
PCSK9 Levels and Metabolic Profiles in Elderly Subjects with Different Glucose Tolerance under Statin Therapy

 ,
, 
Abstract
:1. Introduction
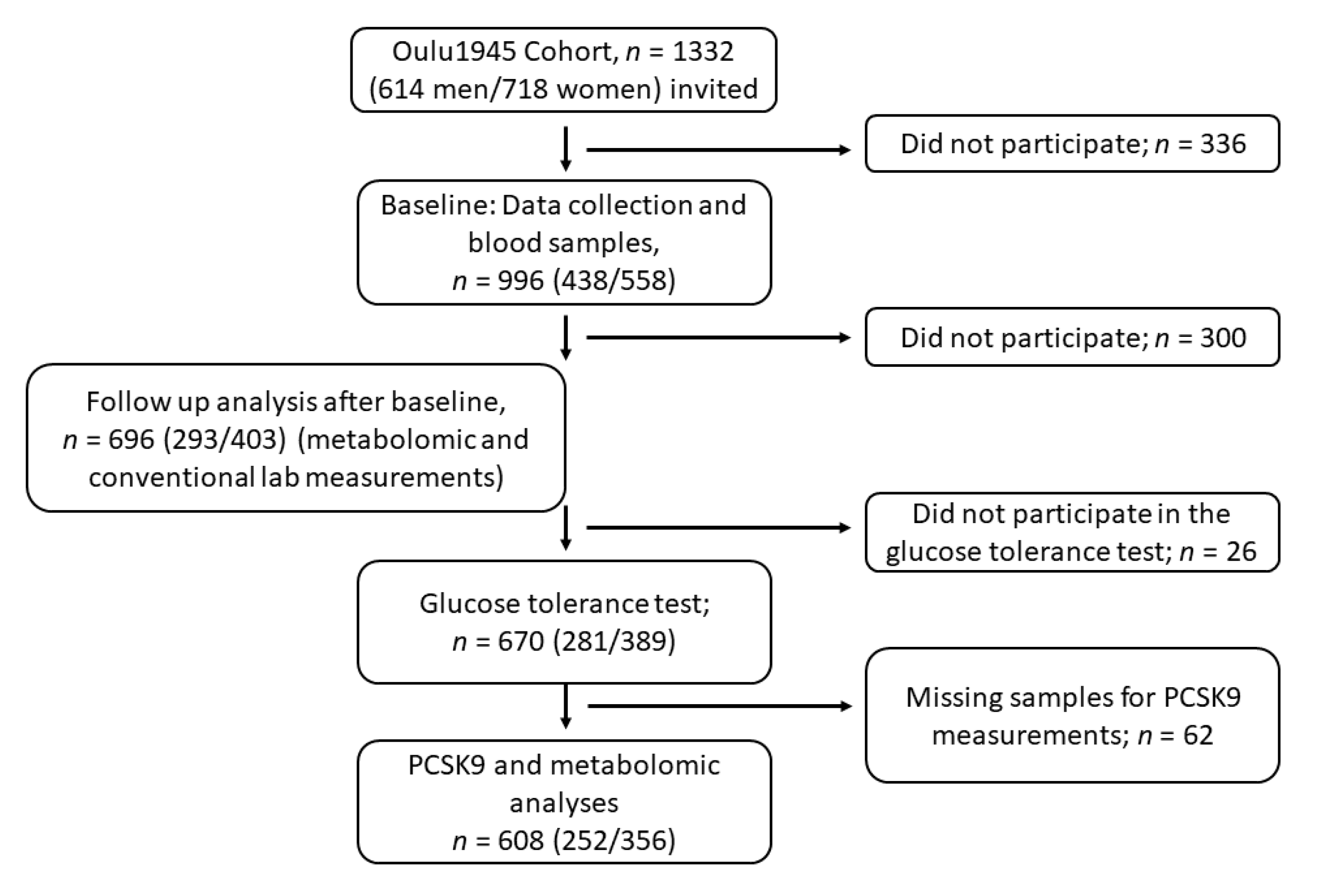
2. Materials and Methods
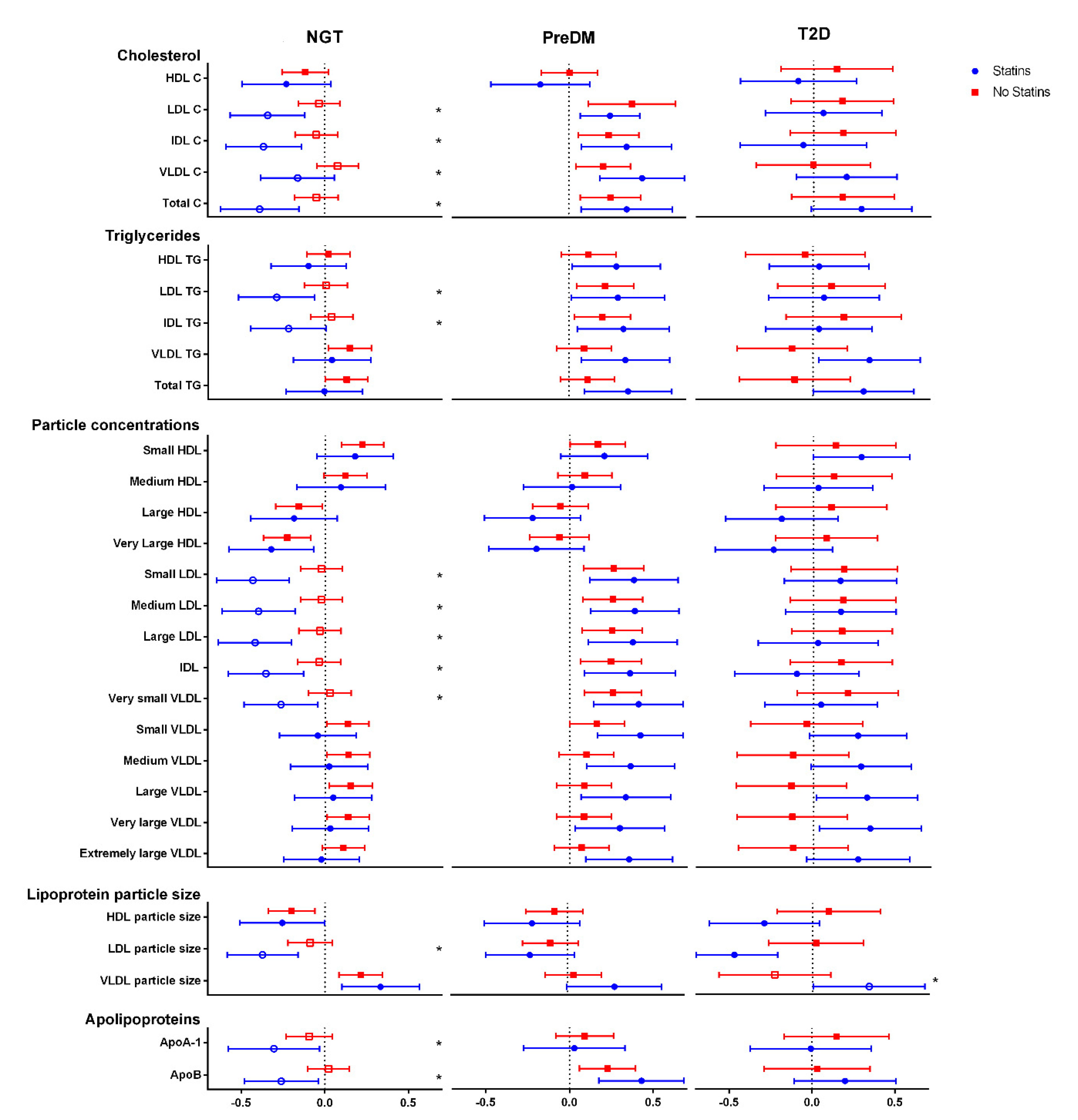
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seidah, N.G.; Awan, Z.; Chrétien, M.; Mbikay, M. PCSK9. Circ. Res. 2014, 114, 1022–1036. [Google Scholar] [CrossRef]
- Abifadel, M.; Varret, M.; Rabès, J.-P.; Allard, D.; Ouguerram, K.; Devillers, M.; Cruaud, C.; Benjannet, S.; Wickham, L.; Erlich, D.; et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat. Genet. 2003, 34, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Cesaro, A.; Bianconi, V.; Gragnano, F.; Moscarella, E.; Fimiani, F.; Monda, E.; Scudiero, O.; Limongelli, G.; Pirro, M.; Calabrò, P. Beyond cholesterol metabolism: The pleiotropic effects of proprotein convertase subtilisin/kexin type 9 (PCSK9). Genetics, mutations, expression, and perspective for long-term inhibition. BioFactors 2020, 46, 367–380. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Pertsemlidis, A.; Kotowski, I.K.; Graham, R.; Garcia, C.K.; Hobbs, H.H. Low LDL cholesterol in individuals of African descent resulting from frequent nonsense mutations in PCSK9. Nat. Genet. 2005, 37, 161–165. [Google Scholar] [CrossRef] [PubMed]
- A Duprez, D.; Handelsman, Y.; Koren, M. Cardiovascular Outcomes and Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors: Current Data and Future Prospects. Vasc. Heal. Risk Manag. 2020, 16, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Momtazi, A.A.; Banach, M.; Pirro, M.; Stein, E.A.; Sahebkar, A. PCSK9 and diabetes: Is there a link? Drug Discov. Today 2017, 22, 883–895. [Google Scholar] [CrossRef]
- Lakoski, S.G.; Lagace, T.A.; Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Genetic and Metabolic Determinants of Plasma PCSK9 Levels. J. Clin. Endocrinol. Metab. 2009, 94, 2537–2543. [Google Scholar] [CrossRef] [PubMed]
- Nekaies, Y.; Baudin, B.; Kelbousi, S.; Sakly, M.; Attia, N. Plasma proprotein convertase subtilisin/kexin type 9 is associated with Lp(a) in type 2 diabetic patients. J. Diabetes Its Complicat. 2015, 29, 1165–1170. [Google Scholar] [CrossRef]
