
Emerging Medical Treatment for Hypertrophic Cardiomyopathy

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Mechanics of LVOT Obstruction
3. Available Medical Armamentarium for LVOTO
4. Disopyramide
5. Targeting HCM Pathophysiology: A Novel Approach Based on Molecular Knowledge
6. Clinical Trials with Mavacamten
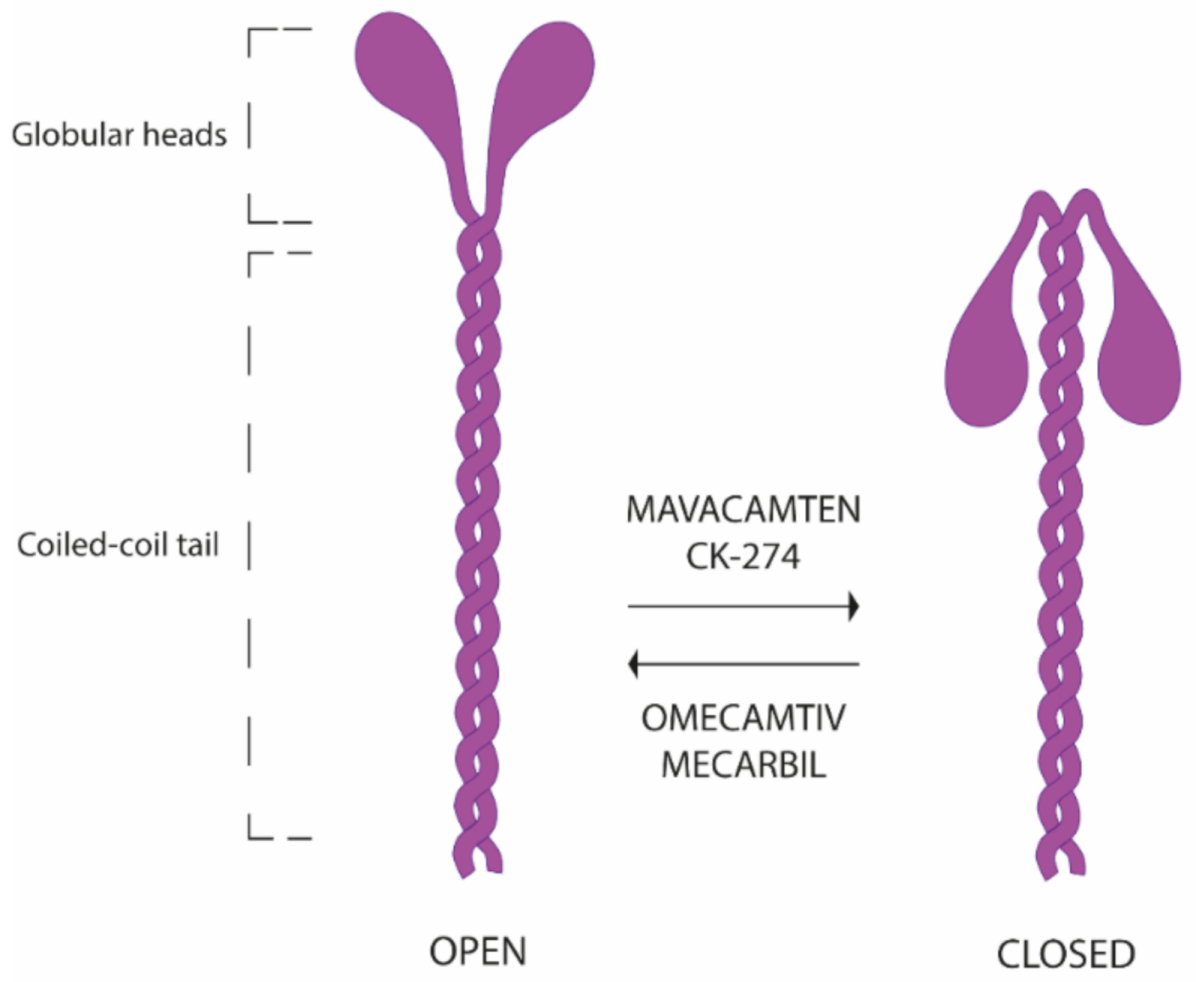
7. New Horizons in Selective Sarcomere Protein Modulation
8. Advances in the Surgical Approach to Obstructive HCM
9. Modifiable Cardiovascular Risk Factors
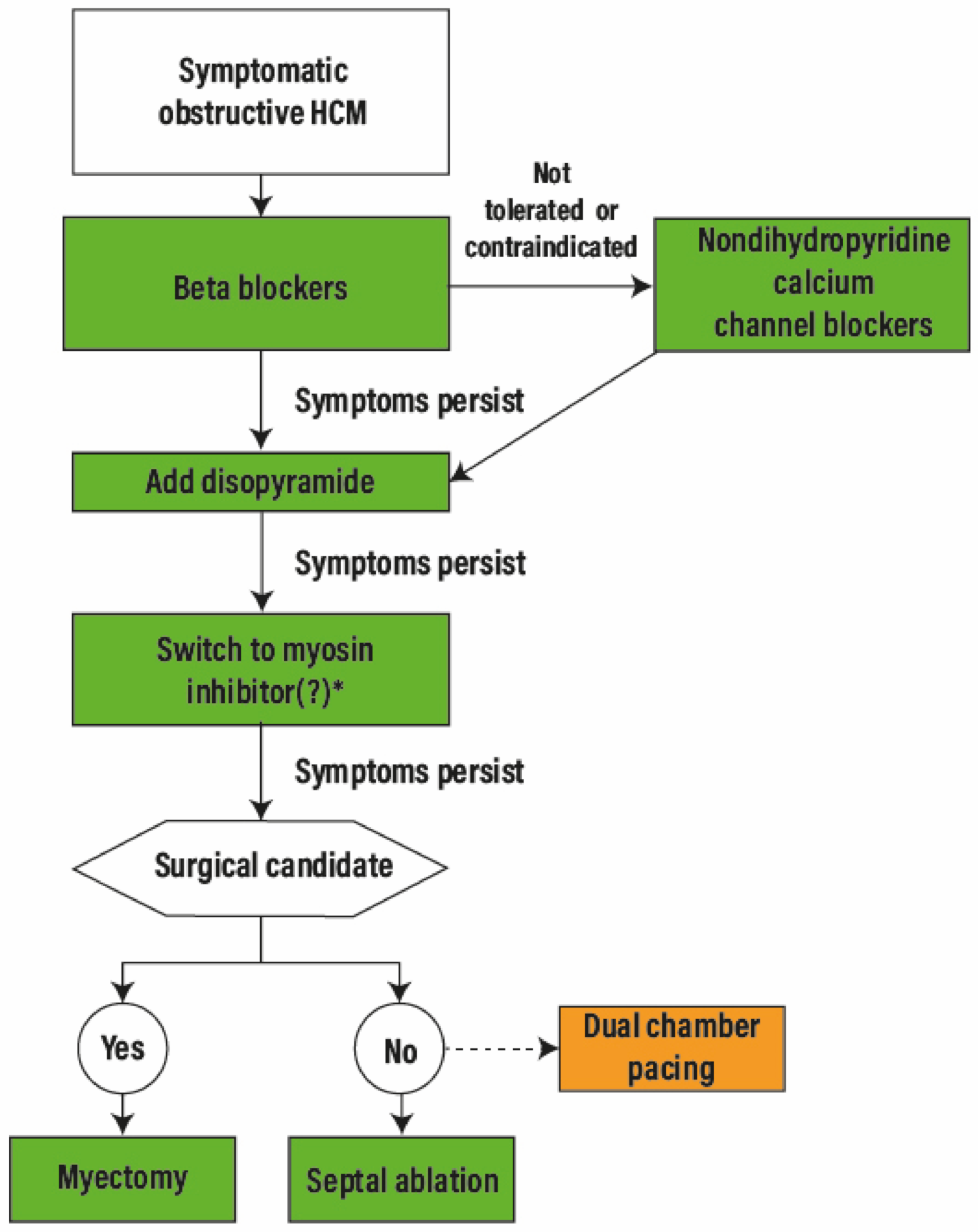
10. A Treatment Algorithm for the Next Decade
11. Conclusions
12. What’s New in This Review?
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| ALS | amyotrophic lateral sclerosis |
| ASA | Alcohol septal ablation |
| AV | Atrioventricular |
| FSTA | Fast skeletal muscle troponin activator |
| HCM | Hypertrophic cardiomyopathy |
| HCMSQ-SoB | Hypertrophic Cardiomyopathy Symptom Questionnaire Shortness-of-Breath |
| HF | Heart failure |
| KCCQ | Kansas City Cardiomyopathy Questionnaire |
| LV | left ventricle/ventricular |
| LVEF | Left ventricular ejection fraction |
| LVOT | Left ventricular outflow tract |
| LVOTO | Left ventricular outflow tract obstruction |
| NYHA | New York Heart Association |
| NTproBNP | N-terminal pro-brain natriuretic peptide |
| oHCM | obstructive HCM |
| pVO2 | peak oxygen consumption |
| SAM | Systolic anterior movement |
| SRT | septal reduction therapy |
References
- Maron, B.J.; Gardin, J.M.; Flack, J.M.; Gidding, S.S.; Kurosaki, T.T.; Bild, D.E. Prevalence of Hypertrophic Cardiomyopathy in a General Population of Young Adults: Echocardiographic Analysis of 4111 Subjects in the CARDIA Study. Circulation 1995, 92, 785–789. [Google Scholar] [CrossRef]
- Maron, B.J.; Maron, M.S.; Semsarian, C. Genetics of Hypertrophic Cardiomyopathy After 20 Years. J. Am. Coll. Cardiol. 2012, 60, 705–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivotto, I.; Cecchi, F.; Poggesi, C.; Yacoub, M.H. Developmental origins of hypertrophic cardiomyopathy phenotypes: A unifying hypothesis. Nat. Rev. Cardiol. 2009, 6, 317–321. [Google Scholar] [CrossRef]
- Maron, B.J.; Rowin, E.J.; Udelson, J.E.; Maron, M.S. Clinical Spectrum and Management of Heart Failure in Hypertrophic Cardiomyopathy. JACC Heart Fail. 2018, 6, 353–363. [Google Scholar] [CrossRef]
