
Renal Denervation for Uncontrolled and Resistant Hypertension: Systematic Review and Network Meta-Analysis of Randomized Trials

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
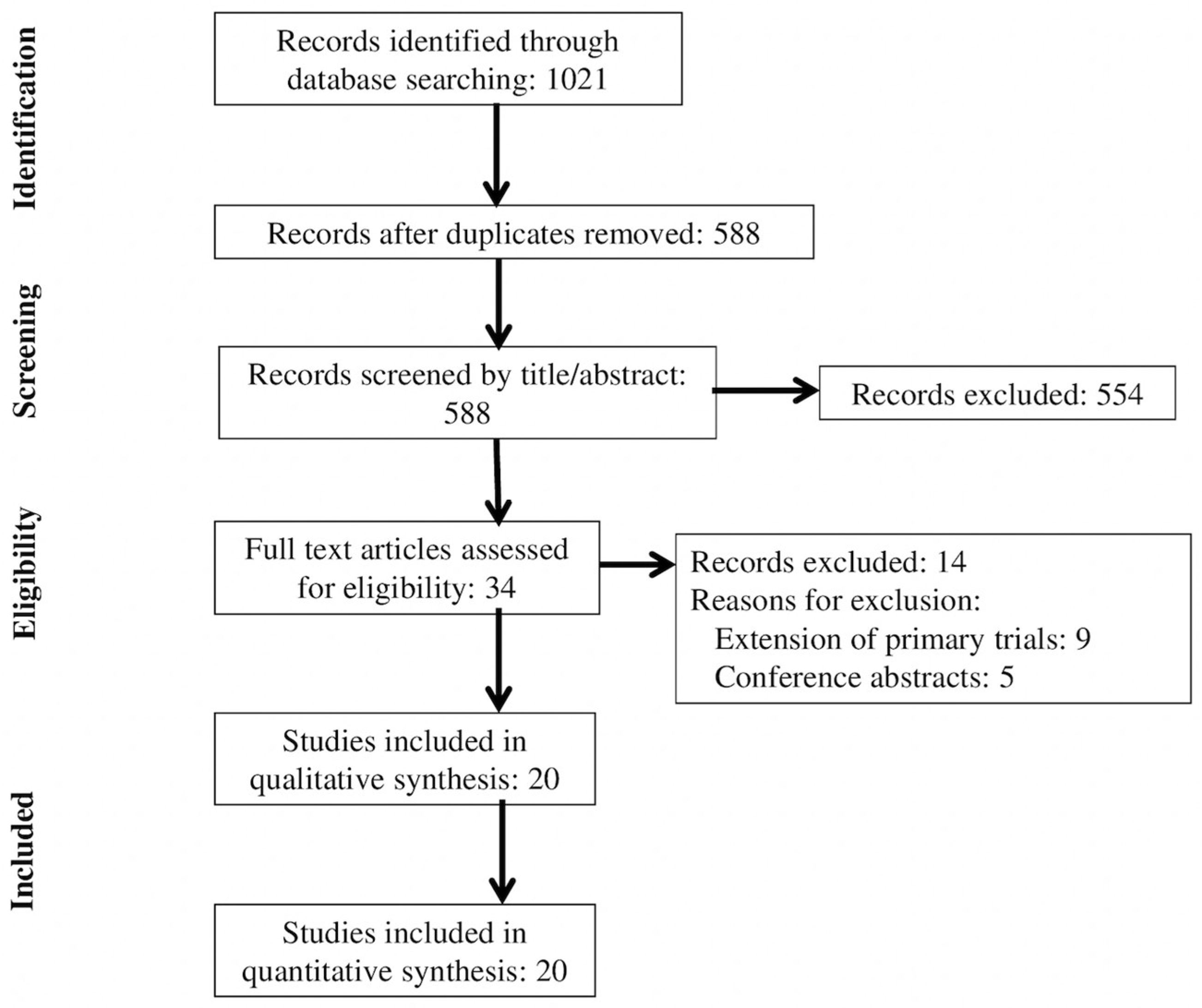
3.1. Study Selection
3.2. Trial Characteristics
3.3. Risk of Bias Assessment
3.4. Network Meta-Analyses of Primary Outcomes
3.5. Network Meta-Analyses of Secondary Outcomes
3.6. Sensitivity Analyses
3.7. Effect of Renal Denervation on Clinical Outcomes
4. Discussion
4.1. Main Findings
4.2. What Is Known in the Literature
4.3. What Our Study Adds to the Literature
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Carey, R.M.; Calhoun, D.A.; Bakris, G.L.; Brook, R.D.; Daugherty, S.L.; Dennison-Himmelfarb, C.R.; Egan, B.M.; Flack, J.M.; Gidding, S.S.; Judd, E.; et al. Resistant hypertension: Detection, evaluation, and management: A scientific statement from the American Heart Association. Hypertension 2018, 72, e53–e90. [Google Scholar] [CrossRef]
- Valderrama, A.L.; Gillespie, C.; King, S.C.; George, M.G.; Hong, Y.; Gregg, E. Vital signs: Awareness and treatment of uncontrolled hypertension among adults-United States, 2003–2010. Morb. Mortal. Wkly. Rep. 2012, 61, 703–709. [Google Scholar]
- Kiuchi, M.G.; Esler, M.D.; Fink, G.D.; Osborn, J.W.; Banek, C.T.; Böhm, M.; Denton, K.M.; DiBona, G.F.; Everett, T.H.; Grassi, G.; et al. Renal denervation update from the International Sympathetic Nervous System Summit. JACC 2019, 73, 3006–3017. [Google Scholar] [CrossRef]
- Weber, M.A.; Mahfoud, F.; Schmieder, R.E.; Kandzari, D.E.; Tsioufis, K.P.; Townsend, R.R.; Kario, K.; Böhm, M.; Sharp, A.S.; Davies, J.E.; et al. Renal denervation for treating hypertension: Current scientific and clinical evidence. JACC Cardiovasc. Interv. 2019, 12, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Zhang, D.; Luo, S.; Qin, S. Effect of catheter-based renal denervation on uncontrolled hypertension: A systematic review and meta-analysis. Mayo Clin. Proc. 2019, 94, 1695–1706. [Google Scholar] [CrossRef]
- Dahal, K.; Khan, M.; Siddiqui, N.; Mina, G.; Katikaneni, P.; Modi, K.; Azrin, M.; Lee, J. Renal denervation in the management of hypertension: A meta-analysis of sham-controlled trials. Cardiovasc. Revasc. Med. 2019, 21, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Coppolino, G.; Pisano, A.; Rivoli, L.; Bolignano, D. Renal denervation for resistant hypertension. Cochrane Database Syst. Rev. 2017, 2, CD011499. [Google Scholar] [PubMed]
- Yao, Y.; Zhang, D.; Qian, J.; Deng, S.; Huang, Y.; Huang, J. The effect of renal denervation on resistant hypertension: Meta-analysis of randomized controlled clinical trials. Clin. Exp. Hypertens. 2016, 38, 278–286. [Google Scholar] [CrossRef]
