
Efficacy and Underlying Mechanism of Acupuncture in the Treatment of Posttraumatic Stress Disorder: A Systematic Review of Animal Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Data Analysis
3. Results
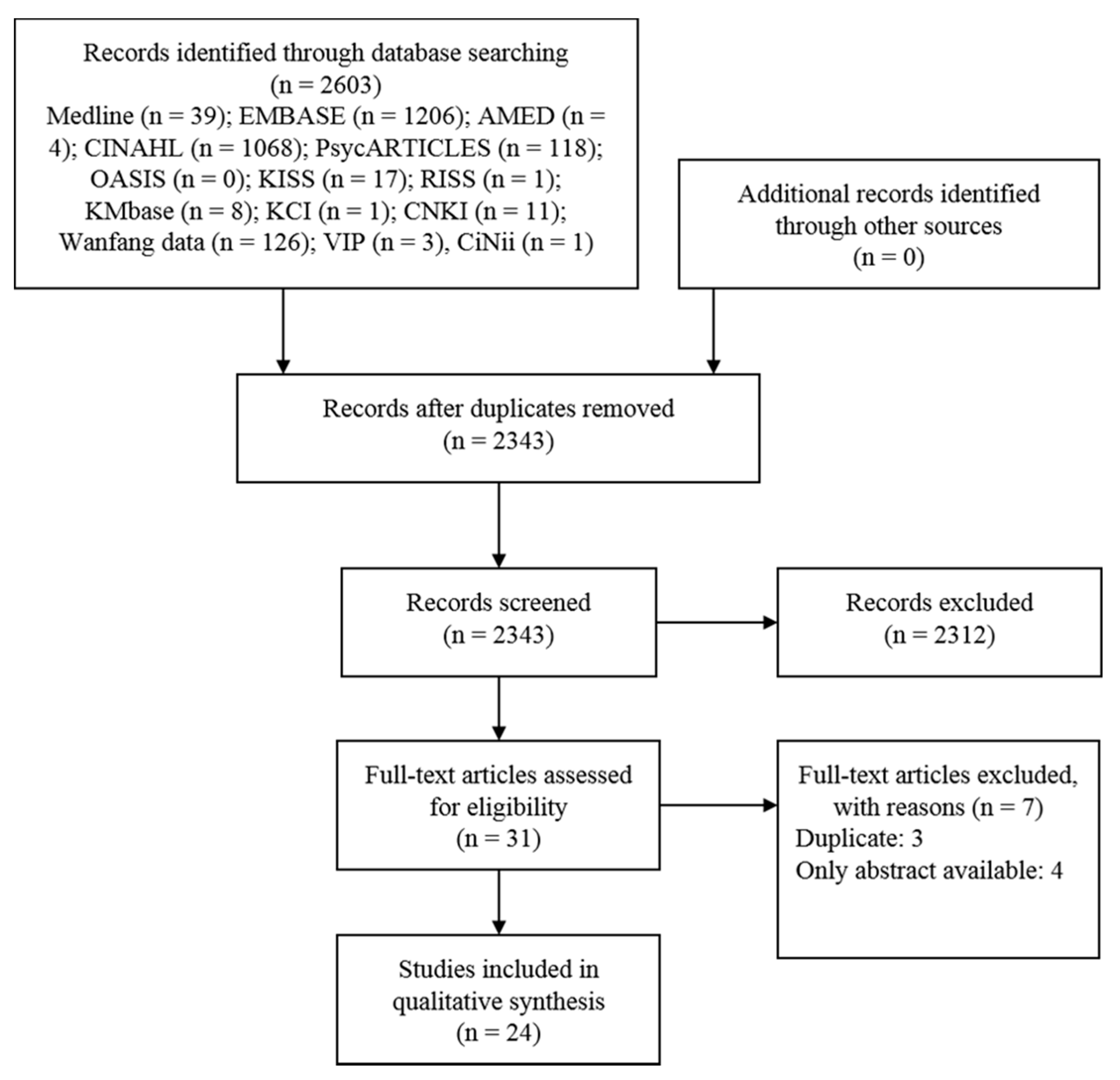
3.1. Search Results
3.2. Study Description
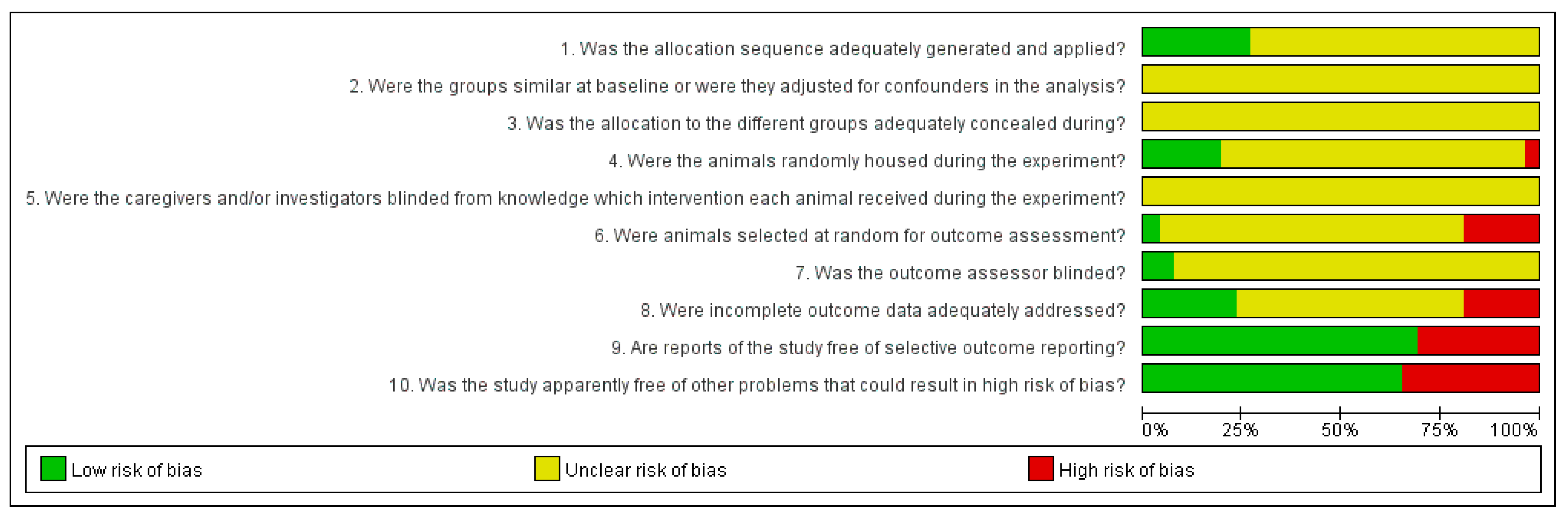
3.3. Methodological Qualities of Included Studies
3.4. Main Results for Each Symptom of PTSD
3.4.1. Anxiety & Fear
3.4.2. Sleep Disturbance
3.4.3. Cognitive Symptom
3.4.4. Depression
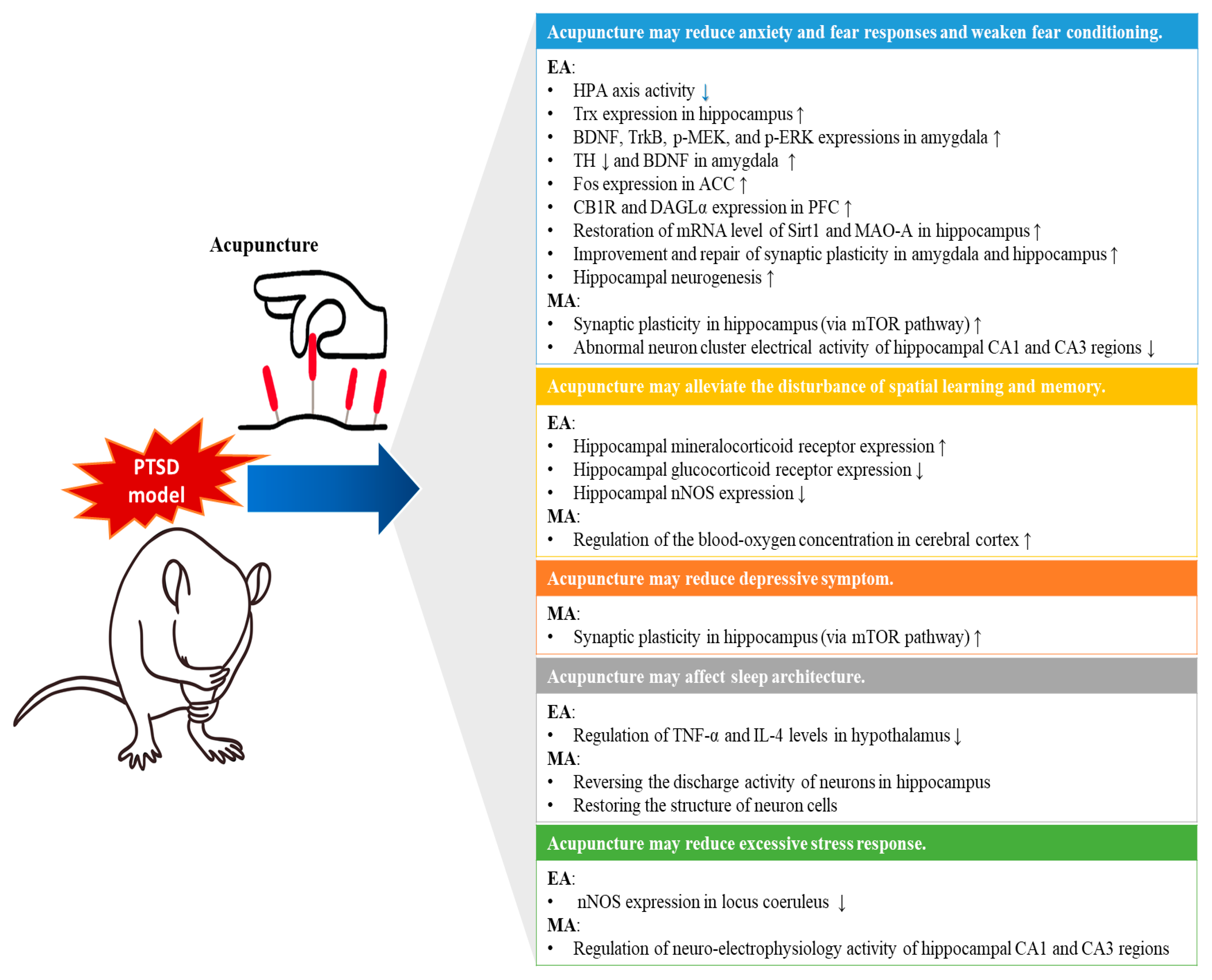
3.5. Proposed Mechanisms
3.5.1. Regulation of Stress Responses in the Neuroendocrine System
3.5.2. Promotion of Neuroprotection, Neurogenesis, and Synaptic Plasticity in Brain
- (1)
- Hippocampus: In PSTD, the hippocampus forms a link between situational stimuli and aversive events and plays an important role in memory recall [56]. Thus, hippocampal dysfunction is considered an important factor that causes PTSD or maintains it by interacting with traumatic experiences [56]. Furthermore, since chronic stress is known to cause atrophy of the hippocampus, interventions targeting adult neurogenesis and synaptic plasticity improvement in the hippocampus may be useful for PTSD and other mental disorders [57]. In this respect, several studies included in this review have reported the potential impact of acupuncture on the hippocampus: upregulation of thioredoxin (Trx) expression in the hippocampus [32], restoration of messenger ribonucleic acid (mRNA) levels of sirtuin 1 and monoamine oxidase A in the hippocampus [33], improvement and repair of synaptic plasticity in hippocampus [36], improvement of hippocampal neurogenesis [40], upregulation of the protein synthesis required for synaptic plasticity via the mammalian target of rapamycin pathway in the hippocampus [44], restoration of the structure of hippocampal neuronal cells [42,49], reverse of the discharge activity of neurons in the hippocampus [49], and regulation of abnormal neuronal cluster electrical activity in the hippocampal CA1 and CA3 regions [48,50].
- (2)
