
Ceramic-on-Ceramic Bearing in Total Hip Arthroplasty Reduces the Risk for Revision for Periprosthetic Joint Infection Compared to Ceramic-on-Polyethylene: A Matched Analysis of 118,753 Cementless THA Based on the German Arthroplasty Registry

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
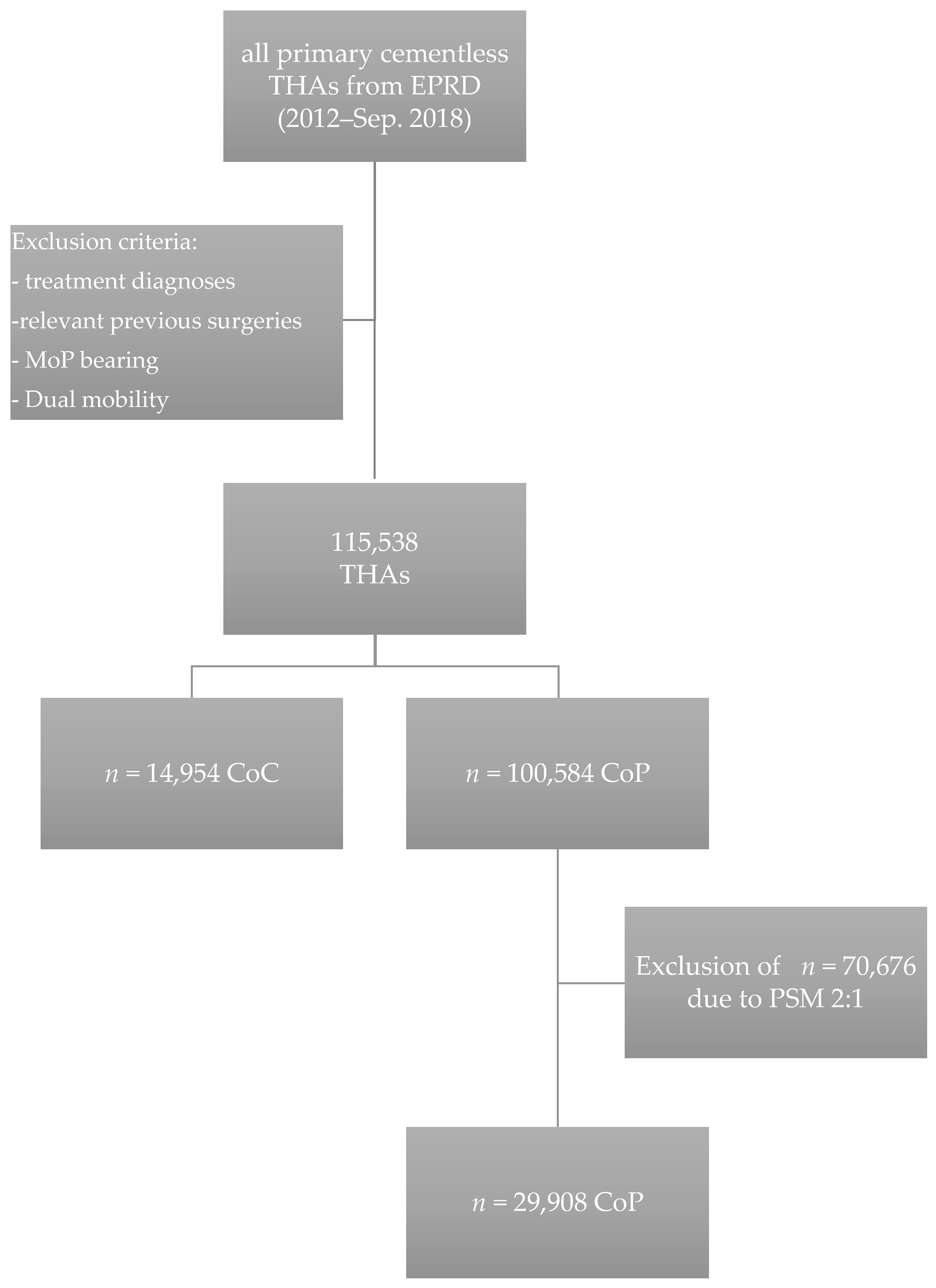
2.2. Study Subjects
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grimberg, A.; Jansson, V.; Lützner, J.; Melsheimer, O.; Morlock, M.; Steinbrück, A. Endoprothesenregister Deutschland (EPRD)—Jahresbericht 2020; EPRD: Berlin, Germany, 2020. [Google Scholar]
- Koek, M.B.G.; van der Kooi, T.I.I.; Stigter, F.C.A.; de Boer, P.T.; de Gier, B.; Hopmans, T.E.M.; de Greeff, S.C.; Burden of SSI Study Group. Burden of surgical site infections in the Netherlands: Cost analyses and disability-adjusted life years. J. Hosp. Infect. 2019, 103, 293–302. [Google Scholar] [CrossRef]
- Maoz, G.; Phillips, M.; Bosco, J.; Slover, J.; Stachel, A.; Inneh, I.; Iorio, R. The Otto Aufranc Award: Modifiable versus nonmodifiable risk factors for infection after hip arthroplasty. Clin. Orthop. Relat. Res. 2015, 473, 453–459. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.M.; van Steenbergen, L.N.; Stewart, R.E.; Stevens, M.; Rijk, P.C.; Bulstra, S.K.; Zijlstra, W.P. Patient Characteristics Influence Revision Rate of Total Hip Arthroplasty: American Society of Anesthesiologists Score and Body Mass Index Were the Strongest Predictors for Short-Term Revision After Primary Total Hip Arthroplasty. J. Arthroplast. 2019, 35, 188–192. [Google Scholar] [CrossRef] [Green Version]
- Dale, H.; Skramm, I.; Lower, H.L.; Eriksen, H.M.; Espehaug, B.; Furnes, O.; Skjeldestad, F.E.; Havelin, L.I.; Engesaeter, L.B. Infection after primary hip arthroplasty: A comparison of 3 Norwegian health registers. Acta Orthop. 2011, 82, 646–654. [Google Scholar] [CrossRef] [Green Version]