- Fadl Elmula, F.E.M.; Jin, Y.; Yang, W.Y.; Thijs, L.; Lu, Y.C.; Larstorp, A.C.; Persu, A.; Sapoval, M.; Rosa, J.; Widimský, P.; et al. Meta-analysis of randomized controlled trials of renal denervation in treatment-resistant hypertension. Blood Press. 2015, 24, 263–274. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef] [Green Version]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Hoaglin, D.C.; Hawkins, N.; Jansen, J.P.; Scott, D.A.; Itzler, R.; Cappelleri, J.C.; Boersma, C.; Thompson, D.; Larholt, K.M.; Diaz, M.; et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: Report of the ISPOR task force on indirect treatment comparisons good research practices: Part 2. Value Health 2011, 14, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Jackson, D.; Barrett, J.K.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.A.; Kirtane, A.J.; Weir, M.R.; Radhakrishnan, J.; Das, T.; Berk, M.; Mendelsohn, F.; Bouchard, A.; Larrain, G.; Haase, M.; et al. The REDUCE HTN: REINFORCE: Randomized, Sham-Controlled Trial of Bipolar Radiofrequency Renal Denervation for the Treatment of Hypertension. JACC Cardiovasc. Interv. 2020, 13, 461–470. [Google Scholar] [CrossRef]
- Böhm, M.; Townsend, R.R.; Kario, K.; Mahfoud, F.; Weber, M.A.; Schmieder, R.E.; Tsioufis, K.; Pocock, S.; Konstantinidis, D.; Choi, J.W.; et al. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED Pivotal): A multicentre, randomised, sham-controlled trial. Lancet 2020, 395, 1444–1451. [Google Scholar] [CrossRef]
- Fengler, K.; Rommel, K.P.; Blazek, S.; Besler, C.; Hartung, P.; von Roeder, M.; Petzold, M.; Winkler, S.; Höllriegel, R.; Desch, S.; et al. A three-arm randomized trial of different renal denervation devices and techniques in patients with resistant hypertension (RADIOSOUND-HTN). Circulation 2019, 139, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Azizi, M.; Schmieder, R.E.; Mahfoud, F.; Weber, M.A.; Daemen, J.; Davies, J.; Basile, J.; Kirtane, A.J.; Wang, Y.; Lobo, M.D.; et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): A multicentre, international, single-blind, randomised, sham-controlled trial. Lancet 2018, 391, 2335–2345. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Böhm, M.; Mahfoud, F.; Townsend, R.R.; Weber, M.A.; Pocock, S.; Tsioufis, K.; Tousoulis, D.; Choi, J.W.; East, C.; et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. Lancet 2018, 391, 2346–2355. [Google Scholar] [CrossRef]
- Schmieder, R.E.; Ott, C.; Toennes, S.W.; Bramlage, P.; Gertner, M.; Dawood, O.; Baumgart, P.; O’Brien, B.; Dasgupta, I.; Nickenig, G.; et al. Phase II randomized sham-controlled study of renal denervation for individuals with uncontrolled hypertension- WAVE IV. J. Hypertens. 2018, 36, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Warchol-Celinska, E.; Prejbisz, A.; Kadziela, J.; Florczak, E.; Januszewicz, M.; Michalowska, I.; Dobrowolski, P.; Kabat, M.; Sliwinski, P.; Klisiewicz, A.; et al. Renal denervation in resistant hypertension and obstructive sleep apnea: Randomized proof-of-concept phase II trial. Hypertension 2018, 72, 381–390. [Google Scholar] [CrossRef]