- Amygdala: In addition to the hippocampus, the amygdala is the most clearly altered limbic region in PTSD, which can lead to an overactive reaction to fear stimuli [58]. In the fear circuit, the hippocampus is thought to play an important role in the explicit memory of traumatic events and mediate learned responses to contextual cues. The PFC reactivates past emotional associations, and the amygdala is activated in PTSD subjects and associated with oversensitivity to stress, generalized fear responses, and impaired extinction [58]. Thus, interventions that promote synaptic plasticity in the amygdala could potentially contribute to fear control and extinction [58]. In this respect, some studies included in this review have reported on the potential impact of acupuncture on the amygdala: upregulation of brain-derived neurotrophic factor (BDNF), tropomyosin-related kinase B (TrkB), phosphorylated mitogen-activated protein/extracellular signal-regulated kinase (p-MEK), phosphorylated extracellular signal-regulated kinase (p-ERK) expression in the amygdala [34], prevention of increase in tyrosine hydroxylase (TH) level and decrease in BDNF level in the amygdala [41], and improvement and repair of synaptic plasticity in the amygdala [36].
- (3)
- Anterior cingulate cortex: In the anterior cingulate cortex (ACC), c-Fos expression is related to emotional regulation and attention and cognitive control [59,60], which are all related to major pathologies of PTSD. c-Fos is a gene involved in cell proliferation and differentiation after extracellular stimuli [61]. In ACC, which plays a role in regulating conditioned fear responses [62], c-FOS expression was significantly increased after EA [37].
- (4)
- Prefrontal cortex: Endocannabinoids regulate various forms of synaptic plasticity in the adult brain, and enhancement of cannabinoid type 1 receptor (CB1R) is highly expressed in the forebrain [63]. A study found that EA could upregulate expressions of CB1R and diacylglycerol lipase α (DAGLα), which generate 2-arachidonoylglycerol (the most abundant ligand for the CB1R), in the PFC [35].
- (5)
- Others: One study [46] indicated the regulatory effect of MA on the blood oxygen level in the cerebral cortex.
