
Retinal Vascularization Analysis on Optical Coherence Tomography Angiography before and after Intraretinal or Subretinal Fluid Resorption in Exudative Age-Related Macular Degeneration: A Pilot Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Follow-Up
2.2. Data Collection
2.3. OCTA Acquisition
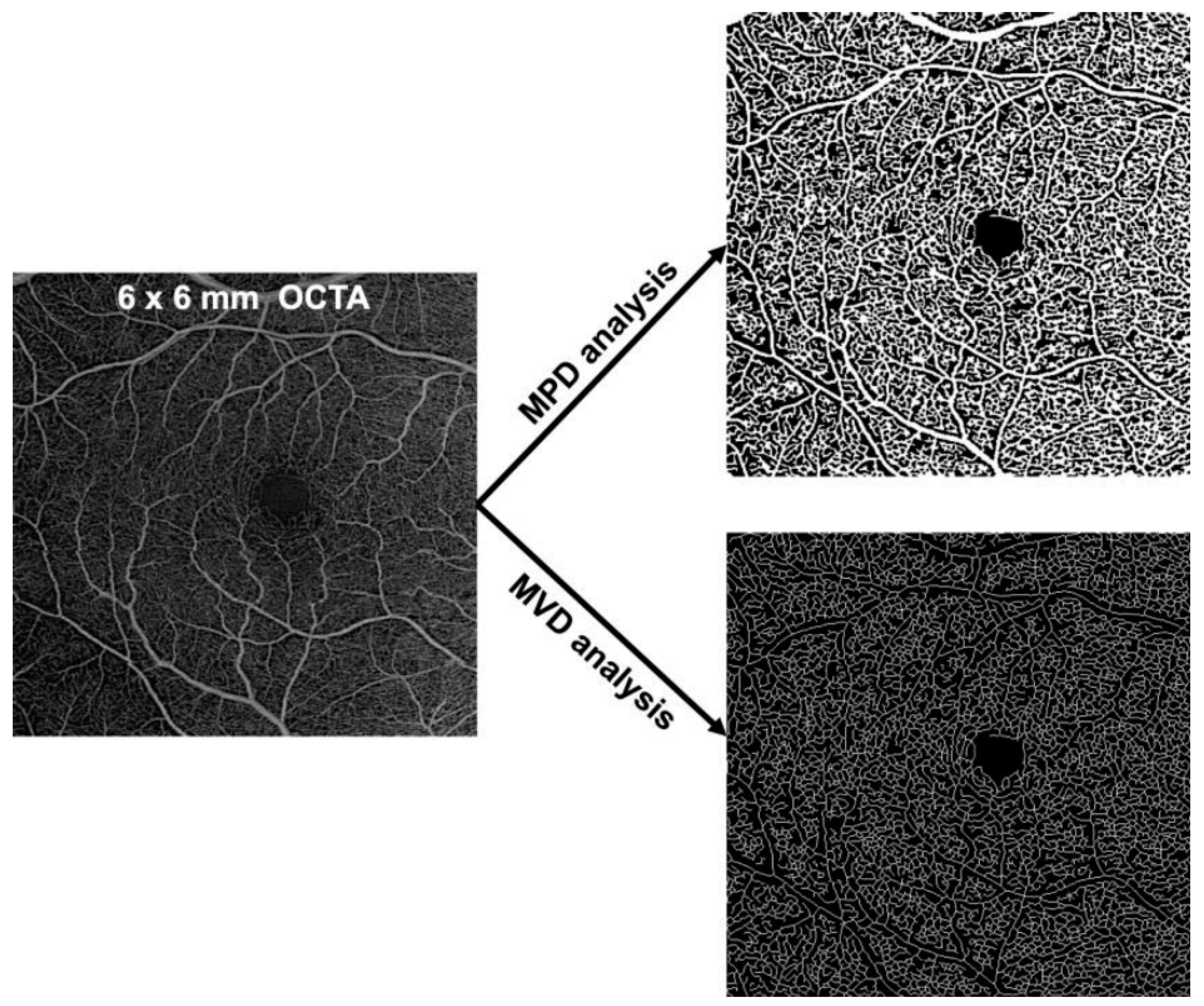
2.4. Image Analysis
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Mean Perfusion Density (MPD) and Mean Vascular Density (MVD) at Baseline
3.2. Effect of Treatment/Time on Mean Perfusion Density (MPD) and Mean Vascular Density (MVD)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klein, R.; Peto, T.; Bird, A.; Vannewkirk, M.R. The epidemiology of age-related macular degeneration. Am. J. Ophthalmol. 2004, 137, 486–495. [Google Scholar] [CrossRef]
- Nowak, J.Z. Age-related macular degeneration (AMD): Pathogenesis and therapy. Pharmacol. Rep. 2006, 58, 353–363. [Google Scholar]
- Ashraf, M.; Souka, A.; Adelman, R.A. Age-related macular degeneration: Using morphological predictors to modify current treatment protocols. Acta Ophthalmol. 2018, 96, 120–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt-Erfurth, U.; Waldstein, S.M.; Deak, G.-G.; Kundi, M.; Simader, C. Pigment epithelial detachment followed by retinal cystoid degeneration leads to vision loss in treatment of neovascular age-related macular degeneration. Ophthalmology 2015, 122, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Ting, T.D.; Oh, M.; Cox, T.A.; Meyer, C.H.; Toth, C.A. Decreased visual acuity associated with cystoid macular edema in neovascular age-related macular degeneration. Arch. Ophthalmol. 2002, 120, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.-R.; Omri, S.; Gélizé, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef] [PubMed]
- Rochepeau, C.; Kodjikian, L.; Garcia, M.-A.; Coulon, C.; Burillon, C.; Denis, P.; Delaunay, B.; Mathis, T. OCT-Angiography Quantitative Assessment of Choriocapillaris Blood Flow in Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2018, 194, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Mané, V.; Dupas, B.; Gaudric, A.; Bonnin, S.; Pedinielli, A.; Bousquet, E.; Erginay, A.; Tadayoni, R.; Couturier, A. Correlation between cystoid spaces in chronic diabetic macular edema and capillary nonperfusion detected by optical coherence tomography angiography. Retina 2016, 36 (Suppl. 1), S102–S110. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Cai, X.; Zhang, S.; Su, L.; Chen, H.; Lin, Y.; Sun, L.; Chen, G.; Zhong, L.; Jin, C.; et al. Quantitative Analysis of Retinal Microvascular Changes after Conbercept Therapy in Branch Retinal Vein Occlusion Using Optical Coherence Tomography Angiography. Ophthalmologica 2019, 242, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Chetrit, M.; Bonnin, S.; Mané, V.; Erginay, A.; Tadayoni, R.; Gaudric, A.; Couturier, A. Acute pseudophakic cystoid macular edema imaged by optical coherence tomography angiography. Retina 2018, 38, 2073–2080. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, E.; Frizziero, L.; Daniele, A.R.; Convento, E.; Longhin, E.; Guidolin, F.; Parrozzani, R.; Cavarzeran, F.; Midena, E. Early OCT angiography changes of type 1 CNV in exudative AMD treated with anti-VEGF. Br. J. Ophthalmol. 2019, 103, 67–71. [Google Scholar] [CrossRef] [PubMed]
- McClintic, S.M.; Gao, S.; Wang, J.; Hagag, A.; Lauer, A.K.; Flaxel, C.J.; Bhavsar, K.; Hwang, T.S.; Huang, D.; Jia, Y.; et al. Quantitative Evaluation of Choroidal Neovascularization under Pro Re Nata Anti-Vascular Endothelial Growth Factor Therapy with OCT Angiography. Ophthalmol. Retin. 2018, 2, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Cho, H.J.; Kim, Y.; Jung, S.H.; Lee, D.W.; Kim, J.W. Responses of Types 1 and 2 Neovascularization in Age-Related Macular Degeneration to Anti-Vascular Endothelial Growth Factor Treatment: Optical Coherence Tomography Angiography Analysis. Semin. Ophthalmol. 2019, 34, 168–176. [Google Scholar] [CrossRef]
- Freund, K.B.; Zweifel, S.A.; Engelbert, M. Do we need a new classification for choroidal neovascularization in age-related macular degeneration? Retina 2010, 30, 1333–1349. [Google Scholar] [CrossRef]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.K.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- Eastline, M.; Munk, M.R.; Wolf, S.; Schaal, K.B.; Ebneter, A.; Tian, M.; Giannakaki-Zimmermann, H.; Zinkernagel, M.S. Repeatability of Wide-field Optical Coherence Tomography Angiography in Normal Retina. Transl. Vis. Sci. Technol. 2019, 8, 6. [Google Scholar] [CrossRef]
- Bagherinia, H.; Knighton, R.W.; Sisternes, L.D.; Chen, M.H.; Durbin, M.K. A Fast Method to Reduce Decorrelation Tail Artifacts in OCT Angiography. Investig. Ophthalmol. Vis. Sci. 2017, 58, 643. [Google Scholar]
- Wang, J.J.; Mitchell, P.; Rochtchina, E.; Tan, A.G.; Wong, T.Y.; Klein, R. Retinal vessel wall signs and the 5 year incidence of age related maculopathy: The Blue Mountains Eye Study. Br. J. Ophthalmol. 2004, 88, 104–109. [Google Scholar] [CrossRef]
- Kornzweig, A.L.; Eliasoph, I.; Feldstein, M. The retinal vasculature in macular degeneration. Arch. Ophthalmol. 1966, 75, 326–333. [Google Scholar] [CrossRef]
