
Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection and Score Calculation
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Survival Results and Survival-Related Variables
3.3. Performance of the ENCOURAGE Score in Predicting the 30-Day Survival
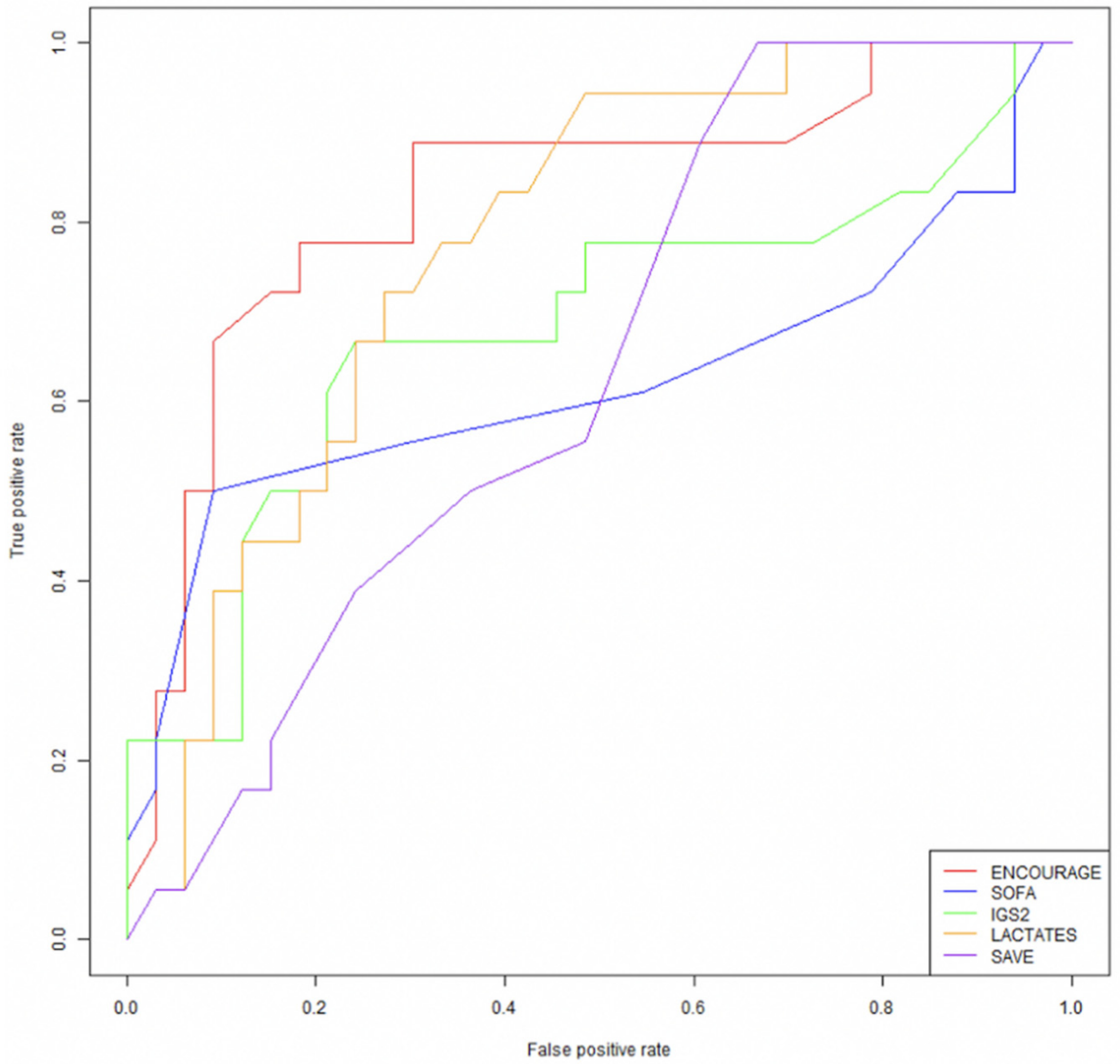
3.4. Comparison of the ENCOURAGE Score with Other Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.; Lim, S.-H.; Hong, J.; Hong, Y.-S.; Lee, C.J.; Jung, J.-H.; Yu, S. Efficacy of Veno-Arterial Extracorporeal Membrane Oxygenation in Acute Myocardial Infarction with Cardiogenic Shock. Resuscitation 2012, 83, 971–975. [Google Scholar] [CrossRef]
- Sheu, J.-J.; Tsai, T.-H.; Lee, F.-Y.; Fang, H.-Y.; Sun, C.-K.; Leu, S.; Yang, C.-H.; Chen, S.-M.; Hang, C.-L.; Hsieh, Y.-K.; et al. Early Extracorporeal Membrane Oxygenator-Assisted Primary Percutaneous Coronary Intervention Improved 30-Day Clinical Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Complicated with Profound Cardiogenic Shock. Crit. Care Med. 2010, 38, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of Cardiogenic Shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.-P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Jüni, P.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization. Kardiol. Pol. 2014, 72, 1253–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care: Endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention. J. Am. Coll. Cardiol. 2015, 65, e7–e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, B.; Bastien, O.; Karim, B.; Benjelid, K.; Cariou, A.; Chouihed, T.; Combes, A.; Mebazaa, A.; Megarbane, B.; Plaisance, P.; et al. Experts’ Recommendations for the Management of Adult Patients with Cardiogenic Shock. Ann. Intensive Care 2015, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal Membrane Oxygenation in Cardiopulmonary Disease in Adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef] [Green Version]
- Sleeper, L.A.; Reynolds, H.R.; White, H.D.; Webb, J.G.; Džavík, V.; Hochman, J.S. A severity scoring system for risk assessment of patients with cardiogenic shock: a report from the shock trial and registry. Am. Heart J. 2010, 160, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Dzavik, V.; Buller, C.E.; Aylward, P.; Col, J.; White, H.D. Early Revascularization Improves Long-Term Survival for Cardiogenic Shock Complicating Acute Myocardial Infarction. JAMA 2006, 295, 2511–2515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babaev, A.; Frederick, P.D.; Pasta, D.J.; Every, N.; Sichrovsky, T.; Hochman, J.S. NRMI Investigators Trends in Management and Outcomes of Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2005, 294, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonello, L.; Delmas, C.; Schurtz, G.; Leurent, G.; Bonnefoy, E.; Aissaoui, N.; Henry, P. Mechanical Circulatory Support in Patients with Cardiogenic Shock in Intensive Care Units: A Position Paper of the “Unité de Soins Intensifs de Cardiologie” Group of the French Society of Cardiology, Endorsed by the “Groupe Athérome et Cardiologie Interventionnelle” of the French Society of Cardiology. Arch. Cardiovasc. Dis. 2018, 111, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Demondion, P.; Fournel, L.; Golmard, J.