4. Discussion
4.1. Regulation of Stress Responses in the Neuroendocrine System
4.2. Promotion of Neuroprotection, Neurogenesis, and Synaptic Plasticity in Several Brain Areas
4.3. Comparison with Previous Clinical Studies
4.4. Strengths and Limitations of this Review
4.5. Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Section/Topic | # | Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | NA |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 3 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 3 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | Appendix A |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 3 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 3 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 3 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 3 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 3–4 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | NA |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | NA |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | NA |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 4, Figure 1 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 4–5, Table 1, Table 2 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 13, Figure 2 |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 14–16 |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | NA |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | NA |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | NA |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 16–19 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 20 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 21 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 21 |
Appendix B. Search Terms Used in Each Database
| Searches | Results | |
|---|---|---|
| #1 | (“Trauma and Stressor Related Disorders” [MeSH] OR “posttraumatic stress disorder” [Title/abstract] OR PTSD [Title/abstract] OR trauma [Title/abstract] OR posttrauma [Title/abstract] OR posttraumatic [Title/abstract]) | 271346 |
| #2 | (“Acupuncture Therapy” [MeSH] OR “Acupuncture, Ear” [MeSH] OR “Acupuncture Points” [MeSH] OR “Acupuncture” [MeSH] OR “Electroacupuncture” [MeSH] OR “Meridians” [MeSH] OR acupuncture [Title/abstract] OR electroacupuncture [Title/abstract] OR electro-acupuncture [Title/abstract] OR acupoint * [Title/abstract]) | 30617 |
| #3 | (“Models, Animal” [MeSH] OR “animal” [ALL] OR “model” [ALL]) | 3183477 |
| #4 | #1 AND #2 AND #3 | 39 |
| Searches | Results | |
|---|---|---|
| #1 | (‘posttraumatic stress disorder’/exp OR ‘posttraumatic stress disorder’ OR ‘trauma’ OR ‘posttrauma’ OR ‘posttraumatic’ OR PTSD) | 2435517 |
| #2 | (‘acupuncture’/exp OR ‘acupuncture’ OR ‘acupuncture therapy’ OR ‘auricular acupuncture’/exp OR ‘auricular acupuncture’ OR ‘ear acupuncture’ OR ‘acupuncture point’/exp OR ‘acupuncture point’ OR ‘electroacupuncture’/exp OR ‘electroacupuncture’ OR ‘electro-acupuncture’ OR ‘body meridian’/exp OR ‘body meridian’ OR ‘acupoint’) | 52903 |
| #3 | (‘animal model’/exp OR ‘animal’ OR ‘model’) | 8415222 |
| #4 | #1 AND #2 AND #3 | 1206 |
| Searches | Results | |
|---|---|---|
| #1 | (“Trauma and Stressor Related Disorders” [SU] OR “posttraumatic stress disorder” [TX] OR PTSD [TX] OR trauma [TX] OR posttrauma [TX] OR posttraumatic [TX]) | 4609 |
| #2 | (“Acupuncture Therapy” [SU] OR “Acupuncture, Ear” [SU] OR “Acupuncture Points” [SU] OR Acupuncture [SU] OR Electroacupuncture [SU] OR Meridians [SU] OR acupuncture [TX] OR electroacupuncture [TX] OR electro-acupuncture [TX] OR acupoint * [TX]) | 11403 |
| #3 | (“Models, Animal” [SU] OR animal [TX] OR model [TX]) | 31989 |
| #4 | #1 AND #2 AND #3 | 4 |
| Searches | Results | |
|---|---|---|
| #1 | (“Trauma and Stressor Related Disorders” [MH] OR “posttraumatic stress disorder” [TX] OR PTSD [TX] OR trauma [TX] OR posttrauma [TX] OR posttraumatic [TX]) | 227540 |
| #2 | (“Acupuncture Therapy” [MH] OR “Acupuncture, Ear” [MH] OR “Acupuncture Points” [MH] OR Acupuncture [MH] OR Electroacupuncture [MH] OR Meridians [MH] OR acupuncture [TX] OR electroacupuncture [TX] OR electro-acupuncture [TX] OR acupoint * [TX]) | 32495 |
| #3 | (“Models, Animal” [MH] OR animal [TX] OR model [TX]) | 1042824 |
| #4 | #1 AND #2 AND #3 | 1068 |
| Searches | Results | |
|---|---|---|
| #1 | mesh (Trauma and Stressor Related Disorders) OR ‘posttraumatic stress disorder’ OR PTSD OR trauma OR posttrauma OR posttraumatic | 20421 |
| #2 | mesh (Acupuncture Therapy) OR mesh (Acupuncture, Ear) OR mesh (Acupuncture Points) OR mesh (Acupuncture) OR mesh (Electroacupuncture) OR mesh (Meridians) OR ‘acupuncture’ OR ‘electroacupuncture’ OR ‘electro-acupuncture’ OR acupoint * | 327 |
| #3 | mesh (Models, Animal) OR ‘animal’ OR ‘model’ | 121684 |
| #4 | #1 AND #2 AND #3 | 118 |
| Searches | Results | |
|---|---|---|
| #1 | (외상 OR 트라우마 OR PTSD) AND 동물 AND 침 | 0 |
| #2 | (외상 OR 트라우마 OR PTSD) AND 모델 AND 침 | 0 |
| #3 | #1 OR #2 | 0 |
| Searches | Results | |
|---|---|---|
| #1 | (외상 OR 트라우마 OR PTSD) AND 동물 AND 침 | 7 |
| #2 | (외상 OR 트라우마 OR PTSD) AND 모델 AND 침 | 11 |
| #3 | #1 OR #2 | 17 |
| Searches | Results | |
|---|---|---|
| #1 | (외상 OR 트라우마 OR PTSD) AND 동물 AND 침 | 0 |
| #2 | (외상 OR 트라우마 OR PTSD) AND 모델 AND 침 | 1 |
| #3 | #1 OR #2 | 1 |
| Searches | Results | |
|---|---|---|
| #1 | (트라우마 OR PTSD) AND (동물 OR 모델) AND 침 | 8 |
| Searches | Results | |
|---|---|---|
| #1 | (외상 OR 트라우마 OR PTSD) AND 동물 AND 침 | 1 |
| #2 | (외상 OR 트라우마 OR PTSD) AND 모델 AND 침 | 0 |
| #3 | #1 OR #2 | 1 |
| Searches | Results | |
|---|---|---|
| #1 | (SU = ‘PTSD’+‘创伤后应激障碍’) AND (SU=‘acupuncture’+‘针’+‘鍼’) AND (SU=‘animal’+‘model’+‘动物’+‘模型’) | 11 |
| Searches | Results | |
|---|---|---|
| #1 | (主题: (“PTSD” + “创伤后应激障碍”) * 主题: (“acupuncture” + “针” + “鍼”) * 主题: (“animal” + “model” + “动物” + “模型”)) | 126 |
| Searches | Results | |
|---|---|---|
| #1 | (M = (PTSD OR 创伤后应激障碍)) AND (M = (acupuncture OR 针 OR 鍼)) AND (M = (animal OR model OR 动物 OR 模型)) | 3 |
| Searches | Results | |
|---|---|---|
| #1 | (PTSD OR 创伤后应激障碍) AND (acupuncture OR 針 OR 鍼) AND (animal OR model OR 动物 OR 模型)) | 1 |
Appendix C
| Studies | Funding Sources |
|---|---|
| Chen 2019 | National Natural Science Foundation of China |
| Ding 2018 | National Natural Science Foundation of China |
| Fang 2012 | National Natural Science Foundation of China Sichuan Provincial Department of Education Natural Science Foundation Key Project |
| Hou 2013a | Anhui Natural Science Foundation Project Doctoral Research Fund of Wannan Medical College |
| Hou 2013b | Anhui Natural Science Foundation Project Doctoral Research Fund of Wannan Medical College |
| Li 2017 | Shaanxi Province Science and Technology Rising Star Funded Project |
| Li 2019 | National Natural Science Foundation of China |
| Li 2016 | Not reported |
| Li 2014 | Not reported |
