
GT-Repeat Polymorphism in the HO-1 Gene Promoter Is Associated with Risk of Liver Cancer: A Follow-Up Study from Arseniasis-Endemic Areas in Taiwan

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Baseline Characteristics
2.2. Determination of HO-1 (GT)n Genotype
2.3. Follow-Up and Ascertainment of Cancer Cases
2.4. Statistical Methods
3. Results
3.1. Baseline Characteristics and Liver Cancer Incidence by HO-1 (GT)n Genotype
3.2. Association of HO-1 (GT)n Genotype with Liver Cancer Risk
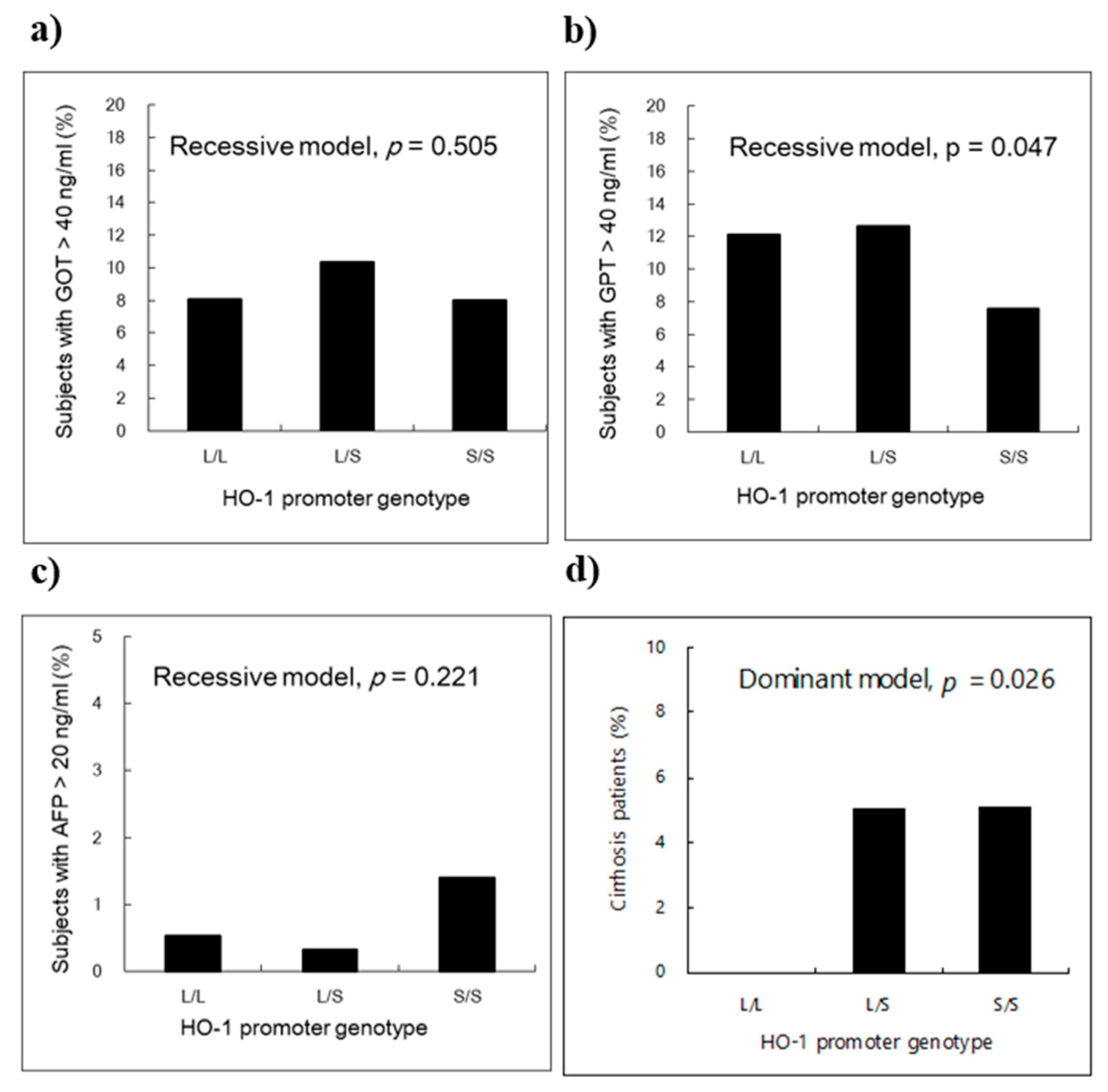
3.3. Frequency of Liver-Related Injury Markers According to the HO-1 (GT)n Genotype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maines, M.D. Heme oxygenase: Function, multiplicity, regulatory mechanisms, and clinical applications. FASEB J. 1988, 2, 2557–2568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyse, S.M.; Tyrrell, R.M. Heme oxygenase is the major 32-kDa stress protein induced in human skin fibroblasts by UVA radiation, hydrogen peroxide, and sodium arsenite. Proc. Natl. Acad. Sci. USA 1989, 86, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Abraham, N.G.; Kappas, A. Pharmacological and clinical aspects of heme oxygenase. Pharmacol. Rev. 2008, 60, 79–127. [Google Scholar] [CrossRef] [Green Version]
- Suttner, D.M.; Dennery, P.A. Reversal of HO-1 related cytoprotection with increased expression is due to reactive iron. FASEB J. 1999, 13, 1800–1809. [Google Scholar] [CrossRef] [PubMed]
- Was, H.; Dulak, J.; Jozkowicz, A. Heme oxygenase-1 in tumor biology and therapy. Curr. Drug Targets 2010, 11, 1551–1570. [Google Scholar] [CrossRef] [PubMed]
- Lavrovsky, Y.; Schwartzman, M.L.; Levere, R.D.; Kappas, A.; Abraham, N.G. Identification of binding sites for transcription factors NF-kappa B and AP-2 in the promoter region of the human heme oxygenase 1 gene. Proc. Natl. Acad. Sci. USA 1994, 91, 5987–5991. [Google Scholar] [CrossRef] [Green Version]
- Yamada, N.; Yamaya, M.; Okinaga, S.; Nakayama, K.; Sekizawa, K.; Shibahara, S.; Sasaki, H. Microsatellite polymorphism in the heme oxygenase-1 gene promoter is associated with susceptibility to emphysema. Am. J. Hum. Genet. 2000, 66, 187–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idriss, N.K.; Blann, A.D.; Lip, G.Y. Hemoxygenase-1 in cardiovascular disease. J. Am. Coll. Cardiol. 2008, 52, 971–978. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Song, F.F.; Huang, Y.B.; Zheng, H.; Song, F.J.; Chen, K.X. Association between the (GT)n polymorphism of the HO-1 gene promoter region and cancer risk: A meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 4617–4622. [Google Scholar] [CrossRef] [Green Version]
- Chau, L.Y. Heme oxygenase-1: Emerging target of cancer therapy. J. Biomed. Sci 2015, 22, 22. [Google Scholar] [CrossRef] [Green Version]
