
Combined Phacoemulsification and Ex-PRESS Implant with Everting Suture in Primary Angle-Closure Glaucoma: Survival Analysis and Predictive Factors

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
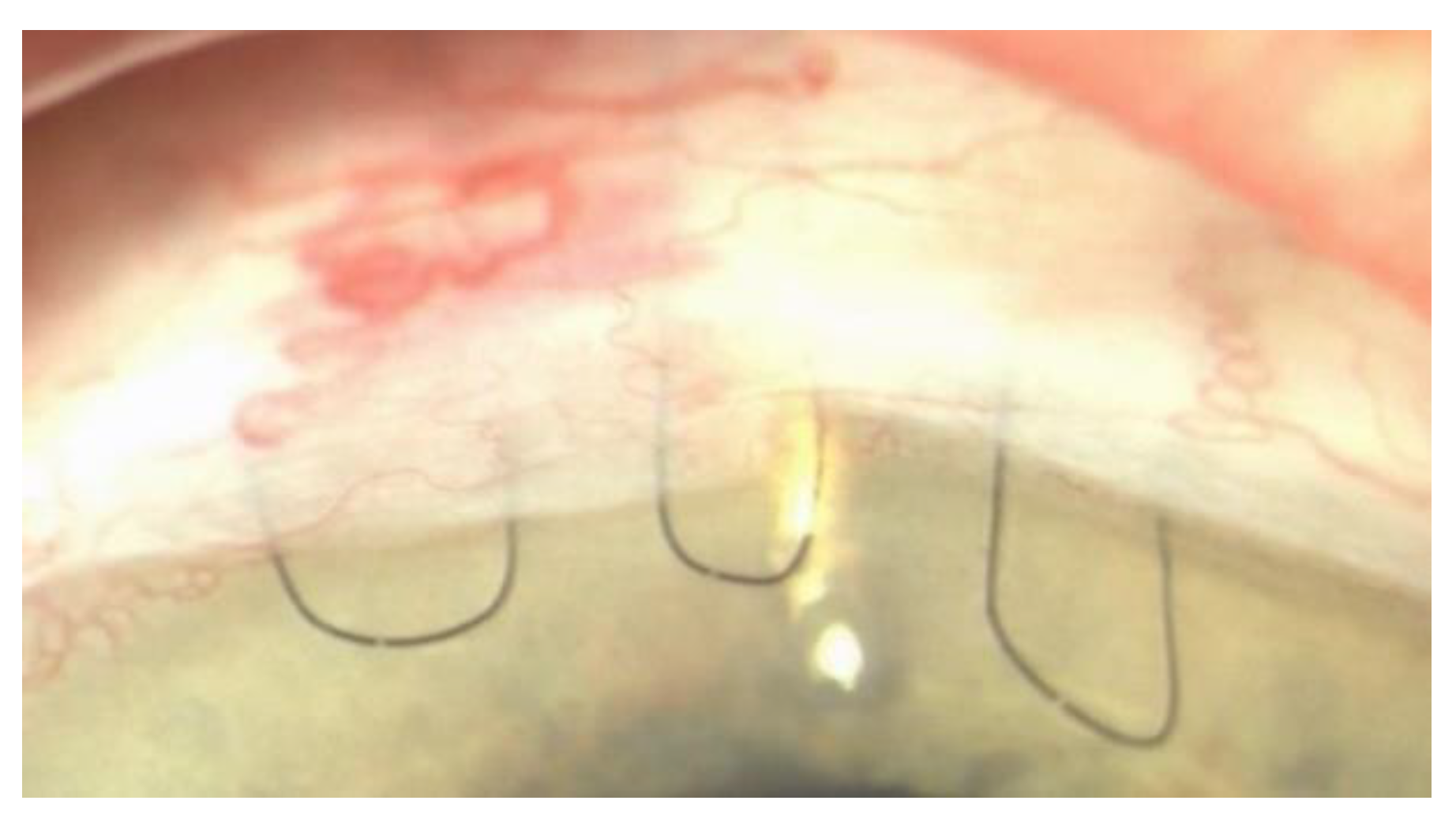
2.1. Surgical Procedure Description
2.2. Success Criteria
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition—Chapter 3: Treatment principles and options Supported by the EGS Foundation: Part 1: Foreword; Introduction; Glossary; Chapter 3 Treatment principles and options. Br. J. Ophthalmol. 2017, 101, 130–195. [CrossRef] [PubMed] [Green Version]
- Azuara-Blanco, A.; Burr, J.; Ramsay, C.; Cooper, D.; Foster, P.J.; Friedman, D.S.; Scotland, G.; Javanbakht, M.; Cochrane, C.; Norrie, J.; et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): A randomised controlled trial. Lancet 2016, 388, 1389–1397. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.S.; Tham, C.C.; Lam, D.S. Incisional surgery for angle closure glaucoma. Semin. Ophthalmol. 2002, 17, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.Y.; Liu, C.J.; Cheng, C.Y. Combined trabeculectomy and cataract extraction versus trabeculectomy alone in primary angle-closure glaucoma. Br. J. Ophthalmol. 2009, 93, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Tham, C.C.; Kwong, Y.Y.; Leung, D.Y.; Lam, S.W.; Li, F.C.; Chiu, T.Y.; Chan, J.C.; Lam, D.S.; Lai, J.S. Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts. Ophthalmology 2009, 116, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Nyska, A.; Glovinsky, Y.; Belkin, M.; Epstein, Y. Biocompatibility of the Ex-PRESS miniature glaucoma drainage implant. J. Glaucoma 2003, 12, 275–280. [Google Scholar]
- Nardi, M.; Posarelli, C.; Nasini, F.; Figus, M. Mini Drainage Devices for Anterior and Intermediate Filtration. Dev. Ophthalmol. 2017, 59, 90–99. [Google Scholar]
- Seider, M.I.; Rofagha, S.; Lin, S.C.; Stamper, R.L. Resident-performed Ex-PRESS shunt implantation versus trabeculectomy. J. Glaucoma 2012, 21, 469–474. [Google Scholar] [CrossRef]
- Dahan, E.; Carmichael, T.R. Implantation of a miniature glaucoma device under a scleral flap. J. Glaucoma 2005, 14, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhou, M.; Huang, W.; Zhang, X. Ex-PRESS implantation versus trabeculectomy in uncontrolled glaucoma: A meta-analysis. PLoS ONE 2013, 8, e63591. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Rodriguez, J.M.; Trope, G.E.; Drori-Wagschal, L.; Jinapriya, D.; Buys, Y.M. Comparison of trabeculectomy versus Ex-PRESS: 3-year follow-up. Br. J. Ophthalmol. 2016, 100, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Wagschal, L.D.; Trope, G.E.; Jinapriya, D.; Jin, Y.P.; Buys, Y.M. Prospective Randomized Study Comparing Ex-PRESS to Trabeculectomy: 1-Year Results. J. Glaucoma 2015, 24, 624–629. [Google Scholar] [CrossRef]