- Victor, R.G.; Haley, R.W.; Willett, D.L.; Peshock, R.M.; Vaeth, P.C.; Leonard, D.; Basit, M.; Cooper, R.S.; Iannacchione, V.G.; A Visscher, W.; et al. The Dallas Heart Study: A population-based probability sample for the multidisciplinary study of ethnic differences in cardiovascular health. Am. J. Cardiol. 2004, 93, 1473–1480. [Google Scholar] [CrossRef]
- Vergès, B.; Duvillard, L.; Brindisi, M.C.; Gautier, E.; Krempf, M.; Costet, P.; Cariou, B. Lack of association between plasma PCSK9 and LDL-apoB100 catabolism in patients with uncontrolled type 2 diabetes. Atherosclerosis 2011, 219, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.; Troutt, J.; van Greevenbroek, M.; Ferreira, I.; Feskens, E.; van der Kallen, C.; Schaper, N.; Schalkwijk, C.; Konrad, R.; Stehouwer, C. Plasma proprotein convertase subtilisin kexin type 9 is not altered in subjects with impaired glucose metabolism and type 2 diabetes mellitus, but its relationship with non-HDL cholesterol and apolipoprotein B may be modified by type 2 diabetes mellitus: The CODAM study. Atherosclerosis 2011, 217, 263–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2013, 37, S81–S90. [CrossRef] [Green Version]
- Bansal, N. Prediabetes diagnosis and treatment: A review. World J. Diabetes 2015, 6, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Ibarretxe, D.; Girona, J.; Plana, N.; Cabré, A.; Ferré, R.; Amigó, N.; Guaita, S.; Mallol, R.; Heras, M.; Masana, L. Circulating PCSK9 in patients with type 2 diabetes and related metabolic disorders. Clínica Investig. Arterioscler. 2016, 28, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Colhoun, H.M.; Ginsberg, H.N.; Robinson, J.G.; Leiter, L.A.; Müller-Wieland, D.; Henry, R.R.; Cariou, B.; Baccara-Dinet, M.T.; Pordy, R.; Merlet, L.; et al. No effect of PCSK9 inhibitor alirocumab on the incidence of diabetes in a pooled analysis from 10 ODYSSEY Phase 3 studies. Eur. Hear. J. 2016, 37, 2981–2989. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, L.S.F.; Campos, A.M.; Sposito, A.C. Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitors and Incident Type 2 Diabetes: A Systematic Review and Meta-analysis with over 96,000 Patient-Years. Diabetes Care 2017, 41, 364–367. [Google Scholar] [CrossRef] [Green Version]