- Bukowska-Strakova, K.; Wlodek, J.; Pitera, E.; Kozakowska, M.; Konturek-Ciesla, A.; Ciesla, M.; Gonka, M.; Nowak, W.; Wieczorek, A.; Pawinska-Wasikowska, K.; et al. Role of HMOX1 promoter genetic variants in chemoresistance and chemotherapy induced neutropenia in children with acute lymphoblastic leukemia. Int. J. Mol. Sci. 2021, 22, 988. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; Khosravian, F.; Sameti, A.A.; Moafi, A.; Merasi, M.R.; Salehi, M.; Nejati, M.; Behjati, M. Association between (GT)n repeats in heme oxygenase-1 gene promoter and 3-year survival of patients with acute leukemia: A controlled, cross-sectional study. Int. J. Hematol. Oncol. Stem Cell Res. 2018, 12, 49–56. [Google Scholar] [PubMed]
- Wu, M.M.; Lee, C.H.; Hsu, L.I.; Cheng, W.F.; Lee, T.C.; Wang, Y.H.; Chiou, H.Y.; Chen, C.J. Effect of heme oxygenase-1 gene promoter polymorphism on cancer risk by histological subtype: A prospective study in arseniasis-endemic areas in Taiwan. Int. J. Cancer 2016, 138, 1875–1886. [Google Scholar] [CrossRef] [Green Version]
- Farombi, E.O.; Surh, Y.J. Heme oxygenase-1 as a potential therapeutic target for hepatoprotection. J. Biochem. Mol. Biol. 2006, 39, 479–491. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Grenard, P.; Nhieu, J.T.; Julien, B.; Mallat, A.; Habib, A.; Lotersztajn, S. Heme oxygenase-1 is an antifibrogenic protein in human hepatic myofibroblasts. Gastroenterology 2003, 125, 460–469. [Google Scholar] [CrossRef]
- Protzer, U.; Seyfried, S.; Quasdorff, M.; Sass, G.; Svorcova, M.; Webb, D.; Bohne, F.; Hosel, M.; Schirmacher, P.; Tiegs, G. Antiviral activity and hepatoprotection by heme oxygenase-1 in hepatitis B virus infection. Gastroenterology 2007, 133, 1156–1165. [Google Scholar] [CrossRef]
- Yu, J.; Chu, E.S.; Wang, R.; Wang, S.; Wu, C.W.; Wong, V.W.; Chan, H.L.; Farrell, G.C.; Sung, J.J. Heme oxygenase-1 protects against steatohepatitis in both cultured hepatocytes and mice. Gastroenterology 2010, 138, 694–704. [Google Scholar] [CrossRef]
- Sass, G.; Soares, M.C.; Yamashita, K.; Seyfried, S.; Zimmermann, W.H.; Eschenhagen, T.; Kaczmarek, E.; Ritter, T.; Volk, H.D.; Tiegs, G. Heme oxygenase-1 and its reaction product, carbon monoxide, prevent inflammation-related apoptotic liver damage in mice. Hepatology 2003, 38, 909–918. [Google Scholar] [CrossRef]
- Lehmann, E.; El-Tantawy, W.H.; Ocker, M.; Bartenschlager, R.; Lohmann, V.; Hashemolhosseini, S.; Tiegs, G.; Sass, G. The heme oxygenase 1 product biliverdin interferes with hepatitis C virus replication by increasing antiviral interferon response. Hepatology 2010, 51, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Wilson, A.T.; Luxon, B.A.; Brown, K.E.; Mathahs, M.M.; Bandyopadhyay, S.; McCaffrey, A.P.; Schmidt, W.N. Biliverdin inhibits hepatitis C virus nonstructural 3/4A protease activity: Mechanism for the antiviral effects of heme oxygenase? Hepatology 2010, 52, 1897–1905. [Google Scholar] [CrossRef] [Green Version]