- Maris, P.J., Jr.; Ishida, K.; Netland, P.A. Comparison of trabeculectomy with Ex-PRESS miniature glaucoma device implanted under scleral flap. J. Glaucoma 2007, 16, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Moisseiev, E.; Zunz, E.; Tzur, R.; Kurtz, S.; Shemesh, G. Standard Trabeculectomy and Ex-PRESS Miniature Glaucoma Shunt: A Comparative Study and Literature Review. J. Glaucoma 2015, 24, 410–416. [Google Scholar]
- Dahan, E.; Ben Simon, G.J.; Lafuma, A. Comparison of trabeculectomy and Ex-PRESS implantation in fellow eyes of the same patient: A prospective, randomised study. Eye 2012, 26, 703–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traverso, C.E.; de Feo, F.; Messas-Kaplan, A.; Denis, P.; Levartovsky, S.; Sellem, E.; Badalà, F.; Zagorski, Z.; Bron, A.; Belkin, M. Long term effect on IOP of a stainless steel glaucoma drainage implant (Ex-PRESS) in combined surgery with phacoemulsification. Br. J. Ophthalmol. 2005, 89, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Li, W.; Jiang, F.; Mao, S.; Tong, Y. Ex-PRESS implantation versus trabeculectomy in open-angle glaucoma: A meta-analysis of randomized controlled clinical trials. PLoS ONE 2014, 9, e86045. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, M.A.; Wellington, D.P.; Ziel, C.J. A releasable scleral-flap tamponade suture for guarded filtration surgery. Arch. Ophthalmol. 1993, 111, 398–403. [Google Scholar] [CrossRef]
- Duman, F.; Faria, B.; Rutnin, N.; Guzel, H.; Ekici, F.; Waisbourd, M.; Katz, L.J.; Moster, M.R.; Spaeth, G.L. Comparison of 3 different releasable suture techniques in trabeculectomy. Eur. J. Ophthalmol. 2016, 26, 307–314. [Google Scholar]
- Figus, M.; Posarelli, C.; Nasini, F.; Casini, G.; Martinelli, P.; Nardi, M. Scleral Flap-Everting Suture for Glaucoma-filtering Surgery. J. Glaucoma 2016, 25, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Netland, P.A.; Sarkisian, S.R., Jr.; Moster, M.R.; Ahmed, I.I.; Condon, G.; Salim, S.; Sherwood, M.B.; Siegfried, C.J. Randomized, prospective, comparative trial of EX-PRESS glaucoma filtration device versus trabeculectomy (XVT study). Am. J. Ophthalmol. 2014, 157, 433–440.e3. [Google Scholar] [CrossRef]
- Lan, J.; Sun, D.P.; Wu, J.; Wang, Y.N.; Xie, L.X. Ex-PRESS implantation with phacoemulsification in POAG versus CPACG. Int. J. Ophthalmol. 2017, 10, 51–55. [Google Scholar]
- Liu, B.; Guo, D.D.; Du, X.J.; Cong, C.Y.; Ma, X.H. Evaluation of Ex-PRESS implantation combined with phacoemulsification in primary angle-closure glaucoma. Medicine 2016, 95, e4613. [Google Scholar] [CrossRef]