- de Jager, R.L.; de Beus, E.; Beeftink, M.M.A.; Sanders, M.F.; Vonken, E.J.; Voskuil, M.; van Maarseveen, E.M.; Bots, M.L.; Blankestijn, P.J.; SYMPATHY Investigators. Impact of medication adherence on the effect of renal denervation: The SYMPATHY trial. Hypertension 2017, 69, 678–684. [Google Scholar] [CrossRef]
- Jacobs, L.; Persu, A.; Huang, Q.F.; Lengelé, J.P.; Thijs, L.; Hammer, F.; Yang, W.Y.; Zhang, Z.Y.; Renkin, J.; Sinnaeve, P.; et al. Results of a randomized controlled pilot trial of intravascular renal denervation for management of treatment-resistant hypertension. Blood Press. 2017, 26, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Pekarskiy, S.E.; Baev, A.E.; Mordovin, V.F.; Semke, G.V.; Ripp, T.M.; Falkovskaya, A.U.; Lichikaki, V.A.; Sitkova, E.S.; Zubanova, I.V.; Popov, S.V. Denervation of the distal renal arterial branches vs. conventional main renal artery treatment: A randomized controlled trial for treatment of resistant hypertension. J. Hypertens. 2017, 35, 369–375. [Google Scholar] [CrossRef]
- Townsend, R.R.; Mahfoud, F.; Kandzari, D.E.; Kario, K.; Pocock, S.; Weber, M.A.; Ewen, S.; Tsioufis, K.; Tousoulis, D.; Sharp, A.S.P.; et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): A randomised, sham-controlled, proof-of-concept trial. Lancet 2017, 390, 2160–2170. [Google Scholar] [CrossRef]
- Mathiassen, O.N.; Vase, H.; Bech, J.N.; Christensen, K.L.; Buus, N.H.; Schroeder, A.P.; Lederballe, O.; Rickers, H.; Kampmann, U.; Poulsen, P.L.; et al. Renal denervation in treatment-resistant essential hypertension. A randomized, SHAM-controlled, double-blinded 24-h blood pressure-based trial. J. Hypertens. 2016, 34, 1639–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveras, A.; Armario, P.; Clarà, A.; Sans-Atxer, L.; Vázquez, S.; Pascual, J.; De la Sierra, A. Spironolactone versus sympathetic renal denervation to treat true resistant hypertension: Results from the DENERVHTA study- a randomized controlled trial. J. Hypertens. 2016, 34, 1863–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, M.; Sapoval, M.; Gosse, P.; Monge, M.; Bobrie, G.; Delsart, P.; Midulla, M.; Mounier-Véhier, C.; Courand, P.Y.; Lantelme, P.; et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): A multicentre, open-label, randomised controlled trial. Lancet 2015, 385, 1957–1965. [Google Scholar] [CrossRef]
- Desch, S.; Okon, T.; Heinemann, D.; Kulle, K.; Röhnert, K.; Sonnabend, M.; Petzold, M.; Müller, U.; Schuler, G.; Eitel, I.; et al. Randomized sham-controlled trial of renal sympathetic denervation in mild resistant hypertension. Hypertension 2015, 65, 1202–1208. [Google Scholar] [CrossRef] [Green Version]
- Kario, K.; Ogawa, H.; Okumura, K.; Okura, T.; Saito, S.; Ueno, T.; Haskin, R.; Negoita, M.; Shimada, K.; SYMPLICITY HTN-Japan Investigators. SYMPLICITY HTN-Japan–First randomized controlled trial of catheter-based renal denervation in Asian patients. Circ. J. 2015, 79, 1222–1229. [Google Scholar] [CrossRef] [Green Version]