- Engesaeter, L.B.; Dale, H.; Schrama, J.C.; Hallan, G.; Lie, S.A. Surgical procedures in the treatment of 784 infected THAs reported to the Norwegian Arthroplasty Register. Acta Orthop. 2011, 82, 530–537. [Google Scholar] [CrossRef]
- Ong, K.L.; Kurtz, S.M.; Lau, E.; Bozic, K.J.; Berry, D.J.; Parvizi, J. Prosthetic joint infection risk after total hip arthroplasty in the Medicare population. J. Arthroplast. 2009, 24, 105–109. [Google Scholar] [CrossRef]
- Kleeman, L.T.; Bala, A.; Penrose, C.T.; Seyler, T.M.; Wellman, S.S.; Bolognesi, M.P. Comparison of Postoperative Complications Following Metal-on-Metal Total Hip Arthroplasty with Other Hip Bearings in Medicare Population. J. Arthroplast. 2018, 33, 1826–1832. [Google Scholar] [CrossRef]
- Grammatopoulos, G.; Munemoto, M.; Inagaki, Y.; Tanaka, Y.; Athanasou, N.A. The Diagnosis of Infection in Metal-on-Metal Hip Arthroplasties. J. Arthroplast. 2016, 31, 2569–2573. [Google Scholar] [CrossRef]
- Bordini, B.; Stea, S.; Castagnini, F.; Busanelli, L.; Giardina, F.; Toni, A. The influence of bearing surfaces on periprosthetic hip infections: Analysis of thirty nine thousand, two hundred and six cementless total hip arthroplasties. Int. Orthop. 2019, 43, 103–109. [Google Scholar] [CrossRef]
- Bozic, K.J.; Kurtz, S.; Lau, E.; Ong, K.; Chiu, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J. The epidemiology of bearing surface usage in total hip arthroplasty in the United States. J. Bone Jt. Surg. Am. 2009, 91, 1614–1620. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Baykal, D.; Springer, B.D. Outcomes of Ceramic Bearings After Primary Total Hip Arthroplasty in the Medicare Population. J. Arthroplast. 