
Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
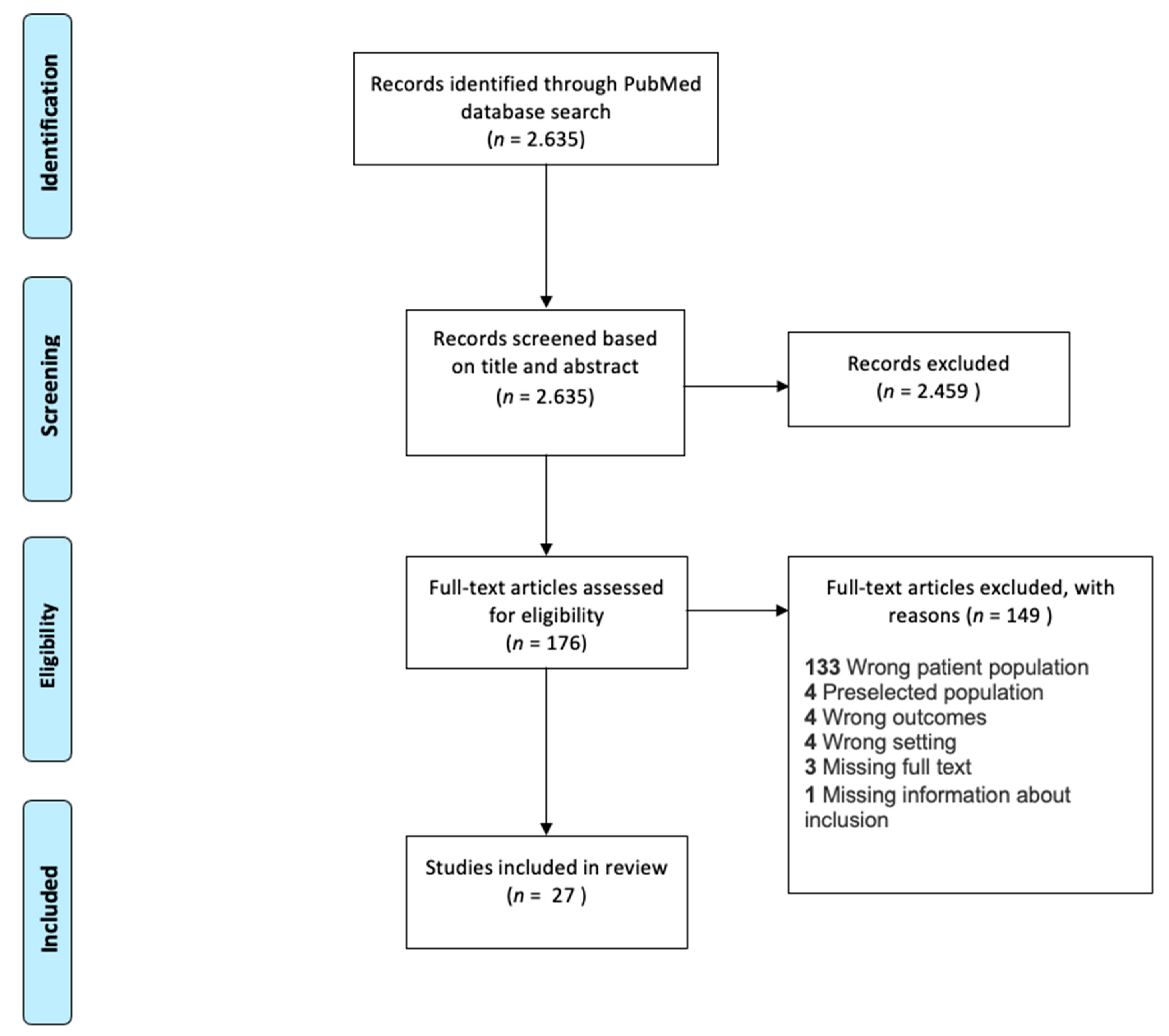
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction and Processing
2.4. Statistics
2.5. Data Sharing and PRISMA Statement
3. Results
3.1. Age Distribution
3.2. Sex Distribution
3.3. Causes for Secondary wAIHA
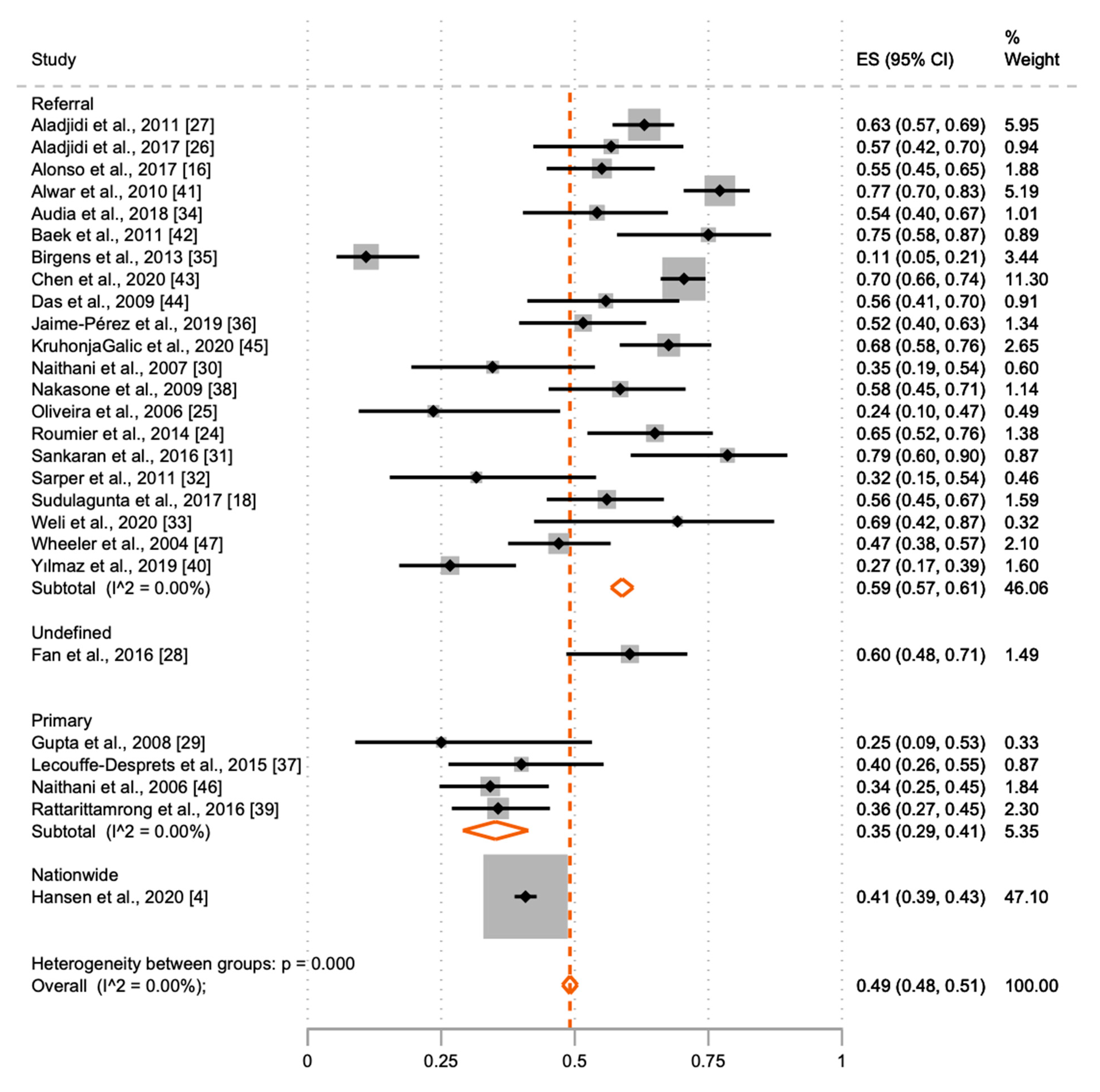
3.4. Level of Health Care Facility for AIHA Diagnostics
4. Discussion
4.1. Causes for Secondary AIHA
4.2. Age and Sex Distribution
4.3. Level of Health Care Facility at wAIHA Diagnosis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, S.H. Diagnosis and treatment of autoimmune hemolytic anemia: Classic approach and recent advances. Blood Res. 2016, 51, 69–71. [Google Scholar] [CrossRef] [Green Version]
- Zanella, A.; Barcellini, W. Treatment of autoimmune hemolytic anemias. Haematologica 2014, 99, 1547–1554. [Google Scholar] [CrossRef]
- Lechner, K.; Jäger, U. How I treat autoimmune hemolytic anemias in adults. Blood 2010, 116, 1831–1838. [Google Scholar] [CrossRef]
- Hansen, D.L.; Möller, S.; Andersen, K.; Gaist, D.; Frederiksen, H. Increasing Incidence and Prevalence of Acquired Hemolytic Anemias in Denmark, 1980–2016. Clin. Epidemiol. 2020, 12, 497–508. [Google Scholar] [CrossRef]
- Sokol, R.J.; Hewitt, S.; Stamps, B.K. Autoimmune haemolysis: An 18-year study of 865 cases referred to a regional transfusion centre. BMJ 1981, 282, 2023–2027. [Google Scholar] [CrossRef] [Green Version]
- Gehrs, B.C.; Friedberg, R.C. Autoimmune hemolytic anemia. Am. J. Hematol. 2002, 69, 258–271. [Google Scholar] [CrossRef]
- Kalfa, T.A. Warm antibody autoimmune hemolytic anemia. Hematology 2016, 2016, 690–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fava, A.; Petri, M. Systemic lupus erythematosus: Diagnosis and clinical management. J. Autoimmun. 2019, 96, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, R.K.; Das, S.S. Autoimmune hemolytic anemia: From lab to bedside. Asian J. Transfus. Sci. 2014, 8, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Packman, C.H. Hemolytic anemia due to warm autoantibodies. Blood Rev. 2008, 22, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Sawitsky, A.; Ozaeta, P.B. Disease-associated autoimmune hemolytic anemia. Bull. N. Y. Acad. Med. 1970, 46, 411–426. [Google Scholar]