- Maron, M.S.; Olivotto, I.; Betocchi, S.; Casey, S.A.; Lesser, J.R.; Losi, M.A.; Cecchi, F.; Maron, B.J. Effect of Left Ventricular Outflow Tract Obstruction on Clinical Outcome in Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2003, 348, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, M.H.; El-Hamamsy, I.; Said, K.; Magdi, G.; Enein, F.A.; George, R.; Rossi, A.; Olivotto, I.; Cecchi, F. The Left Ventricular Outflow in Hypertrophic Cardiomyopathy: From Structure to Function. J. Cardiovasc. Transl. Res. 2009, 2, 510–517. [Google Scholar] [CrossRef]
- Ferrazzi, P.; Spirito, P.; Binaco, I.; Zyrianov, A.; Poggio, D.; Vaccari, G.; Grillo, M.; Pezzoli, L.; Scatigno, A.; Dorobantu, L.; et al. Congenital Muscular Mitral-Aortic Discontinuity Identified in Patients With Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2020, 76, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Sherrid, M.V.; Balaram, S.; Kim, B.; Axel, L.; Swistel, D.G. The Mitral Valve in Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 1846–1858. [Google Scholar] [CrossRef]
- MEMBERS WRITING COMMITTEE; Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef]
- Braunwald, E.; Lambrew, C.T.; Rockoff, S.D.; Ross, J.; Morrow, A.G. Idiopathic Hypertrophic Subaortic Stenosis: I. A Description of the Disease Based Upon an Analysis of 64 Patients. Circulation 1964, 29, 3–119. [Google Scholar] [CrossRef]
- Ammirati, E.; Contri, R.; Coppini, R.; Cecchi, F.; Frigerio, M.; Olivotto, I. Pharmacological treatment of hypertrophic cardiomyopathy: Current practice and novel perspectives: Pharmacological treatment of HCM. Eur. J. Heart Fail. 2016, 18, 1106–1118. [Google Scholar] [CrossRef]
- Epstein, S.E.; Rosing, D.R. Verapamil: Its potential for causing serious complications in patients with hypertrophic cardiomyopathy. Circulation 1981, 64, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Rosing, D.R.; Condit, J.R.; Maron, B.J.; Kent, K.M.; Leon, M.B.; Bonow, R.O.; Lipson, L.C.; Epstein, S.E. Verapamil therapy: A new approach to the pharmacologic treatment of hypertrophic cardiomyopathy: III. Effects of long-term administration. Am. J. Cardiol. 1981, 48, 545–553. [Google Scholar] [CrossRef]
- Kajimoto, K.; Imai, T.; Minami, Y.; Kasanuki, H. Comparison of Acute Reduction in Left Ventricular Outflow Tract Pressure Gradient in Obstructive Hypertrophic Cardiomyopathy by Disopyramide Versus Pilsicainide Versus Cibenzoline. Am. J. Cardiol. 2010, 106, 1307–1312. [Google Scholar] [CrossRef]
