
Depression Associated with Reduced Heart Rate Variability Predicts Outcome in Adult Congenital Heart Disease


Abstract
:1. Introduction
2. Methods
2.1. Measurement of Heart Rate Variability
2.2. Statistics
3. Results
3.1. Predictors of Heart Rate Variability
3.2. Adverse Events
3.3. Adverse Events Related to Reduced HRV and to Reduced HRV Comorbid with MDD
4. Discussion
4.1. Heart Rate Variability in Adult Congenital Heart Disease
4.2. Prognostic Value of Reduced Heart Rate Variability and MDD
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Westhoff-Bleck, M.; Briest, J.; Fraccarollo, D.; Hilfiker-Kleiner, D.; Winter, L.; Maske, U.E.; Busch, M.A.; Bleich, S.; Bauersachs, J.; Kahl, K.G. Mental disorders in adults with congenital heart disease: Unmet needs and impact on quality of life. J. Affect. Disord. 2016, 204, 180–186. [Google Scholar] [CrossRef]
- Kovacs, A.H.; Saidi, A.S.; Kuhl, E.A.; Sears, S.F.; Silversides, C.; Harrison, J.L.; Ong, L.; Colman, J.; Oechslin, E.; Nolan, R.P. Depression and anxiety in adult congenital heart disease: Predictors and prevalence. Int. J. Cardiol. 2009, 137, 158–164. [Google Scholar] [CrossRef]
- Bromberg, J.I.; Beasley, P.J.; D’Angelo, E.J.; Landzberg, M.; DeMaso, D.R. Depression and anxiety in adults with congenital heart disease: A pilot study. Heart Lung 2003, 32, 105–110. [Google Scholar] [CrossRef]
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Sokoreli, I.; Pauws, S.C.; Steyerberg, E.W.; De Vries, G.-J.; Riistama, J.M.; Tesanovic, A.; Kazmi, S.; Pellicori, P.; Cleland, J.G.; Clark, A.L. Prognostic value of psychosocial factors for first and recurrent hospitalizations and mortality in heart failure patients: Insights from the OPERA-HF study. Eur. J. Heart Fail. 2018, 20, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Jani, B.D.; Mair, F.S.; Roger, V.L.; Weston, S.A.; Jiang, R.; Chamberlain, A.M. Comorbid Depression and Heart Failure: A Community Cohort Study. PLoS ONE 2016, 11, e0158570. [Google Scholar] [CrossRef]
- Ramos, S.; Prata, J.; Bettencourt, P.; Gonçalves, F.R.; Coelho, R. Depression predicts mortality and hospitalization in heart failure: A six-years follow-up study. J. Affect Disord. 2016, 201, 162–170. [Google Scholar] [CrossRef]
- Vader, J.M.; LaRue, S.J.; Stevens, S.R.; Mentz, R.J.; Devore, A.D.; Lala, A.; Groarke, J.D.; AbouEzzeddine, O.F.; Dunlay, S.M.; Grodin, J.L.; et al. Timing and Causes of Readmission After Acute Heart Failure Hospitalization—Insights from the Heart Failure Network Trials. J. Card. Fail. 2016, 22, 875–883. [Google Scholar] [CrossRef]
- Frasure-Smith, N.; Lespérance, F.; Habra, M.; Talajic, M.; Khairy, P.; Dorian, P.; Roy, D. Atrial Fibrillation and Congestive Heart Failure Investigators. Elevated depression symptoms predict long-term cardiovascular mortality in patients with atrial fibrillation and heart failure. Circulation 2009, 120, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Whang, W.; Albert, C.M.; Sears, S.F., Jr.; Lampert, R.; Conti, J.B.; Wang, P.J.; Singh, J.P.; Ruskin, J.N.; Muller, J.E.; Mittleman, M.A. Depression as a predictor for appropriate shocks among patients with implantable cardioverter-defibrillators: Results from the Triggers of Ventricular Arrhythmias (TOVA) study. J. Am. Coll. Cardiol. 2005, 45, 1090–1095. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.K.; O’Neal, W.T.; Diez-Roux, A.V.; Alonso, A.; Soliman, E.Z.; Heckbert, S. Negative Affect and Risk of Atrial Fibrillation: MESA. J. Am. Heart Assoc. 2019, 8, e010603. [Google Scholar] [CrossRef]
- Craney, R.M.; Freeland, K.E.; Veith, R.C. Depression, the autonomic nervous system, and coronary heart disease. Pschosomatic Med. 2005, 67 (Suppl. 1), S29–S33. [Google Scholar] [CrossRef]