- Puthenparambil, J.; Lechner, K.; Kornek, G. Autoimmune hemolytic anemia as a paraneoplastic phenomenon in solid tumors: A critical analysis of 52 cases reported in the literature. Wien. Klin. Wochenschr. 2010, 122, 229–236. [Google Scholar] [CrossRef]
- Packman, C.H. The Clinical Pictures of Autoimmune Hemolytic Anemia. Transfus. Med. Hemotherapy 2015, 42, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, P. A review of autoimmune diseases associated with cancer. Front. Biosci. 2010, 2, 122–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, K.; Ferrer, G.; Pereira, A.; Moreno, C.; Montserrat, E. Autoimmune cytopenia in chronic lymphocytic leukaemia: Diagnosis and treatment. Br. J. Haematol. 2011, 154, 14–22. [Google Scholar] [CrossRef]
- Alonso, H.-C.; Manuel, A.-A.V.; Amir, C.G.C.; Sergio, R.-R.; Allan, P.; Xavier, L.-K.; Juventina, T.-A.E. Warm autoimmune hemolytic anemia: Experience from a single referral center in Mexico City. Blood Res. 2017, 52, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Zent, C.S.; Kay, N.E. Autoimmune Complications in Chronic Lymphocytic Leukaemia (CLL). Best Pr. Res. Clin. Haematol. 2010, 23, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Sudulagunta, S.R.; Kumbhat, M.; Sodalagunta, M.B.; Nataraju, A.S.; Raja, S.K.B.; Thejaswi, K.C.; Deepak, R.; Mohammed, A.H.; Sunny, S.P.; Visweswar, A.; et al. Warm Autoimmune Hemolytic Anemia: Clinical Profile and Management. J. Hematol. 2017, 6, 12–20. [Google Scholar] [CrossRef]
- Vaglio, S.; Arista, M.C.; Perrone, M.P.; Tomei, G.; Testi, A.M.; Coluzzi, S.; Girelli, G. Autoimmune hemolytic anemia in childhood: Serologic features in 100 cases. Transfusion 2007, 47, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Garratty, G. Drug-induced immune hemolytic anemia. Hematology 2009, 2009, 73–79. [Google Scholar] [CrossRef]
- Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019; Available online: https://www.stata.com/gsearch.php?q=release+16&site=stata&client=stata&proxystylesheet=stata&restrict=Default&output=xml_no_dtd (accessed on 16 March 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roumier, M.; Loustau, V.; Guillaud, C.; Languille, L.; Mahevas, M.; Khellaf, M.; Limal, N.; Noizat-Pirenne, F.; Godeau, B.; Michel, M. Characteristics and outcome of warm autoimmune hemolytic anemia in adults: New insights based on a single-center experience with 60 patients. Am. J. Hematol. 2014, 89, E150–E155. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.C.L.; Oliveira, B.M.; Murao, M.; Vieira, Z.M.; Gresta, L.T.; Viana, M.B. Clinical course of autoimmune hemolytic anemia: An observational study. J. Pediatr. 2006, 82, 58–62. [Google Scholar] [CrossRef]