- Coppini, R.; Ferrantini, C.; Pioner, J.M.; Santini, L.; Wang, Z.J.; Palandri, C.; Scardigli, M.; Vitale, G.; Sacconi, L.; Stefàno, P.; et al. Electrophysiological and Contractile Effects of Disopyramide in Patients With Obstructive Hypertrophic Cardiomyopathy. JACC: Basic Transl. Sci. 2019, 4, 795–813. [Google Scholar] [CrossRef] [PubMed]
- Sherrid, M.V.; Shetty, A.; Winson, G.; Kim, B.; Musat, D.; Alviar, C.L.; Homel, P.; Balaram, S.K.; Swistel, D.G. Treatment of Obstructive Hypertrophic Cardiomyopathy Symptoms and Gradient Resistant to First-Line Therapy With β-Blockade or Verapamil. Circ. Heart Fail. 2013, 6, 694–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrid, M.V.; Barac, I.; McKenna, W.J.; Elliott, P.M.; Dickie, S.; Chojnowska, L.; Casey, S.; Maron, B.J. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2005, 45, 1251–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, W.; Ivanov, J.; Rakowski, H.; Wigle, E.D.; Linghorne, M.; Ralph-Edwards, A.; Williams, W.G.; Schwartz, L.; Guttman, A.; Woo, A. Long-Term Survival in Patients With Resting Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2011, 58, 2313–2321. [Google Scholar] [CrossRef] [Green Version]
- Adler, A.; Fourey, D.; Weissler-Snir, A.; Hindieh, W.; Chan, R.H.; Gollob, M.H.; Rakowski, H. Safety of Outpatient Initiation of Disopyramide for Obstructive Hypertrophic Cardiomyopathy Patients. J. Am. Heart Assoc. 2017, 6, e005152. [Google Scholar] [CrossRef]
- Pollick, C.; Giacomini, K.M.; Blaschke, T.F.; Nelson, W.L.; Turner-Tamiyasu, K.; Briskin, V.; Popp, R.L. The cardiac effects of d- and l-disopyramide in normal subjects: A noninvasive study. Circulation 1982, 66, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Sherrid, M.V. Indications for Surgery in Obstructive Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2021, 10, e019419. [Google Scholar] [CrossRef]
- Krendel, M.; Mooseker, M.S. Myosins: Tails (and Heads) of Functional Diversity. Physiology 2005, 20, 239–251. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.L.; Trivedi, D.V.; Sarkar, S.S.; Henze, M.; Ma, W.; Gong, H.; Rogers, C.S.; Gorham, J.M.; Wong, F.L.; Morck, M.M.; et al. Deciphering the super relaxed state of human β-cardiac myosin and the mode of action of mavacamten from myosin molecules to muscle fibers. Proc. Natl. Acad. Sci. USA 2018, 115, E8143–E8152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, E.M.; Wakimoto, H.; Anderson, R.L.; Evanchik, M.J.; Gorham, J.M.; Harrison, B.C.; Henze, M.; Kawas, R.; Oslob, J.D.; Rodriguez, H.M.; et al. A small-molecule inhibitor of sarcomere contractility suppresses hypertrophic cardiomyopathy in mice. Science 2016, 351, 617–621. [Google Scholar] [CrossRef] [Green Version]
- Heitner, S.B.; Jacoby, D.; Lester, S.J.; Owens, A.; Wang, A.; Zhang, D.; Lambing, J.; Lee, J.; Semigran, M.; Sehnert, A.J. Mavacamten Treatment for Obstructive Hypertrophic Cardiomyopathy: A Clinical Trial. Ann. Intern. Med. 2019, 170, 741–748. [Google Scholar] [CrossRef]
- Kubo, T.; Kitaoka, H.; Okawa, M.; Yamanaka, S.; Hirota, T.; Baba, Y.; Hayato, K.; Yamasaki, N.; Matsumura, Y.; Yasuda, N.; et al. Combined Measurements of Cardiac Troponin I and Brain Natriuretic Peptide Are Useful for Predicting Adverse Outcomes in Hypertrophic Cardiomyopathy. Circ. J. 2011, 75, 919–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saberi, S.; Cardim, N.; Yamani, M.H.; Schulz-Menger, J.; Li, W.; Florea, V.; Sehnert, A.J.; Kwong, R.Y.; Jerosch-Herold, M.; Masri, A.; et al. Mavacamten Favorably Impacts Cardiac Structure in Obstructive Hypertrophic Cardiomyopathy: EXPLORER-HCM CMR Substudy Analysis. Circulation 2021, 143, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.Y.; Mealiffe, M.E.; Bach, R.G.; Bhattacharya, M.; Choudhury, L.; Edelberg, J.M.; Hegde, S.M.; Jacoby, D.; Lakdawala, N.K.; Lester, S.J.; et al. Evaluation of Mavacamten in Symptomatic Patients With Nonobstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2020, 75, 2649–2660. [Google Scholar] [CrossRef]
- Hwee, D.T.; Hartman, J.J.; Wang, J.; Wu, Y.; Schaletzky, J.; Paliwal, P.; Lee, K.; Taheri, K.D.; Wehri, E.; Chuang, C.; et al. Abstract 332: Pharmacologic Characterization of the Cardiac Myosin Inhibitor, CK-3773274: A Potential Therapeutic Approach for Hypertrophic Cardiomyopathy. Circ. Res. 2019, 125, A332. [Google Scholar] [CrossRef]
- Cytokinetics Announces Start of REDWOOD-HCM, a Phase 2 Clinical Trial of CK-3773274 | Cytokinetics, Inc. Available online: https://ir.cytokinetics.com/news-releases/news-release-details/cytokinetics-announces-start-redwood-hcm-phase-2-clinical-trial (accessed on 16 January 2021).