- Rosa, J.; Widimský, P.; Toušek, P.; Petrák, O.; Čurila, K.; Waldauf, P.; Bednář, F.; Zelinka, T.; Holaj, R.; Štrauch, B.; et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true-resistant hypertension: Six-month results from the Prague-15 study. Hypertension 2015, 65, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.L.; Kandzari, D.E.; O’Neill, W.W.; D’Agostino, R.; Flack, J.M.; Katzen, B.T.; Leon, M.B.; Liu, M.; Mauri, L.; Negoita, M.; et al. A controlled trial of renal denervation for resistant hypertension. N. Engl. J. Med. 2014, 370, 1393–1401. [Google Scholar] [CrossRef] [Green Version]
- Fadl Elmula, F.E.M.; Hoffmann, P.; Larstorp, A.C.; Fossum, E.; Brekke, M.; Kjeldsen, S.E.; Gjønnæss, E.; Hjørnholm, U.; Kjaer, V.N.; Rostrup, M.; et al. Adjusted drug treatment is superior to renal sympathetic denervation in patients with true treatment-resistant hypertension. Hypertension 2014, 63, 991–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esler, M.D.; Krum, H.; Sobotka, P.A.; Schlaich, M.P.; Schmieder, R.E.; Böhm, M.; Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): A randomised controlled trial. Lancet 2010, 376, 1903–1909. [Google Scholar] [PubMed]
- Ruilope, L.M.; Rodríguez-Sánchez, E.; Navarro-García, J.A.; Segura, J.; Órtiz, A.; Lucia, A.; Ruiz-Hurtado, G. Resistant hypertension: New insights and therapeutic perspectives. Resistant hypertension: New insights and therapeutic perspectives. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 6, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Bosch, J.; Dagenais, G.; Zhu, J.; Xavier, D.; Liu, L.; Pais, P.; López-Jaramillo, P.; Leiter, L.A.; Dans, A.; et al. Cholesterol lowering in intermediate-risk persons without cardiovascular disease. N. Engl. J. Med. 2016, 374, 2021–2031. [Google Scholar] [CrossRef] [Green Version]
- Mahfoud, F.; Renkin, J.; Sievert, H.; Bertog, S.; Ewen, S.; Böhm, M.; Lengelé, J.P.; Wojakowski, W.; Schmieder, R.; van der Giet, M.; et al. Alcohol-Mediated Renal Denervation Using the Peregrine System Infusion Catheter for Treatment of Hypertension. J. Am. Coll. Cardiol. Interv. 2020, 13, 471–484. [Google Scholar] [CrossRef]
- Grossman, E. Ambulatory blood pressure monitoring in the diagnosis and management of hypertension. Diabetes Care 2013, 36, S307–S311. [Google Scholar] [CrossRef] [Green Version]
- Rücker, G.; Schwarzer, G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Acronym/Author, Year [reference] | Country (ies) | RDN Arm(s); Sample | Follow-Up Time (mo) | Type of HTN Patients; Definition of HTN | Description of RDN Type (s) | Type of Control Arm; Description of Control | Primary Outcome | Mean Age (SD) | Mean BMI (SD) | Number of AHT Drugs Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|
| REDUCE HTN: REINFORCE/Weber, 2020 [14] | USA | RF MRA; 51 | 2 | UH; office SBP of ≥150 and <180 mm Hg, an average 24-h ambulatory SBP of ≥135, and <170 mm Hg after 4-week antihypertensive medication washout | RF of the full renal artery length | Sham; renal angiography alone | Mean reduction in ambulatory SBP at 2 months | 58.4 (9.9) | NR | Off AHT |