- Aladjidi, N.; Jutand, M.-A.; Beaubois, C.; Fernandes, H.; Jeanpetit, J.; Coureau, G.; Gilleron, V.; Kostrzewa, A.; Lauroua, P.; Jeanne, M.; et al. Reliable assessment of the incidence of childhood autoimmune hemolytic anemia. Pediatr. Blood Cancer 2017, 64, e26683. [Google Scholar] [CrossRef]
- Aladjidi, N.; Leverger, G.; Leblanc, T.; Picat, M.Q.; Michel, G.; Bertrand, Y.; Bader-Meunier, B.; Robert, A.; Nelken, B.; Gandemer, V.; et al. New insights into childhood autoimmune hemolytic anemia: A French national observational study of 265 children. Haematology 2011, 96, 655–663. [Google Scholar] [CrossRef]
- Fan, J.; He, H.; Zhao, W.; Wang, Y.; Lu, J.; Li, J.; Li, J.; Xiao, P.; Lu, Y.; Chai, Y.; et al. Clinical Features and Treatment Outcomes of Childhood Autoimmune Hemolytic Anemia. J. Pediatr. Hematol. 2016, 38, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Shukla, J.; Bhatia, B.D. Autoimmune hemolytic anemia. Indian J. Pediatr. 2008, 75, 451–454. [Google Scholar] [CrossRef]
- Naithani, R.; Agrawal, N.; Mahapatra, M.; Kumar, R.; Pati, H.P.; Choudhry, V.P. AUTOIMMUNE HEMOLYTIC ANEMIA IN CHILDREN. Pediatr. Hematol. Oncol. 2007, 24, 309–315. [Google Scholar] [CrossRef]
- Sankaran, J.; Rodriguez, V.; Jacob, E.K.; Kreuter, J.D.; Go, R.S. Autoimmune Hemolytic Anemia in Children. J. Pediatr. Hematol. 2016, 38, e120–e124. [Google Scholar] [CrossRef]
- Sarper, N.; Kılıç, S.Ç.; Zengin, E.; Gelen, S.A. Management of autoimmune hemolytic anemia in children and adolescents: A single center experience. Turk. J. Hematol. 2011, 28, 198–205. [Google Scholar] [CrossRef]
- Weli, M.; Ben Hlima, A.; Belhadj, R.; Maalej, B.; Elleuch, A.; Mekki, N.; Gargouri, L.; Kamoun, T.; Barbouche, M.-R.; Mahfoudh, A. Diagnosis and management of autoimmune hemolytic anemia in children. Transfus. Clin. Biol. 2020, 27, 61–64. [Google Scholar] [CrossRef]
- Audia, S.; Bach, B.; Samson, M.; Lakomy, D.; Bour, J.-B.; Burlet, B.; Guy, J.; Duvillard, L.; Branger, M.; Leguy-Seguin, V.; et al. Venous thromboembolic events during warm autoimmune hemolytic anemia. PLoS ONE 2018, 13, e0207218. [Google Scholar] [CrossRef] [Green Version]