- Cytokinetics Announces Progression of REDWOOD-HCM to Cohort 2 Nasdaq:CYTK. Available online: https://www.globenewswire.com/news-release/2020/12/09/2142115/0/en/Cytokinetics-Announces-Progression-of-REDWOOD-HCM-to-Cohort-2.html (accessed on 16 January 2021).
- Planelles-Herrero, V.J.; Hartman, J.J.; Robert-Paganin, J.; Malik, F.I.; Houdusse, A. Mechanistic and structural basis for activation of cardiac myosin force production by omecamtiv mecarbil. Nat. Commun. 2017, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Teerlink, J.R.; Clarke, C.P.; Saikali, K.G.; Lee, J.H.; Chen, M.M.; Escandon, R.D.; Elliott, L.; Bee, R.; Habibzadeh, M.R.; Goldman, J.H.; et al. Dose-dependent augmentation of cardiac systolic function with the selective cardiac myosin activator, omecamtiv mecarbil: A first-in-man study. Lancet 2011, 378, 667–675. [Google Scholar] [CrossRef]
- Teerlink, J.R.; Felker, G.M.; McMurray, J.J.V.; Solomon, S.D.; Adams, K.F.; Cleland, J.G.F.; Ezekowitz, J.A.; Goudev, A.; Macdonald, P.; Metra, M.; et al. Chronic Oral Study of Myosin Activation to Increase Contractility in Heart Failure (COSMIC-HF): A phase 2, pharmacokinetic, randomised, placebo-controlled trial. Lancet 2016, 388, 2895–2903. [Google Scholar] [CrossRef] [Green Version]
- Teerlink, J.R.; Diaz, R.; Felker, G.M.; McMurray, J.J.; Metra, M.; Solomon, S.D.; Adams, K.F.; Anand, I.; Arias-Mendoza, A.; Biering-Sørensen, T.; et al. Cardiac Myosin Activation with Omecamtiv Mecarbil in Systolic Heart Failure. N. Engl. J. Med. 2020, 384, 105–116. [Google Scholar] [CrossRef]
- Russell, A.J.; Hartman, J.J.; Hinken, A.C.; Muci, A.R.; Kawas, R.; Driscoll, L.; Godinez, G.; Lee, K.H.; Marquez, D.; Iv, W.F.B.; et al. Activation of fast skeletal muscle troponin as a potential therapeutic approach for treating neuromuscular diseases. Nat. Med. 2012, 18, 452–455. [Google Scholar] [CrossRef] [Green Version]
- Andrews, J.A.; Cudkowicz, M.E.; Hardiman, O.; Meng, L.; Bian, A.; Lee, J.; Wolff, A.A.; Malik, F.I.; Shefner, J.M. VITALITY-ALS, a phase III trial of tirasemtiv, a selective fast skeletal muscle troponin activator, as a potential treatment for patients with amyotrophic lateral sclerosis: Study design and baseline characteristics. Amyotroph. Later. Scler. Frontotempo. Degener. 2018, 19, 256–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, J.A.; Miller, T.M.; Vijayakumar, V.; Stoltz, R.; James, J.K.; Meng, L.; Wolff, A.A.; Malik, F.I. CK-2127107 amplifies skeletal muscle response to nerve activation in humans: CK-107 Effect on Muscle Force. Muscle Nerve 2017, 57, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Shefner, J.M.; Handiman, A.G.O.; Cudkowics, M.; Kupfer, S.; Malik, F.I.; Meng, L.; Wei, J.; Wolff, A.A.; Rudnicki, S. CLT-04: A Phase 3, Multi-Center, Double-Blind, Randomized, Placebo Controlled Trial to Evaluate the Efficacy and Safety of Reldesemtiv in Patients with Amyotrophic Lateral Sclerosis (ALS): COURAGE-ALS Trial Design. In Proceedings of the 31st International Symposium on ALS/MND, Basel, Switzerland, 9–11 December 2020. [Google Scholar]
- Redwood, D.R.; Goldstein, R.E.; Hirshfeld, J.; Borer, J.S.; Morganroth, J.; Morrow, A.G.; Epstein, S.E. Exercise performance after septal myotomy and myectomy in patients with obstructive hypertrophic cardiomyopathy. Am. J. Cardiol. 1979, 44, 215–220. [Google Scholar] [CrossRef]
- McCully, R.B.; Nishimura, R.A.; Tajik, A.J.; Schaff, H.V.; Danielson, G.K. Extent of Clinical Improvement After Surgical Treatment of Hypertrophic Obstructive Cardiomyopathy. Circulation 1996, 94, 467–471. [Google Scholar] [CrossRef]