- Ferri, N.; Tibolla, G.; Pirillo, A.; Cipollone, F.; Mezzetti, A.; Pacia, S.; Corsini, A.; Catapano, A.L. Proprotein convertase subtilisin kexin type 9 (PCSK9) secreted by cultured smooth muscle cells reduces macrophages LDLR levels. Atherosclerosis 2012, 220, 381–386. [Google Scholar] [CrossRef]
- Cicero, A.; Toth, P.; Fogacci, F.; Virdis, A.; Borghi, C. Improvement in arterial stiffness after short-term treatment with PCSK9 inhibitors. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 527–529. [Google Scholar] [CrossRef]
- Gencer, B.; Montecucco, F.; Nanchen, D.; Carbone, F.; Klingenberg, R.; Vuilleumier, N.; Aghlmandi, S.; Heg, D.; Räber, L.; Auer, R.; et al. Prognostic value of PCSK9 levels in patients with acute coronary syndromes. Eur. Hear. J. 2016, 37, 546–553. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhu, C.-G.; Xu, R.-X.; Li, S.; Guo, Y.-L.; Sun, J.; Li, J.-J. Relation of circulating PCSK9 concentration to fibrinogen in patients with stable coronary artery disease. J. Clin. Lipidol. 2014, 8, 494–500. [Google Scholar] [CrossRef]
- Dubuc, G.; Chamberland, A.; Wassef, H.; Davignon, J.; Seidah, N.G.; Bernier, L.; Prat, A. Statins UpregulatePCSK9, the Gene Encoding the Proprotein Convertase Neural Apoptosis-Regulated Convertase-1 Implicated in Familial Hypercholesterolemia. Arter. Thromb. Vasc. Biol. 2004, 24, 1454–1459. [Google Scholar] [CrossRef] [Green Version]
- Careskey, H.E.; Davis, R.A.; Alborn, W.E.; Troutt, J.S.; Cao, G.; Konrad, R.J. Atorvastatin increases human serum levels of proprotein convertase subtilisin/kexin type 9. J. Lipid Res. 2008, 49, 394–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayne, J.; Dewpura, T.; Raymond, A.; Cousins, M.; Chaplin, A.; A Lahey, K.; A LaHaye, S.; Mbikay, M.; Ooi, T.C.; Chrétien, M. Plasma PCSK9 levels are significantly modified by statins and fibrates in humans. Lipids Health Dis. 2008, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Mäkelä, K.A.; Leppäluoto, J.; Jokelainen, J.; Jämsä, T.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. Effect of Physical Activity on Plasma PCSK9 in Subjects with High Risk for Type 2 Diabetes. Front. Physiol. 2019, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Caselli, C.; Del Turco, S.; Ragusa, R.; Lorenzoni, V.; De Graaf, M.; Basta, G.; Scholte, A.; De Caterina, R.; Neglia, D. Association of PCSK9 plasma levels with metabolic patterns and coronary atherosclerosis in patients with stable angina. Cardiovasc. Diabetol. 