- Birgens, H.S.; Frederiksen, H.; Hasselbalch, H.C.; Rasmussen, I.H.; Nielsen, O.J.; Kjeldsen, L.; Larsen, H.; Mourits-Andersen, T.; Plesner, T.; Rønnov-Jessen, D.; et al. A phase III randomized trial comparing glucocorticoid monotherapyversusglucocorticoid and rituximab in patients with autoimmune haemolytic anaemia. Br. J. Haematol. 2013, 163, 393–399. [Google Scholar] [CrossRef]
- Jaime-Pérez, J.C.; Aguilar-Calderón, P.; Salazar-Cavazos, L.; León, A.G.-D.; Gómez-Almaguer, D. Treatment of autoimmune hemolytic anemia: Real world data from a reference center in Mexico. Blood Res. 2019, 54, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Lecouffe-Desprets, M.; Néel, A.; Graveleau, J.; Leux, C.; Perrin, F.; Visomblain, B.; Artifoni, M.; Masseau, A.; Connault, J.; Pottier, P.; et al. Venous thromboembolism related to warm autoimmune hemolytic anemia: A case–control study. Autoimmun. Rev. 2015, 14, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Nakasone, H.; Kako, S.; Endo, H.; Ito, A.; Sato, M.; Terasako, K.; Okuda, S.; Tanaka, Y.; Yamazaki, R.; Oshima, K.; et al. Diabetes mellitus is associated with high early-mortality and poor prognosis in patients with autoimmune hemolytic anemia. Hematology 2009, 14, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Rattarittamrong, E.; Eiamprapai, P.; Tantiworawit, A.; Rattanathammethee, T.; Hantrakool, S.; Chai-Adisaksopha, C.; Norasetthada, L. Clinical characteristics and long-term outcomes of warm-type autoimmune hemolytic anemia. Hematology 2016, 21, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yılmaz, F.; Kiper, D.; Koç, M.; Karslı, T.; Kılınç, M.; Gediz, F.; Toptaş, T.; Payzın, B. Clinical Features and Treatment Outcomes of Warm Autoimmune Hemolytic Anemia: A Retrospective Analysis of 60 Turkish Patients. Indian J. Hematol. Blood Transfus. 2019, 35, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Alwar, V.; Shanthala, D.A.; Sitalakshmi, S.; Karuna, R.K. Clinical Patterns and Hematological Spectrum in Autoimmune Hemolytic Anemia. J. Lab. Physicians 2010, 2, 17–20. [Google Scholar] [CrossRef]
- Baek, S.-W.; Lee, M.-W.; Ryu, H.-W.; Lee, K.-S.; Song, I.-C.; Lee, H.-J.; Yun, H.-J.; Kim, S.; Jo, D.-Y. Clinical features and outcomes of autoimmune hemolytic anemia: A retrospective analysis of 32 cases. Korean J. Hematol. 2011, 46, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Wang, L.; Han, B.; Qin, L.; Ying, B. Autoimmune hemolytic anemia in hospitalized patients. Medicine 2020, 99, e18739. [Google Scholar] [CrossRef]