- Chakravarthy, U.; Wong, T.Y.; Fletcher, A.; Piault, E.; Evans, C.; Zlateva, G.; Buggage, R.; Pleil, A.M.; Mitchell, P. Clinical risk factors for age-related macular degeneration: A systematic review and meta-analysis. BMC Ophthalmol. 2010, 10, 31. [Google Scholar] [CrossRef]
- Klein, R.; Clegg, L.; Cooper, L.S.; Hubbard, L.D.; Klein, B.E.; King, W.N.; Folsom, A.R. Prevalence of age-related maculopathy in the Atherosclerosis Risk in Communities Study. Arch. Ophthalmol. 1999, 117, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- Toto, L.; Borrelli, E.; Mastropasqua, R.; Di Antonio, L.; Doronzo, E.; Carpineto, P.; Mastropasqua, L. Association between outer retinal alterations and microvascular changes in intermediate stage age-related macular degeneration: An optical coherence tomography angiography study. Br. J. Ophthalmol. 2017, 101, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Scharf, J.; Corradetti, G.; Corvi, F.; Sadda, S.; Sarraf, D. Optical Coherence Tomography Angiography of the Choriocapillaris in Age-Related Macular Degeneration. J. Clin. Med. 2021, 10, 751. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Rabiolo, A.; Sacconi, R.; Lamanna, F.; Querques, L.; Bandello, F.; Querques, G. Retinal vascular alterations in reticular pseudodrusen with and without outer retinal atrophy assessed by optical coherence tomography angiography. Br. J. Ophthalmol. 2018, 102, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- You, Q.S.; Wang, J.; Guo, Y.; Flaxel, C.J.; Hwang, T.S.; Huang, D.; Jia, Y.; Bailey, S.T. Detection of Reduced Retinal Vessel Density in Eyes with Geographic Atrophy Secondary to Age-Related Macular Degeneration Using Projection-Resolved Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2020, 209, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Feigl, B. Age-related maculopathy—linking aetiology and pathophysiological changes to the ischaemia hypothesis. Prog. Retin. Eye Res. 2009, 28, 63–86. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Retinal vascular cystoid macular edema: Review and New Theory. Retina 2016, 36, 1823–1842. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A. Gass’ Atlas of Macular Diseases E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; p. 1357. [Google Scholar]