- Rehermann, B.; Nascimbeni, M. Immunology of hepatitis B virus and hepatitis C virus infection. Nat. Rev. Immunol. 2005, 5, 215–229. [Google Scholar] [CrossRef]
- Zou, C.; Zhang, H.; Li, Q.; Xiao, H.; Yu, L.; Ke, S.; Zhou, L.; Liu, W.; Wang, W.; Huang, H.; et al. Heme oxygenase-1: A molecular brake on hepatocellular carcinoma cell migration. Carcinogenesis 2011, 32, 1840–1848. [Google Scholar] [CrossRef] [Green Version]
- Bonkovsky, H.L.; Lambrecht, R.W.; Naishadham, D. Genetic variations in heme oxygenase-1 and chronic hepatitis. Hepatology 2010, 52, 400–401. [Google Scholar] [CrossRef]
- Lemaire, A.; Trepo, E.; Ouziel, R.; Gustot, T.; Moreno, C.; Degre, D.; Minsart, C.; Quertinmont, E.; Vercruysse, V.; De Wilde, V.; et al. Microsatellite polymorphism in the heme oxygenase-1 gene promoter is not associated with alcoholic liver disease severity. Hepatology 2014, 59, 352–353. [Google Scholar] [CrossRef]
- Urbanek, P.; Lenicek, M.; Muchova, L.; Subhanova, I.; Dusek, L.; Kasprikova, N.; Hrabal, P.; Bruha, R.; Vitek, L. No association of promoter variations of HMOX1 and UGT1A1 genes with liver injury in chronic hepatitis C. Ann. Hepatol. 2011, 10, 445–451. [Google Scholar] [CrossRef]
- Chen, C.J.; Hsu, L.I.; Wang, C.H.; Shih, W.L.; Hsu, Y.H.; Tseng, M.P.; Lin, Y.C.; Chou, W.L.; Chen, C.Y.; Lee, C.Y.; et al. Biomarkers of exposure, effect, and susceptibility of arsenic-induced health hazards in Taiwan. Toxicol. Appl. Pharmacol. 2005, 206, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.I.; Wang, Y.H.; Hsieh, F.I.; Yang, T.Y.; Wen-Juei Jeng, R.; Liu, C.T.; Chen, C.L.; Hsu, K.H.; Chiou, H.Y.; Wu, M.M.; et al. Effects of arsenic in drinking water on risk of hepatitis or cirrhosis in persons with and without chronic viral hepatitis. Clin. Gastroenterol. Hepatol. 2016, 14, 1347–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC. Some drinking-water disinfectants and contaminants, including arsenic. In IARC Monographs on the Evaluation of the Carcinogenic Risks of Chemicals to Humans; International Agency for Research on Cancer: Lyon, France, 2004; Volume 84, pp. 1–477. [Google Scholar]
- Wu, M.M.; Chiou, H.Y.; Lee, T.C.; Chen, C.L.; Hsu, L.I.; Wang, Y.H.; Huang, W.L.; Hsieh, Y.C.; Yang, T.Y.; Lee, C.Y.; et al. GT-repeat polymorphism in the heme oxygenase-1 gene promoter and the risk of carotid atherosclerosis related to arsenic exposure. J. Biomed. Sci. 2010, 17, 70. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.L.; Hsu, L.I.; Chiou, H.Y.; Hsueh, Y.M.; Chen, S.Y.; Wu, M.M.; Chen, C.J. Ingested arsenic, cigarette smoking, and lung cancer risk: A follow-up study in arseniasis-endemic areas in Taiwan. JAMA 2004, 292, 2984–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.J.; Kuo, T.L.; Wu, M.M. Arsenic and cancers. Lancet 1988, 1, 414–415. [Google Scholar] [CrossRef]