| SPYRAL Pivotal/Bohm, 2020 [15] | Australia, Austria, Canada, Germany, Greece, Ireland, Japan, the UK, and the USA | RF MRA + branches; 331 | 3 | UH; office SBP 150 to 180 mmHg, office DBP at least 90 mmHg | The catheter has four electrodes designed to simultaneously or individually deliver radiofrequency ablation (intended duration of 60 s) to all four quadrants of the renal arteries and branch vessels with each activation; 45 s or longer was considered a successful ablation | Sham; renal angiogram only | Mean reduction in ambulatory SBP at 3 months | 52.5 (10.6) | 31.0 (5.7) | Off AHT |
| RADIOSOUND HTN/Fengler, 2019 [16] | Germany | US MRA; 120 | 3 | RH; office SBP >160 or DBP >90 despite treatment with ≥3 classes of AHT drugs on ≥50% max doses including ≥1 diuretic. AHT meds had to be stable for ≥4 weeks | US Paradise catheter; balloon cooled devise creates fully circumferential thermal ablation using acoustic energy | RF MRA; RF MRA + branches; RF: Symplicity Spyral catheter; administers ≤ 4 ablations simultaneously in spiral pattern using heat | Change in ambulatory daytime SBP at 3 months | 63.5 (9.4) | 31.6 (5.6) | 5.0 (1.4) |
| RADIANCE HTN SOLO/Azizi, 2018 [17] | USA, Germany, Netherlands, Belgium, UK | US MRA; 146 | 2 | UH; at screening: uncontrolled office BP ≥140/90 but <180/110 on 0 to 2 drugs; or controlled: office BP <140/90 on 1 to 2 drugs. After 4 weeks of AHT discontinuation: Ambulatory SBP ≥135, DBP ≥85 and <170/105 | US Paradise RDN system; patients received about 5.4 US emissions in the MRAs; 9 patients received ablation in accessory RAs; ≥2 US emissions were performed in 71 patients | Sham; renal angiogram only | Change in ambulatory daytime SBP at 2 months | 53.9 (10.1) | 29.5 (5.4) | Off AHT |
| SPYRAL HTN ON/Kandazari, 2018 [18] | USA, Germany, Japan, UK, Australia, Austria, Greece | RF MRA + branches; 80 | 6 | UH; office SBP 150 to 180 and DBP ≥90. 24-h ambulatory BP 140 to 170 at second screening and were on 1 to 3 AHT meds ≥50% of the max doses for ≥6 weeks | Symplicity Spyral catheter; circumferential RF ablation in the 4 quadrants of the RA and branch vessels between 3 and 8 mm in diameter | Sham; renal angiogram required to stay on the procedure table for at least 20 min with sensory masking post angiogram | Ambulatory BP change at 6 months | 53.4 (9.8) | 32 (5.5) | 2.3 (0.85) |
| WAVE IV/Schmeider, 2018 [19] | Czech Republic, Germany, New Zealand, Poland, UK | US MRA; 81 | 6 | RH; office SBP ≥160 while taking ≥3 AHT meds at max tolerated doses with 1 being a diuretic | Kona Surround Sound system; bilateral RDN using therapeutic levels of ultrasound energy | Sham; bilateral sham treatment using diagnostic levels of ultrasound energies | Difference in office SBP at 24 weeks | 61.1 (11.1) | 29.8 (4.3) | 4.6 (1.5) |