| Liu 2019 | Natural Science Foundation of China Science Research fund of Shanghai Municipal Commission of Health and Family The Three-Year development plan project for Traditional Chinese Medicine |
| Wei 2019 | Hubei Province Traditional Chinese Medicine Integrated Traditional Chinese and Western Medicine Project High-level talent research projects in Xianning City, Hubei Province |
| Xie 2015 | Anhui Province University Student Innovation Training Project |
| Xue 2019 | National Natural Science Foundation of China National Science and technology support program of China the Fundamental Research Funds of Shaanxi Province |
| Zhou 2019 | National Natural Science Foundation of China National Science and Technology Support Program of China the Fundamental Research Funds of Shaanxi Province |
| Zhu 2019 | Provincial Excellent Young Talents Fund Project of Anhui Colleges and Universities Provincial Natural Science Foundation Project of Anhui Universities |
| Han 2017 | 2014 National Natural Science Foundation of China Regional Project and 2013 Gansu Provincial Natural Science Research Foundation Project |
| Oh 2018 | the National Research Foundation of Korea funded by the Korean government (NRF-2015M3A9E3052338 and 2017R1A2B4009963) and the Korea Institute of Oriental Medicine |
| Wei 2018 | Regional Science Fund of National Natural Science Foundation of China Natural Science Foundation of Gansu Province, China |
| Yu 2019 | 2015 Wuhan Clinical Medicine Research Project |
| Zhang 2018 | Regional fund project of 2014 national natural science foundation of China 2013 Gansu provincial natural science foundation |
| Zhao 2018a | National Natural Science Foundation of China Gansu Province Natural Science Research Fund Project The 62nd batch of general projects of China Postdoctoral Science Foundation |
| Zhao 2016 | National Natural Science Foundation of China Regional Projects and 2013 Gansu Provincial Natural Science Research Fund Projects |
| Zhao 2018b | National Natural Science Foundation of China Gansu Province Natural Science Research Fund Project General funded project of China Postdoctoral Science Foundation |
| Zhao 2019 | General project of China postdoctoral science foundation Regional science fund of national natural science foundation of china 2013 natural science foundation of gansu province |
Appendix D
| Study | Acupuncture Methods | Acupoints | Course of Treatment | Treatment Duration |
|---|---|---|---|---|
| Fang 2012 | EA, dilatational wave | Baihui (GV 20), Changqiang (GV 1) | 15 min, once a day, total 3 sessions | 3 days |
| Hou 2013a | EA, 2 Hz, 1 mA | Baihui (GV 20), Zusanli (ST 36) | 30 min, once a day, total 7 sessions | 1 week |
| Hou 2013b | EA, 2 Hz, 1 mA | Baihui (GV 20), Zusanli (ST 36) | 30 min, once a day, total 7 sessions | 1 week |
| Li 2014 | EA, continuous wave, 2 Hz | Baihui (GV 20), Dazhui (GV 14) | 20 min, once a day, total 10 sessions | 10 days |
| Xie 2015 | EA, 2 Hz, 3 V | Baihui (GV 20), Zusanli (ST 36) | 20 min, once a day, total 7 sessions | 1 week |
| Li 2016 | EA, dilatational wave, 2/15 Hz, 1 mA | Baihui (GV 20) | 30 min, once a day, total 5 sessions | 1 week |
| Li 2017 | EA, dilatational wave, 2/15 Hz, 1 mA | Baihui (GV 20) | 30 min, once a day, total 7 sessions | 1 week |
| Ding 2018 | EA, dilatational wave, 2/100 Hz, 1 mA | Baihui (GV 20), Shenting (GV 24), Shenshu (BL 23) | 20 min, once a day, total 21 sessions | 3 weeks |
| Chen 2019 | EA, dilatational wave, 2/15 Hz, 1 mA | Baihui (GV 20) | 30 min, once a day, total 7 sessions | 1 week |
| Li 2019 | EA, dilatational wave, 2/100 Hz, 1 mA | Baihui (GV 20), Shenting (GV 24), Shenshu (BL 23) | 20 min, once a day, total 21 sessions | 3 weeks |
| Liu 2019 | EA, constant current square wave, 2 Hz, 3 mA | Zusanli (ST 36) | 20 min, once a day, total 7 sessions | 1 week |
| Wei 2019 | EA, 50/s | Baihui (GV 20) | 20 min, once a day, total 7 sessions | 1 week |
| Xue 2019 | EA, dilatational wave, 2/15 Hz, 1 mA | Baihui (GV 20) | 30 min, once a day, total 7 sessions | 1 week |
| Zhou 2019 | EA, dilatational wave, 2/15 Hz, 1 mA | Baihui (GV 20) | 30 min, once a day, total 7 sessions | 1 week |
| Zhu 2019 | EA, continuous wave, 2 Hz | Baihui (GV 20), Zusanli (ST 36) | 20 min, once a day, total 21 sessions | 3 weeks |
| Zhao 2016 (same in experiment (A) and (B)) | MA, basic manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 14 sessions | 14 days |
| Han 2017 | MA, small-amplitude twirling manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 12 sessions | 12 days |
| Oh 2018 (same in experiment (A) and (B)) | MA, turned at a rate of 2 spins/sec for 30 sec and removed immediately. | Shaofu (HT 8) | No retention, once a day, total 8 sessions | 18 days |
| Wei 2018 | MA, small-amplitude twirling manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 12 sessions | 12 days |
| Zhang 2018 | MA, minor lifting and thrusting and twirling for 1 min at each point | Baihui (GV 20), Neiguan (PC 6), Shenmen (HT 7), Taichong (LR 3) | 4 min, once a day, total 12 sessions | 12 days |
| Zhao 2018a | MA, minor lifting and thrusting and twirling for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 12 sessions | 12 days |
| Zhao 2018b | MA, basic manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 14 sessions | 2 weeks |
| Yu 2019 | MA, manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6), Shenmen (HT 7), Taichong (LR 3) | 4 min, once a day, total 7 sessions | 1 week |
| Zhao 2019 | MA, basic manipulation for 1 min at each point | Baihui (GV 20), Neiguan (PC 6) *, Shenmen (HT 7) *, Taichong (LR 3) * | 4 min, once a day, total 14 sessions | 2 weeks |
Appendix E
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Fang 2012 | U | U | U | U | U | N | U | U | Y | N |
| Hou 2013a | U | U | U | U | U | U | U | U | N | N |
| Hou 2013b | U | U | U | U | U | N | U | U | Y | Y |
| Li 2014 | U | U | U | U | U | N | U | U | N | N |
| Xie 2015 | U | U | U | U | U | U | U | U | Y | N |
| Li 2016 | U | U | U | U | U | U | U | U | Y | N |
| Li 2017 | U | U | U | U | U | N | U | U | Y | N |
| Ding 2018 | U | U | U | U | U | U | Y | U | Y | Y |
| Chen 2019 | U | U | U | U | U | U | U | U | Y | N |
| Li 2019 | U | U | U | U | U | U | U | U | Y | Y |
| Liu 2019 | U | U | U | Y | U | U | Y | U | Y | Y |
| Wei 2019 | U | U | U | U | U | N | U | U | Y | Y |
| Xue 2019 | U | U | U | U | U | U | U | U | Y | N |
| Zhou 2019 | U | U | U | U | U | U | U | U | Y | N |
| Zhu 2019 | U | U | U | U | U | U | U | U | N | Y |
| Zhao 2016 (experiment (A)) | Y | U | U | U | U | U | U | N | Y | Y |
| Zhao 2016 (experiment (B)) | Y | U | U | U | U | U | U | Y | Y | Y |
| Han 2017 | Y | U | U | U | U | U | U | N | Y | Y |
| Oh 2018 (experiment (A)) | U | U | U | Y | U | U | U | N | Y | Y |
| Oh 2018 (experiment (B)) | U | U | U | Y | U | U | U | N | N | Y |
