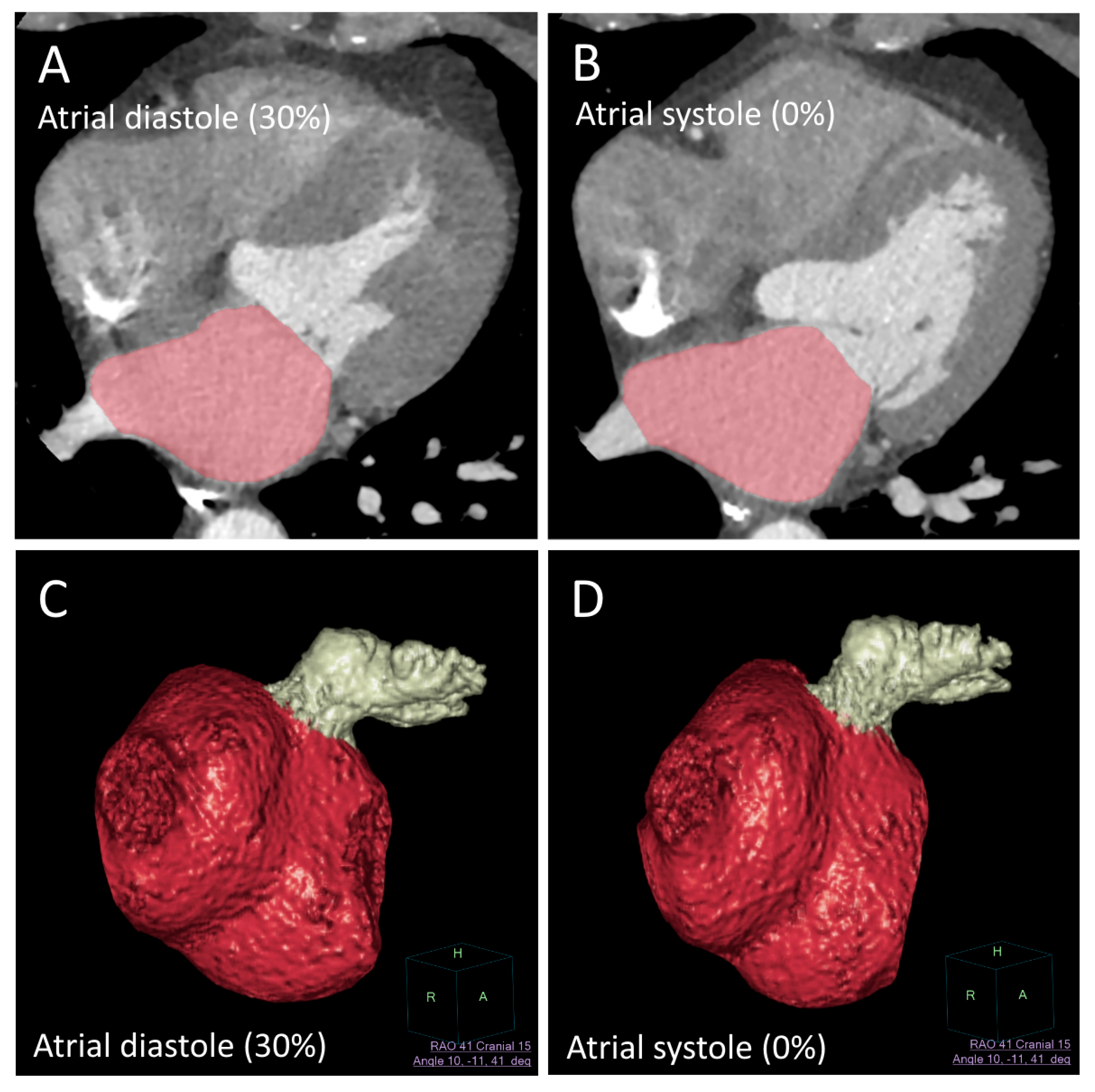
2.2. Imaging Data
2.3. Statistical Analysis
3. Results
3.1. Demographics and Clinical Data
3.2. Cardiac CT Parameters
3.3. Paroxysmal vs. Persistent
3.4. Ablation Technique
3.5. Interobserver Reliability
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mujović, N.; Marinković, M.; Lenarczyk, R.; Tilz, R.; Potpara, T.S. Catheter Ablation of Atrial Fibrillation: An Overview for Clinicians. Adv. Ther. 2017, 34, 1897–1917. [Google Scholar] [CrossRef] [Green Version]
- De Greef, Y.; Ströker, E.; Schwagten, B.; Kupics, K.; De Cocker, J.; Chierchia, G.-B.; De Asmundis, C.; Stockman, D.; Buysschaert, I. Complications of pulmonary vein isolation in atrial fibrillation: Predictors and comparison between four different ablation techniques: Results from the MIddelheim PVI-registry. Europace 2017, 20, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Prioli, A.; Marino, P.; Lanzoni, L.; Zardini, P. Increasing degrees of left ventricular filling impairment modulate left atrial function in humans. Am. J. Cardiol. 1998, 82, 756–761. [Google Scholar] [CrossRef]
- Pagel, P.S.; Kehl, F.; Gare, M.; Hettrick, D.A.; Kersten, J.R.; Warltier, D.C. Mechanical function of the left atrium: New insights based on analysis of pressure-volume relations and doppler echocardiography. Anesthesiology 2003, 98, 975–994. [Google Scholar] [CrossRef]
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Caputo, M.; Mondillo, S.; Ballo, P.; Palmerini, E.; Lisi, M.; Marino, E.; Galderisi, M. Feasibility and reference values of left atrial longitudinal strain imaging by two-dimensional speckle tracking. Cardiovasc. Ultrasound 2009, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Salvo, G.; Caso, P.; Piccolo, R.L.; Fusco, A.; Martiniello, A.R.; Russo, M.G.; D’Onofrio, A.; Severino, S.; Calabroó, P.; Pacileo, G.; et al. Atrial myocardial deformation properties predict maintenance of sinus rhythm after external cardioversion of re-cent-onset lone atrial fibrillation: A color Doppler myocardial imaging and transthoracic and transesophageal echocar-diographic study. Circulation 2005, 112, 387–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.; Malisius, R.; Krause, K.; Lampe, F.; Bahlmann, E.; Boczor, S.; Antz, M.; Ernst, S.; Kuck, K.