-L.; Niculescu, M.; Pavie, A.; Leprince, P. Predictors of 30-Day Mortality and Outcome in Cases of Myocardial Infarction with Cardiogenic Shock Treated by Extracorporeal Life Support. Eur. J. Cardiothoracic Surg. 2014, 45, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combes, A.; Leprince, P.; Luyt, C.-E.; Bonnet, N.; Trouillet, J.-L.; Léger, P.; Pavie, A.; Chastre, J. Outcomes and Long-Term Quality-of-Life of Patients Supported by Extracorporeal Membrane Oxygenation for Refractory Cardiogenic Shock. Crit. Care Med. 2008, 36, 1404–1411. [Google Scholar] [CrossRef]
- Schmidt, M.; Burrell, A.; Roberts, L.; Bailey, M.; Sheldrake, J.; Rycus, P.T.; Hodgson, C.; Scheinkestel, C.; Cooper, D.J.; Thiagarajan, R.R.; et al. Predicting Survival after ECMO for Refractory Cardiogenic Shock: The Survival after Veno-Arterial-ECMO (SAVE)-Score. Eur. Heart J. 2015, 36, 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- Worku, B.; Gaudino, M.; Avgerinos, D.; Ramasubbu, K.; Gambardella, I.; Gulkarov, I.; Khin, S. A Comparison of Existing Risk Prediction Models in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation. Heart Lung 2020, 49, 599–604. [Google Scholar] [CrossRef]
- Muller, G.; Flecher, E.; Lebreton, G.; Luyt, C.-E.; Trouillet, J.-L.; Bréchot, N.; Schmidt, M.; Mastroianni, C.; Chastre, J.; Leprince, P.; et al. The ENCOURAGE Mortality Risk Score and Analysis of Long-Term Outcomes after VA-ECMO for Acute Myocardial Infarction with Cardiogenic Shock. Intensive Care Med. 2016, 42, 370–378. [Google Scholar] [CrossRef]
- Pabst, D.; Foy, A.J.; Peterson, B.; Soleimani, B.; Brehm, C.E. Predicting Survival in Patients Treated With Extracorporeal Membrane Oxygenation After Myocardial Infarction. Crit. Care Med. 2018, 46, e359–e363. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014; ISBN 3-900051-07-0. [Google Scholar]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Vallabhajosyula, S.; Prasad, A.; Bell, M.R.; Sandhu, G.S.; Eleid, M.F.; Dunlay, S.M.; Schears, G.J.; Stulak, J.M.; Singh, M.; Gersh, B.J.; et al. Extracorporeal Membrane Oxygenation Use in Acute Myocardial Infarction in the United States, 2000 to 2014. Circ. Heart Fail. 2019, 12, e005929. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; de Waha, A.; Richardt, G.; Hennersdorf, M.; Empen, K.; et al. Intra-Aortic Balloon Counterpulsation in Acute Myocardial Infarction Complicated by Cardiogenic Shock (IABP-SHOCK II): Final 12 Month Results of a Randomised, Open-Label Trial. Lancet 2013, 382, 1638–1645. [Google Scholar] [CrossRef]