- Waldstein, S.M.; Simader, C.; Staurenghi, G.; Chong, N.V.; Mitchell, P.; Jaffe, G.J.; Lu, C.; Katz, T.A.; Schmidt-Erfurth, U. Morphology and Visual Acuity in Aflibercept and Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration in the VIEW Trials. Ophthalmology 2016, 123, 1521–1529. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Lee, K.; Zhang, L.; Sonka, M.; Abràmoff, M.D. Stratified Sampling Voxel Classification for Segmentation of Intraretinal and Subretinal Fluid in Longitudinal Clinical OCT Data. IEEE Trans. Med. Imaging 2015, 34, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Waldstein, S.M.; Philip, A.-M.; Leitner, R.; Simader, C.; Langs, G.; Gerendas, B.S.; Schmidt-Erfurth, U. Correlation of 3-Dimensionally Quantified Intraretinal and Subretinal Fluid With Visual Acuity in Neovascular Age-Related Macular Degeneration. JAMA Ophthalmol. 2016, 134, 182–190. [Google Scholar] [CrossRef]
- Wickremasinghe, S.S.; Janakan, V.; Sandhu, S.S.; Amirul-Islam, F.M.; Abedi, F.; Guymer, R.H. Implication of recurrent or retained fluid on optical coherence tomography for visual acuity during active treatment of neovascular age-related macular degeneration with a treat and extend protocol. Retina 2016, 36, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Chang, H.R.; Song, S. Ischaemic change after intravitreal bevacizumab (Avastin) injection for macular oedema secondary to non-ischaemic central retinal vein occlusion. Acta Ophthalmol. 2008, 86, 925–927. [Google Scholar] [CrossRef]
- Kim, S.W.; Woo, J.E.; Yoon, Y.S.; Lee, S.; Woo, J.M.; Min, J.K. Retinal and Choroidal Changes after Anti Vascular Endothelial Growth Factor Therapy for Neovascular Age-related Macular Degeneration. Curr. Pharm. Des. 2019, 25, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, D.N.; Mendrinos, E.; Mangioris, G.; Donati, G.; Pournaras, C.J. Intravitreal ranibizumab may induce retinal arteriolar vasoconstriction in patients with neovascular age-related macular degeneration. Ophthalmology. 2009, 116, 1755–1761. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Toto, L.; Borrelli, E.; Carpineto, P.; Di Antonio, L.; Mastropasqua, R. Optical coherence tomography angiography assessment of vascular effects occurring after aflibercept intravitreal injections in treatment-naive patients with wet age-related macular degeneration. Retina 2017, 37, 247–256. [Google Scholar] [CrossRef]
- Sampson, D.M.; Gong, P.; An, D.; Menghini, M.; Hansen, A.; Mackey, D.A.; Sampson, D.D.; Chen, F.K. Axial Length Variation Impacts on Superficial Retinal Vessel Density and Foveal Avascular Zone Area Measurements Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3065–3072. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K. Image artifacts in optical coherence tomography angiography. Retina 2015, 35, 2163–2180. [Google Scholar] [CrossRef]