-H. Strain rate imaging for functional quantification of the left atrium: Atrial deformation predicts the maintenance of sinus rhythm after catheter ablation of atrial fibrillation. Eur. Heart J. 2008, 29, 1397–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammerstingl, C.; Schwekendiek, M.; Momcilovic, D.; Schueler, R.; Sinning, J.; Schrickel, J.W.; Mittmann-Braun, E.; Nickenig, G.; Lickfett, L. Left atrial deformation imaging with ultrasound based two-dimensional speckle-tracking predicts the rate of recurrence of paroxysmal and persistent atrial fibrillation after successful ablation procedures. J. Cardiovasc. Electrophysiol. 2011, 23, 247–255. [Google Scholar] [CrossRef]
- Bs, R.S.O.; Badger, T.J.; Kholmovski, E.G.; Akoum, N.; Burgon, N.S.; Fish, E.N.; Bs, J.J.E.B.; Rao, S.N.; DiBella, E.V.R.; Segerson, N.M.; et al. Detection and quantification of left atrial structural remodeling with delayed-enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation 2009, 119, 1758–1767. [Google Scholar] [CrossRef] [Green Version]
- Benito, E.M.; Carlosena-Remirez, A.; Guasch, E.; Prat-González, S.; Perea, R.J.; Figueras, R.; Borràs, R.; Andreu, D.; Arbelo, E.; Tolosana, J.M.; et al. Left atrial fibrosis quantification by late gadolinium-enhanced magnetic resonance: A new method to standardize the thresholds for reproducibility. Europace 2016, 19, 1272–1279. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.H.; Oh, Y.-W.; Lee, D.I.; Shim, J.; Park, S.-W.; Kim, Y.-H. Evaluation of quantification methods for left arial late gadolinium enhancement based on different references in patients with atrial fibrillation. Int. J. Cardiovasc. Imaging 2014, 31, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Taron, J.; Foldyna, B.; Eslami, P.; Hoffmann, U.; Nikolaou, K.; Bamberg, F. Cardiac computed tomography—More than coronary arteries? A clinical update. RöFo-Fortschritte Auf Dem Geb. Der Röntgenstrahlen Und Der Bildgeb. Verfahr. 2019, 191, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, A.G. Cardiac computed tomography for atrial fibrillation ablation—One-stop-shop? Rev. Port. Cardiol. 2018, 37, 885–887. [Google Scholar] [CrossRef] [PubMed]
- Michniewicz, E.; Mlodawska, E.; Lopatowska, P.; Tomaszuk-Kazberuk, A.; Malyszko, J. Patients with atrial fibrillation and coronary artery disease—Double trouble. Adv. Med. Sci. 2018, 63, 30–35. [Google Scholar] [CrossRef]
- Hiraya, D.; Sato, A.; Hoshi, T.; Watabe, H.; Yoshida, K.; Komatsu, Y.; Sekiguchi, Y.; Nogami, A.; Ieda, M.; Aonuma, K. Impact of coronary artery disease and revascularization on recurrence of atrial fibrillation after catheter ablation: Importance of ischemia in managing atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Marques, H.; Gonçalves, P.D.A.; Ferreira, A.M.; Cruz, R.; Lopes, J.; Dos Santos, R.; Radu, L.; Costa, F.; Mesquita, J.; Carmo, P.; et al. Cardiac computed tomography previous to atrial fibrillation ablation—Effects of technological improvements and protocol optimization. Rev. Port. Cardiol. 2018, 37, 873–883. [Google Scholar] [CrossRef] [PubMed]