- Ommen, S.R.; Maron, B.J.; Olivotto, I.; Maron, M.S.; Cecchi, F.; Betocchi, S.; Gersh, B.J.; Ackerman, M.J.; McCully, R.B.; Dearani, J.A.; et al. Long-Term Effects of Surgical Septal Myectomy on Survival in Patients With Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2005, 46, 470–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maron, B.J. Clinical Course and Management of Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2018, 379, 655–668. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Chaudhry, F.A.; Swistel, D.G. Obstructive hypertrophic cardiomyopathy: Echocardiography, pathophysiology, and the continuing evolution of surgery for obstruction. Ann. Thorac. Surg. 2003, 75, 620–632. [Google Scholar] [CrossRef]
- Ferrazzi, P.; Spirito, P.; Iacovoni, A.; Calabrese, A.; Migliorati, K.; Simon, C.; Pentiricci, S.; Poggio, D.; Grillo, M.; Amigoni, P.; et al. Transaortic Chordal Cutting. J. Am. Coll. Cardiol. 2015, 66, 1687–1696. [Google Scholar] [CrossRef] [Green Version]
- Nampiaparampil, R.G.; Swistel, D.G.; Schlame, M.; Saric, M.; Sherrid, M.V. Intraoperative Two- and Three-Dimensional Transesophageal Echocardiography in Combined Myectomy-Mitral Operations for Hypertrophic Cardiomyopathy. J. Am. Soc. Echocardiogr. 2018, 31, 275–288. [Google Scholar] [CrossRef]
- Musharbash, F.N.; Schill, M.R.; Hansalia, V.H.; Schuessler, R.B.; Leidenfrost, J.E.; Melby, S.J.; Damiano, R.J. Minimally Invasive versus Full-Sternotomy Septal Myectomy for Hypertrophic Cardiomyopathy. Innovations 2018, 13, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Boll, G.; Rowin, E.J.; Maron, B.J.; Wang, W.; Rastegar, H.; Maron, M.S. Efficacy of Combined Cox-Maze IV and Ventricular Septal Myectomy for Treatment of Atrial Fibrillation in Patients With Obstructive Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2020, 125, 120–126. [Google Scholar] [CrossRef]
- Cavigli, L.; Fumagalli, C.; Maurizi, N.; Rossi, A.; Arretini, A.; Targetti, M.; Passantino, S.; Girolami, F.; Tomberli, B.; Baldini, K.; et al. Timing of invasive septal reduction therapies and outcome of patients with obstructive hypertrophic cardiomyopathy. Int. J. Cardiol. 2018, 273, 155–161. [Google Scholar] [CrossRef]
- Alashi, A.; Smedira, N.G.; Hodges, K.; Popovic, Z.B.; Thamilarasan, M.; Wierup, P.; Lever, H.M.; Desai, M.Y. Outcomes in Guideline-Based Class I Indication Versus Earlier Referral for Surgical Myectomy in Hypertrophic Obstructive Cardiomyopathy. J. Am. Heart Assoc. 2021, 10, e016210. [Google Scholar] [CrossRef]
- Pasqualucci, D.; Fornaro, A.; Castelli, G.; Rossi, A.; Arretini, A.; Chiriatti, C.; Targetti, M.; Girolami, F.; Corda, M.; Orrù, P.; et al. Clinical Spectrum, Therapeutic Options, and Outcome of Advanced Heart Failure in Hypertrophic Cardiomyopathy. Circ. Heart Fail. 2015, 8, 1014–1021. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Magavern, E.; Sinagra, G.; Ashley, E.; Papadakis, M.; Tome-Esteban, M.; Sharma, S.; Olivotto, I. Impact of Demographic Features, Lifestyle, and Comorbidities on the Clinical Expression of Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2017, 6, e007161. [Google Scholar] [CrossRef] [Green Version]
- Sorajja, P.; Ommen, S.R.; Nishimura, R.A.; Gersh, B.J.; Berger, P.B.; Tajik, A.J. Adverse Prognosis of Patients With Hypertrophic Cardiomyopathy Who Have Epicardial Coronary Artery Disease. Circulation 2003, 108, 2342–2348. [Google Scholar] [CrossRef]
- Olivotto, I.; Maron, B.J.; Tomberli, B.; Appelbaum, E.; Salton, C.; Haas, T.S.; Gibson, C.M.; Nistri, S.; Servettini, E.; Chan, R.H.; et al. Obesity and its Association to Phenotype and Clinical Course in Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2013, 62, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Fumagalli, C.; Maurizi, N.; Day, S.M.; Ashley, E.A.; Michels, M.; Colan, S.D.; Jacoby, D.; Marchionni, N.; Vincent-Tompkins, J.; Ho, C.Y.; et al. Association of Obesity With Adverse Long-term Outcomes in Hypertrophic Cardiomyopathy. JAMA Cardiol. 2020, 5, 65–68. [Google Scholar] [CrossRef]