- Loria, O.; Kodjikian, L.; Denis, P.; Vartin, C.; Dimassi, S.; Gervolino, L.; Maignan, A.; Kermarrec, R.; Chambard, C.; Pradat, P.; et al. Quantitative analysis of choriocapillaris alterations in swept source OCT angiography in diabetic patients. Retina 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| IRF ± SRF Group (n = 22) | SRF Group (n = 11) | Healthy Group (n = 11) | |
|---|---|---|---|
| Mean age, years (SD) | 81.7 (8.3) | 79.9 (5.8) | 78.6 (2.8) |
| Sex (male/female), n | 5/17 | 5/6 | 6/5 |
| Laterality (R/L), n | 10/12 | 7/4 | 5/6 |
| Mean disease duration, months (SD) | 22.6 (26.1) | 33.7 (29.3) | - |
| Mean duration between T0 and T1, months (SD) | 2.7 (1.7) | 1.2 (0.4) | - |
| Mean number of IVI before inclusion, n (SD) | 9.1 (11.8) | 18.6 (16.9) | - |
| Mean number of IVI between T0 and T1, n (SD) | 2.0 (1.0) | 1.3 (0.5) | - |
| Treatment regimen, n (%) Pro re nata Treat and Extend Treatment-naive | 7 (31.8) 7 (31.8) 8 (36.4) | 1 (9.1) 7 (63.6) 3 (27.3) | - |
| Presence of SRF, n (%) | 6 (27.3) | 11 (100) | - |
| Presence of IRF, n (%) | 22 (100) | 0 (0) | - |
| Presence of atrophy, n (%) | 13 (59.1) | 2 (18.2) | - |
| Presence of fibrosis, n (%) | 8 (36.4) | 1 (9.0) | - |
| Mean BCVA at T0, ETDRS (SD) | 56.8 (19.7) | 72.0 (15.5) | - |
| Mean BCVA at T1, ETDRS (SD) | 58.1 (19.8) | 72.7 (16.0) | - |
| Type of anti-VEGF, n (%) Aflibercept Ranibizumab | 19 (86.4) 3 (13.6) | 11 (100) 0 (0) | - |
| MPD SCP | ||||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| Estimate (95%CI) | p-Value | Estimate (95%CI) | p-Value | |
| Fluid group | ||||
| Healthy | Ref | Ref | ||
| IRF ± SRF | −7.0 (−9.6, −4.6) | <0.001 | −5.7 (−8.7, −2.7) | <0.001 |
| SRF | −2.2 (−5.1, 0.7) | 0.13 | −1.8 (−4.7, 1.1) | 0.2 |
| Age | −0.2 (−0.4, 0.01) | 0.061 | −0.1 (−0.3, 0.05) | 0.2 |
| Sex (Male) | 2.1 (−0.7, 4.9) | 0.14 | - | - |
| Disease duration | −0.02 (−0.08, 0.04) | 0.5 | - | - |
| Number of IVI | 0.02 (−0.09, 0.1) | 0.7 | - | - |
| Atrophy | −2.8 (−5.7, 0.1) | 0.062 | −0.7 (−3.4, 1.9) | 0.6 |
| Fibrosis | −3.3 (−6.5, −0.07) | 0.045 | −1.7 (−4.6, 1.2) | 0.2 |
| MNV subtype | ||||
| Type 1 | Ref | |||
| Type 2 | −1.5 (−6.3, 3.4) | 0.5 | - | - |
| Type 3 | 1.3 (−2.1, 4.7) | 0.4 | - | - |
| Anti-VEGF | ||||
| Aflibercept | Ref | |||
| Lucentis | 0.4 (−5.0, 5.7) | 0.9 | - | - |
| Treatment | ||||
| Naive | Ref | |||
| PRN | −0.4 (−4.6, 3.7) | 0.8 | - | - |
| TAE | 0.8 (−2.8, 4.4) | 0.6 | - | - |
| MVD SCP | ||||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| Estimate (95%CI) | p-Value | Estimate (95%CI) | p-Value | |
| Fluid group | ||||
| Healthy | Ref | Ref | ||