- Tseng, W.P.; Chu, H.M.; How, S.W.; Fong, J.M.; Lin, C.S.; Yeh, S. Prevalence of skin cancer in an endemic area of chronic arsenicism in Taiwan. J. Natl. Cancer Inst. 1968, 40, 453–463. [Google Scholar] [PubMed]
- Wu, M.M.; Kuo, T.L.; Hwang, Y.H.; Chen, C.J. Dose-response relation between arsenic concentration in well water and mortality from cancers and vascular diseases. Am. J. Epidemiol. 1989, 130, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Chuang, Y.C.; Lin, T.M.; Wu, H.Y. Malignant neoplasms among residents of a blackfoot disease-endemic area in Taiwan: High-arsenic artesian well water and cancers. Cancer Res. 1985, 45, 5895–5899. [Google Scholar] [PubMed]
- Chen, C.L.; Chiou, H.Y.; Hsu, L.I.; Hsueh, Y.M.; Wu, M.M.; Chen, C.J. Ingested arsenic, characteristics of well water consumption and risk of different histological types of lung cancer in northeastern Taiwan. Environ. Res. 2010, 110, 455–462. [Google Scholar] [CrossRef]
- Chen, C.L.; Chiou, H.Y.; Hsu, L.I.; Hsueh, Y.M.; Wu, M.M.; Wang, Y.H.; Chen, C.J. Arsenic in drinking water and risk of urinary tract cancer: A follow-up study from northeastern Taiwan. Cancer Epidemiol. Biomark. Prev. 2010, 19, 101–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiou, H.Y.; Chiou, S.T.; Hsu, Y.H.; Chou, Y.L.; Tseng, C.H.; Wei, M.L.; Chen, C.J. Incidence of transitional cell carcinoma and arsenic in drinking water: A follow-up study of 8102 residents in an arseniasis-endemic area in northeastern Taiwan. Am. J. Epidemiol. 2001, 153, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.M.; Chiou, H.Y.; Chen, C.L.; Wang, Y.H.; Hsieh, Y.C.; Lien, L.M.; Lee, T.C.; Chen, C.J. GT-repeat polymorphism in the heme oxygenase-1 gene promoter is associated with cardiovascular mortality risk in an arsenic-exposed population in northeastern Taiwan. Toxicol. Appl. Pharmacol. 2010, 248, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Kimpara, T.; Takeda, A.; Watanabe, K.; Itoyama, Y.; Ikawa, S.; Watanabe, M.; Arai, H.; Sasaki, H.; Higuchi, S.; Okita, N.; et al. Microsatellite polymorphism in the human heme oxygenase-1 gene promoter and its application in association studies with Alzheimer and Parkinson disease. Hum. Genet. 1997, 100, 145–147. [Google Scholar] [CrossRef]
- Chen, Y.H.; Lin, S.J.; Lin, M.W.; Tsai, H.L.; Kuo, S.S.; Chen, J.W.; Charng, M.J.; Wu, T.C.; Chen, L.C.; Ding, Y.A.; et al. Microsatellite polymorphism in promoter of heme oxygenase-1 gene is associated with susceptibility to coronary artery disease in type 2 diabetic patients. Hum. Genet. 2002, 111, 1–8. [Google Scholar] [CrossRef]
- TCRTF. Cancer Registry Annual Report; Bureau of Health Promotion, Department of Health, The Executive Yuan: Taipei, Taiwan, 2008. [Google Scholar]