- Liebregts, M.; Vriesendorp, P.A.; Berg, J.M.T. Alcohol Septal Ablation for Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2017, 70, 481–488. [Google Scholar] [CrossRef]
- Liebregts, M.; Vriesendorp, P.A.; Mahmoodi, B.K.; Schinkel, A.F.; Michels, M.; Berg, J.M.T. A Systematic Review and Meta-Analysis of Long-Term Outcomes After Septal Reduction Therapy in Patients With Hypertrophic Cardiomyopathy. JACC Heart Fail. 2015, 3, 896–905. [Google Scholar] [CrossRef]
- Vriesendorp, P.A.; Liebregts, M.; Steggerda, R.C.; Schinkel, A.F.; Willems, R.; Cate, F.J.T.; Van Cleemput, J.; Berg, J.M.T.; Michels, M. Long-Term Outcomes After Medical and Invasive Treatment in Patients With Hypertrophic Cardiomyopathy. JACC Heart Fail. 2014, 2, 630–636. [Google Scholar] [CrossRef]
- Guerrero, I.; Dhoble, A.; Fasulo, M.; Denktas, A.E.; Sami, S.; Choi, S.; Balan, P.; Arain, S.A.; Smalling, R.W. Safety and efficacy of coil embolization of the septal perforator for septal ablation in patients with hypertrophic obstructive cardiomyopathy: Coil Embolization of the Septal Perforator in Patients with HOCM. Catheter. Cardiovasc. Interv. 2016, 88, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Galve, E.; Sambola, A.; Saldaña, G.; Quispe, I.; Nieto, E.; Diaz, A.; Evangelista, A.; Candell-Riera, J. Late benefits of dual-chamber pacing in obstructive hypertrophic cardiomyopathy: A 10-year follow-up study. Heart 2009, 96, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Lucon, A.; Palud, L.; Pavin, D.; Donal, E.; Behar, N.; Leclercq, C.; Mabo, P.; Daubert, J.-C. Very late effects of dual chamber pacing therapy for obstructive hypertrophic cardiomyopathy. Arch. Cardiovasc. Dis. 2013, 106, 373–381. [Google Scholar] [CrossRef]
- Román, A.J.; Cabezas, J.M.M.; Alonso, B.R.; Tejada, J.G.; Hernández, F.H.; González-Trevilla, A.A.; Martín, M.T.V.; Samartín, R.C.; García, J.R.; Pérez, J.C.T. Sequential Atrioventricular Pacing in Patients With Hypertrophic Cardiomyopathy: An 18-year Experience. Revista Española de Cardiología 2016, 69, 377–383. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef] [PubMed]
- Sorajja, P.; Pedersen, W.A.; Bae, R.; Lesser, J.R.; Jay, D.; Lin, D.; Harris, K.; Maron, B.J. First Experience With Percutaneous Mitral Valve Plication as Primary Therapy for Symptomatic Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 2811–2818. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.M.; Gimeno, J.R.; Tomé, M.T.; Shah, J.; Ward, D.; Thaman, R.; Mogensen, J.; McKenna, W.J. Left ventricular outflow tract obstruction and sudden death risk in patients with hypertrophic cardiomyopathy. Eur. Heart J. 2006, 27, 1933–1941. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, C.; Jichi, F.; Pavlou, M.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Gimeno, J.R.; Limongelli, G.; McKenna, W.J.; et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM Risk-SCD). Eur. Heart J. 2013, 35, 2010–2020. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Alfieri, O.; Calabrò, P.; Cecchi, F.; Ferrazzi, P.; Gragnano, F.; Kaski, J.P.; Limongelli, G.; Maron, M.; Rapezzi, C.; et al. Multidisciplinary evaluation and management of obstructive hypertrophic cardiomyopathy in 2020: Towards the HCM Heart Team. Int. J. Cardiol. 2020, 304, 86–92. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Name and Status | Molecule | Study | Population | Primary Endpoints | Secondary Endpoints |
|---|---|---|---|---|---|