- Das, S.S.; Nityanand, S.; Chaudhary, R. Clinical and serological characterization of autoimmune hemolytic anemia in a tertiary care hospital in North India. Ann. Hematol. 2009, 88, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Galic, Z.K.; Jagnjic, S.; Bingulac-Popovic, J.; Peraica, A.P.; Hecimovic, A.; Patko, M.S.; Jukic, I. Warm red blood cell autoantibodies and clinical diagnoses in patients with or without autoimmune hemolysis. Transfus. Clin. Biol. 2020, 27, 25–29. [Google Scholar] [CrossRef]
- Naithani, R.; Agrawal, N.; Mahapatra, M.; Pati, H.; Kumar, R.; Choudhary, V. Autoimmune hemolytic anemia in India: Clinico-hematological spectrum of 79 cases. Hematology 2006, 11, 73–76. [Google Scholar] [CrossRef]
- Wheeler, C.A.; Calhoun, L.; Sbb, M.A.; Blackall, D.P. Warm Reactive Autoantibodies: Clinical and Serologic Correlations. Am. J. Clin. Pathol. 2004, 122, 680–685. [Google Scholar] [CrossRef]
- Hill, Q.A.; Hill, A.; Berentsen, S. Defining autoimmune hemolytic anemia: A systematic review of the terminology used for diagnosis and treatment. Blood Adv. 2019, 3, 1897–1906. [Google Scholar] [CrossRef] [Green Version]
- Jäger, U.; Barcellini, W.; Broome, C.M.; Gertz, M.A.; Hill, A.; Hill, Q.A.; Jilma, B.; Kuter, D.J.; Michel, M.; Montillo, M.; et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting. Blood Rev. 2020, 41, 100648. [Google Scholar] [CrossRef]
- Zeerleder, S. Autoimmune haemolytic anaemia—A practical guide to cope with a diagnostic and therapeutic challenge. Neth. J. Med. 2011, 69, 177–184. [Google Scholar] [PubMed]
- Shaikh, H.; Mewawalla, P. Evans Syndrome; StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Moulis, G.; Palmaro, A.; Montastruc, J.-L.; Godeau, B.; Lapeyre-Mestre, M.; Sailler, L. Epidemiology of incident immune thrombocytopenia: A nationwide population-based study in France. Blood 2014, 124, 3308–3315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekhlyudov, L.; Latosinsky, S. The Interface of Primary and Oncology Specialty Care: From Symptoms to Diagnosis. J. Natl. Cancer Inst. Monogr. 2010, 2010, 11–17. [Google Scholar] [CrossRef]
- Barcellini, W.; Fattizzo, B. The Changing Landscape of Autoimmune Hemolytic Anemia. Front. Immunol. 2020, 11, 946. [Google Scholar] [CrossRef] [PubMed]
- Catovsky, D.; Wade, R.; Else, M. The clinical significance of patients’ sex in chronic lymphocytic leukemia. Haematology 2014, 99, 1088–1094. [Google Scholar] [CrossRef]