- Nie, L.; Fang, A.; Pan, W.; Ye, H.; Chan, Y.K.; Fu, L.; Qu, J. Prospective Study on Ex-PRESS Implantation Combined with Phacoemulsification in Primary Angle-Closure Glaucoma Coexisting Cataract: 3-Year Results. Curr. Eye Res. 2018, 43, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Kanner, E.M.; Netland, P.A.; Sarkisian, S.R., Jr.; Du, H. Ex-PRESS miniature glaucoma device implanted under a scleral flap alone or combined with phacoemulsification cataract surgery. J. Glaucoma 2009, 18, 488–491. [Google Scholar] [CrossRef] [PubMed]
- Tham, C.C.; Leung, D.Y.; Kwong, Y.Y.; Li, F.C.; Lai, J.S.; Lam, D.S. Effects of phacoemulsification versus combined phaco-trabeculectomy on drainage angle status in primary angle closure glaucoma (PACG). J. Glaucoma 2010, 19, 119–123. [Google Scholar] [CrossRef]
- Rękas, M.; Barchan-Kucia, K.; Konopińska, J.; Mariak, Z.; Żarnowski, T. Analysis and Modeling of Anatomical Changes of the Anterior Segment of the Eye After Cataract Surgery with Consideration of Different Phenotypes of Eye Structure. Curr. Eye Res. 2015, 40, 1018–1027. [Google Scholar] [CrossRef]
- Wells, A.P.; Bunce, C.; Khaw, P.T. Flap and suture manipulation after trabeculectomy with adjustable sutures: Titration of flow and intraocular pressure in guarded filtration surgery. J. Glaucoma 2004, 13, 400–406. [Google Scholar]
- Loon, S.C.; Chew, P.T. A major review of antimetabolites in glaucoma therapy. Ophthalmologica 1999, 213, 234–245. [Google Scholar] [CrossRef] [PubMed]
- Janson, B.J.; Alward, W.L.; Kwon, Y.H.; Bettis, D.I.; Fingert, J.H.; Provencher, L.M.; Goins, K.M.; Wagoner, M.D.; Greiner, M.A. Glaucoma-associated corneal endothelial cell damage: A review. Surv. Ophthalmol. 2018, 63, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Casini, G.; Loiudice, P.; Pellegrini, M.; Sframeli, A.T.; Martinelli, P.; Passani, A.; Nardi, M. Trabeculectomy Versus EX-PRESS Shunt Versus Ahmed Valve Implant: Short-term Effects on Corneal Endothelial Cells. Am. J. Ophthalmol. 2015, 160, 1185–1190.e1. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Results |
|---|---|
| Age | 68.7 ± 8.9 |
| Gender | |
| Male | 27 (39.1%) |
| Female | 42 (60.9%) |
| Laterality | |
| Right | 33 (47.8%) |
| Left | 36 (52.2%) |
| Baseline IOP (mmHg) | 18.4 ± 0.6 |
| Baseline n. of medications | 2.6 ± 0.1 |
| Baseline BCVA (logMAR) | 0.33 ± 0.01 |
| Previous iridotomy | 12 (52.2%) |
| Mean IOP in mmHg | Mean Number of Medications | Mean BCVA | |
|---|---|---|---|
| Baseline | 18.4 ± 0.6 | 2.6 ± 0.1 | 0.33 ± 0.01 |
| 1 day | 13.9 ± 4.6 * | 0.04 ± 0.2 * | 0.23 ± 0.17 |
| 1 month | 12.9 ± 1.87 * | 0.04 ± 0.2 * | 0.18 ± 0.17 * |
| 3 months | 12.86 ± 2.66 * | 0.04 ± 0.2 * | 0.20 ± 0.21 * |
| 6 months | 13.04 ± 2.33 * | 0.08 ± 0.28 * | 0.17 ± 0.19 * |