2019, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Stenbäck, V.; Mutt, S.J.; Leppäluoto, J.; Gagnon, D.D.; Mäkelä, K.A.; Jokelainen, J.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. Association of Physical Activity With Telomere Length Among Elderly Adults—The Oulu Cohort 1945. Front. Physiol. 2019, 10, 444. [Google Scholar] [CrossRef] [PubMed]
- Mutt, S.J.; Jokelainen, J.; Sebert, S.; Auvinen, J.; Järvelin, M.-R.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65°North). Nutrients 2019, 11, 1229. [Google Scholar] [CrossRef] [Green Version]
- Leinonen, A.-M.; Ahola, R.; Kulmala, J.; Hakonen, H.; Vähä-Ypyä, H.; Herzig, K.-H.; Auvinen, J.; Keinänen-Kiukaanniemi, S.; Sievänen, H.; Tammelin, T.H.; et al. Measuring Physical Activity in Free-Living Conditions—Comparison of Three Accelerometry-Based Methods. Front. Physiol. 2017, 7. [Google Scholar] [CrossRef] [Green Version]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Tukiainen, T.; Tynkkynen, T.; Laatikainen, R.; Järvelin, M.-R.; Kähönen, M.; Lehtimäki, T.; Viikari, J.; et al. High-throughput serum NMR metabonomics for cost-effective holistic studies on systemic metabolism. Analyst 2009, 134, 1781–1785. [Google Scholar] [CrossRef]
- Saukkonen, T.; Mutt, S.J.; Jokelainen, J.; Saukkonen, A.-M.; Raza, G.S.; Karhu, T.; Härkönen, P.; Eckel, J.; Herzig, K.-H.; Rajala, U.; et al. Adipokines and inflammatory markers in elderly subjects with high risk of type 2 diabetes and cardiovascular disease. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arsenault, B.J.; Petrides, F.; Tabet, F.; Bao, W.; Hovingh, G.K.; Boekholdt, S.M.; Ramin-Mangata, S.; Meilhac, O.; Demicco, D.; Rye, K.-A.; et al. Effect of atorvastatin, cholesterol ester transfer protein inhibition, and diabetes mellitus on circulating proprotein subtilisin kexin type 9 and lipoprotein(a) levels in patients at high cardiovascular risk. J. Clin. Lipidol. 2018, 12, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilvo, M.; Simolin, H.; Metso, J.; Ruuth, M.; Öörni, K.; Jauhiainen, M.; Laaksonen, R.; Baruch, A. PCSK9 inhibition alters the lipidome of plasma and lipoprotein fractions. Atherosclerosis 2018, 269, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Soffer, G.; Pavlyha, M.; Ngai, C.; Thomas, T.; Holleran, S.; Ramakrishnan, R.; Karmally, W.; Nandakumar, R.; Fontanez, N.; Obunike, J.C.; et al. Effects of PCSK9 Inhibition With Alirocumab on Lipoprotein Metabolism in Healthy Humans. Circulation 2017, 135, 352–362. [Google Scholar] [CrossRef]