| Wei 2018 | U | U | U | U | U | U | U | N | Y | Y |
| Zhang 2018 | Y | U | U | N | U | Y | U | Y | N | Y |
| Zhao 2018a | U | U | U | U | U | U | U | Y | N | Y |
| Zhao 2018b | Y | U | U | Y | U | U | U | Y | N | Y |
| Yu 2019 | Y | U | U | U | U | U | U | Y | Y | Y |
| Zhao 2019 | Y | U | U | Y | U | U | U | Y | N | Y |
References
- Association, A.P. Diagnostic and statistical manual of mental disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Spottswood, M.; Davydow, D.S.; Huang, H. The prevalence of posttraumatic stress disorder in primary care: A systematic review. Harv. Rev. Psychiatry 2017, 25, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wang, F.; Wen, J.; Shi, Y. Risk factors of post-traumatic stress disorder (PTSD) after Wenchuan earthquake: A case control study. PLoS ONE 2014, 9, e96644. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.; Ganeshamoorthy, S.; Myers, J. Risk factors associated with posttraumatic stress disorder in US veterans: A cohort study. PLoS ONE 2017, 12, e0181647. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Deng, Q.; Glik, D.; Dong, J.; Zhang, L. A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. Int. J. Environ. Res. Public Health 2017, 14, 1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guideline Development Panel for the Treatment of PTSD in Adults, American Psychological Association. Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. Am. Psychol. 2019, 74, 596–607. [Google Scholar] [CrossRef]
- Kawakita, K.; Okada, K. Acupuncture therapy: Mechanism of action, efficacy, and safety: A potential intervention for psychogenic disorders? BioPsychoSocial Med. 2014, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Yeung, A.S.; Schnyer, R.; Wang, Y.; Mischoulon, D. Acupuncture for depression: A review of clinical applications. Canadian journal of psychiatry. Rev. Can. Psychiatry 2012, 57, 397–405. [Google Scholar] [CrossRef] [Green Version]
- He, W.; Li, M.; Zuo, L.; Wang, M.; Jiang, L.; Shan, H.; Han, X.; Yang, K.; Han, X. Acupuncture for treatment of insomnia: An overview of systematic reviews. Complementary Ther. Med. 2019, 42, 407–416. [Google Scholar] [CrossRef]
- Li, M.; Xing, X.; Yao, L.; Li, X.; He, W.; Wang, M.; Li, H.; Wang, X.; Xun, Y.; Yan, P.; et al. Acupuncture for treatment of anxiety, an overview of systematic reviews. Complementary Ther. Med. 2019, 43, 247–252. [Google Scholar] [CrossRef]
- Grant, S.; Colaiaco, B.; Motala, A.; Shanman, R.; Sorbero, M.; Hempel, S. Acupuncture for the treatment of adults with posttraumatic stress disorder: A systematic review and meta-analysis. J. Trauma Dissociation Off. J. Int. Soc. Study Dissociation 2018, 19, 39–58. [Google Scholar] [CrossRef] [Green Version]
- Wahbeh, H.; Senders, A.; Neuendorf, R.; Cayton, J. Complementary and alternative medicine for posttraumatic stress disorder symptoms: A systematic review. J. Evid. Based Complementary Altern Med. 2014, 19, 161–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollifield, M. Acupuncture for posttraumatic stress disorder: Conceptual, clinical, and biological data support further research. CNS Neurosci. Ther. 2011, 17, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.Y.; Lee, B.; Kim, S.H. Effectiveness and safety of ear acupuncture for trauma-related mental disorders after large-scale disasters: A PRISMA-compliant systematic review. Medicine 2020, 99, e19342. [Google Scholar] [CrossRef] [PubMed]
- Ritskes-Hoitinga, M.; Leenaars, M.; Avey, M.; Rovers, M.; Scholten, R. Systematic reviews of preclinical animal studies can make significant contributions to health care and more transparent translational medicine. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Borghans, B.; Homberg, J.R. Animal models for posttraumatic stress disorder: An overview of what is used in research. World J. Psychiatry 2015, 5, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1. 0 [Updated March 2011]. The Cochrane Collaboration, 2011. Available online: www.cochrane-handbook.org (accessed on 18 March 2020).
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Wang, W.; Zong, Y.; Yang, H.; Lu, Y. Electroacupuncture inhibits decrease of BDNF and increase of GABAARa1 in the medial prefrontal cortex of PTSD rats. Chin. J. Histochem. Cytochem. 2016, 25, 54–58. [Google Scholar] [CrossRef]
- Zhang, J.B. Study on Brain Functional Mechanism of “Dispersing Liver and Regulating Spirit” Acupuncture Therapy on Post-traumatic Stress Disorder Based on the Technology of fNIRs. Master’s Thesis, Gansu University of Chinese Medicine, Gansu, China, 2017. [Google Scholar]
- Zhang, Y.F.; Zhao, Z.T.; Yan, X.K. Effect of acupuncture on blood oxygen concentration in brain of rats with post-traumatic stress disorder based on functional near-infrared spectroscopy. J. Acupunct. Tuina Sci. 2019, 17, 9–15. [Google Scholar] [CrossRef]
- Fang, Y.Q.; Cai, D.J.; Liu, S.G.; Yu, S.G.; Zhu, Q.Z. Effect of electroacupuncture on Spontaneous activity rhythm of rats with PTSD-like Anxiety Model. In Proceedings of the 10th China Time Biomedical Symposium 2013, Nanchang, China, 17 October 2013; p. 23. [Google Scholar]
- Li, M.; Ding, N.; Zhang, H. Study on the synaptic plasticity in hippocampus and medial prefrontal cortex of PTSD rats intervened by calming-shen and regulating-kidney electro-acupuncture method. Basic Clin. Pharmacol. Toxicol. 2018, 123, 37. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Li, K.; Ding, N.; Xie, Y.Q.; Niu, K.; Zhang, H. Effect of electroacupuncture on expression of CREB and its ability to bind to synaptic proteins in rats with post-traumatic stress disorder. Asian Pac. J. Trop. Med. 2019, 12, 7. [Google Scholar] [CrossRef]
- Zhou, C.; Xue, S.; Peng, Z.; Wang, H. Electroacupuncture pre-treatment ameliorates PTSD symptoms in rats by enhancinghippocampal neurogenesis via the Nrf2 antioxidant signal pathway. Brain Stimul. 2019, 12, 416. [Google Scholar] [CrossRef]
- Fang, Y.Q.; Cai, D.J.; Zhou, Q.Z.; Yu, S.G.; Peng, X.H.; Zheng, Z. Comparative research on intervention in anxiety behavior of PTSD-like rats by electro-acupncture and repetitive transcranial magnetic stimulation and serum corticosterone. J. Nanjing Univ. TCM 2012, 28, 357–359. [Google Scholar]
- Hou, L.Q.; Liu, S.; Xiong, K.R. Effects of electroacupuncture on hippocampal nNOS expression in rats of post-traumatic stress disorder model. Chin. Acupunct. Moxibustion 2013, 33, 632–636. [Google Scholar]
- Hou, L.Q.; Liu, S.; Xiong, K.R. Effects of electroacupuncture intervention on behavior changes and hippocampal glucocorticoid receptor and mineralocorticoid receptor expression levels in post-traumatic stress disorder rats. Acupunct. Res. 2013, 38, 140–145. [Google Scholar]
- Li, Y.M.; Zhao, G.J. Effect of electroacupuncture on body weight and spatial learning and memory in PTSD rats. Heilongjiang Med. J. 2014, 38, 233–235. [Google Scholar] [CrossRef]