- Ostenfeld, S.; Lindholm, M.G.; Kjaergaard, J.; Bro-Jeppesen, J.; Møller, J.E.; Wanscher, M.; Hassager, C. Prognostic Implication of Out-of-Hospital Cardiac Arrest in Patients with Cardiogenic Shock and Acute Myocardial Infarction. Resuscitation 2015, 87, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of Extracorporeal Membrane Oxygenation for Treatment of Cardiogenic Shock and Cardiac Arrest: A Meta-Analysis of 1,866 Adult Patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in Collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Danziger-Isakov, L.; Kirklin, J.K.; Kirk, R.; Kushwaha, S.S.; et al. The 2016 International Society for Heart Lung Transplantation Listing Criteria for Heart Transplantation: A 10-Year Update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Schoenrath, F.; Hoch, D.; Maisano, F.; Starck, C.T.; Seifert, B.; Wenger, U.; Ruschitzka, F.; Wilhelm, M.J. Survival, Quality of Life and Impact of Right Heart Failure in Patients with Acute Cardiogenic Shock Treated with ECMO. Heart Lung 2016, 45, 409–415. [Google Scholar] [CrossRef]
- Jessup, M.; Drazner, M.H.; Book, W.; Cleveland, J.C.; Dauber, I.; Farkas, S.; Ginwalla, M.; Katz, J.N.; Kirkwood, P.; Kittleson, M.M.; et al. 2017 ACC/AHA/HFSA/ISHLT/ACP Advanced Training Statement on Advanced Heart Failure and Transplant Cardiology (Revision of the ACCF/AHA/ACP/HFSA/ISHLT 2010 Clinical Competence Statement on Management of Patients With Advanced Heart Failure and Cardiac Transplant): A Report of the ACC Competency Management Committee. J. Am. Coll. Cardiol. 2017, 69, 2977–3001. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Ramzy, D.; Azarbal, B.; Arabia, F.A.; Esmailian, F.; Czer, L.S.; Kobashigawa, J.A.; Moriguchi, J.D. Device Strategies for Patients in INTERMACS Profiles 1 and 2 Cardiogenic Shock: Double Bridge With Extracorporeal Membrane Oxygenation and Initial Implant of More Durable Devices. Artif. Organs 2017, 41, 224–232. [Google Scholar] [CrossRef]
- Stretch, R.; Sauer, C.M.; Yuh, D.D.; Bonde, P. National Trends in the Utilization of Short-Term Mechanical Circulatory Support: Incidence, Outcomes, and Cost Analysis. J. Am. Coll. Cardiol. 2014, 64, 1407–1415. [Google Scholar] [CrossRef] [Green Version]
- Ouweneel, D.M.; Schotborgh, J.V.; Limpens, J.; Sjauw, K.D.; Engström, A.E.; Lagrand, W.K.; Cherpanath, T.G.V.; Driessen, A.H.G.; de Mol, B.A.J.M.; Henriques, J.P.S. Extracorporeal Life Support during Cardiac Arrest and Cardiogenic Shock: A Systematic Review and Meta-Analysis. Intensive Care Med. 2016, 42, 1922–1934. [Google Scholar] [CrossRef] [Green Version]