- Wold Health Organization. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Tseng, W.P. Effects and dose-response relationships of skin cancer and blackfoot disease with arsenic. Environ. Health Perspect. 1977, 19, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Kah, J.; Volz, T.; Lutgehetmann, M.; Groth, A.; Lohse, A.W.; Tiegs, G.; Sass, G.; Dandri, M. Haem oxygenase-1 polymorphisms can affect HCV replication and treatment responses with different efficacy in humanized mice. Liver Int. 2017, 37, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Taha, H.; Skrzypek, K.; Guevara, I.; Nigisch, A.; Mustafa, S.; Grochot-Przeczek, A.; Ferdek, P.; Was, H.; Kotlinowski, J.; Kozakowska, M.; et al. Role of heme oxygenase-1 in human endothelial cells: Lesson from the promoter allelic variants. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1634–1641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.M.; Chiou, H.Y.; Ho, I.C.; Chen, C.J.; Lee, T.C. Gene expression of inflammatory molecules in circulating lymphocytes from arsenic-exposed human subjects. Environ. Health Perspect. 2003, 111, 1429–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | L/L Genotypes 1 (n = 328) | L/S Genotypes (n = 569) | S/S Genotypes (n = 256) | p-Value 3 |
|---|---|---|---|---|
| Mean age, year | 54.9 (11.5) 2 | 56.1 (11.4) | 55.7 (10.5) | 0.362 |
| Male gender, n | 145 (44.2) | 262 (46.1) | 115 (44.9) | 0.861 |
| Education level, n | 0.167 | |||
| No schooling | 110 (33.5) | 207 (36.4) | 111 (43.4) | |
| Elementary | 172 (52.4) | 283 (49.8) | 111 (43.4) | |
| Junior high or above | 46 (14.0) | 78 (13.7) | 34 (13.3) | |
| Cigarette smokers, yes | 85 (25.9) | 165 (29.0) | 67 (26.2) | 0.652 |
| Alcohol drinkers, yes | 46 (14.0) | 92 (16.2) | 33 (12.9) | 0.728 |
| Body mass index, kg/m2 | 0.370 | |||
| <27 | 110 (33.7) | 221 (39.3) | 94 (37.0) | |
| 23–27 | 151 (46.3) | 229 (40.8) | 101 (40.1) | |
| ≥27 | 65 (19.9) | 112 (19.9) | 57 (22.6) | |
| Total cholesterol, mg/dL | 0.966 | |||
| ≥240 | 113 (34.6) | 191 (33.7) | 86 (34.0) | |
| Triglyceride, mg/dL | 0.202 | |||
| ≥150 | 98 (30.0) | 140 (24.7) | 72 (28.5) | |
| Arsenic exposure, μg/L | 0.319 | |||
| Median (IQR) | 357 (76 to 700) | 270 (74 to 700) | 260 (85 to 700) | |
| 0–50 | 46 (16.0) | 73 (14.6) | 25 (12.0) | |
| 50–150 | 73 (25.4) | 141 (28.3) | 65 (31.1) | |
| 150–300 | 15 (5.2) | 43 (8.6) | 9 (4.3) | |
| 300–750 | 91 (31.7) | 143 (28.7) | 64 (30.6) | |
| >750 | 62 (21.6) | 99 (19.8) | 46 (22.0) | |
| Liver cancer (T155.0) 4 | ||||
| Cases number (n = 29) | 7 | 11 | 11 | |
| Person-years | 5911.5 | 10,213.3 | 4344.9 | |
| Incidence rate per 105 | 118.4 | 107.7 | 253.2 |
| Age-Gender-Adjusted | Multivariate-Adjusted 2 | |||
|---|---|---|---|---|
| Characteristics | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age, year | 1.05 (1.01–1.09) | 0.007 1 | 1.04 (1.00–1.09) | 0.049 |
| Gender | ||||
| Females | 1.00 | 1.00 | ||
| Males | 4.23 (1.80–9.91) | 0.001 | 2.78 (0.77–10.0) | 0.118 |