- Lemola, K.; Desjardins, B.; Sneider, M.; Case, I.; Chugh, A.; Good, E.; Han, J.; Tamirisa, K.; Tsemo, A.; Reich, S.; et al. Effect of left atrial circumferential ablation for atrial fibrillation on left atrial transport function. Heart Rhythm. 2005, 2, 923–928. [Google Scholar] [CrossRef]
- Stojanovska, J.; Cronin, P.; Gross, B.H.; Kazerooni, E.A.; Tsodikov, A.; Frank, L.; Oral, H. Left atrial function and maximum volume as determined by MDCT are independently associated with atrial fibrillation. Acad. Radiol. 2014, 21, 1162–1171. [Google Scholar] [CrossRef]
- Wolf, F.; Ourednicek, P.; Loewe, C.; Richter, B.; Gössinger, H.D.; Gwechenberger, M.; Plank, C.; Schernthaner, R.E.; Toepker, M.; Lammer, J.; et al. Evaluation of left atrial function by multidetector computed tomography before left atrial radiofrequency-catheter ablation: Comparison of a manual and automated 3D volume segmentation method. Eur. J. Radiol. 2010, 75, e141–e146. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Conte, E.; Perchinunno, M.; Guglielmo, M.; Volpato, V.; Annoni, A.; Baggiano, A.; Formenti, A.; et al. Atrial fibrillation: Diagnostic accuracy of coronary CT angiography performed with a whole-heart 230-µm spatial resolution CT scanner. Radiology 2017, 284, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xu, L.; Schoepf, U.J.; Wichmann, J.L.; Fox, M.A.; Yan, J.; Fan, Z.; Zhang, Z. Prospectively ECG-triggered sequential dual-source coronary CT angiography in patients with atrial fibrillation: Influence of heart rate on image quality and evaluation of diagnostic accuracy. PLoS ONE 2015, 10, e0134194. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, P.; Gragnano, F.; Cesaro, A.; Marsico, F.; Pariggiano, I.; Patti, G.; Moscarella, E.; Cavallari, I.; Sardu, C.; Parato, V.M.; et al. Non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation and atrial thrombosis: An appraisal of current evidence. Arch. Cardiovasc. Dis. 2020, 113, 642–651. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A Non-Recurrence | Group B AF Recurrence | p | |||
| Total number of patients | 41 | 9 | |||
| Sex (female) | 9 (22%) | 4 (44%) | 0.19 | ||
| Radiofrequency vs. cryoablation | 5 (12%) | 3 (33%) | 0.14 | ||