- Vedsted, P.; Olesen, F. A differentiated approach to referrals from general practice to support early cancer diagnosis—The Danish three-legged strategy. Br. J. Cancer 2015, 112, S65–S69. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients | Number of Females | Median Age (Range) | Number of Patients with Secondary AIHA | Age Groups | Location of Diagnosis |
|---|---|---|---|---|---|---|
| Aladjidi et al., 2017 [26] | 44 | 21 | 8.6 (0.1–17.9) | 25 | Paediatric cohort < 18 | Referral |
| Aladjidi et al., 2011 [27] | 265 | 114 | 3.8 (0.1–17.4) | 167 | Paediatric cohort < 18 | Referral |
| Fan et al., 2016 [28] | 68 | 28 | 1.3 (0.3–15) | 41 | Paediatric cohort < 16 | Not described |
| Gupta et al., 2008 [29] | 12 | 4.5 (0.6–8) | 3 | Paediatric cohort | Primary | |
| Naithani et al., 2007 [30] | 26 | 16 | 11 (2.5–17) | 9 | Paediatric cohort < 18 | Referral |
| Oliveira et al., 2006 [25] | 17 | 7 | 0.9 (0.1–15) | 4 | Paediatric cohort < 15 | Referral |
| Sankaran et al., 2016 [31] | 28 | 8 | 10 (0.1–18) | 22 | Paediatric cohort ≤ 18 | Referral |
| Sarper et al., 2011 [32] | 19 | 5 | 5 (0.1–17) | 6 | Paediatric cohort < 18 | Referral |
| Weli et al., 2020 [33] | 13 | 8 | 4.5 (0.2–13) | 9 | Paediatric cohort | Referral |
| Alonso et al., 2017 [16] | 89 | 65 | 36 (17–86) | 49 | Adult only cohort ≥ 16 | Referral |
| Audia et al., 2018 [34] | 48 | 24 | 65 | 26 | Adult only cohort ≥ 18 | Referral |
| Birgens et al., 2013 [35] | 64 | 27 | 66 (35–90) | 7 | Adult only cohort ≥ 18 | Referral |
| Jaime-Pérez et al., 2019 [36] | 64 | 39 | 37 (16–77) | 33 | Adult only cohort ≥ 16 | Referral |
| Lecouffe-Desprets et al., 2015 [37] | 40 | 27 | 54 (14–86) | 16 | Adult only cohort > 18 | Primary |
| Nakasone et al., 2009 [38] | 53 | 23 | 65 (28–88) | 31 | Adult only cohort | Referral |
| Rattarittamrong et al., 2016 [39] | 101 | 78 | 43 (15–83) | 36 | Adult only cohort > 15 | Primary |
| Roumier et al., 2014 [24] | 60 | 30 | 53.6 (16–95) | 39 | Adult only cohort ≥ 16 | Referral |
| Sudulagunta et al., 2017 [18] | 75 | 38 | 53 | 42 | Adult only cohort ≥ 16 | Referral |
| Yılmaz et al., 2019 [40] | 60 | 38 | 52 (20–85) | 16 | Adult only cohort | Referral |
| Alwar et al., 2010 [41] | 175 | - | - | 135 | All ages included | Referral |
| Baek et al., 2011 [42] | 32 | 31 | 49 (17–86) | 24 | All ages included | Referral |
| Chen et al., 2020 [43] | 450 | 315 | 51 (31–71) | 317 | All ages included | Referral |