| Warchol-Celinska, 2018 [20] | Poland | RF MRA; 60 | 3 | RH + OSA; office SBP ≥140, mean daytime SBP ABPM ≥135 mmHg receiving and adhering to full doses of ≥3 AHT drugs including a diuretic for ≥4 weeks before screening | Symplicity Flex catheter; RF ablations of ≤8 W were applied, lasting <2 min each to obtain ≤6 ablations separated both longitudinally and rotationally within RA | AHT; maintenance of AHT medications only | Reduction in office SBP at 3 months | 55.2 (9.2) | 34.3 (5.4) | 4.95 (0.87) |
| SYMPATHY/De Jager, 2017 [21] | Netherlands | RF MRA + AHT; 139 | 6 | RH; average daytime SBP ABPM ≥135 despite use of ≥3 BP lowering agents | Symplicity Flex catheter (n = 60); EnligHTN ablation catheter (n = 40). Mean number of ablations was 15; also, usual AHT | AHT; medication only | Change in daytime systolic ABPM after 6 months | 61.4 (11.4) | 28.8 (4.7) | 3.4 (1.3) |
| INSPIRED/Jacobs, 2017 [22] | Belgium | RF MRA + AHT; 15 | 6 | RH; 24-h ambulatory SBP ≥130 or DBP ≥80 while taking ≥3 AHT meds | EnligHTN catheter; RDN + usual AHT; 8 to 12 ablations were made from the distal MRA to the ostium. In case of a long RA, the basket was placed more proximal | AHT; optimized drug regimen maintenance | Change in 24-h ambulatory SBP and in glomerular filtration rate at 6 months | 48.1 (9.3) | 30.3 (4.6) | 4.0 (1.5) |
| Pekarskiy, 2017 [23] | Russia | RF MRA + branches; 51 | 6 | RH; office SBP ≥160 or DBP ≥100 despite stable (>3 mo) prescribed treatment with full doses of ≥3 AHT drugs including a diuretic | Symplicity Flex catheter; further advanced into segmental branches beyond main bifurcation, 2–4 separate point treatments per branch; 4 lesions if branch diameter ≥4 mm, 2 lesions if less | RF MRA; Symplicity Flex catheter; ablations in MRA only | Change in 24-h mean ambulatory SBP at 6 months | 55.7 (8.6) | NR | 4.1 (0.9) |
| SPYRAL HTN OFF/Townsend, 2017 [24] | USA, Germany, Japan, UK, Australia, Austria, Greece | RF MRA + branches; 80 | 3 | UH; office SBP 150 to 180, DBP ≥90, and a mean 24-h ambulatory SBP 140 to 170 | Symplicity Spyral catheter; 4 electrodes positioned to apply RF energy circumferentially in all 4 quadrants of the RA and branch vessels | Sham; renal angiogram only | BP reduction based on ABPM at 3 months | 54.2 (10.9) | 30.0 (5.1) | Off AHT |
| ReSET/Mathiassen, 2016 [25] | Denmark | RF MRA; 69 | 6 | RH; daytime ABPM SBP ≥ 145, one month of stable AHT with ≥3 meds including a diuretic | Symplicity Flex catheter; 4–6 RF treatments of 5–8 W were applied for 2 min to cover the entire circumference in a spiral manner along the length of each MRA | Sham; dummy radiograph scan performed for another 10–15 min before removing sheath | Change in daytime ABPM SBP at 3 months | 55.7 (8.8) | 28.5 (4.5) | 4.1 (1.1) |
| DENERVHT/Oliveras, 2016 [26] | Spain | RF MRA + AHT; 24 | 6 | RH; office SBP ≥150 and 24-h SBP ≥140 despite getting ≥3 full dose AHT drugs (1 a diuretic but no aldosterone antagonist) | Symplicity Flex catheter; 4–6 applications of low power RF energy (8 W) delivered to each RA from distal to proximal; also, baseline AHT | AHT; baseline AHT + 25 mg spironolactone with forced titration to 50 mg after 1 mo | Change in ambulatory 24-h SBP at 6 months | 63.5 (7.5) | 32.0 (5.7) | 4.1 (0.7) |