- Xie, K.N.; Tang, G.Q.; Zhan, H.B.; Yang, K.; Zhao, J. Effect of electroacupuncture on locus nNOS expression in rats of post-traumatic stress disorder model. J. Med. Theor. Pr. 2015, 28, 2421–2423. [Google Scholar]
- Li, R. Electroacupuncture Preconditioning Ameliorates Anxiety-Like Behavior and Cognitive Impairments in Posttraumatic Stress Disorder Model via Upregulation of Thioredoxin Reductases. Master’s Thesis, Shaanxi University of Chinese Medicine, Shaanxi, China, 2016. [Google Scholar]
- Li, F.L.; Zhou, C.H.; Peng, Z.W.; Xue, S.S. The influence of electroacupuncture (EA) preconditioning on anxiety-like behavior and the expression of Sirt1/MAO-A in the hippocampus of PTSD rats. Prog. Mod. Biomed. 2017, 17, 6839–6843. [Google Scholar] [CrossRef]
- Ding, N. Study of the Effects on Fear Memory of PTSD Rats Intervened by Calming Shen-Restoring Consciousness-Regulating Kidney Electro-Acupuncture Therapy Based on BDNF-TrkB-ERK Pathway in Amygdala. Master’s Thesis, Chengdu University of Traditional Chinese Medicine, Chengdu, China, 2018. [Google Scholar]
- Chen, Y.H.; Xue, F.; Gu, T.T.; Wang, S.Q.; Wang, H.N.; Peng, Z.W. Effect of electroacupuncture pretreatment on anxiety-like behavior and expression of endogenous cannabinoid related genes in the prefrontal cortex of PTSD rats model. J. Neurosci. Ment. Health 2019, 19, 658–662. [Google Scholar] [CrossRef]
- Li, M.; Li, K.; Zhang, H.; Jiang, Y. Study on the mechanism of TMRK electroacupuncture in repairing synaptic plasticity in amygdala and hippocampus to relieve fear memory in PTSD rats. Technol. Health Care 2019, 27, S425–S443. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Liu, H.; Hou, Y.; Shen, J.; Qu, X.; Liu, S. Temporal effect of electroacupuncture on anxiety-like behaviors and c-Fos expression in the anterior cingulate cortex in a rat model of post-traumatic stress disorder. Neurosci. Lett. 2019, 711, 134432. [Google Scholar] [CrossRef]
- Wei, K.X.; Huang, C.L.; Chen, X.P.; Cao, H. Effects of electrical acupuncturing in Baihui acupoint on sleep phases of post-traumatic stress disorder rats and the mechanisms. Shaanxi J. Tradit. Chin. Med. 2019, 40, 1333–1335. [Google Scholar] [CrossRef]
- Xue, F.; Xue, S.S.; Liu, L.; Sang, H.F.; Ma, Q.R.; Tan, Q.R.; Wang, H.N.; Zhou, C.H.; Peng, Z.W. Early intervention with electroacupuncture prevents PTSD-like behaviors in rats through enhancing hippocampal endocannabinoid signaling. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2019, 93, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.H.; Xue, F.; Xue, S.S.; Sang, H.F.; Liu, L.; Wang, Y.; Cai, M.; Zhang, Z.J.; Tan, Q.R.; Wang, H.N.; et al. Electroacupuncture pretreatment ameliorates PTSD-like behaviors in rats by enhancing hippocampal neurogenesis via the Keap1/Nrf2 antioxidant signaling pathway. Front. Cell. Neurosci. 2019, 13. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.L.; Lu, Y.P. Electroacupuncture inhibits increase of TH and decrease of BDNF in the amygdala of PTSD rats. Acta Acad. Med. Wannan. 2019, 38, 115–119. [Google Scholar] [CrossRef]
- Zhao, Z.T. Study on the Effect of “Dispersing Liver and Regulating Spirit” Acupuncture Method on Hippocampal Neural Coding and Functional Reconfiguration of PTSD Rats with Sleep Disorder. Ph.D. Thesis, Chengdu University of Traditional Chinese Medicine, Chengdu, China, 2016. [Google Scholar]
- Han, Y.D. Study on the Effect of “Dispersing Liver and Regulating Spirit” Acupuncture Method on the Neuroethology and the Cognitive Dysfunction of PTSD Rats. Master’s Thesis, Gansu University of Chinese Medicine, Gansu, China, 2017. [Google Scholar]
- Oh, J.Y.; Kim, Y.K.; Kim, S.N.; Lee, B.; Jang, J.H.; Kwon, S.; Park, H.J. Acupuncture modulates stress response by the mTOR signaling pathway in a rat post-traumatic stress disorder model. Sci. Rep. 2018, 8, 11864. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.T.; Yan, X.K.; Han, Y.D.; Zhang, Y.F. Effect of liver-soothing and mind-regulating acupuncture on resting-state electroencephalographic signals in rats with post-traumatic stress disorder. J. Acupunct. Tuina Sci. 2018, 16, 289–296. [Google Scholar] [CrossRef]
- Zhang, Y.F.; Han, Y.D.; Zhao, Z.T.; Yan, X.K. Study on “liver-soothing and mind-regulating” acupuncture manipulation in regulating the blood-oxygen concentration in cerebral cortex of PTSD rats. World J. Moxibustion 2018, 28, 198–203. [Google Scholar] [CrossRef]
- Zhao, Y.K.; Han, Y.; Zhang, Y.F.; Zhu, T.T.; Ma, C.B.; Zhao, Z.T.; Yan, X.K. Acupuncture intervention improves behavior reactions and learning-memory ability in post-traumatic stress disorder rats. Acupunct. Res. 2018, 43, 562–566. [Google Scholar] [CrossRef]
- Zhao, Z.T.; Zhang, A.; Zhang, Y.F.; Zhu, T.T.; Zhao, Y.K.; Liu, A.G.; Yan, X.K. Effects of dispersing liver and regulating spirit acupuncture therapy on spatial and temporal patterns of neural coding in hippocampal CA1, CA3 regions of rats with PTSD. China J. Tradit. Chin. Med. Pharm. 2018, 33, 3895–3900. [Google Scholar]
- Yu, C.; Tian, l.; Zhang, S.H.; Yao, Y. Effect of acupuncture and moxibustion on the spatial and temporal patterns of abnormal neuronal information in hippocampus of rats with sleep disroder induced by post-traumatic stress disroder and the ultrastructure of damaged neurons. J. Sichuan Tradit. Chin. Med. 2019, 37, 29–32. [Google Scholar]
- Zhao, Z.T.; Zhao, Y.K.; Zhu, T.T.; Xing, J.M.; Bu, X.M.; Zhang, Y.F.; Yan, X.K. Effects of acupuncture on neuro-electrophysiological activities in hippocampal CA1 and CA3 areas of rats with post-traumatic stress disorder. J. Acupunct. Tuina Sci. 2019, 17, 67–73. [Google Scholar] [CrossRef]
- Dunlop, B.W.; Wong, A. The hypothalamic-pituitary-adrenal axis in PTSD: Pathophysiology and treatment interventions. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 361–379. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.-G.; Zhu, X.-H.; Nemes, A.D.; Zhu, D.-Y. Neuronal nitric oxide synthase and affective disorders. IBRO Rep. 2018, 5, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.P.; Patel, P.D.; Akil, H.; Watson, S.J. Localization and regulation of glucocorticoid and mineralocorticoid receptor messenger RNAs in the hippocampal formation of the rat. Mol. Endocrinol. 1989, 3, 1886–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Kloet, E.R.; Oitzl, M.S.; Joëls, M. Functional implications of brain corticosteroid receptor diversity. Cell Mol. Neurobiol. 1993, 13, 433–455. [Google Scholar] [CrossRef]
- Zhou, Q.G.; Zhu, L.J.; Chen, C.; Wu, H.Y.; Luo, C.X.; Chang, L.; Zhu, D.Y. Hippocampal neuronal nitric oxide synthase mediates the stress-related depressive behaviors of glucocorticoids by downregulating glucocorticoid receptor. J. Neurosci. Off. J. Soc. Neurosci. 2011, 31, 7579–7590. [Google Scholar] [CrossRef]
