
Symptomatic and Asymptomatic Patients in the Polish Atrial Fibrillation (POL-AF) Registry


 ,
,  , , , , , ,
, , , , , ,  , , , ,
, , , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
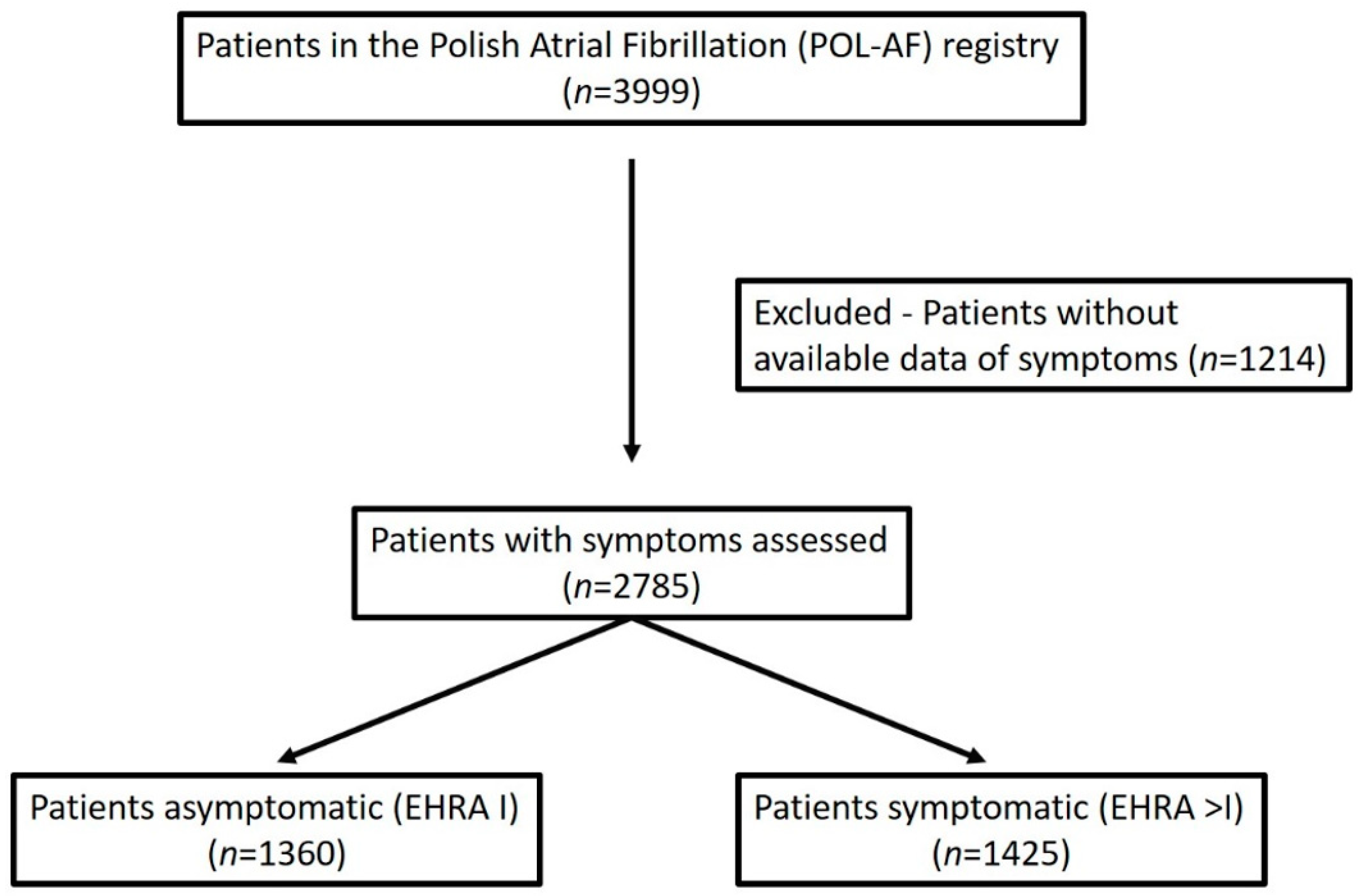
2.1. Patients
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, ehaa612. [Google Scholar] [CrossRef]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceornodolea, A.D.; Bal, R.; Severens, J.L. Epidemiology and management of atrial fibrillation and stroke: Review of data from four European countries. Stroke Res. Treat. 2017, 8593207. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Laroche, C.; Diemberger, I.; Fantecchi, E.; Popescu, M.I.; Rasmussen, L.H.; Sinagra, G.; Petrescu, L.; Tavazzi, L.; Maggioni, A.P.; et al. Asymptomatic atrial fibrillation: Clinical correlates, management, and outcomes in the EORP-AF Pilot General Registry. Am. J. Med. 2015, 128, 509.e2–518.e2. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Polovina, M.M.; Marinkovic, J.M.; Lip, G.Y. A comparison of clinical characteristics and long-term prognosis in asymptomatic and symptomatic patients with first-diagnosed atrial fibrillation: The Belgrade Atrial Fibrillation Study. Int. J. Cardiol. 2013, 168, 4744–4749. [Google Scholar] [CrossRef] [PubMed]
- Flaker, G.C.; Belew, K.; Beckman, K.; Vidaillet, H.; Kron, J.; Safford, R.; Mickel, M.; Barrell, P. AFFIRM Investigators. Asymptomatic atrial fibrillation: Demographic features and prognostic information from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am. Heart J. 2005, 149, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Freeman, J.V.; Simon, D.N.; Go, A.S.; Spertus, J.; Fonarow, G.C.; Gersh, B.J.; Hylek, E.M.; Kowey, P.R.; Mahaffey, K.W.; Thomas, L.E.; et al. Outcomes Registry for Better Informed Treatment of Atrial Fibrillation Investigators. Association between atrial fibrillation symptoms, quality of life, and patient outcomes: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circ. Cardiovasc. Qual. Outcomes 2015, 8, 393–402. [Google Scholar] [PubMed] [Green Version]
- Xiong, Q.; Proietti, M.; Senoo, K.; Lip, G.Y. Asymptomatic versus symptomatic atrial fibrillation: A systematic review of age/gender differences and cardiovascular outcomes. Int. J. Cardiol. 2015, 191, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, I.; Jelonek, O.; Uziębło-Życzkowska, B.; Chrapek, M.; Maciorowska, M.; Wójcik, M.; Błaszczyk, R.; Kapłon-Cieślicka, A.; Gawałko, M.; Budnik, M.; et al. Trends in the prescription of non-vitamin K antagonist oral anticoagulants for atrial fibrillation: Results of the Polish Atrial Fibrillation (POL-AF) Registry. J. Clin. Med. 2020, 9, 3565. [Google Scholar] [CrossRef] [PubMed]