- Sliz, E.; Kettunen, J.; Holmes, M.V.; Williams, C.O.; Boachie, C.; Wang, Q.; Männikkö, M.; Sebert, S.; Walters, R.; Lin, K.; et al. Metabolomic Consequences of Genetic Inhibition of PCSK9 Compared With Statin Treatment. Circulation 2018, 138, 2499–2512. [Google Scholar] [CrossRef]
- Kwakernaak, A.J.; Lambert, G.; Dullaart, R.P. Plasma proprotein convertase subtilisin–kexin type 9 is predominantly related to intermediate density lipoproteins. Clin. Biochem. 2014, 47, 679–682. [Google Scholar] [CrossRef]
- Sullivan, S.; Fabbrini, E.; Horton, J.D.; Korenblat, K.; Patterson, B.W.; Klein, S. Lack of a relationship between plasma PCSK9 concentrations and hepatic lipoprotein kinetics in obese people. Transl. Res. 2011, 158, 302–306. [Google Scholar] [CrossRef] [Green Version]
- Ai, D.; Chen, C.; Han, S.; Ganda, A.; Murphy, A.J.; Haeusler, R.; Thorp, E.; Accili, D.; Horton, J.D.; Tall, A.R. Regulation of hepatic LDL receptors by mTORC1 and PCSK9 in mice. J. Clin. Investig. 2012, 122, 1262–1270. [Google Scholar] [CrossRef] [Green Version]
- Mbikay, M.; Sirois, F.; Mayne, J.; Wang, G.-S.; Chen, A.; Dewpura, T.; Prat, A.; Seidah, N.G.; Chretien, M.; Scott, F.W. PCSK9-deficient mice exhibit impaired glucose tolerance and pancreatic islet abnormalities. FEBS Lett. 2010, 584, 701–706. [Google Scholar] [CrossRef]
- Da Dalt, L.; Ruscica, M.; Bonacina, F.; Balzarotti, G.; Dhyani, A.; Di Cairano, E.; Baragetti, A.; Arnaboldi, L.; De Metrio, S.; Pellegatta, F.; et al. PCSK9 deficiency reduces insulin secretion and promotes glucose intolerance: The role of the low-density lipoprotein receptor. Eur. Hear. J. 2019, 40, 357–368. [Google Scholar] [CrossRef]
- Sattar, N.; Preiss, D.; Murray, H.M.; Welsh, P.; Buckley, B.M.; De Craen, A.J.M.; Seshasai, S.R.K.; McMurray, J.J.; Freeman, D.J.; Jukema, J.W.; et al. Statins and risk of incident diabetes: A collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | NGT | PreDM | DM | p-Value | |
|---|---|---|---|---|---|