| Education level | ||||
| No school | 1.00 | 1.00 | ||
| Elementary | 1.19 (0.49–2.86) | 0.704 | 0.86 (0.33–2.26) | 0.759 |
| Cigarette smoking | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.66 (0.66–4.14) | 0.280 | 2.68 (0.94–7.63) | 0.066 |
| Alcohol consumption | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.47 (0.16–1.41) | 0.178 | 0.51 (0.17–1.58) | 0.244 |
| Body mass index, kg/m2 | ||||
| <27 | 1.00 | 1.00 | ||
| ≥27 | 1.41 (0.60–3.31) | 0.438 | 1.14 (0.41–3.16) | 0.805 |
| Total cholesterol, mg/dL | ||||
| <240 | 1.00 | 1.00 | ||
| ≥240 | 0.74 (0.32–1.71) | 0.485 | 0.83 (0.33–2.08) | 0.689 |
| Triglyceride, mg/dL | ||||
| <150 | 1.00 | 1.00 | ||
| ≥150 | 1.05 (0.48–2.31) | 0.905 | 1.15 (0.48–2.75) | 0.758 |
| Arsenic exposure, μg/L | ||||
| ≤300 | 1.00 | 1.00 | ||
| 300–750 | 1.38 (0.53–3.59) | 0.505 | 1.38 (0.52–3.67) | 0.515 |
| >750 | 1.28 (0.43–3.80) | 0.660 | 1.06 (0.33–3.38) | 0.923 |
| All Study Subjects | Subjects without HBV/HCV (+) | |||
|---|---|---|---|---|
| HO-1 Genotype 2 | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Additive model | ||||
| L/L | 1.00 | 1.00 | ||
| L/S | 1.36 (0.42–4.37) | 0.605 | 1.06 (0.19–5.84) | 0.945 |
| S/S | 3.78 (1.18–12.13) | 0.025 | 5.06 (1.01–25.42) | 0.049 |
| Trend test | 2.11 (1.16–3.87) | 0.015 | 2.79 (1.14–6.82) | 0.025 |
| Dominant model | ||||
| L/L | 1.00 | 1.00 | ||
| L/S or S/S | 2.01 (0.68–5.39) | 0.204 | 2.02 (0.44–9.27) | 0.367 |
| Recessive model | ||||
| L/L or L/S | 1.00 | 1.00 | ||
| S/S | 3.07 (1.35–6.95) | 0.007 | 4.86 (1.55–15.27) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-M.; Hsieh, F.-I.; Hsu, L.-I.; Lee, T.-C.; Chiou, H.-Y.; Chen, C.-J. GT-Repeat Polymorphism in the HO-1 Gene Promoter Is Associated with Risk of Liver Cancer: A Follow-Up Study from Arseniasis-Endemic Areas in Taiwan. J. Clin. Med. 2021, 10, 1489. https://doi.org/10.3390/jcm10071489
Wu M-M, Hsieh F-I, Hsu L-I, Lee T-C, Chiou H-Y, Chen C-J. GT-Repeat Polymorphism in the HO-1 Gene Promoter Is Associated with Risk of Liver Cancer: A Follow-Up Study from Arseniasis-Endemic Areas in Taiwan. Journal of Clinical Medicine. 2021; 10(7):1489. https://doi.org/10.3390/jcm10071489
Chicago/Turabian StyleWu, Meei-Maan, Fang-I Hsieh, Ling-I Hsu, Te-Chang Lee, Hung-Yi Chiou, and Chien-Jen Chen. 2021. "GT-Repeat Polymorphism in the HO-1 Gene Promoter Is Associated with Risk of Liver Cancer: A Follow-Up Study from Arseniasis-Endemic Areas in Taiwan" Journal of Clinical Medicine 10, no. 7: 1489. https://doi.org/10.3390/jcm10071489
APA StyleWu, M. -M., Hsieh, F. -I., Hsu, L. -I., Lee, T. -C., Chiou, H. -Y., & Chen, C. -J. (2021). GT-Repeat Polymorphism in the HO-1 Gene Promoter Is Associated with Risk of Liver Cancer: A Follow-Up Study from Arseniasis-Endemic Areas in Taiwan. Journal of Clinical Medicine, 10(7), 1489. https://doi.org/10.3390/jcm10071489