| 12 months | 13.56 ± 2.38 * | 0.13 ± 0.34 * | 0.16 ± 0.20 * |
| 24 months | 13.45 ± 1.99 * | 0.13 ± 0.34 * | 0.13 ± 0.19 * |
| Risk Factor | Criterion 1 | Criterion 2 | Criterion 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P | HR | 95% CI | P | HR | 95% CI | P | |
| Age (per decade) | 1.073 | 00926–1.243 | 0.350 | 0.971 | 0.895–1.053 | 0.471 | 0.998 | 0.948–1.051 | 0.944 |
| As continuous variable | 1.556 | 0.481–5.037 | 0.460 | 0.626 | 0.308–1.274 | 0.196 | 0.935 | 0.604–1.448 | 0.935 |
| Gender | 0.291 | 0.026–3.214 | 0.314 | 0.471 | 0.105–2.105 | 0.324 | 0.256 | 0.2237–1.467 | 0.256 |
| Baseline IOP | 1.123 | 0.938–1.347 | 0.207 | 1.001 | 1.001–0.860 | 0.990 | 0.982 | 0.899–1.073 | 0.687 |
| Baseline n. of medications | 4.233 | 0.665–26.937 | 0.126 | 1.231 | 0.494–3.064 | 0.655 | 1.116 | 0.662–1.883 | 0.680 |
| N. of medications at 1 month | 1.00 | 0.00–14926.77 | 1.00 | 4.400 | 0.514–37.661 | 0.176 | 1.571 | 0.207–11.950 | 0.662 |
| N. of medications at 3 months | 1.132 | 0.025–14638.27 | 0.986 | 3.540 | 0.567–32.621 | 0.396 | 0.682 | 0.507–1.684 | 0.253 |
| N. of medications at 6 months | 14.849 | 0.891–247.51 | 0.060 | 5.250 | 0.962–28.663 | 0.056 | 1.615 | 0.625–7.158 | 0.528 |
| N. of medications at 12 months | 22.293 | 1.922–258.62 | 0.013 | 6.779 | 1.369–33.582 | 0.019 | 1.667 | 0.470–5.906 | 0.429 |
| IOP at day 1 | 1.094 | 0.865–1.383 | 0.453 | 0.842 | 0.674–1.053 | 0.132 | 1.005 | 0.891–1.133 | 0.936 |
| IOP at month 3 | 1.330 | 0.752–2.352 | 0.327 | 1.191 | 0.859–1.652 | 0.293 | 1.357 | 1.078–1.708 | 0.009 |
| IOP at month 6 | 2.713 | 1.190–6.189 | 0.018 | 1.186 | 0.846–1.661 | 0.322 | 1.318 | 1.061–1.636 | 0.012 |
| IOP at month 12 | 1.843 | 0.949–3.576 | 0.071 | 1.396 | 0.978–1.994 | 0.066 | 1.315 | 1.058–1.636 | 0.014 |
| IOP before 1st releasable | 1.427 | 1.034–1.969 | 0.031 | 0.906 | 0.736–1.115 | 0.350 | 0.998 | 0.895–1.114 | 0.976 |
| IOP after 1st releasable | 1.283 | 0.988–1.667 | 0.061 | 0.906 | 0.735–1.117 | 0.356 | 0.939 | 0.724–1.071 | 0.348 |
| IOP change after 1st releasable | 1.181 | 0.855–1.631 | 0.312 | 1.009 | 0.802–1.270 | 0.938 | 1.081 | 0.943–1.240 | 0.263 |
| IOP before 2nd releasable | 17.876 | 0.034–9528.05 | 0.368 | 1.029 | 0.895–1.184 | 0.686 | 1.046 | 0.965–1.134 | 0.269 |
| IOP after 2nd releasable | 1.223 | 0.741–2.0149 | 0.431 | 0.951 | 0.716–1.263 | 0.730 | 1.066 | 0.900–1.264 | 0.458 |
| IOP change after 2nd releasable | 1.218 | 0.997–1.488 | 0.054 | 1.019 | 0.890–1.166 | 0.789 | 1.021 | 0.939–1.110 | 0.630 |
| IOP before everting | 2.593 | 0.929–7.239 | 0.069 | 0.781 | 0.350–1.744 | 0.546 | 1.236 | 0.793–1.928 | 0.349 |
| IOP after everting | 1.307 | 0.835–2.047 | 0.242 | 1.238 | 0.883–1.735 | 0.215 | 1.182 | 0.958–1.457 | 0.118 |