| Paroxysmal vs. persistent AF | 35 (85%) | 3 (33%) | 0.003 * | ||
| Additional ablation | 12 (29%) | 1 (11%) | 0.41 | ||
| Coronary artery disease | 26 (63%) | 6 (67%) | 0.89 | ||
| Arterial hypertension | 23 (56%) | 8 (89%) | 0.072 | ||
| Stroke in history | 4 (10%) | 1 (11%) | 0.88 | ||
| Diabetes mellitus | 37 (93%) | 8 (89%) | 0.57 | ||
| Alcohol | 10 (24%) | 2 (22%) | 0.79 | ||
| Smoking | 11 (27%) | 2 (22%) | 0.90 | ||
| Antiarrhythmic agents, class Ic | 8 (24%) | 1 (13%) | 0.66 | ||
| Antiarrhythmic agents, class II | 28 (82%) | 8 (89%) | 0.58 | ||
| Antiarrhythmic agents, class III | 5 (15%) | 1 (13%) | 1.0 | ||
| Anticoagulation with VKA | 8 (20%) | 4 (44%) | 0.19 | ||
| Anticoagulation with NOAC | 33 (80%) | 5 (56%) | 0.19 | ||
| Mean | SD | Mean | SD | p | |
| Age (years) | 57.4 | 10.84 | 60.2 | 12.7 | 0.55 |
| Agatston Score | 149.2 | 242.9 | 68.5 | 115.8 | 0.15 |
| CHA2DS2-VASc Score | 1.59 | 1.09 | 2.33 | 1.41 | 0.19 |
| HAS-BLED Score | 0.46 | 0.70 | 0.78 | 1.03 | 0.20 |
| Hemoglobin (g/dL) | 15.11 | 1.15 | 15.40 | 1.63 | 0.53 |
| Leukocytes (G/L) | 6.96 | 1.83 | 6.66 | 1.48 | 0.64 |
| Creatinine (mg/dL) | 0.97 | 0.22 | 0.96 | 0.15 | 0.89 |
| TSH (mU/L) | 2.42 | 2.07 | 1.54 | 0.82 | 0.24 |
| CK (U/L) | 137.31 | 101.86 | 149.33 | 46.98 | 0.73 |
| pBNP (pg/mL) | 393.62 | 871.06 | 744.49 | 392.79 | 0.31 |
| Hba1c (%) | 5.51 | 0.44 | 5.44 | 0.32 | 0.68 |
| LDL (mg/dL) | 113.54 | 43.92 | 99.60 | 50.77 | 0.41 |
| HR (beats/min) | 64.3 | 17.6 | 84.1 | 20.5 | 0.006 * |
| QRS (ms) | 100.3 | 14.7 | 106.5 | 27.0 | 0.93 |
| QTc (ms) | 423.4 | 30.2 | 459.8 | 30.4 | 0.003 * |
| LV ejection fraction (%) | 56.1 | 2.37 | 52.11 | 7.61 | 0.17 |
| Septal thickness (mm) | 9.05 | 1.79 | 10.1 | 1.9 | 0.12 |
| LV end-diastolic diameter (mm) | 53.39 | 5.05 | 53.44 | 6.16 | 0.98 |
| Morphological Parameters | ||||
| LAVmax (mL) | LAVImax | LAAVmax (mL) | LAAVImax | |
| Mean A | 125.8 ± 29.4 | 60.6 ± 14.0 | 10.0 ± 3.54 | 4.96 ± 1.87 |
| Mean B | 163.7 ± 49.6 | 81.4 ± 22.7 | 14.3 ± 4.4 | 7.07 ± 1.87 |
| p | 0.036 | 0.026 | 0.003 | 0.004 |
| Accuracy (%) | 86 | 88 | 82 | 84 |
| Sensitivity (%) | 33 | 44 | 22 | 33 |
| Specificity (%) | 98 | 98 | 95 | 95 |
| NPV (%) | 87 | 89 | 84 | 86 |
| PPV (%) | 75 | 80 | 50 | 60 |
| Functional Parameters | ||||
| LAEF (%) | LASV (mL) | LAAEF (%) | LAASV (mL) | |
| Mean A | 36 ± 10 | 43.4 ± 11.48 | 42 ± 14 | 4.1 ± 1.91 |
| Mean B | 16 ± 8 | 25.0 ± 11.2 | 16 ± 8 | 2.4 ± 1.39 |
| p | 0.00002 | 0.0008 | 0.000002 | 0.015 |