- Nikolin, S.; Boonstra, T.W.; Loo, C.K.; Martin, D. Combined effect of prefrontal transcranial direct current stimulation and a working memory task on heart rate variability. PLoS ONE 2017, 12, e0181833. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Anker, S.D.; Chua, T.P.; Szelemej, R.; Piepoli, M.; Adamopoulos, S.; Webb-Peploe, K.; Harrington, D.; Banasiak, W.; Wrabec, K.; et al. Depressed heart rate variability as an independent predictor of death in chronic congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1997, 79, 1645–1650. [Google Scholar] [CrossRef]
- Walter, F.A.; Gathright, E.; Redle, J.D.; Gunstad, J.; Hughes, J.W. Depressive Symptoms are Associated with Heart Rate Variability Independently of Fitness: A Cross-Sectional Study of Patients with Heart Failure. Ann. Behav. Med. 2019, 53, 955–963. [Google Scholar] [CrossRef]
- Norrish, G.; Cantarutti, N.; Pissaridou, E.; Ridout, D.A.; Limongelli, G.; Elliott, P.M.; Kaski, J.P. Risk factors for sudden cardiac death in childhood hypertrophic cardiomyopathy: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1220–1230. [Google Scholar] [CrossRef] [Green Version]
- Doehner, W.; Ural, D.; Haeusler, K.G.; Čelutkienė, J.; Bestetti, R.; Cavusoglu, Y.; Peña-Duque, M.A.; Glavas, D.; Iacoviello, M.; Laufs, U.; et al. Heart and brain interaction in patients with heart failure: Overview and proposal for a taxonomy. A position paper from the Study Group on Heart and Brain Interaction of the Heart Failure Association. Eur. J. Heart Fail. 2017, 20, 199–215. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Huikuri, H.V.; Niemelä, M.J.; Ojala, S.; Rantala, A.; Ikäheimo, M.J.; Airaksinen, K.E. Circadian rhythms of frequency domain measures of heart rate variability in healthy subjects and patients with coronary artery disease. Effects of arousal and upright posture. Circulation 1994, 90, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohuchi, H.; Hasegawa, S.; Yasuda, K.; Yamada, O.; Ono, Y.; Echigo, S. Severely impaired cardiac autonomic nervous activity after the Fontan operation. Circulation 2001, 104, 1513–1518. [Google Scholar] [CrossRef] [Green Version]
- Davos, C.H.; Francis, D.P.; Leenarts, M.F.; Yap, S.C.; Li, W.; Davlouros, P.A.; Wensel, R.; Coats, A.J.; Piepoli, M.; Sreeram, N.; et al. Global impairment of cardiac autonomic nervous activity late after the Fontan operation. Circulation 2003, 108 (Suppl. 1), II180–II185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLeod, K.A.; Hillis, W.S.; Houston, A.B.; Wilson, N.; Trainer, A.; Neilson, J.; Doig, W.B. Reduced heart rate variability following repair of tetralogy of Fallot. Heart 1999, 81, 656–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandstra, T.; Kiès, P.; Maan, A.; Man, S.-C.; Bootsma, M.; Vliegen, H.; Egorova, A.; Mertens, B.; Holman, E.; Schalij, M.; et al. Association between reduced heart rate variability components and supraventricular tachyarrhythmias in patients with a systemic right ventricle. Auton. Neurosci. 2020, 227, 102696. [Google Scholar] [CrossRef]
- Heiberg, J.; Eckerström, F.; Rex, C.E.; Maagaard, M.; Mølgaard, H.; Redington, A.; Gatzoulis, M.; Hjortdal, V.E. Heart rate variability is impaired in adults after closure of ventricular septal defect in childhood: A novel finding associated with right bundle branch block. Int. J. Cardiol. 2019, 274, 88–92. [Google Scholar] [CrossRef]
- Moon, J.R.; Huh, J.; Song, J.; Kang, I.S.; Yang, J.H.; Jun, T.G.; Chang, S.A.; Park, S.W. Depression and Heart Rate Variability in Adults with Cyanotic Congenital Heart Disease. Circulation 2019, 140, A13169. Available online: https://www.ahajournals.org/doi/abs/10.1161/circ.140.suppl_1.13169 (accessed on 11 November 2019).