- Acheson, D.T.; Gresack, J.E.; Risbrough, V.B. Hippocampal dysfunction effects on context memory: Possible etiology for posttraumatic stress disorder. Neuropharmacology 2012, 62, 674–685. [Google Scholar] [CrossRef] [Green Version]
- Duman, R.S. Neuronal damage and protection in the pathophysiology and treatment of psychiatric illness: Stress and depression. Dialogues Clin. Neurosci. 2009, 11, 239–255. [Google Scholar] [CrossRef]
- Mahan, A.L.; Ressler, K.J. Fear conditioning, synaptic plasticity and the amygdala: Implications for posttraumatic stress disorder. Trends Neurosci. 2012, 35, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Etkin, A.; Egner, T.; Kalisch, R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn. Sci. 2011, 15, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etkin, A.; Egner, T.; Peraza, D.M.; Kandel, E.R.; Hirsch, J. Resolving emotional conflict: A role for the rostral anterior cingulate cortex in modulating activity in the amygdala. Neuron 2006, 51, 871–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velazquez, F.N.; Caputto, B.L.; Boussin, F.D. c-Fos importance for brain development. Aging 2015, 7, 1028–1029. [Google Scholar] [CrossRef] [Green Version]
- Hamner, M.B.; Lorberbaum, J.P.; George, M.S. Potential role of the anterior cingulate cortex in PTSD: Review and hypothesis. Depress Anxiety 1999, 9, 1–14. [Google Scholar] [CrossRef]
- Harkany, T.; Mackie, K.; Doherty, P. Wiring and firing neuronal networks: Endocannabinoids take center stage. Curr. Opin. Neurobiol. 2008, 18, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, R.R.; Noble, L.J.; McIntyre, C.K. Using the single prolonged stress model to examine the pathophysiology of PTSD. Front. Pharmacol. 2017, 8, 615. [Google Scholar] [CrossRef]
- Speer, K.E.; Semple, S.; Naumovski, N.; D’Cunha, N.M.; McKune, A.J. HPA axis function and diurnal cortisol in post-traumatic stress disorder: A systematic review. Neurobiol. Stress 2019, 11, 100180. [Google Scholar] [CrossRef]
- Carletto, S.; Borsato, T.; Pagani, M. The role of slow wave sleep in memory pathophysiology: Focus on post-traumatic stress disorder and eye movement desensitization and reprocessing. Front. Psychol. 2017, 8, 2050. [Google Scholar] [CrossRef]
- Germain, A. Sleep disturbances as the hallmark of PTSD: Where are we now? Am. J. Psychiatry 2013, 170, 372–382. [Google Scholar] [CrossRef]
- Shergis, J.L.; Ni, X.; Jackson, M.L.; Zhang, A.L.; Guo, X.; Li, Y.; Lu, C.; Xue, C.C. A systematic review of acupuncture for sleep quality in people with insomnia. Complementary Ther. Med. 2016, 26, 11–20. [Google Scholar] [CrossRef]
- Feng, H.; Liu, Y.; Xu, H.; Liu, Y.H.; Chen, G.L.; Liu, W.J. Effect of acupuncture and estazolam on episodic memory and sleep structure in patients with chronic insomnia disorder: A randomized controlled trial. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2020, 40, 707–712. [Google Scholar] [CrossRef]
- Kim, T.D.; Lee, S.; Yoon, S. Inflammation in post-traumatic stress disorder (PTSD): A review of potential correlates of PTSD with a neurological perspective. Antioxidants 2020, 9, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dincheva, I.; Lynch, N.B.; Lee, F.S. The Role of BDNF in the development of fear learning. Depress Anxiety 2016, 33, 907–916. [Google Scholar] [CrossRef] [Green Version]
- Church, D.; Feinstein, D. The manual stimulation of acupuncture points in the treatment of post-traumatic stress disorder: A review of clinical emotional freedom techniques. Med. Acupunct. 2017, 29, 194–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Church, D.; Stapleton, P.; Yang, A.; Gallo, F. Is tapping on acupuncture points an active ingredient in emotional freedom techniques? A systematic review and meta-analysis of comparative studies. J. Nerv. Ment. Dis. 2018, 206, 783–793. [Google Scholar] [CrossRef]
- MacPherson, H.; Maschino, A.C.; Lewith, G.; Foster, N.E.; Witt, C.M.; Vickers, A.J. Characteristics of acupuncture treatment associated with outcome: An individual patient meta-analysis of 17,922 patients with chronic pain in randomised controlled trials. PLoS ONE 2013, 8, e77438. [Google Scholar] [CrossRef]
- Langevin, H.M.; Wayne, P.M.; Macpherson, H.; Schnyer, R.; Milley, R.M.; Napadow, V.; Lao, L.; Park, J.; Harris, R.E.; Cohen, M.; et al. Paradoxes in acupuncture research: Strategies for moving forward. Evid. Based Complement Altern. Med. 2011, 2011, 180805. [Google Scholar] [CrossRef]
- Lundeberg, T.; Lund, I.; Sing, A.; Näslund, J. Is placebo acupuncture what it is intended to be? Evid. Based Complementary Altern. Med. Ecam. 2011, 2011, 932407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, J.J.; Xie, S.X.; Bowman, M.A. Uncovering the expectancy effect: The validation of the acupuncture expectancy scale. Altern. Ther. Health Med. 2010, 16, 22–27. [Google Scholar]
- Zheng, C.; Tan, L.; Zhou, T.; Zhang, H. Effects of electroacupuncture on resting-state encephalic functional connectivity network in patients with PTSD. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2015, 35, 469–473. [Google Scholar]
- Wang, Y.; Hu, Y.P.; Wang, W.C.; Pang, R.Z.; Zhang, A.R. Clinical studies on treatment of earthquake-caused posttraumatic stress disorder using electroacupuncture. Evid. Based Complement Altern. Med. 2012, 2012, 431279. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Study | Species (Sex) | Age/Weight | PTSD Model Method | Main Outcome | Main Results Compared to MG (Acupuncture Group) |
|---|---|---|---|---|---|
| Fang 2012 [27] | SD rats (male) | NR/180–220 g | SPS | 1. EPM (1) Time spent in open arms, (2) Entries in open arms 2. Serum corticosterone | 1. (1) ↑ *, (2) ↑ † 2. ↓ * |
| Hou 2013a [28] | SD rats (male) | NR/220 ± 20 g | SPS | 1. nNOS mRNA expression in hippocampus 2. nNOS protein expression in hippocampal (1) CA1 and (2) CA3 regions | 1. ↓ * 2. (1) ↑ *, (2) ↑ * |
| Hou 2013b [29] | SD rats (male) | NR/220 ± 20 g | SPS | 1. MWM (escape latency) 2. Protein expression in hippocampus (1) Glucocorticoid receptor, (2) Mineralocorticoid receptor 3. Ratio of mineralocorticoid receptor/glucocorticoid receptor expression | 1. ↓ * 2. (1) ↓ *, (2) ↑ * 3. ↑ * |
| Li 2014 [30] | SD rats (male) | NR/180–220 g | Compound stress stimulation of restraint, electric shock, and exhaustive swimming | 1. MWM (1) Escape latency, (2) Percent time in the III quadrant, (3) Crossing number in the III quadrant | 1. (1) ↓ *, (2) ↑ *, (3) ↑ * |
| Xie 2015 [31] | SD rats (male) | NR/200–250 g | SPS | 1. Behavioral observation (1) Number of grids, (2) Number of erection 2. Locus coeruleus nNOS positive cells 3. Mean gray value | 1. (1) ↑ †, (2) ↑ † 2. ↓ † 3. ↑ † |