- Karami, M.; den Uil, C.A.; Ouweneel, D.M.; Scholte, N.T.; Engström, A.E.; Akin, S.; Lagrand, W.K.; Vlaar, A.P.; Jewbali, L.S.; Henriques, J.P. Mechanical Circulatory Support in Cardiogenic Shock from Acute Myocardial Infarction: Impella CP/5.0 versus ECMO. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Vdovin, N.; Günther, S.P.W.; de Waha, S.; Seizer, P.; Brunner, S.; Schlensak, C.; Thiele, H.; Hagl, C.; Massberg, S.; Bauer, A. Early Risk Stratification in Patients With Cardiogenic Shock Complicating Acute Myocardial Infarction Treated With Extracorporeal Life Support and Primary Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2017, 10, 2469–2471. [Google Scholar] [CrossRef]
- Brunner, S.; Guenther, S.P.W.; Lackermair, K.; Peterss, S.; Orban, M.; Boulesteix, A.-L.; Michel, S.; Hausleiter, J.; Massberg, S.; Hagl, C. Extracorporeal Life Support in Cardiogenic Shock Complicating Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 2355–2357. [Google Scholar] [CrossRef] [PubMed]
- Russo, J.J.; Aleksova, N.; Pitcher, I.; Couture, E.; Parlow, S.; Faraz, M.; Visintini, S.; Simard, T.; Di Santo, P.; Mathew, R.; et al. Left Ventricular Unloading During Extracorporeal Membrane Oxygenation in Patients With Cardiogenic Shock. J. Am. Coll. Cardiol. 2019, 73, 654–662. [Google Scholar] [CrossRef]
- Petroni, T.; Harrois, A.; Amour, J.; Lebreton, G.; Brechot, N.; Tanaka, S.; Luyt, C.-E.; Trouillet, J.-L.; Chastre, J.; Leprince, P.; et al. Intra-Aortic Balloon Pump Effects on Macrocirculation and Microcirculation in Cardiogenic Shock Patients Supported by Venoarterial Extracorporeal Membrane Oxygenation*. Crit. Care Med. 2014, 42, 2075–2082. [Google Scholar] [CrossRef] [PubMed]
- Aso, S.; Matsui, H.; Fushimi, K.; Yasunaga, H. The Effect of Intraaortic Balloon Pumping Under Venoarterial Extracorporeal Membrane Oxygenation on Mortality of Cardiogenic Patients: An Analysis Using a Nationwide Inpatient Database. Crit. Care Med. 2016, 44, 1974–1979. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Vogt, A.; Zahn, R.; Weber, M.A.; Tebbe, U.; Gottwik, M.; Bonzel, T.; Senges, J.; Neuhaus, K.-L.; Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte (ALKK). Predictors of In-Hospital Mortality in 1333 Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock Treated with Primary Percutaneous Coronary Intervention (PCI); Results of the Primary PCI Registry of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte (ALKK). Eur. Heart J. 2004, 25, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Klein, L.W.; Shaw, R.E.; Krone, R.J.; Brindis, R.G.; Anderson, H.V.; Block, P.C.; McKay, C.R.; Hewitt, K.; Weintraub, W.S.; American College of Cardiology National Cardiovascular Data Registry. Mortality after Emergent Percutaneous Coronary Intervention in Cardiogenic Shock Secondary to Acute Myocardial Infarction and Usefulness of a Mortality Prediction Model. Am. J. Cardiol. 2005, 96, 35–41. [Google Scholar] [CrossRef]