- Kourkoveli, P.; Rammos, S.; Parissis, J.; Maillis, A.; Kremastinos, D.; Paraskevaidis, I. Depressive Symptoms in Patients with Congenital Heart Disease: Incidence and Prognostic Value of Self-Rating Depression Scales. Congenit. Heart Dis. 2014, 10, 240–247. [Google Scholar] [CrossRef]
- Diller, G.-P.; Bräutigam, A.; Kempny, A.; Uebing, A.; Alonso-Gonzalez, R.; Swan, L.; Babu-Narayan, S.V.; Baumgartner, H.; Dimopoulos, K.; Gatzoulis, M.A. Depression requiring anti-depressant drug therapy in adult congenital heart disease: Prevalence, risk factors, and prognostic value. Eur. Heart J. 2016, 37, 771–782. [Google Scholar] [CrossRef] [Green Version]
- Benderly, M.; Kalter-Leibovici, O.; Weitzman, D.; Blieden, L.; Buber, J.; Dadashev, A.; Mazor-Dray, E.; Lorber, A.; Nir, A.; Yalonetsky, S.; et al. Depression and anxiety are associated with high health care utilization and mortality among adults with congenital heart disease. Int. J. Cardiol. 2019, 276, 81–86. [Google Scholar] [CrossRef]
- Kahl, K.G.; Fraccarollo, D.; Winter, L.; Bauersachs, J.; Westhoff-Bleck, M. Increased epicardial adipose tissue in young adults with congenital heart disease comorbid with major depressive disorder. J. Affect. Disord. 2019, 257, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Westhoff-Bleck, M.; Winter, L.; Davila, L.A.; Herrmann-Lingen, C.; Treptau, J.; Bauersachs, J.; Bleich, S.; Kahl, K.G. Diagnostic evaluation of the hospital depression scale (HADS) and the Beck depression inventory II (BDI-II) in adults with congenital heart disease using a structured clinical interview: Impact of depression severity. Eur. J. Prev. Cardiol. 2020, 27, 381–390. [Google Scholar] [CrossRef]
- Warnes, C.A.; Liberthson, R.; Danielson, G.K.; Dore, A.; Harris, L.; Hoffman, J.I.; Somerville, J.; Williams, R.G.; Webb, G.D. Task Force 1: The changing profile of congenital heart disease in adult life. J. Am. Coll. Cardiol. 2001, 37, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Sandercock, G.R.H.; Brodie, D.A. The role of heart rate variability in prognosis for different modes of death in chronic heart failure. Pacing Clin. Electrophysiol. 2006, 29, 892–904. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Mortara, A.; Capomolla, S.; Febo, O.; Ferrari, R.; Franchini, M.; Gnemmi, M.; Opasich, C.; et al. Short-Term Heart Rate Variability Strongly Predicts Sudden Cardiac Death in Chronic Heart Failure Patients. Circulation 2003, 107, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Smilde, T.D.J.; Van Veldhuisen, D.J.; Berg, M.P.V.D. Prognostic value of heart rate variability and ventricular arrhythmias during 13-year follow-up in patients with mild to moderate heart failure. Clin. Res. Cardiol. 2009, 98, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann-Viehoff, F.; Orth-Gomer, K.; Wang, H.-X.; Deter, H.-C.; Merswolken, M.; Ghadiyali, Z.; Weber, C.S. Depressive symptoms and heart rate variability in younger women after an acute coronary event. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Drago, S.; Bergerone, S.; Anselmino, M.; Varalda, P.G.; Cascio, B.; Palumbo, L.; Angelini, G.; Trevi, P.G. Depression in patients with acute myocardial infarction: Influence on autonomic nervous system and prognostic role. Results of a five-year follow-up study. Int. J. Cardiol. 2007, 115, 46–51. [Google Scholar] [CrossRef]
- Kemp, A.H.; Quintana, D.S.; Gray, M.A.; Felmingham, K.L.; Brown, K.; Gatt, J.M. Impact of depression and antidepressant treatment on heart rate variability: A review and meta-analysis. Biol. Psychiatry 2010, 67, 1067–1074. [Google Scholar] [CrossRef]
- Stetler, C.; Miller, G.E. Depression and hypothalamic-pituitary-adrenal activation: A quantitative summary of four decades of research. Psychosom. Med. 2011, 73, 114–126. [Google Scholar] [CrossRef]
- Cosan, A.S.; Schweiger, J.U.; Kahl, K.G.; Hamann, B.; Deuschle, M.; Schweiger, U.; Westermair, A.L. Fat compartments in patients with depression: A meta-analysis. Brain Behav. 2021, 11, e01912. [Google Scholar] [CrossRef]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M.; et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef]
- Tjora, T.; Hetland, J.; Aarø, L.E.; Wold, B.; Wiium, N.; Øverland, S. The association between smoking and depression from adolescence to adulthood. Addiction 2014, 109, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Glassman, A.H.; Bigger, J.T.; Gaffney, M. Psychiatric characteristics associated with long-term mortality among 361 patients having an acute coronary syndrome and major depression: Seven-year follow-up of SADHART participants. Arch. Gen. Psychiatry 2009, 66, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Kempny, A.; Diller, G.-P.; Dimopoulos, K.; Alonso-Gonzalez, R.; Uebing, A.; Li, W.; Babu-Narayan, S.; Swan, L.; Wort, S.J.; Gatzoulis, M.A. Determinants of outpatient clinic attendance amongst adults with congenital heart disease and outcome. Int. J. Cardiol. 2016, 203, 245–250. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Underlying Cardiovascular Disease | n |