- Uziębło-Życzkowska, B.; Krzesiński, P.; Maciorowska, M.; Gorczyca, I.; Jelonek, O.; Wójcik, M.; Błaszczyk, R.; Kapłon-Cieślicka, A.; Gawałko, M.; Tokarek, T.; et al. Antithrombotic therapy in patients with atrial fibrillation undergoing percutaneous coronary intervention, including compliance with current guidelines—Data from the POLish Atrial Fibrillation (POL-AF) Registry. Cardiovasc. Diagn. Ther. 2021, 11, 14–27. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y.H. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simantirakis, E.N.; Papakonstantinou, P.E.; Chlouverakis, G.I.; Kanoupakis, E.M.; Mavrakis, H.E.; Kallergis, E.M.; Arkolaki, E.G.; Vardas, P.E. Asymptomatic versus symptomatic episodes in patients with paroxysmal atrial fibrillation via long-term monitoring with implantable loop recorders. Int. J. Cardiol. 2017, 231, 125–130. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Laroche, C.; Ioachim, P.M.; Rasmussen, L.H.; Vitali-Serdoz, L.; Petrescu, L.; Darabantiu, D.; Crijns, H.J.; Kirchhof, P.; Vardas, P.; et al. Prognosis and treatment of atrial fibrillation patients by European cardiologists: One year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry). Eur. Heart J. 2014, 35, 3365–3376. [Google Scholar] [CrossRef]
- Dilaveris, P.E.; Kennedy, H.L. Silent atrial fibrillation: Epidemiology, diagnosis, and clinical impact. Clin. Cardiol. 2017, 40, 413–418. [Google Scholar] [CrossRef]
- Lévy, S.; Santini, L.; Cappato, R.; Steinbeck, G.; Capucci, A.; Saksena, S. Clinical classification and the subclinical atrial fibrillation challenge: A position paper of the European Cardiac Arrhythmia Society. J. Interv. Card. Electrophysiol. 2020, 59, 495–507. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Laroche, C.; Dan, G.-A.; Santini, M.; Kalarus, Z.; Rasmussen, L.H.; Oliveira, M.M.; Mairesse, G.; Crijns, H.J.G.M.; Simantirakis, E.; et al. A prospective survey in European Society of Cardiology member countries of atrial fibrillation management: Baseline results of EURObservational Research Programme Atrial Fibrillation (EORP-AF) Pilot General Registry. EP Eur. 2014, 16, 308–319. [Google Scholar] [CrossRef]
- Elliott, A.D.; Verdicchio, C.V.; Gallagher, C.; Linz, D.; Mahajan, R.; Mishima, R.; Kadhim, K.; Emami, M.; Middeldorp, M.E.; Hendriks, J.M.; et al. Factors contributing to exercise intolerance in patients with atrial fibrillation. Heart Lung Circ. 2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | EHRA I | EHRA > I | p | |
|---|---|---|---|---|
| Reasons for admission, n (%) | ||||