2017, 32, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Migaud, H.; Putman, S.; Kern, G.; Isida, R.; Girard, J.; Ramdane, N.; Delaunay, C.P.; Hamadouche, M.; So, F.S.G. Do the Reasons for Ceramic-on-ceramic Revisions Differ from Other Bearings in Total Hip Arthroplasty? Clin. Orthop. Relat. Res. 2016, 474, 2190–2199. [Google Scholar] [CrossRef] [Green Version]
- Germain, M.A.; Hatton, A.; Williams, S.; Matthews, J.B.; Stone, M.H.; Fisher, J.; Ingham, E. Comparison of the cytotoxicity of clinically relevant cobalt-chromium and alumina ceramic wear particles in vitro. Biomaterials 2003, 24, 469–479. [Google Scholar] [CrossRef]
- Pitto, R.P.; Sedel, L. Periprosthetic Joint Infection in Hip Arthroplasty: Is There an Association Between Infection and Bearing Surface Type? Clin. Orthop. Relat. Res. 2016, 474, 2213–2218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madanat, R.; Laaksonen, I.; Graves, S.E.; Lorimer, M.; Muratoglu, O.; Malchau, H. Ceramic bearings for total hip arthroplasty are associated with a reduced risk of revision for infection. Hip. Int. 2018, 28, 222–226. [Google Scholar] [CrossRef]
- Hexter, A.T.; Hislop, S.M.; Blunn, G.W.; Liddle, A.D. The effect of bearing surface on risk of periprosthetic joint infection in total hip arthroplasty: A systematic review and meta-analysis. Bone Jt. J. 2018, 100-B, 134–142. [Google Scholar] [CrossRef]
- Jansson, V.; Grimberg, A.; Melsheimer, O.; Perka, C.; Steinbruck, A. Orthopaedic registries: The German experience. EFORT Open Rev. 2019, 4, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Grimberg, A.W.; Grupp, T.M.; Elliott, J.; Melsheimer, O.; Jansson, V.; Steinbruck, A. Ceramic Coating in Cemented Primary Total Knee Arthroplasty is Not Associated with Decreased Risk of Revision due to Early Prosthetic Joint Infection. J. Arthroplast. 2020, 36, 991–997. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2010. [Google Scholar]