|---|---|
| Tetralogy of Fallot | 25 |
| Atrioventricular septal defect | 7 |
| Simple shunts | 9 |
| Mild valve disease | 7 |
| Subaortic stenosis | 4 |
| Aortic valve disease (valve replacement, conduit, more than mild valve lesions) | 18 |
| Fontan circulation | 12 |
| D-Transposition of the great arteries: Atrial redirection surgery | 17 |
| Congenital pulmonary stenosis | 7 |
| Marfan | 15 |
| Coarctation | 20 |
| Eisenmenger syndrome | 4 |
| Congenitally corrected transposition | 3 |
| Ebstein anomaly | 4 |
| Miscellaneous | 19 |
| Total cohort | 171 |
| Parameter | Total Cohort (n = 171) | Without 13 MDD (Group a: n = 123) | Mild 13 MDD (Group b: n = 20) | Moderate/Severe 13 MDD (Group c: n = 28) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 35.6 ± 11.4 | 35.2 ± 11.7 | 36.1 ± 2.3 | 37.0 ± 11.0 | 14 n.s. |
| Body Mass Index (kg/m2) | 25.3 ± 6.0 | 24.9 ± 6.4 | 25.9 ± 4.825.3 | 26.6 ± 4.9 | n.s. |
| Disease Complexity: Great/moderate/low (%) | 53.2/28.1/18.7 | 53.6/27.6/18.8 | 35/35/30.7 | 64.3/25/10.7 | b/c < 0.001 |
| 1 NYHA-Class I/II/(II/IV) (%) | 76.0/18.7/5.3 | 83.7/11.4/4.9 | 70/25/5 | 46.4/46.4/7.2 | a/c < 0.001 |
| Male sex (n/%) | 73/42.7 | 47/61.3 | 11/55 | 15/53.6 | n.s. |
| Hypertension (%) | 29 | 20.2 | 36.8 | 14 | n.s. |
| Epicardial fat (cm) | 0.43 ± 0.18 | 0.39 ± 0.17 | 0.52 ± 0.18 | 0.55 ± 0.20 | a/b = 0.005 a/c < 0.001 |
| 2 HADS-D | 3.6 ± 3.8 | 2.1 ± 2.5 | 5.5 ± 2.2 | 9.1 ± 4.3 | a/b < 0.001 a/c < 0.001 b/c < 0.001 |
| 3 BDI-II | 7.6 ± 8.53 | 4.0 ± 4.8 | 11.7 ± 6.6 | 20.9 ± 8.0 | a/b < 0.001 a/c < 0.001 b/c < 0.001 |
| Oxygen-saturation (%) | 98.3 ± 2.5 | 98.5 ± 2.1 | 97.4 ± 3.9 | 98.3 ± 2.5 | n.s. |
| 4 HsCRP (mg/L) | 3.3 ± 6.1 | 3.2 ± 5.9 | 3.3 ± 6.3 | 3.8 ± 7.1 | n.s. |
| Creatinine (µmol/L) | 77.5 ± 15.6 | 77.0 ± 15.0 | 71.9 ± 13.9 | 83.5 ± 17.4 | n.s. |
| 5 GGT (U/L) | 39.8 ± 60.3 | 39.5 ± 64.0 | 30.8 ± 21.9 | 47.6 ± 62.8 | n.s. |
| 6 NT-proBNP (ng/L) | 182 ± 253 | 169 ± 208 | 99 ± 96 | 302 ± 428 | c/a = 0.034 c/b = 0.018 |
| 7 HBA1c (%) | 5.34 ± 0.34 | 5.31 ± 0.33 | 5.34 ± 0.42 | 5.45 ± 0.28 | n.s. |
| 8 LDL(mg/dL) | 118.9 ± 31.2 | 116.4 ± 32.1 | 128.6 ± 23.2 | 122.9 ± 31.0 | n.s. |
| QRS (ms) | 120 ± 28 | 119 ± 28 | 109 ± 19 | 127 ± 33 | n.s. |