| Accuracy (%) | 94 | 88 | 90 | 86 |
| Sensitivity (%) | 67 | 56 | 67 | 22 |
| Specificity (%) | 100 | 95 | 95 | 100 |
| NPV (%) | 93 | 90 | 93 | 85 |
| PPV (%) | 100 | 71 | 75 | 100 |
| Paroxysmal AF | |||
| Mean Group A | Mean Group B | p | |
| LAVmax (mL) | 126.1 ± 31 | 157.5 ± 42.2 | 0.11 |
| LAVImax (mL/m²) | 61.1 ± 14.8 | 78.6 ± 26.7 | 0.07 |
| LASV (mL) | 44.2 ± 11.1 | 25.8 ± 4.7 | 0.008 * |
| LAEF (%) | 0.4 ± 0.1 | 0.2 ± 0.1 | 0.002 * |
| LAAVmax (mL) | 9.8 ± 3.5 | 13.7 ± 1.9 | 0.06 |
| LAAVImax (mL/m²) | 4.8 ± 1.8 | 6.8 ± 1.5 | 0.08 |
| LAASV (mL) | 4.2 ± 1.9 | 2.4 ± 0.9 | 0.11 |
| LAAEF (%) | 0.4 ± 0.1 | 0.2 ± 0.1 | 0.001 * |
| Persistent AF | |||
| LAVmax (mL) | 126.58 ± 17 | 166.85 ± 56.5 | 0.15 |
| LAVImax (mL/m²) | 57.93 ± 5 | 82.83 ± 23 | 0.045 * |
| LASV (mL) | 40.60 ± 14.6 | 24.65 ± 13.8 | 0.08 |
| LAEF (%) | 0.32 ± 0.11 | 0.16 ± 0.1 | 0.020 * |
| LAAVmax (mL) | 11.45 ± 3.74 | 14.53 ± 5.4 | 0.28 |
| LAAVImax (mL/m²) | 5.61 ± 2.12 | 7.20 ± 2.2 | 0.23 |
| LAASV (mL) | 3.60 ± 2.1 | 2.38 ± 1.7 | 0.29 |
| LAAEF (%) | 0.31 ± 0.1 | 0.16 ± 0.1 | 0.035 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaufmann, R.; Rezar, R.; Strohmer, B.; Wernly, B.; Lichtenauer, M.; Hitzl, W.; Meissnitzer, M.; Hergan, K.; Granitz, M. Left Atrial Ejection Fraction Assessed by Prior Cardiac CT Predicts Recurrence of Atrial Fibrillation after Pulmonary Vein Isolation. J. Clin. Med. 2021, 10, 752. https://doi.org/10.3390/jcm10040752
Kaufmann R, Rezar R, Strohmer B, Wernly B, Lichtenauer M, Hitzl W, Meissnitzer M, Hergan K, Granitz M. Left Atrial Ejection Fraction Assessed by Prior Cardiac CT Predicts Recurrence of Atrial Fibrillation after Pulmonary Vein Isolation. Journal of Clinical Medicine. 2021; 10(4):752. https://doi.org/10.3390/jcm10040752
Chicago/Turabian StyleKaufmann, Reinhard, Richard Rezar, Bernhard Strohmer, Bernhard Wernly, Michael Lichtenauer, Wolfgang Hitzl, Matthias Meissnitzer, Klaus Hergan, and Marcel Granitz. 2021. "Left Atrial Ejection Fraction Assessed by Prior Cardiac CT Predicts Recurrence of Atrial Fibrillation after Pulmonary Vein Isolation" Journal of Clinical Medicine 10, no. 4: 752. https://doi.org/10.3390/jcm10040752
APA StyleKaufmann, R., Rezar, R., Strohmer, B., Wernly, B., Lichtenauer, M., Hitzl, W., Meissnitzer, M., Hergan, K., & Granitz, M. (2021). Left Atrial Ejection Fraction Assessed by Prior Cardiac CT Predicts Recurrence of Atrial Fibrillation after Pulmonary Vein Isolation. Journal of Clinical Medicine, 10(4), 752. https://doi.org/10.3390/jcm10040752