| PIONEER-HCM Status: completed | Mavacamten MyoKardia, Inc. | Multi-center phase II open-label non-randomized 2 sequential cohorts (A and B) 12-weeks treatment phase followed by a 4-weeks post-treatment phase | 21 oHCM patients Cohort A: 56y Cohort B: 58y 57% men 57% NYHA II 43% NYHA III | Cohort A: mean post-exercise LVOT gradient decreased from 103 ± 50 mmHg to 19 ± 13 mmHg at 12 weeks (p = 0.008) Cohort B: mean LVOT gradient decreased from 86 ± 43 mmHg to 64 ± 26 mmHg (p = 0.020) | Cohort A: Resting LVEF reduction −15% (CI, −23% to −6%). Peak VO2 increased by a mean of 3.5 mL/kg/min (CI, 1.2 to 5.9 mL/kg/min). Cohort B: mean change in resting LVEF −6% (CI, −10% to −1%). Peak VO2 increased by a mean of 1.7 mL/kg/min (CI, 0.03 to 3.3 mL/kg/min). Dyspnea scores improved in both cohorts. |
| EXPLORER-HCM Status: completed | Mavacamten MyoKardia, Inc. | Multi-center phase III randomised double-blind placebo-controlled | 251 oHCM, Mean age 58 ± 11 years, 59% men | ≥1.5 mL/kg/min increase in pVO2 with ≥1 NYHA class improvement OR ≥ 3.0 mL/kg/min increase in pVO2 with no worsening of NYHA class in 37% of pt in MG vs. 17% in PG (p <0.0005) | Post-exercise LVOT gradient −47 mmHg in MG vs. −10 mmHg in PG (p < 0.0001) pVO2 +1.4 mL/kg/min in MG vs. −0.05 mL/kg/min in PG (p < 0.0006) ≥ NYHA class improvement 65% pt in MG vs. 31% pt in PG (p < 0.0001) KCCQ-CSS (n): +14 in MG vs. +4 in PG (p < 0.0001) HCMSQ-SoB (n) (negative better): −2.8 in MG vs. −0.9 in PG (p < 0.0001) |
| MAVERICK-HCM Status: completed | Mavacamten MyoKardia, Inc. | Multi-center phase II randomized double-blind placebo-controlled | 59 non-oHCM, mean age 54 ± 14 y, 58% women | Serious adverse events occurred in 10% pt in MG and in 21% of pt in PG 5 pt in MG had reversible reduction in LVEF ≤45%. | NTproBNP decreased by 53% in the MG vs. 1% in the PG, (p = 0.0005). Troponin I decreased by 34% in the MG vs. a 4% increase in the PG, (p = 0.009). |
| VALOR-HCM Status: on-going | Mavacamten MyoKardia, Inc. | Multi-center phase III randomized double-blind placebo-controlled | oHCM | Number of subjects who proceed or remain guideline eligible for SRT within week 16 | Number of subjects who proceed or remain guideline eligible for SRT within week 32; change from baseline to week 16 in NYHA, KCCQ-CSS, NTproBNP, troponin, LVOT gradient |
| MAVA-LTE Status: ongoing | Mavacamten MyoKardia, Inc. | Multi-center phase III randomized | A Long-Term Safety Extension Study of Mavacamten in who have completed the MAVERICK-HCM or EXPLORER-HCM Trials | Frequency and severity of treatment-emergent adverse events and serious adverse events | |
| REDWOOD-HCM Status: ongoing | CK-274 Cytokinetics Inc. | Multi-center phase II randomized double-blind placebo-controlled | oHCM | Safety and tolerability | Concentration-response and dose-response on the resting and post-Valsalva LVOT gradient; effect on NTproBNP and NYHA. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argirò, A.; Zampieri, M.; Berteotti, M.; Marchi, A.; Tassetti, L.; Zocchi, C.; Iannone, L.; Bacchi, B.; Cappelli, F.; Stefàno, P.; et al. Emerging Medical Treatment for Hypertrophic Cardiomyopathy. J. Clin. Med. 2021, 10, 951. https://doi.org/10.3390/jcm10050951
Argirò A, Zampieri M, Berteotti M, Marchi A, Tassetti L, Zocchi C, Iannone L, Bacchi B, Cappelli F, Stefàno P, et al. Emerging Medical Treatment for Hypertrophic Cardiomyopathy. Journal of Clinical Medicine. 2021; 10(5):951. https://doi.org/10.3390/jcm10050951
Chicago/Turabian StyleArgirò, Alessia, Mattia Zampieri, Martina Berteotti, Alberto Marchi, Luigi Tassetti, Chiara Zocchi, Luisa Iannone, Beatrice Bacchi, Francesco Cappelli, Pierluigi Stefàno, and et al. 2021. "Emerging Medical Treatment for Hypertrophic Cardiomyopathy" Journal of Clinical Medicine 10, no. 5: 951. https://doi.org/10.3390/jcm10050951
APA StyleArgirò, A., Zampieri, M., Berteotti, M., Marchi, A., Tassetti, L., Zocchi, C., Iannone, L., Bacchi, B., Cappelli, F., Stefàno, P., Marchionni, N., & Olivotto, I. (2021). Emerging Medical Treatment for Hypertrophic Cardiomyopathy. Journal of Clinical Medicine, 10(5), 951. https://doi.org/10.3390/jcm10050951