| IRF ± SRF | −3.1 (−4.3, −1.9) | <0.001 | −2.4 (−3.8, −0.9) | 0.002 |
| SRF | −0.9 (−2.3, 0.5) | 0.2 | −0.7 (−2.1, 0.7) | 0.3 |
| Age | −0.07 (−0.2, 0.02) | 0.14 | −0.03 (−0.1, 0.04) | 0.4 |
| Sex (Male) | 1.0 (−0.3, 2.3) | 0.14 | - | - |
| Disease duration | −0.01 (−0.03, 0.02) | 0.6 | - | - |
| Number of IVI | 0.01 (−0.04, 0.07) | 0.6 | - | - |
| Atrophy | −1.4 (−2.8, −0.01) | 0.048 | −0.4 (−1.7, 0.9) | 0.5 |
| Fibrosis | −1.7 (−3.2, −0.1) | 0.032 | −0.9 (−2.3, 0.5) | 0.2 |
| MNV subtype | ||||
| Type 1 | Ref | |||
| Type 2 | −0.9 (−3.2, 1.3) | 0.4 | - | - |
| Type 3 | 0.9 (−0.7, 2.5) | 0.3 | - | - |
| Anti-VEGF | ||||
| Aflibercept | Ref | |||
| Lucentis | 0.4 (−2.2, 2.9) | 0.8 | - | - |
| Treatment | ||||
| Naive | Ref | |||
| PRN | −0.07 (−2.0, 1.9) | >0.9 | - | - |
| TAE | 0.8 (−1.3, 2.1) | 0.6 | - | - |
| MPD DCP | ||||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| Estimate (95%CI) | p-Value | Estimate (95%CI) | p-Value | |
| Fluid group | ||||
| Healthy | Ref | Ref | ||
| IRF ± SRF | −13.4 (−19.0, −8.0) | <0.001 | −13.0 (−19.0, −5.9) | <0.001 |
| SRF | −9.3 (−16.0, −3.1) | 0.004 | −9.2 (−16.0, −2.7) | 0.007 |
| Age | −0.02 (−0.4, 0.4) | >0.9 | 0.1 (−0.2, 0.5) | 0.4 |
| Sex (Male) | 4.1 (−1.5, 9.7) | 0.15 | - | - |
| Disease duration | −0.06 (−0.2, 0.04) | 0.2 | - | - |
| Number of IVI | −0.10 (−0.3, 0.1) | 0.3 | - | - |
| Atrophy | −2.9 (−8.3, 2.6) | 0.3 | −1.1 (−7.1, 4.9) | 0.7 |
| Fibrosis | −2.9 (−9.0, 3.2) | 0.3 | −1.5 (−8.0, 5.0) | 0.6 |
| MNV subtype | ||||
| Type 1 | Ref | |||
| Type 2 | −4.4 (−13.0, 4.3) | 0.3 | - | - |
| Type 3 | 2.4 (−3.6, 8.3) | 0.4 | - | - |
| Anti-VEGF | ||||
| Aflibercept | Ref | |||
| Lucentis | −1.9 (−12.0, 7.7) | 0.7 | - | - |
| Treatment | ||||
| Naive | Ref | |||
| PRN | −2.8 (−10.0, 4.6) | 0.4 | - | - |
| TAE | −1.0 (−7.4, 5.5) | 0.8 | - | - |
| MVD DCP | ||||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| Estimate (95%CI) | p-Value | Estimate (95%CI) | p-Value | |
| Fluid group | ||||
| Healthy | Ref | Ref | ||
| IRF ± SRF | −5.6 (−8.3, −3.0) | <0.001 | −5.3 (−8.6, −2.1) | 0.002 |
| SRF | −3.0 (−6.1, −0.05) | 0.046 | −2.9 (−6.1, 0.2) | 0.068 |
| Age | −0.09 (−0.3, 0.1) | 0.3 | −0.02 (−0.2, 0.1) | 0.8 |
| Sex (Male) | 1.9 (−0.7, 4.1) | 0.15 | - | - |
| Disease duration | −0.02 (−0.07, 0.03) | 0.4 | - | - |
| Number of IVI | −0.01 (−0.1, 0.09) | 0.8 | - | - |
| Atrophy | −1.3 (−4.1, 1.4) | 0.3 | −0.5 (−3.4, 2.4) | 0.7 |
| Fibrosis | −0.8 (−3.9, 2.2) | 0.6 | −0.1 (−3.0, 3.3) | >0.9 |
| MNV subtype | ||||
| Type 1 | Ref | |||
| Type 2 | −0.3 (−4.7, 4.2) | 0.9 | - | - |