- Witso, E. The rate of prosthetic joint infection is underestimated in the arthroplasty registers. Acta Orthop. 2015, 86, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Kunutsor, S.K.; Burston, B.; Porter, M.; Blom, A.W. Risk factors associated with revision for prosthetic joint infection after hip replacement: A prospective observational cohort study. Lancet Infect. Dis. 2018, 18, 1004–1014. [Google Scholar] [CrossRef] [Green Version]
- Menendez, M.E.; Neuhaus, V.; van Dijk, C.N.; Ring, D. The Elixhauser comorbidity method outperforms the Charlson index in predicting inpatient death after orthopaedic surgery. Clin. Orthop. Relat. Res. 2014, 472, 2878–2886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karbysheva, S.; Cabric, S.; Trampuz, A. Biofilm investigation on ceramic, metal and polyethylene bearing components from explanted hip joint replacement systems. In Proceedings of the eCM XIX Orthopaedic Infection, Davos Platz, Switzerland, 26–28 June 2019; p. 8. [Google Scholar]
- An, Y.H.; Friedman, R.J. Concise review of mechanisms of bacterial adhesion to biomaterial surfaces. J. Biomed. Mater. Res. 1998, 43, 338–348. [Google Scholar] [CrossRef]
- Katsikogianni, M.; Missirlis, Y.F. Concise review of mechanisms of bacterial adhesion to biomaterials and of techniques used in estimating bacteria-material interactions. Eur. Cell Mater. 2004, 8, 37–57. [Google Scholar] [CrossRef]
- Zmantar, T.; Bettaieb, F.; Chaieb, K.; Ezzili, B.; Mora-Ponsonnet, L.; Othmane, A.; Jaffrézic, N.; Bakhrouf, A. Atomic force microscopy and hydrodynamic characterization of the adhesion of staphylococcus aureus to hydrophilic and hydrophobic substrata at different pH values. World J. Microbiol. Biotechnol. 2011, 27, 887–896. [Google Scholar] [CrossRef]