| AF | 994 (35.7) | 480 (35.3) | 514 (36.1) | 0.67 |
| CIED implantation | 233 (8.4) | 122 (9.0) | 111 (7.8) | 0.26 |
| Planned coronary angiography/angioplasty | 343 (12.3) | 181 (13.3) | 162 (11.4) | 0.13 |
| Acute coronary syndrome | 199 (7.1) | 94 (6.9) | 105 (7.4) | 0.64 |
| Heart failure | 458 (16.4) | 159 (11.7) | 299 (21.0) | <0.0001 |
| AF characteristics, n (%) | ||||
| History of cardioversion | 783 (28.1) | 457 (33.6) | 345 (24.2) | <0.0001 |
| AF at admission | 1893 (68.0) | 941 (69.2) | 952 (66.8) | 0.19 |
| First-diagnosed AF | 211 (7.6) | 60 (4.4) | 151 (10.6) | <0.0001 |
| Paroxysmal AF | 1355 (48.7) | 711 (52.3) | 644 (45.2) | 0.0002 |
| Time from first AF diagnosis * (years), mean(SD) | 4.8 (4.7) | 5.3 (4.7) | 4.3 (4.6) | <0.0001 |
| Total | EHRA I | EHRA > I | p | |
|---|---|---|---|---|
| Demographic data | ||||
| Age, mean (SD) | 72 (11) | 72 (11) | 72 (11) | 0.84 |
| Female gender, n (%) | 1181 (42.4) | 556 (40.9) | 625 (43.9) | 0.12 |
| Concomitant diseases, n (%) | ||||
| Hypertension | 2405 (86.4) | 1172 (86.2) | 1233 (86.5) | 0.83 |
| Diabetes | 1000 (35.9) | 479 (35.2) | 521 (36.6) | 0.48 |
| Heart failure | 1842 (66.1) | 961 (70.7) | 881 (61.8) | <0.0001 |
| HFrEF | 650 (23.7) | 292 (21.9) | 358 (25.4) | 0.033 |
| HFmrEF | 287 (10.5) | 138 (10.3) | 149 (10.6) | 0.88 |
| HFpEF | 951 (34.7) | 531 (39.8) | 374 (26.5) | <0.0001 |
| Coronary artery disease | 1481 (53.2) | 782 (57.5) | 699 (49.1) | <0.0001 |
| Previous myocardial infarction | 662 (23.8) | 311 (22.9) | 351 (24.6) | 0.29 |
| Chronic kidney disease | 778 (27.9) | 366 (26.9) | 412 (28.9) | 0.26 |
| Previous thromboembolic incident | 434 (15.6) | 248 (18.2) | 186 (13.1) | 0.0002 |
| Previous bleeding | 78 (2.8) | 41 (3.0) | 37 (2.6) | 0.58 |
| Thromboembolism and Bleeding Risk Scores | ||||
| CHA2DS2-VASc score (points), median (IQR) | 5 (4–6) | 5 (4–6) | 5 (3–6) | 0.10 |
| CHA2DS2-VASc ≥ 3 (points), mean (SD) | 2485 (89.2) | 1249 (91.8) | 1236 (86.7) | <0.0001 |
| HAS-BLED score (points), median (IQR) | 2 (2–3) | 2 (2–3) | 2 (2–3) | 0.13 |
| Total | EHRA I | EHRA > I | p | |
|---|---|---|---|---|
| Laboratory data, mean (SD) | ||||
| Hemoglobin, g/dL | 13.18 (1.96) | 13.15 (0.50) | 13.21 (0.50) | 0.67 |
| Creatinine, mg/dL | 1.259 (0.74) | 1.09 (0.9–1.38) | 1.10 (0.9–1.4) | 0.03 |
| Total cholesterol, mg/dL * | 162 (52) | 155 (50) | 168 (53) | <0.0001 |
| Echocardiography data, median (IQR) | ||||
| LVEF, % | 54 (40–60) | 55 (40–60) | 52 (40–60) | 0.001 |
| LA, mm * | 47 (42–51) | 48 (43–53) | 46 (42–50) | <0.0001 |
| LA area, cm square * | 29.0 (25.0–35.0) | 29.1 (25.0–34.9) | 29.0 (25.0–35.0) | 0.54 |