| n = 670 | n = 348 | n = 217 | n = 105 | ||
| Age | 68.9 (0.55) | 68.9 (0.57) | 68.9 (0.52) | 68.8 (0.55) | 0.239 |
| Sex | 0.002 | ||||
| Men | 281 (41.9%) | 132 (37.9%) | 89 (41.0%) | 60 (57.1%) | |
| Women | 389 (58.1%) | 216 (62.1%) | 128 (59.0%) | 45 (42.9%) | |
| BMI (kg/m2) | 27.6 (4.69) | 26.0 (3.75) | 28.6 (4.70) | 30.7 (5.31) | <0.001 |
| Normal | 201 (30.3%) | 140 (40.8%) | 49 (22.6%) | 12 (11.5%) | |
| Overweight | 293 (44.1%) | 162 (47.2%) | 94 (43.3%) | 37 (35.6%) | |
| Obese | 170 (25.6%) | 41 (12.0%) | 74 (34.1%) | 55 (52.9%) | |
| Waist circumference (cm) | 94.0 (13.7) | 88.9 (11.5) | 97.0 (12.8) | 105 (14.0) | <0.001 |
| Fasting glucose (mmol/L) | 5.75 (1.03) | 5.31 (0.41) | 5.88 (0.55) | 7.02 (1.85) | <0.001 |
| Fasting insulin (pmol/L) | 15.4 (17.0) | 11.3 (5.62) | 16.1 (9.42) | 27.8 (37.3) | <0.001 |
| HOMA2-B | 109 (42.0) | 108 (33.7) | 112 (42.9) | 106 (62.1) | 0.406 |
| HOMA2-S | 71.7 (39.9) | 82.4 (38.7) | 63.2 (38.4) | 52.3 (35.8) | <0.001 |
| HOMA2-IR | 1.91 (1.36) | 1.48 (0.71) | 2.12 (1.20) | 2.98 (2.42) | <0.001 |
| DP (mmHg) | 85.6 (9.73) | 84.1 (9.50) | 88.1 (9.44) | 85.2 (10.1) | <0.001 |
| SP (mmHg) | 144 (17.7) | 141 (17.2) | 148 (18.0) | 147 (16.6) | <0.001 |
| Daily steps | 8869 (3696) | 9283 (3613) | 8499 (3686) | 8118 (3885) | 0.024 |
| Physical activity questionaires | <0.001 | ||||
| Non-active a | 153 (23.3%) | 62 (18.1%) | 46 (21.4%) | 45 (44.6%) | |
| Active b | 505 (76.7%) | 280 (81.9%) | 169 (78.6%) | 56 (55.4%) | |
| Smoking: | 0.001 | ||||
| Current | 81 (12.4%) | 39 (11.4%) | 20 (9.5%) | 22 (21.8%) | |
| Former (>6 months earlier) | 225 (34.4%) | 107 (31.2%) | 75 (35.5%) | 43 (42.6%) | |
| Never | 349 (53.2%) | 197 (57.4%) | 116 (55.0%) | 36 (35.6%) | |
| Alcohol (g/d) | 1.85 (4.61) | 1.23 (2.29) | 2.80 (7.11) | 1.99 (3.37) | <0.001 |
| Total cholesterol (mmol/L) | 5.33 (1.22) | 5.44 (1.15) | 5.51 (1.18) | 4.60 (1.26) | <0.001 |
| HDL-C (mmol/L) | 1.65 (0.46) | 1.74 (0.46) | 1.61 (0.43) | 1.40 (0.38) | <0.001 |
| Triglycerides (mmol/L) | 1.27 (0.81) | 1.07 (0.42) | 1.42 (0.70) | 1.63 (1.53) | <0.001 |
| HbA1c (mmol/L) | 40.6 (5.87) | 38.9 (3.45) | 40.2 (4.00) | 47.1 (9.95) | <0.001 |
| FLI | 45.6 (28.9) | 33.2 (23.9) | 54.5 (28.0) | 68.0 (25.9) | <0.001 |
| h-CRP (mg/L) | 3.49 (9.47) | 2.30 (4.42) | 4.49 (12.7) | 5.36 (13.0) | 0.002 |