| 9 QTc (ms) | 451 ± 31 | 451 ± 37 | 423 ± 21 | 436 ± 40 | n.s. |
| 10 SDNN | 97.9 ± 47.4 | 101.0 ± 48.8 | 83.3 ± 34.7 | 94.1 ± 49.0 | n.s. |
| 11 Triangular Index | 15.7 ± 8.6 | 16.3 ± 8.7 | 15.4 ± 7.3 | 13.5 ± 9.1 | n.s. |
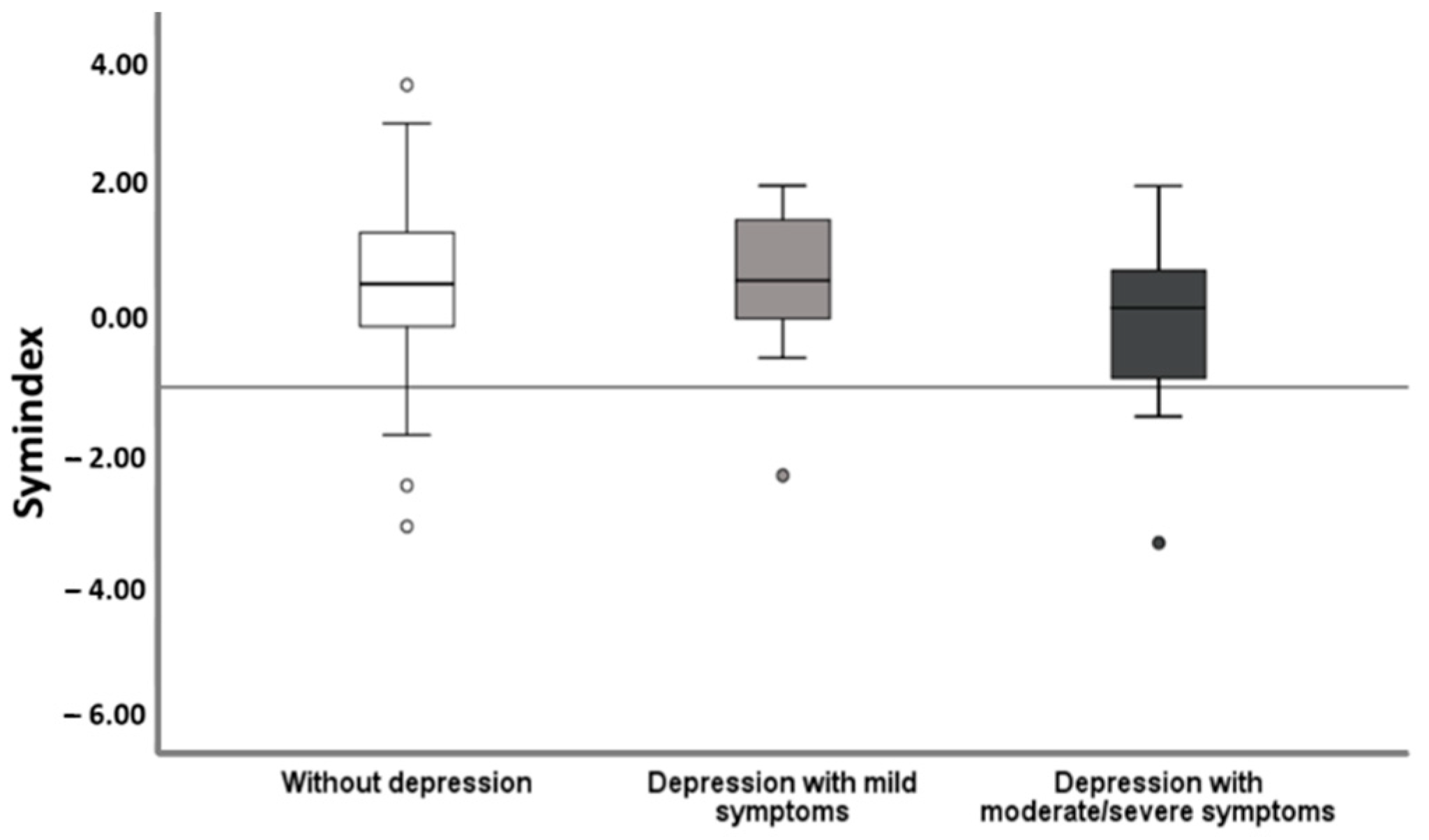
| 12 Symindex | 0.48 ± 1.12 | 0.59 ± 1.00 | 0.65 ± 1.06 | −0.11 ± 1.45 | c/a < 0.001 c/b = 0.057 |
| Binary Logistic Regression Analysis | Without Depression Versus all Patients with Depression | p-Value | Without Depression Versus Mild Depressive Symptoms | p-Value | Without Depression/ Mild Depressive Symtoms Versus Moderate/ Severe Symptoms | p-Value | Without Depression Versus Moderate/ Severe Depressive Symptoms | p-Value |
|---|---|---|---|---|---|---|---|---|
| Univariate analysis | 9 HR (95%10 CI) | 9 HR (95%10 CI) | 9 HR (95%10 CI) | 9 HR (95%10 CI) | ||||
| 1 Symindex | 0.74 (0.55–0.99) | 0.048 | 1.06 (0.66–1.70) | 0.813 | 0.59 (0.41–0.85) | 0.004 | 0.59 (0.40–0.86) | 0.006 |
| Age | 1.01 (0.98–1.04 | 0.461 | 1.01 (0.97–1.05) | 0.743 | 1.02 (0.98–1.05) | 0.476 | 1.01 (0.98–1.05) | 0.456 |
| Sex | 1.91 (0.97–3.75) | 0.060 | 1.98 (0.76–51.3) | 0.161 | 0.21 (0.75–3.82) | 0.206 | 1.97 (0.82–4.27) | 0.193 |
| 2 NYHA-Class | 2.32 (1.31–4.10) | 0.004 | 1.53 (0.71–3.34) | 0.280 | 2.64 (1.42–4.90) | 0.002 | 2.83 (1.49–5.41) | 0.002 |
| Disease Complexity | 1.03 (0.67–1.58) | 0.902 | 1.58 (0.89–2.83) | 0.119 | 0.66 (0.37 1–18) | 0.159 | 0.71 (0.39–1.27) | 0.247 |
| Number of cardiac operations | 0.99 (0.73–1.35) | 0.958 | 0.76 (0.48–1.22) | 0.256 | 1.22 (0.85–1.75) | 0.291 | 1.17 (0.81–1.67) | 0.393 |
| Hypertension | 1.31 (0.59–2.87) | 0.505 | 2.61 (0.97–7.08) | 0.059 | 0.56 (0.18–1.72) | 0.307 | 0.65 (0.21–2.06) | 0.467 |
| Body Mass Index | 1.04 (0.98–1.10) | 0.175 | 1.02 (0.96–1.09) | 0.473 | 1.04 (0.98–1.10 | 0.226 | 1.04 (0.98–1.10) | 0.206 |
| Epicardial fat | 123 (14.3–1061) | <0.0001 | 41.4 (3.19–537) | 0.004 | 64.5 (6.23–666) | <0.0001 | 149 (11.7–1917) | <0.0001 |
| Oxygen-saturation (%) | 0.91 (0.80–1.03) | 0.132 | 0.99 (0.80–1.25) | 0.992 | 0.87 (0.76–0.99) | 0.041 | 0.87 (0.76–0.99) | 0.047 |
| 3 HsCRP (mg/L) | 1.01 (0.96–1.06) | 0.727 | 1.00 (0.93–1.08) | 0.964 | 1.01 (0.96–1.08) | 0.655 | 1.01 (0.96–1.08) | 0.654 |
| Creatinine (µmol/L) | 1.01 (0.97–1.03) | 0.531 | 0.97 (0.94–1.01) | 0.156 | 1.03 (1.03–1.05) | 0.029 | 1.03 (1.00–1.05) | 0.053 |