| DENERHTN/Azizi, 2015 [27] | France | RF MRA + AHT; 106 | 6 | RH; office SBP ≥140 or DBP ≥90 despite stable regimen of max doses of ≥3 AHT drugs of different classes, including a diuretic | Symplicity Flex catheter; 2–4 weeks after randomization | AHT; spironolactone 25 mg/d, bisoprolol 10 mg/d, SR prazosin 5 mg/d, rilmenidine 1 mg/d added to triple drugs | Change in daytime ambulatory SBP at 6 months | 55.2 (10.4) | 30.2 (4.7) | NR |
| Desch, 2015 [28] | Germany | RF MRA; 71 | 6 | RH; mean daytime SBP on 24-h ambulatory BP measurement 135 to 149 or DBP 90 to 94 despite intake of ≥3 AHT drugs including a diuretic at max tolerated doses | Symplicity Flex catheter; 4–6 ablation runs for 2 min in each RA delivered circumferentially to wall from distal to proximal | Sham; saline infusion, angiography of renal arteries and simulated RDN procedure with 4–6 sham runs | Change in 24-h SBP at 6 months | 60.9 (8.8) | 31.5 (4.5) | 4.3 (1.3) |
| SYMPLICITY HTN JAPAN/Kario, 2015 [29] | Japan | RF MRA; 41 | 6 | RH; office SBP ≥160 on stable regimen of ≥3 AHT classes at max tolerated dose including a diuretic for ≥6 w prior to enrollment. 24-h ambulatory SBP ≥135 | Symplicity Flex catheter; 4–6 ablations in each RA in a helical pattern, rotating as the catheter is pulled back from the distal portion to the proximal portion of the MRA | AHT; current AHT only | Change in office SBP at 6 months | 57.9 (12.4) | 27.5 (4.8) | 4.9 (1.6) |
| PRAGUE-15/Rosa, 2015 [30] | Czech Republic | RF MRA; 106 | 6 | RH; office SBP >140 after treatment with ≥3 AHT drugs at optimal doses, including a diuretic | Symplicity Flex catheter; 4–6 applications of low power RF energy to each RA. Helical fashion within the artery by rotating the catheter during pullback. Distance between ablation sites was 5 mm | AHT; including spironolactone | SBP and DBP by 24-h ABPM at 6 months | 57.5 (10.6) | 32.3 (4.6) | 5.2 (1.2) |
| SYMPLICITY HTN-3/Bhatt, 2014 [31] | USA | RF MRA; 535 | 6 | RH; SBP of ≥160 and taking max tolerated doses of ≥3 AHT drugs of complementary classes, 1 being a diuretic | Symplicity Flex catheter; delivers low-level RF energy (8W); 4 to 6 ablations up to 120 s to the distal RA and rotating helical pattern | Sham; renal angiography only | Change in office SBP at 6 months | 57.4 (10.7) | 34.1 (6.5) | 5.1 (1.4) |
| OSLO RDN/Fadl Elmula, 2014 [32] | Norway | RF MRA; 20 | 6 | RH; office SBP >140 despite max tolerated doses of ≥3 AHT drugs including a diuretic | Symplicity Flex catheter system as described in SYMPLICITY HTN-2 trial | AHT; AHT medication adjusted at baseline, 1 and 3 months | Change in office SBP at 6 months | 59.8 (8.8) | 29.5 (5.2) | 5.0 (1.4) |
| SYMPLICITY HTN-2/Elser, 2010 [33] | Europe, Australia, New Zealand | RF MRA + AHT; 106 | 6 | RH; SBP ≥160 despite compliance with ≥3 AHT drugs | Symplicity Flex catheter; 4–6 discrete low power RF treatments applied along the length of both MRA | AHT; maintenance of previous AHT | Change in seated office SBP at 6 months | 58 (12) | 31 (5) | 5.2 (1.6) |