- Chung, M.; Zhao, Y.; Strom, J.B.; Shen, C.; Yeh, R.W. Extracorporeal Membrane Oxygenation Use in Cardiogenic Shock: Impact of Age on In-Hospital Mortality, Length of Stay, and Costs. Crit. Care Med. 2019, 47, e214–e221. [Google Scholar] [CrossRef]
- Lee, W.-C.; Fang, C.-Y.; Chen, H.-C.; Chen, C.-J.; Yang, C.-H.; Hang, C.-L.; Yip, H.-K.; Fang, H.-Y.; Wu, C.-J. Associations with 30-Day Survival Following Extracorporeal Membrane Oxygenation in Patients with Acute ST Segment Elevation Myocardial Infarction and Profound Cardiogenic Shock. Heart Lung 2016, 45, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.-Y.; Tong, M.-S.; Sheu, J.-J.; Lee, F.-Y.; Sung, P.-H.; Chen, C.-J.; Yang, C.-H.; Wu, C.-J.; Yip, H.-K. Short-Term and Long-Term Prognostic Outcomes of Patients with ST-Segment Elevation Myocardial Infarction Complicated by Profound Cardiogenic Shock Undergoing Early Extracorporeal Membrane Oxygenator-Assisted Primary Percutaneous Coronary Intervention. Int. J. Cardiol. 2016, 223, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Werdan, K.; Gielen, S.; Ebelt, H.; Hochman, J.S. Mechanical Circulatory Support in Cardiogenic Shock. Eur. Heart J. 2014, 35, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 51) | Survivors (n = 32) | Non-Survivors (n = 19) | p-Value |
|---|---|---|---|---|
| Age (years) | 53 (47–58) | 52 (42–57) | 54 (51–64) | 0.14 |
| Male Gender | 41 (80) | 27 (84) | 14 (73) | 0.35 |
| BMI (kg/m2) | 26 (23–28) | 25 (22–28) | 27 (25–29) | 0.17 |
| CV Risk Factors | ||||
| Smoking habits | 35 (69) | 22 (69) | 13 (68) | 0.98 |
| Dyslipidemia | 12 (23) | 7 (21) | 5 (26) | 0.72 |
| Arterial Hypertension | 21 (41) | 15 (47) | 6 (32) | 0.28 |
| Diabetes mellitus | 11 (22) | 7 (22) | 4 (21) | 0.94 |
| Family history of CHD | 6 (12) | 2 (6) | 4 (21) | 0.11 |
| Vascular History | ||||
| Previous coronary angioplasty or CABG | 3 (6) | 1 (3) | 2 (11) | 0.28 |
| Peripheral artery disease | 3 (6) | 1 (3) | 2 (11) | 0.28 |
| SOFA Score | 9 (8–10) | 9 (8–10) | 11 (7–12) | 0.09 |
| SAPS II Score | 38 (29–44) | 33 (29–40) | 44 (35–67) | 0.02 |
| STEMI-ECMO Period (days) | 1 (0–4) | 1 (0–7) | 0 (0–3) | 0.36 |
| Pre-ECMO Cardiac Arrest | 17 (33) | 9 (28) | 8 (42) | 0.31 |
| No Flow duration (min) | 0 (0–0) | 0 (0–0) | 0 (0–10) | |
| Low Flow duration (min) | 20 (12–45) | 10 (12–20) | 30 (20–40) | |
| Shockable Rhythm | 12/17 (71) | 8/9 (89) | 4/8 (50) | |
| ECMO under CPR | 6 (12) | 1 (3) | 5 (26) | 0.01 |
| Intravenous fibrinolysis | 3 (6) | 3 (10) | 0 | 0.17 |
| Anterior STEMI | 39 (76) | 24 (75) | 15 (79) | 0.75 |
| Primary Angioplasty | 47 (92) | 29 (90) | 18 (95) | 0.60 |
| Successful PA | 41/47 (87) | 26/29 (90) | 15/18 (83) | |
| Post-PA ECMO | 50 (98) | 31 (96) | 19 (100) | 0.43 |
| Time from PA to ECMO (h) | 7 (0–84) | 8 (0–114) | 2 (0–52) | 0.49 |
| Percutaneous ECMO implantation | 23 (45) | 13 (57) | 10 (43) | 0.56 |