| 4 GGT (U/L) | 1.00 (0.99–1.01) | 0.981 | 0.99 (0.98–1.01) | 0.552 | 1.00 (0.99–1.01) | 0.647 | 1.00 (0.97–1.01) | 0.551 |
| 5 NT-proBNP (ng/L) | 1.00 (0.99–1.00) | 0.273 | 0.99 (0.99–1.00) | 0.128 | 1.00 (1.00–1.01) | 0.020 | 1.00 (1.00–1.01) | 0.035 |
| 6 HBA1c (%) | 2.24 (0.83–6.07) | 0.133 | 1.31 (0.38–4.56) | 0.672 | 2.67 (0.90–7.89) | 0.076 | 3.17 (0.90–11.2) | 0.072 |
| 7 LDL(mg/dL) | 1.01 (0.99–1.02) | 0.096 | 1.01 (0.99–1.03) | 0.108 | 1.01 (0.96–1.02) | 0.451 | 1.00 (0.99–1.02) | 0.326 |
| QRS (ms) | 1.00 (0.99–1.01) | 0.945 | 0.98 (0.96–1.01) | 0.119 | 1.01 (0.99–1.02) | 0.141 | 1.01 (0.99–1.02) | 0.237 |
| 8 QTC (ms) | 1.00 (0.99–1.01) | 0.452 | 0.99 (0.98–1.11) | 0.793 | 1.01 (0.99–1.02) | 0.179 | 1.01 (0.99–1.02) | 0.212 |
| Multivariate analysis | ||||||||
| 1 Symindex | 0.63 (0.44–0.91) | 0.014 | 0.62 (0.43–0.90) | 0.013 | ||||
| Epicardial fat | 48.8 (4.30–558) | 0.004 | 131 (9.60–1798) | <0.0001 |
| Cox Proportional Regression Analysis | Heart Failure and All-Cause Mortality | p-Value | Hospitalization | p-Value | Supraventricular/Ventricular Tachycardia | p-Value |
|---|---|---|---|---|---|---|
| Univariate analysis | 9 HR (95%CI) | 9 HR (95%CI) | 9 HR (95%CI) | |||
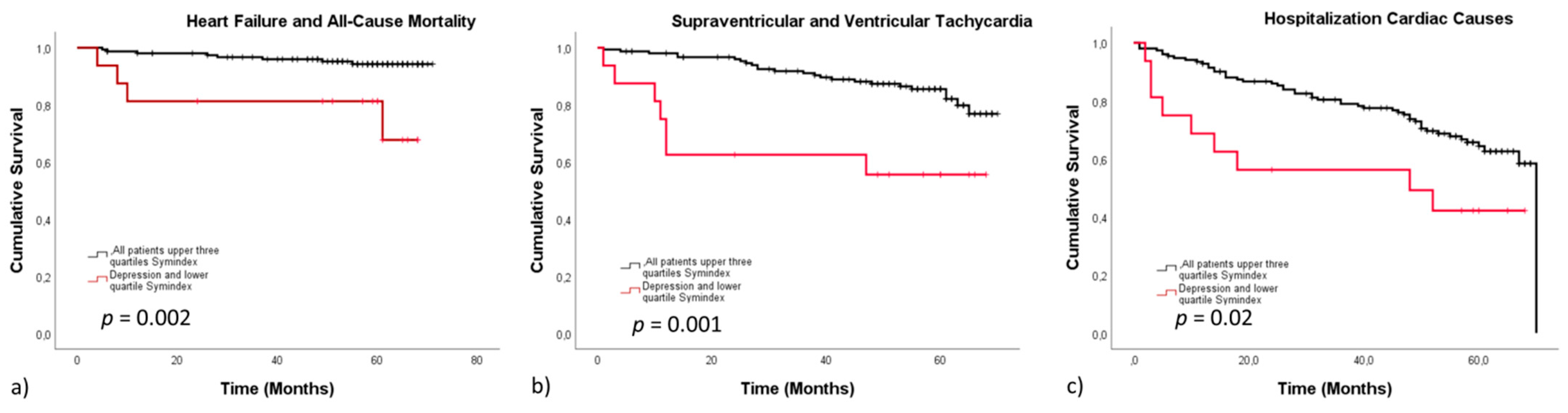
| 1 Symindex (lower quartile) | 3.95 (1.25–12.5) | 0.019 | 1.88 (1.11–3.17) | 0.029 | 2.90 (1.43–5.87) | 0.003 |
| 1 Symindex (lower quartile) comorbid with depression | 5.30 (1.59–17.6) | 0.006 | 2.27 (1.13–4.61) | 0.024 | 3.80 (1.63–8.80) | 0.002 |
| 2 Major depressive disorder | 3.94 (1.25–12.4) | 0.019 | 1.26 (0.66–2.43) | 0.487 | 2.14 (0.96–4.80) | 0.064 |
| Age | 1.00 (0.96–1.059 | 0.902 | 1.01 (0.99–1.04) | 0.264 | 0.98 (0.99–1.04) | 0.364 |
| Sex | 0.66 (0.20–2.20) | 0.504 | 0.83 (0.49–1.40) | 0.485 | 0.44 (0.20–0.99) | 0.048 |
| 3 NYHA-Class | 2.71 (1.34–4.55) | 0.006 | 2.30 (1.59–3.32) | <0.0001 | 1.87 (1.12–3.12) | 0.016 |
| Disease Complexity | 0.14 (0.02–0.96) | 0.045 | 0.33 (0.20–0.59) | <0.0001 | 0.25 (0.11–0.58) | 0.001 |
| Number of cardiac operations | 0.64 (0.26–1.59) | 0.340 | 1.51 (1.17–1.95) | 0.001 | 1.65 (1.20–2.27) | 0.002 |
| Hypertension | 1.19 (0.32–4.39) | 0.796 | 0.91 (0.48–1.72) | 0.779 | 0.85 (0.35–2.08) | 0.725 |
| Body Mass Index | 1.04 (0.98–1.10) | 0.246 | 1.01 (0.98–1.05) | 0.532 | 1.02 (0.98–1.07) | 0.290 |
| Epicardial fat | 18.50 (1.24–276) | 0.034 | 7.93 (2.03–31.0) | 0.003 | 26.8(4.04–178) | 0.001 |