| RF MRA + branches | −4.2 (−8.3 to −0.2) | −6.6 (−13.4 to 0.25) | −2.5 (−7.8 to 3.7) | −3.7 (−7.1 to −0.2) | −6.8 (−12.7 to −0.8) |
| −7.8 (−15.1 to −0.4) | RF MRA | −2.3 (−7.8 to 3.1) | 1.7 (−3.0 to 6.4) | 0.6 (−2.1 to 3.2) | −2.5 (−6.8 to 1.8) |
| −11.9 (−23.4 to −0.4) | −4.1 (−13.0 to 4.8) | RF MRA + AHT R | 4.0 (−3.2 to 11.2) | 2.9 (−3.2 to 8.9) | −0.2 (−3.5 to 3.1) |
| −6.0 (−15.8 to 3.8) | 1.8 (−7.1 to 10.7) | 5.9 (−6.7 to 18.5) | US MRA | −1.1 (−5.1 to 2.8) | −4.2 (−10.6 to 2.2) |
| −7.2 (−13.6 to −0.8) | 0.6 (−4.4 to 5.5) | 4.7 (−5.5 to 14.8) | −1.2 (−8.6 to 6.2) | Sham S | −3.1 (−8.1 to 1.2) |
| −12.9 (−22.6 to −3.2) | 5.9 (−11.4 to 1.3) | −1.0 (−7.2 to 5.2) | −6.9 (−17.8 to 4.1) | −5.6 (−13.7 to 2.4) | AHT |
| RF MRA + branches | −2.2 (−10.6 to 6.3) | 3.2 (−6.3 to 12.7) | −3.1 (−10.9 to 4.7) | −3.5 (−8.6 to 1.5) | −2.2 (−10.6 to 6.3) |
| −6.7 (−22.2 to 8.9) | RF MRA | 6.1 (−0.9 to 13.0) | −0.2 (−8.2 to 7.8) | −0.7 (−6.0 to 4.6) | 0.7 (−4.76 to 6.2) |
| 3.64 (−18.1 to 25.4) | 10.3 (−4.9 to 25.5) | RF MRA + AHT | −6.3 (−16.9 to 4.3) | −6.7 (−15.5 to 2.0) | −5.4 (−9.6 to −1.1) |
| −9.15 (−29.2 to 10.9) | −2.46 (−22.6 to 17.7) | −12.8 (−38.0 to 12.5) | US MRA | −0.5 (−6.4 to 5.5) | 0.9 (−8.8 to 10.6) |
| −6.9 (−19.9 to 6.3) | −0.2 (−13.4 to 13.1) | −10.5 (−30.7 to 9.7) | 2.3 (−12.9 to 17.5) | Sham | 1.4 (−6.2 to 9.0) |
| −7.3 (−26.4 to 11.8) | −0.7 (−11.7 to 10.4) | −10.1 (−21.4 to −0.6) | 1.8 (−21.2 to 24.8) | −0.5 (−17.7 to 16.7) | AHT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silverwatch, J.; Marti, K.E.; Phan, M.T.; Amin, H.; Roman, Y.M.; Pasupuleti, V.; Banach, M.; Barboza, J.J.; Hernandez, A.V. Renal Denervation for Uncontrolled and Resistant Hypertension: Systematic Review and Network Meta-Analysis of Randomized Trials. J. Clin. Med. 2021, 10, 782. https://doi.org/10.3390/jcm10040782
Silverwatch J, Marti KE, Phan MT, Amin H, Roman YM, Pasupuleti V, Banach M, Barboza JJ, Hernandez AV. Renal Denervation for Uncontrolled and Resistant Hypertension: Systematic Review and Network Meta-Analysis of Randomized Trials. Journal of Clinical Medicine. 2021; 10(4):782. https://doi.org/10.3390/jcm10040782
Chicago/Turabian StyleSilverwatch, Jonathan, Kristen E. Marti, Mi T. Phan, Hinali Amin, Yuani M. Roman, Vinay Pasupuleti, Maciej Banach, Joshuan J. Barboza, and Adrian V. Hernandez. 2021. "Renal Denervation for Uncontrolled and Resistant Hypertension: Systematic Review and Network Meta-Analysis of Randomized Trials" Journal of Clinical Medicine 10, no. 4: 782. https://doi.org/10.3390/jcm10040782
APA StyleSilverwatch, J., Marti, K. E., Phan, M. T., Amin, H., Roman, Y. M., Pasupuleti, V., Banach, M., Barboza, J. J., & Hernandez, A. V. (2021). Renal Denervation for Uncontrolled and Resistant Hypertension: Systematic Review and Network Meta-Analysis of Randomized Trials. Journal of Clinical Medicine, 10(4), 782. https://doi.org/10.3390/jcm10040782