- Lass, R.; Giurea, A.; Kubista, B.; Hirschl, A.M.; Graninger, W.; Presterl, E.; Windhager, R.; Holinka, J. Bacterial adherence to different components of total hip prosthesis in patients with prosthetic joint infection. Int. Orthop. 2014, 38, 1597–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unmatched | Matched 2:1 | SMD | |||||
|---|---|---|---|---|---|---|---|
| Variable | Characteristics | CoP | CoP | CoC | |||
| mean age at surgery | years (SD) | 67.4 (9.8) | 62.7 (10.1) | 62.6 (10.2) | 0.012 | ||
| % | n | % | n | % | |||
| sex | male | 39.1 | 12,491 | 41.8 | 6406 | 42.8 | 0.022 |
| female | 60.9 | 17,417 | 58.2 | 8548 | 57.22 | ||
| Complicated diabetes | no | 98.8 | 29,638 | 99.1 | 14,779 | 98.8 | 0.026 |
| yes | 1.2 | 270 | 0.9 | 175 | 1.2 | ||
| obesity | no | 81.3 | 24,712 | 82.6 | 12,374 | 82.7 | 0.003 |
| yes | 18.7 | 5196 | 17.4 | 2580 | 17.3 | ||
| head size category | <32 mm | 6.0 | 713 | 2.4 | 371 | 2.5 | 0.010 |
| 32 mm | 59.5 | 11,245 | 37.6 | 5557 | 37.2 | ||
| >32 mm | 34.5 | 17,950 | 60.0 | 9026 | 60.4 | ||
| Elixhauser index | ≥5 | 3.0 | 770 | 2.6 | 410 | 2.7 | 0.014 |
| 0 | 22.8 | 8499 | 28.4 | 4304 | 28.8 | ||
| 1–4 | 74.1 | 20,639 | 69.0 | 10,240 | 68.5 | ||
| year of surgery | 2012–2014 2015 2016 2017 2018 | 6.3 14.1 25.3 30.1 24.1 | 2575 5155 7447 8436 6295 | 8.6 17.2 24.9 28.2 21.0 | 1401 2627 3741 4150 3035 | 9.4 17.6 25.0 27.8 20.3 | 0.033 |
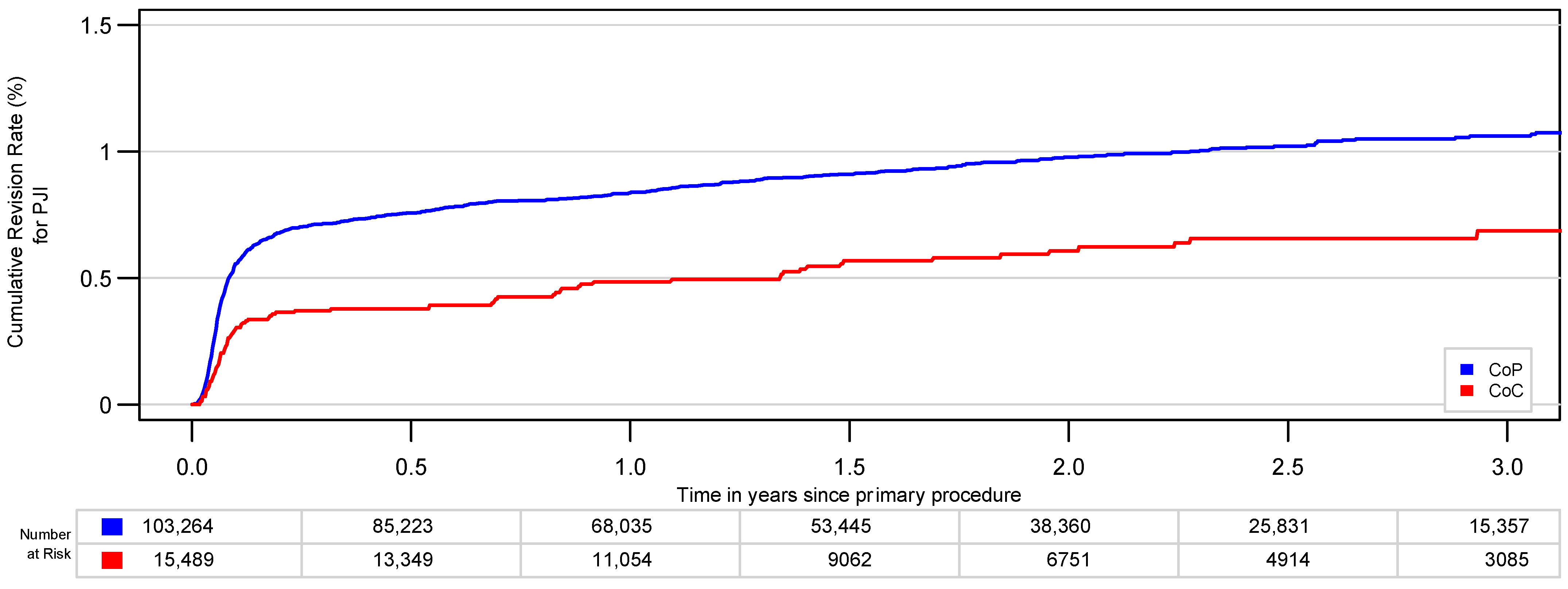
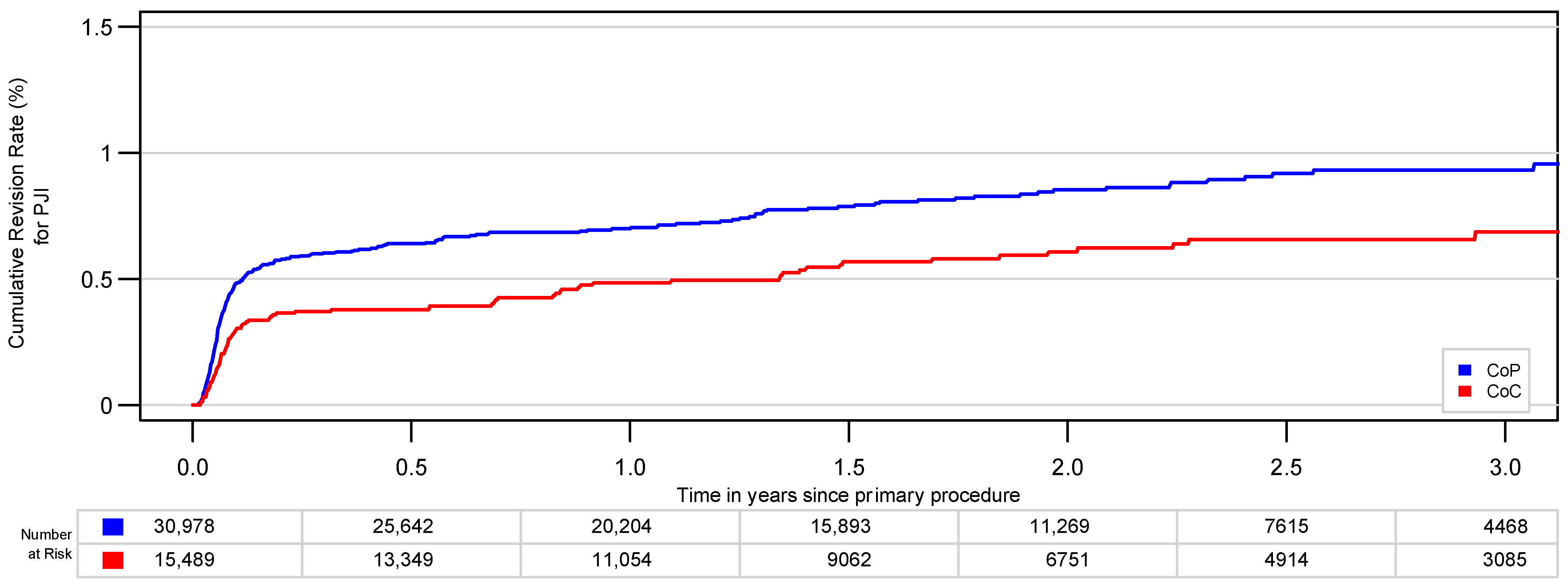
| CPR (95% CI) and Numbers at Risk since Primary THA | ||||||
|---|---|---|---|---|---|---|
| 1 year | 2 years | 3 years | ||||
| CoC | 0.5 (0.4; 0.6) | 10,625 | 0.6 (0.4; 0.6) | 6485 | 0.7 (0.5; 0.9) | 2971 |