| IOP change after everting | 0.909 | 0.532–1.554 | 0.727 | 0.784 | 0.584–1.052 | 0.105 | 0.872 | 0.700–1.087 | 0.224 |
| Time of removal of 1st releasable | 1.017 | 0.850–1.218 | 0.851 | 1.013 | 0.901–1.139 | 0.827 | 0.949 | 0.787–1.026 | 0.186 |
| Time of removal of 2nd releasable | 0.991 | 0.880–1.116 | 0.880 | 1.045 | 0.995–1.098 | 0.075 | 0.991 | 0.942–1.04.3 | 0.733 |
| Time of everting suture removal | 0.983 | 0.835–1.158 | 0.840 | 1.025 | 0.907–1.159 | 0.690 | 0.958 | 0.899–1.021 | 0.188 |
| Iridotomy (yes vs. no) | 0.454 | 0.041–5.013 | 0.519 | 1.217 | 0.272–5.437 | 0.797 | 1.289 | 0.531–3.132 | 0.575 |
| Complications (yes vs. no) | 0.547 | 0.050–6.041 | 0.623 | 30.330 | 0.016–578.85 | 0.376 | 0.949 | 0.342–2.634 | 0.921 |
| Risk Factor | Criterion 1 | Criterion 2 | Criterion 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P | HR | 95% CI | P | HR | 95% CI | P | |
| Age (per decade) | 2.414 | 0.477–12.211 | 0.287 | 0.628 | 0.311–1.267 | 0.194 | 0.928 | 0.596–1.443 | 0.739 |
| As continuous variable | 1.115 | 0.907–1.39 | 0.301 | 0.971 | 0.896–1.053 | 0.475 | 0.997 | 0.954–1.051 | 0.902 |
| Gender | 0.606 | 0.038–9.702 | 0.723 | 0.470 | 0.105–2.102 | 0.323 | 0.615 | 0.251–1.509 | 0.288 |
| Baseline IOP | 1.072 | 0.842–1.366 | 0.571 | 1.00 | 0.859–1.164 | 0.999 | 0.977 | 0.894–1.067 | 0.603 |
| Baseline n. of medications | 7.261 | 0.593–88.850 | 0.121 | 1.229 | 0.485–3.114 | 0.664 | 1.111 | 0.656–1.881 | 0.695 |
| N. of medications at 1 month | 0.046 | 0.00–4.339 | 0.840 | 4.202 | 0.490–36.020 | 0.190 | 0.946 | 0.123–7.207 | 0.957 |
| N. of medications at 3 months | 0.677 | 0.03–4.352 | 0.760 | 3.219 | 0.265–5–897 | 0.154 | 0.957 | 0.003–5.297 | 0.840 |
| N. of medications at 6 months | 0.043 | 0.00–8766.60 | 0.774 | 6.656 | 1.030–31.044 | 0.046 | 1.229 | 0.282–5.352 | 0.783 |
| N. of medications at 12 months | 6.498 | 0.406–103.90 | 0.186 | 7.745 | 1.528–39.259 | 0.013 | 1.386 | 0.401–4.789 | 0.606 |
| IOP at day 1 | 1.062 | 0.782–1.443 | 0.700 | 0.832 | 0.662–1.045 | 0.114 | 1.001 | 0.886–13131 | 0.983 |
| IOP at month 3 | 7.378 | 0.399–136.51 | 0.179 | 1.214 | 0.986–1.696 | 0.256 | 1.441 | 1.125–1.845 | 0.004 |
| IOP at month 6 | 3.952 | 0.914–17.084 | 0.066 | 1.204 | 0.853–1.700 | 0.291 | 1.288 | 1.049–1.583 | 0.016 |
| IOP at month 12 | 1.983 | 0.812–4.841 | 0.133 | 1.435 | 0.993–2.073 | 0.054 | 1.292 | 1.051–1.587 | 0.015 |
| IOP before 1st releasable | 1.089 | 0.825–1.438 | 0.547 | 0.894 | 0.723–1.105 | 0.298 | 0.984 | 0.885–1.093 | 0.758 |
| IOP after 1st releasable | 1.301 | 0.922–1.837 | 0.134 | 0.901 | 0.733–1.108 | 0.324 | 0.927 | 0.810–1.059 | 0.264 |
| IOP change after 1st releasable | 0.755 | 0.396–1.441 | 0.394 | 1.005 | 0.799–1.263 | 0.969 | 1.056 | 0.930–1.200 | 0.402 |