| Distal perfusion cannulation | 51 (100) | 32 (100) | 19 (100) | |
| ECMO-related IABP | 46 (90) | 30 (94) | 16 (84) | 0.27 |
| Pre-ECMO IABP | 27 (53) | 20 (62) | 7 (37) | 0.08 |
| Pre-ECMO MV | 51 (100) | 32 (100) | 19 (100) | |
| Glasgow Coma Scale score | 14 (3–14) | 14 (14–14) | 3 (3–14) | 0.03 |
| Arterial Lactate (mmol/L) | 3.1 (1.9–7.3) | 2.2 (1.5–3.7) | 6.5 (3.2–13.3) | <0.01 |
| Prothrombin ratio (%) | 55 (45–66) | 55 (53–70) | 45 (36–55) | <0.01 |
| Serum Creatinine (µmol/L) | 122 (100–170) | 115 (93–176) | 149 (115–167) | 0.52 |
| Arterial pH | 7.32 (7.29–7.43) | 7.32 (7.31–7.43) | 7.32 (7.19–7.44) | 0.08 |
| Variables | All Patients (n = 51) | Survivors (n = 32) | Non-Survivors (n = 19) | p-Value |
|---|---|---|---|---|
| ECMO Duration (days) | 7 (4–14) | 7 (5–12) | 6 (2–15) | 0.54 |
| Hospital Stay (days) | 27 (12–40) | 34 (28–54) | 7 (2–17) | <0.01 |
| Weaned off ECMO/recovery | 17 (33) | 16 (50) | 1 (5) | <0.01 |
| LVAD Assist | 7 (13) | 5 (16) | 2 (11) | 0.61 |
| Heart transplant | 11 (22) | 11 (34) | 0 | <0.01 |
| BARC III bleeding event | 17 (33) | 8 (25) | 9 (47) | 0.10 |
| Acute Limb Ischemia | 8 (16) | 3 (9) | 5 (26) | 0.11 |
| Scarpa Infection | 5 (10) | 4 (13) | 1 (5) | 0.40 |
| Acute Pulmonary Edema | 16 (31) | 7 (22) | 9 (47) | 0.06 |
| Renal replacement therapy | 12 (23) | 4 (12) | 8 (42) | 0.01 |
| Left ventricle thrombus | 6 (12) | 0 (0) | 6 (32) | <0.01 |
| Harlequin syndrome | 4 (8) | 0 (0) | 4 (21) | 0.02 |
| Switch from peripheral to Central ECMO | 2 (4) | 0 | 2 (10) | 0.04 |
| Massive Hemolysis | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semaan, C.; Charbonnier, A.; Pasco, J.; Darwiche, W.; Saint Etienne, C.; Bailleul, X.; Bourguignon, T.; Fauchier, L.; Angoulvant, D.; Ivanes, F.; et al. Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation. J. Clin. Med. 2021, 10, 956. https://doi.org/10.3390/jcm10050956
Semaan C, Charbonnier A, Pasco J, Darwiche W, Saint Etienne C, Bailleul X, Bourguignon T, Fauchier L, Angoulvant D, Ivanes F, et al. Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation. Journal of Clinical Medicine. 2021; 10(5):956. https://doi.org/10.3390/jcm10050956
Chicago/Turabian StyleSemaan, Carl, Arthur Charbonnier, Jeremy Pasco, Walid Darwiche, Christophe Saint Etienne, Xavier Bailleul, Thierry Bourguignon, Laurent Fauchier, Denis Angoulvant, Fabrice Ivanes, and et al. 2021. "Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation" Journal of Clinical Medicine 10, no. 5: 956. https://doi.org/10.3390/jcm10050956
APA StyleSemaan, C., Charbonnier, A., Pasco, J., Darwiche, W., Saint Etienne, C., Bailleul, X., Bourguignon, T., Fauchier, L., Angoulvant, D., Ivanes, F., & Genet, T. (2021). Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation. Journal of Clinical Medicine, 10(5), 956. https://doi.org/10.3390/jcm10050956