| CoP | 0.7 (0.6; 0.8) | 20,694 | 0.8 (0.7; 1.0) | 12,588 | 0.9 (0.8; 1.1) | 5714 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renner, L.; Perka, C.; Melsheimer, O.; Grimberg, A.; Jansson, V.; Steinbrück, A. Ceramic-on-Ceramic Bearing in Total Hip Arthroplasty Reduces the Risk for Revision for Periprosthetic Joint Infection Compared to Ceramic-on-Polyethylene: A Matched Analysis of 118,753 Cementless THA Based on the German Arthroplasty Registry. J. Clin. Med. 2021, 10, 1193. https://doi.org/10.3390/jcm10061193
Renner L, Perka C, Melsheimer O, Grimberg A, Jansson V, Steinbrück A. Ceramic-on-Ceramic Bearing in Total Hip Arthroplasty Reduces the Risk for Revision for Periprosthetic Joint Infection Compared to Ceramic-on-Polyethylene: A Matched Analysis of 118,753 Cementless THA Based on the German Arthroplasty Registry. Journal of Clinical Medicine. 2021; 10(6):1193. https://doi.org/10.3390/jcm10061193
Chicago/Turabian StyleRenner, Lisa, Carsten Perka, Oliver Melsheimer, Alexander Grimberg, Volkmar Jansson, and Arnd Steinbrück. 2021. "Ceramic-on-Ceramic Bearing in Total Hip Arthroplasty Reduces the Risk for Revision for Periprosthetic Joint Infection Compared to Ceramic-on-Polyethylene: A Matched Analysis of 118,753 Cementless THA Based on the German Arthroplasty Registry" Journal of Clinical Medicine 10, no. 6: 1193. https://doi.org/10.3390/jcm10061193
APA StyleRenner, L., Perka, C., Melsheimer, O., Grimberg, A., Jansson, V., & Steinbrück, A. (2021). Ceramic-on-Ceramic Bearing in Total Hip Arthroplasty Reduces the Risk for Revision for Periprosthetic Joint Infection Compared to Ceramic-on-Polyethylene: A Matched Analysis of 118,753 Cementless THA Based on the German Arthroplasty Registry. Journal of Clinical Medicine, 10(6), 1193. https://doi.org/10.3390/jcm10061193