| Type 3 | 0.4 (−2.6, 3.5) | 0.8 | - | - |
| Anti-VEGF | ||||
| Aflibercept | Ref | |||
| Lucentis | −2.0 (−6.7, 2.8) | 0.4 | - | - |
| Treatment | ||||
| Naive | Ref | |||
| PRN | −1.2 (−4.8, 2.4) | 0.5 | - | - |
| TAE | −1.1 (−2.1, 4.3) | 0.5 | - | - |
| T0 | T1 | Estimate (95%CI) | p-Value | |
|---|---|---|---|---|
| Healthy group SCP DCP | 44.4 ± 2.2 34.1 ± 6.1 | - | - | |
| IRF ± SRF group SCP DCP | 37.4 ± 4.1 20.7 ± 7.8 | 40.1 ± 5.8 27.5 ± 8.4 | 2.7 (0.2, 5.2) 6.8 (2.1, 11.4) | 0.048 0.009 |
| SRF group SCP DCP | 42.2 ± 2.3 24.8 ± 6.9 | 41.4 ± 3.0 23.8 ± 6.3 | −0.8 (−2.6, 0.9) −1.0 (−5.7, 3.8) | 0.36 0.64 |
| T0 | T1 | Estimate (95%CI) | p-Value | |
|---|---|---|---|---|
| Healthy group SCP DCP | 19.7 ± 1.1 16.2 ± 2.8 | - | - | |
| IRF ± SRF group SCP DCP | 16.6 ± 1.9 10.6 ± 3.7 | 18.1 ± 2.1 12.7 ± 3.6 | 1.5 (0.5, 2.4) 2.1 (−0.02, 4.34) | 0.008 0.066 |
| SRF group SCP DCP | 18.8 ± 1.3 13.2 ± 2.9 | 18.3 ± 1.5 12.2 ± 2.7 | −0.5 (−1.2, 0.4) −1.0 (−3.4, 1.6) | 0.33 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathis, T.; Dimassi, S.; Loria, O.; Sudhalkar, A.; Bilgic, A.; Denis, P.; Pradat, P.; Kodjikian, L. Retinal Vascularization Analysis on Optical Coherence Tomography Angiography before and after Intraretinal or Subretinal Fluid Resorption in Exudative Age-Related Macular Degeneration: A Pilot Study. J. Clin. Med. 2021, 10, 1524. https://doi.org/10.3390/jcm10071524
Mathis T, Dimassi S, Loria O, Sudhalkar A, Bilgic A, Denis P, Pradat P, Kodjikian L. Retinal Vascularization Analysis on Optical Coherence Tomography Angiography before and after Intraretinal or Subretinal Fluid Resorption in Exudative Age-Related Macular Degeneration: A Pilot Study. Journal of Clinical Medicine. 2021; 10(7):1524. https://doi.org/10.3390/jcm10071524
Chicago/Turabian StyleMathis, Thibaud, Sarra Dimassi, Olivier Loria, Aditya Sudhalkar, Alper Bilgic, Philippe Denis, Pierre Pradat, and Laurent Kodjikian. 2021. "Retinal Vascularization Analysis on Optical Coherence Tomography Angiography before and after Intraretinal or Subretinal Fluid Resorption in Exudative Age-Related Macular Degeneration: A Pilot Study" Journal of Clinical Medicine 10, no. 7: 1524. https://doi.org/10.3390/jcm10071524
APA StyleMathis, T., Dimassi, S., Loria, O., Sudhalkar, A., Bilgic, A., Denis, P., Pradat, P., & Kodjikian, L. (2021). Retinal Vascularization Analysis on Optical Coherence Tomography Angiography before and after Intraretinal or Subretinal Fluid Resorption in Exudative Age-Related Macular Degeneration: A Pilot Study. Journal of Clinical Medicine, 10(7), 1524. https://doi.org/10.3390/jcm10071524