| Analyte | No Statin (n = 427) | Statin Medication (n = 181) | Total (n = 608) | p-Value | |
|---|---|---|---|---|---|
| PCSK9 (ng/mL) | NGT | 251.6 (77.0) | 326.3 (136.1) | 270.6 (100.7) | <0.001 |
| PreDM | 248.5 (70.5) | 331.9 (74.3) | 271.4 (80.6) | <0.001 | |
| T2D | 275.5 (215.1) | 315.6 (85.5) | 295.3 (164.7) | <0.001 | |
| p-value | 0.258 | 0.751 | 0.131 | ||
| LDL-C (mmol/L) | NGT | 1.7 (0.5) | 1.2 (0.4) | 1.6 (0.5) | <0.001 |
| PreDM | 1.7 (0.5) | 1.3 (0.5) | 1.6 (0.5) | <0.001 | |
| T2D | 1.4 (0.6) | 1.0 (0.3) | 1.2 (0.5) | <0.001 | |
| p-value | <0.001 | <0.001 | <0.001 | ||
| VLDL-C (mmol/L) | NGT | 0.6 (0.2) | 0.5 (0.2) | 0.6 (0.2) | <0.001 |
| PreDM | 0.7 (0.2) | 0.5 (0.2) | 0.7 (0.2) | <0.001 | |
| T2D | 0.7 (0.4) | 0.5 (0.2) | 0.6 (0.3) | 0.001 | |
| p-value | <0.001 | 0.298 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mäkelä, K.A.; Jokelainen, J.; Stenbäck, V.; Auvinen, J.; Järvelin, M.-R.; Tulppo, M.; Leppäluoto, J.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. PCSK9 Levels and Metabolic Profiles in Elderly Subjects with Different Glucose Tolerance under Statin Therapy. J. Clin. Med. 2021, 10, 994. https://doi.org/10.3390/jcm10050994
Mäkelä KA, Jokelainen J, Stenbäck V, Auvinen J, Järvelin M-R, Tulppo M, Leppäluoto J, Keinänen-Kiukaanniemi S, Herzig K-H. PCSK9 Levels and Metabolic Profiles in Elderly Subjects with Different Glucose Tolerance under Statin Therapy. Journal of Clinical Medicine. 2021; 10(5):994. https://doi.org/10.3390/jcm10050994
Chicago/Turabian StyleMäkelä, Kari A., Jari Jokelainen, Ville Stenbäck, Juha Auvinen, Marjo-Riitta Järvelin, Mikko Tulppo, Juhani Leppäluoto, Sirkka Keinänen-Kiukaanniemi, and Karl-Heinz Herzig. 2021. "PCSK9 Levels and Metabolic Profiles in Elderly Subjects with Different Glucose Tolerance under Statin Therapy" Journal of Clinical Medicine 10, no. 5: 994. https://doi.org/10.3390/jcm10050994
APA StyleMäkelä, K. A., Jokelainen, J., Stenbäck, V., Auvinen, J., Järvelin, M. -R., Tulppo, M., Leppäluoto, J., Keinänen-Kiukaanniemi, S., & Herzig, K. -H. (2021). PCSK9 Levels and Metabolic Profiles in Elderly Subjects with Different Glucose Tolerance under Statin Therapy. Journal of Clinical Medicine, 10(5), 994. https://doi.org/10.3390/jcm10050994