| Oxygen-saturation (%) | 0.93 (0.78–1.10) | 0.418 | 0.88 (0.81–0.95) | 0.002 | 0.92 (0.82–1.03) | 0.145 |
| 4 HsCRP (mg/L) | 1.01 (0.96–1.09) | 0.607 | 0.99 (0.96–1.03) | 0.524 | 0.96 (0.88–1.05) | 0.420 |
| Creatinine (µmol/L) | 1.03 (0.99–1.06) | 0.059 | 1.00 (0.99–1.02) | 0.847 | 1.03 (1.01–1.05) | 0.006 |
| 5 GGT (U/L) | 1.00 (0.99–1.01) | 0.212 | 1.00 (1.00–1.01) | 0.017 | 1.00 (0.98–1.01) | 0.605 |
| 6 NT-proBNP (ng/L) | 1.00 (1.00–1.00) | <0.0001 | 1.00 (1.00–1.00) | <0.0001 | 1.00 (1.00–1.01) | <0.0001 |
| 7 HBA1c (%) | 1.82 (0.62–5.38) | 0.280 | 1.38 (0.78–2.45) | 0.265 | 1.97 (1.05–3.71) | 0.035 |
| 8 LDL(mg/dL) | 0.99 (0.98–1.02) | 0.770 | 0.99 (0.99–1.01) | 0.513 | 1.00 (0.99–1.01) | 0.842 |
| QRS | 1.01 (0.99–1.03) | 0.163 | 1.01 (1.01–1.02) | 0.019 | 1.01 (0.97–1.02) | 0.186 |
| QTc | 1.01 (0.96–1.03) | 0.166 | 1.01 (1.00–1.02) | 0.021 | 0.99 (0.98–1.01) | 0.615 |
| Multivariate analysis | ||||||
| 1 Symindex (Lower Quartile) comorbid with depression | 7.04 (1.87–26.5) | 0.004 | 3.8 (1.36–10.6) | 0.011 | 4.90 (1.74–9.25) | 0.003 |
| 6 NT-proBNP | 1.00 (1.00–1.00) | <0.0001 | 1.00 (1.00–1.03) | 0.010 | 1.00 (1.00–1.00) | <0.0001 |
| Disease complexity | 0.39 (0.22–0.66) | 0.001 | 0.39(0.16–0.92) | 0.032 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Westhoff-Bleck, M.; Lemke, L.H.; Bleck, J.-M.S.; Bleck, A.C.; Bauersachs, J.; Kahl, K.G. Depression Associated with Reduced Heart Rate Variability Predicts Outcome in Adult Congenital Heart Disease. J. Clin. Med. 2021, 10, 1554. https://doi.org/10.3390/jcm10081554
Westhoff-Bleck M, Lemke LH, Bleck J-MS, Bleck AC, Bauersachs J, Kahl KG. Depression Associated with Reduced Heart Rate Variability Predicts Outcome in Adult Congenital Heart Disease. Journal of Clinical Medicine. 2021; 10(8):1554. https://doi.org/10.3390/jcm10081554
Chicago/Turabian StyleWesthoff-Bleck, Mechthild, Lars H. Lemke, Jan-Marc S. Bleck, Anja C. Bleck, Johann Bauersachs, and Kai G. Kahl. 2021. "Depression Associated with Reduced Heart Rate Variability Predicts Outcome in Adult Congenital Heart Disease" Journal of Clinical Medicine 10, no. 8: 1554. https://doi.org/10.3390/jcm10081554
APA StyleWesthoff-Bleck, M., Lemke, L. H., Bleck, J. -M. S., Bleck, A. C., Bauersachs, J., & Kahl, K. G. (2021). Depression Associated with Reduced Heart Rate Variability Predicts Outcome in Adult Congenital Heart Disease. Journal of Clinical Medicine, 10(8), 1554. https://doi.org/10.3390/jcm10081554