| Das et al., 2009 [44] | 43 | 33 | 31 (12–70) | 24 | All ages included | Referral |
| Hansen et al., 2020 [4] | 2175 | 1518 | 68.7 | 887 | All ages included | All |
| KruhonjaGalic et al., 2020 [45] | 111 | 72 | 68 (14–82) | 75 | All ages included | Referral |
| Naithani et al., 2006 [46] | 79 | 45 | 30.5 (0.2–66) | 27 | All ages included | Primary |
| Wheeler et al., 2004 [47] | 100 | 44 | 53.3 (3–90) | 47 | All ages included | Referral |
| Total | 4311 | 2654 | - | 2117 |
| Patients | Females (%) | Median Age (Year) | Secondary (%) | |
|---|---|---|---|---|
| Paediatric cohorts | 492 | 43.1 (42.5; 43.8) | 3.8 | 58.1 (53.6; 62.5) |
| Adult cohorts | 654 | 59.5 (58.5; 60.4) | 53 | 45.1 (41.2; 49.0) |
| All ages | 3165 | 64.4 (64.0; 64.7) | 68.7 | 48.5 (46.8; 50.3) |
| Total | 4311 | 68.8 (68.6; 69.0) | 68.7 | 49.1 (47.6; 50.6) |
| Disease | Studies Including Patients of All Ages | Studies Only Including Adult Patients | Studies Only Including Paediatric Patients | Total (n) |
|---|---|---|---|---|
| Systemic lupus erythematosus | 51.4% | 39.5% | 9.1% | 220 |
| Evans syndrome | 11.5% | 10.3% | 78.2% | 156 |
| Connective tissue disease * | 98.9% | 1.1% | 93 | |
| Infection | 11.1% | 1.6% | 87.3% | 63 |
| Non-Hodgkin lymphomas | 86.4% | 13.6% | 59 | |
| Lymphoid diseases | 100% | 45 | ||
| Chronic lymphocytic leukaemia | 55.3% | 44.7% | 38 | |
| Unspecified | 72.2% | 27.8% | 36 | |
| Autoimmune diseases * | 93.8% | 3.1% | 3.1% | 32 |
| B-cell lymphomas | 100% | 32 | ||
| Rheumatoid arthritis | 46.2% | 46.2% | 7.6% | 26 |
| Antiphospholipid syndrome | 14.3% | 80.9% | 4.8% | 21 |
| Diabetes mellitus | 90% | 10% | 20 | |
| Renal failure | 100% | 19 | ||
| Lymphoma not otherwise specified | 55.6% | 43.4% | 18 | |
| Sjøgrens disease | 70.6% | 29.4% | 17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tranekær, S.; Hansen, D.L.; Frederiksen, H. Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1244. https://doi.org/10.3390/jcm10061244
Tranekær S, Hansen DL, Frederiksen H. Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(6):1244. https://doi.org/10.3390/jcm10061244
Chicago/Turabian StyleTranekær, Stinne, Dennis Lund Hansen, and Henrik Frederiksen. 2021. "Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 6: 1244. https://doi.org/10.3390/jcm10061244
APA StyleTranekær, S., Hansen, D. L., & Frederiksen, H. (2021). Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(6), 1244. https://doi.org/10.3390/jcm10061244