| IOP before 2nd releasable | 1.120 | 0.946–1.325 | 0.189 | 1.027 | 0.892–1.181 | 0.715 | 1.026 | 0.951–1.106 | 0.511 |
| IOP after 2nd releasable | 1.319 | 0.666–2.610 | 0.427 | 0.949 | 0.714–1.262 | 0.720 | 1.069 | 0.901–1.269 | 0.442 |
| IOP change after 2nd releasable | 0.920 | 0.656–1.290 | 0.629 | 1.015 | 0.886–1.163 | 0.831 | 1.005 | 0.929–1.087 | 0.906 |
| IOP before everting | 3.892 | 1.086–13.946 | 0.037 | 0.757 | 0.328–1.745 | 0.513 | 1.251 | 0.800–1.956 | 0.326 |
| IOP after everting | 1.447 | 0.871–2.402 | 0.153 | 1.274 | 0.897–1.809 | 0.177 | 1.198 | 0.970–1.479 | 0.094 |
| IOP change after everting | 0.872 | 0.470–1.619 | 0.665 | 0.761 | 0.562–1.031 | 0.078 | 0.861 | 0.690–1.075 | 0.186 |
| Time of removal of 1st releasable | 1.110 | 0.930–1.326 | 0.248 | 1.014 | 0.903–1.138 | 0.819 | 0.954 | 0.884–1.029 | 0.219 |
| Time of removal of 2nd releasable | 1.020 | 0.915–1.137 | 0.719 | 1.052 | 1.00–1.106 | 0.051 | 0.993 | 0.944–1.045 | 0.788 |
| Time of everting suture traction | 0.975 | 0.799–1.190 | 0.802 | 1.025 | 0.905–1.161 | 0.698 | 0.955 | 0.895–1.019 | 0.164 |
| Iridotomy (yes vs. no) | 0.013 | 0.00–1202.91 | 0.458 | 1.194 | 0.267–5.335 | 0.817 | 1.254 | 0.518–3.035 | 0.616 |
| Complications (yes vs. no) | 4.025 | 0.251–64.627 | 0.326 | 0.032 | 0.00–55.342 | 0.366 | 1.077 | 0.388–2.988 | 0.887 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covello, G.; Loiudice, P.; Maglionico, M.N.; Nardi, M.; Figus, M.; Posarelli, C. Combined Phacoemulsification and Ex-PRESS Implant with Everting Suture in Primary Angle-Closure Glaucoma: Survival Analysis and Predictive Factors. J. Clin. Med. 2021, 10, 774. https://doi.org/10.3390/jcm10040774
Covello G, Loiudice P, Maglionico MN, Nardi M, Figus M, Posarelli C. Combined Phacoemulsification and Ex-PRESS Implant with Everting Suture in Primary Angle-Closure Glaucoma: Survival Analysis and Predictive Factors. Journal of Clinical Medicine. 2021; 10(4):774. https://doi.org/10.3390/jcm10040774
Chicago/Turabian StyleCovello, Giuseppe, Pasquale Loiudice, Maria Novella Maglionico, Marco Nardi, Michele Figus, and Chiara Posarelli. 2021. "Combined Phacoemulsification and Ex-PRESS Implant with Everting Suture in Primary Angle-Closure Glaucoma: Survival Analysis and Predictive Factors" Journal of Clinical Medicine 10, no. 4: 774. https://doi.org/10.3390/jcm10040774
APA StyleCovello, G., Loiudice, P., Maglionico, M. N., Nardi, M., Figus, M., & Posarelli, C. (2021). Combined Phacoemulsification and Ex-PRESS Implant with Everting Suture in Primary Angle-Closure Glaucoma: Survival Analysis and Predictive Factors. Journal of Clinical Medicine, 10(4), 774. https://doi.org/10.3390/jcm10040774