| LVDd, mm * | 52 (47–58) | 53 (48–58) | 51 (47–57) | <0.0001 |
| Type of Treatment, n (%) | EHRA I | EHRA > I | p |
|---|---|---|---|
| OAC | 1122 (82.8) | 1152 (81.1) | 0.27 |
| Amiodarone | 209 (15.6) | 332 (23.5) | <0.0001 |
| I class AAD | 176 (13.1) | 101 (7.2) | <0.0001 |
| Beta blockers | 1186 (88.4) | 1212 (85.8) | 0.048 |
| ACE inhibitors/sartans | 1094 (81.6) | 1069 (75.7) | 0.0002 |
| Aldosteron antagonists | 612 (45.6) | 504 (35.7) | <0.0001 |
| Calcium channel blockers | 509 (38.0) | 481 (34.1) | 0.037 |
| Statins | 1077 (80.3) | 1051 (74.4) | 0.0003 |
| Parameter | HR | 95% CI | p |
|---|---|---|---|
| First-diagnosed AF | 2.29 | 1.61–3.24 | <0.001 |
| Paroxysmal AF | 0.80 | 0.67–0.96 | 0.016 |
| History of electrical cardioversion | 0.65 | 0.53–0.79 | <0.001 |
| Heart failure | 0.59 | 0.48–0.72 | <0.001 |
| Coronary artery disease | 0.78 | 0.65–0.93 | 0.006 |
| Previous thromboembolic event | 0.77 | 0.61–0.97 | 0.03 |
| Left ventricular EF | 0.99 | 0.98–0.99 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiliszek, M.; Uziębło-Życzkowska, B.; Gorczyca, I.; Maciorowska, M.; Jelonek, O.; Wożakowska-Kapłon, B.; Wójcik, M.; Błaszczyk, R.; Gawałko, M.; Kapłon-Cieślicka, A.; et al. Symptomatic and Asymptomatic Patients in the Polish Atrial Fibrillation (POL-AF) Registry. J. Clin. Med. 2021, 10, 1091. https://doi.org/10.3390/jcm10051091
Kiliszek M, Uziębło-Życzkowska B, Gorczyca I, Maciorowska M, Jelonek O, Wożakowska-Kapłon B, Wójcik M, Błaszczyk R, Gawałko M, Kapłon-Cieślicka A, et al. Symptomatic and Asymptomatic Patients in the Polish Atrial Fibrillation (POL-AF) Registry. Journal of Clinical Medicine. 2021; 10(5):1091. https://doi.org/10.3390/jcm10051091
Chicago/Turabian StyleKiliszek, Marek, Beata Uziębło-Życzkowska, Iwona Gorczyca, Małgorzata Maciorowska, Olga Jelonek, Beata Wożakowska-Kapłon, Maciej Wójcik, Robert Błaszczyk, Monika Gawałko, Agnieszka Kapłon-Cieślicka, and et al. 2021. "Symptomatic and Asymptomatic Patients in the Polish Atrial Fibrillation (POL-AF) Registry" Journal of Clinical Medicine 10, no. 5: 1091. https://doi.org/10.3390/jcm10051091
APA StyleKiliszek, M., Uziębło-Życzkowska, B., Gorczyca, I., Maciorowska, M., Jelonek, O., Wożakowska-Kapłon, B., Wójcik, M., Błaszczyk, R., Gawałko, M., Kapłon-Cieślicka, A., Tokarek, T., Rajtar-Salwa, R., Bil, J., Wojewódzki, M., Szpotowicz, A., Krzciuk, M., Bednarski, J., Bakuła-Ostalska, E., Tomaszuk-Kazberuk, A., ... Krzesiński, P. (2021). Symptomatic and Asymptomatic Patients in the Polish Atrial Fibrillation (POL-AF) Registry. Journal of Clinical Medicine, 10(5), 1091. https://doi.org/10.3390/jcm10051091