| Li 2016 [32] | SD rats (male) | NR/ 280–320 g | SPS | 1. Freezing condition (freezing time) 2. EPM (1) Time spent in open arms, (2) Entries in open arms 3. Protein expression in hippocampus (1) Ask-1, (2) Bax, (3) Trx | 1. ↓ * 2. (1) ↑ †, (2) ↑ † 3. (1) ↓ *, (2) ↓ *, (3) ↑ * |
| Li 2017 [33] | SD rats (male) | 8 weeks/250 ± 20 g | SPS&S | 1. OFT (1) Entries in center, (2) time spent in center 2. EPM (Time spent in open arms) 3. mRNA expression in hippocampus (1) Sirt1, (2) MAO-A | 1. (1) ↑ †, (2) ↑ * 2. ↑ * 3. (1) ↓ †, (2) ↓ * |
| Ding 2018 [34] | SD rats (male) | NR/NR | SPS&S | 1. Scene conditioned fear response detection (1) Memory acquisition, (2) Memory extinction, (3) Memory reconstruction 2. Cue conditioned fear response detection (1) Memory acquisition, (2) Memory extinction, (3) Memory reconstruction 3. Protein expression in amygdala (1) BDNF, (2) TrkB, (3) p-ERK, (4) p-MEK, (5) p-ERK1/2 | 1. (1) N.S., (2) ↓ †, 3) ↓ † 2. (1) N.S. or ↓ * or ↓ †, (2) ↓ †, (3) ↓ † 3. (1) ↑ †, (2) ↑ †, (3) ↑ †, (4) ↑ †, (5) ↑ † |
| Chen 2019 [35] | SD rats (male) | 8 weeks/220 ± 20 g | Enhanced SPS | 1. OFT (1) Time spent in center, (2) Entries in center 2. EPM (1) Time spent in open arms, (2) Entries in open arms 3. Expression in prefrontal lobe (1) Endocannabinoid receptor type 1, (2) Monoacylglycerol lipase, (3) Diacylglycerol lipase | 1. (1) N.S., (2) ↑ * 2. (1) ↑ *, (2) ↑ * 3. (1) ↑ *, (2) ↑ *, (3) N.S. |
| Li 2019 [36] | SD rats (male) | 2 months/180–220 g | MG1: SPS MG2: SPS&S | 1. Radial six-arm water maze test (1) Escape latency, (2) Distance travelled 2. Locomotor activity (1) Distance, (2) Shock intensity 3. EPM (1) Time spent in open arms, (2) Entries in open arms 4. Assessment of conditional fear response (1) Memory acquisition, (2) Memory extinction 5. PSD thickness (1) Amygdala, (2) Hippocampus 6. Synaptic gap width (1) Amygdala, (2) Hippocampus 7. Curvature of synaptic interfact (1) Amygdala, (2) Hippocampus 8. BDNF levels (1) Amygdala, (2) Hippocampus 9. fEPSP amplitude of hippocampus 10. Protein expression in amygdala (1) SYN, (2) GAP43, (3) PSD95 11. mRNA expression in amygdala (1) SYN, (2) GAP43, (3) PSD95 12. Protein expression in hippocampus (1) SYN, (2) GAP43, (3) PSD95 13. mRNA expression in hippocampus (1) SYN, (2) GAP43, (3) PSD95 | MG1 + acupuncture, MG2 + acupuncture 1. (1) ↑ †, ↑ †, (2) ↑ †, ↑ † 2. (1) ↑ * or ↑ †, ↑ * or ↑ †, (2) N.S., N.S. 3. (1) ↑ †, ↑ †, (2) ↑ †, ↑ † 4. (1) N.S. or ↓ * or ↓ †, N.S. or ↓ * or ↓ †, (2) ↓ †, ↓ † 5. (1) ↑ *, ↑ *, (2) ↑ *, ↑ † 6. (1) N.S., N.S., (2) N.S., ↓ * 7. (1) N.S., ↑ *, (2) ↑ †, ↑ † 8. (1) ↑ *, ↑ †, (2) ↑ †, ↑ † 9. p-value was not presented 10. (1) ↑ †, ↑ †, (2) ↑ †, ↑ †, (3) ↑ †, ↑ † 11. (1) ↑ †, ↑ †, (2) ↑ †, ↑ †, (3) ↑ †, ↑ † 12. (1) ↑ †, ↑ †, (2) ↑ †, ↑ †, (3) ↑ †, ↑ † 13. (1) ↑ †, ↑ †, (2) ↑ †, ↑ †, (3) ↑ †, ↑ † |
| Liu 2019 [37] | SD rats (male) | NR/180–220 g | SPS | 1. OFT (1) Time spent in center, (2) Total distance 2. EPM (time spent in open arms) 3. Serum corticosterone 4. Fos-positive nuclei in the anterior cingulate cortex | 1. (1) ↑ †, (2) N.S. 2. ↑ * 3. ↓ * 4. ↑ * |
| Wei 2019 [38] | SD rats (male) | NR/250 ± 10 g | SPS | 1. REMS 2. Slow wave sleep stage 1 3. Slow wave sleep stage 2 4. Levels in hypothalamus (1) IL-1β, (2) TNF-α, (3) IL-4, (4) IL-10 | 1. ↑ * 2. N.S. 3. ↑ * 4. (1) N.S., (2) ↓ *, (3) ↓ *, (4) N.S. |
| Xue 2019 [39] | SD rats (male) | NR/280–320 g | Enhanced SPS | 1. OFT (1) Total distance, (2) Time spent in center, (3) Distance traveled in center 2. EPM (1) Time spent in open arms, (2) Entries in open arms, (3) distance traveled in open arms 3. Fear conditioning test (1) contextual freezing time, (2) cued freezing time 4. Protein expression in hippocampus (1) BDNF, (2) PSD95, (3) Syn, (4) CB1R, (5) DAGLα | 1. (1) N.S., (2) ↑ *, (3) ↑ * 2. (1) ↑ *, (2) ↑ *, (3) ↑ * 3. (1) ↓ *, (2) ↓ * 4. (1) ↑ *, (2) ↑ *, (3) ↑ *, (4) ↑ *, (5) ↑ † |
| Zhou 2019 [40] | SD rats (male) | NR/280–320 g | Enhanced SPS | 1. OFT (1) Total distance, (2) Time spent in center 2. EPM (1) Time spent in open arms, (2) Entries in open arms 3. Fear conditioning test (1) contextual freezing time, (2) cued freezing time 4. Number of cells in dentate gyrus (1) BrdU † cells, (2) DCX † cells, (3) NeuN †/Nrf2 † cells, (4) GFAP †/Nrf2 † cells 5. Ratio of DCX/β-actin 6. Ratio of BDNF/β-actin 7. Ratio of pAMPKα/AMPKα 8. Ratio of Nrf2/β-actin 9. Ratio of HO-1/β-actin | 1. (1) N.S., (2) ↑ * 2. (1) ↑ *, (2) ↑ * 3. (1) ↓ *, (2) ↓ * 4. (1) ↑ *, (2) ↑ *, (3) ↑ *, (4) ↑ * 5. ↑ * 6. ↑ * 7. ↑ * 8. ↑ † 9. ↑ † |
| Zhu 2019 [41] | SD rats | NR/NR | SPS | 1. Number in amygdala (1) BDNF positive neuron, (2) Tyrosine hydroxylase positive fiber | 1. (1) ↓ †, (2) ↓ † |
| Zhao 2016 [42] | SD rats (male) | 2 month old/180–220 g | SPS & S | Experiment (A) 1. Non-REMS latency (min) for 12 h in daytime 2. REMS latency (min) for 12 h in daytime 3. Awakening period (min) for 12 h in daytime 4. Total sleep time (min) for 12 h in daytime Experiment (B) 1. Action potential release of hippocampal 1) CA1 and 2) CA3 regions 2. Discharge frequency of hippocampal 1) CA1 and 2) CA3 regions (Hz) 3. Wave amplitude of hippocampal 1) CA1 and 2) CA3 regions (μV) 4. Interspike interval of hippocampal 1) CA1 and 2) CA3 regions 5. Power spectral densities of hippocampal 1) CA1 and 2) CA3 regions | Experiment (A) 1. ↓ † 2. ↓ * 3. ↓ † 4. ↑ † Experiment (B) 1. (1) ↑ †, (2) ↑ † 2. (1) ↑ †, (2) ↑ † 3. (1) ↑ †, (2) ↑ † 4. (1) ↓ *, (2) ↓ † 5. (1) ↑ *, (2) ↑ † |
| Han 2017 [43] | SD rats (male) | 6 weeks old/180 ± 20 g | SPS&S | 1. OFT (1) Horizontal crossing grid number, (2) Vertical frequency, (3) Number of fecal particle 2. MWM (1) Daily latency during positioning navigation experiment (sec), (2) Space exploration experiment-times crossing platform, (3) Space exploration experiment-times crossing the effective areas 3. New object recognition test (discrimination index) 4. EEG power spectrum values of bilateral cerebral hemispheres (left/right) (1) α-wave, (2) β-wave, (3) δ’-wave, (4) θ-wave | 1. (1) ↑ †, (2) ↑ †, (3) ↓ † 2. (1) ↓ †, (2) ↑ †, (3) ↑ † 3. ↑ † 4. (1) ↑ †, (2) ↓ †, (3) ↓ †, (4) ↓ † |
| Oh 2018 [44] | SD rats (male) | 8 weeks old/200–220 g | SPS | Experiment (A) 1. FST (1) Immobility time (s), (2) Climbing time (s), (3) Swimming time (s) 2. OFT (1) Entries in center, (2) Travel distance (cm) 3. EPM (1) Entries in open arms, (2) Entries in closed arms, (3) Time spent in open arms (open/total), (4) Anxiety index 4. Corticotrophin-releasing factor expression levels in the paraventricular nucleus of hypothalamus by immunofluorescence 5. Serum corticosterone (pg/mL) 6. Protein expression levels in the hippocampus (1) Extracellular signal-regulated kinase, (2) Akt, (3) mTOR, (4) p70S6K, (5) 4E-BP-1, (6) CREB 7. Synaptic protein expression levels in the hippocampus (1) PSD95, (2) Syn1, (3) GluR1, (4) BDNF Experiment (B) 1. FST (1) Immobility time (s), (2) Climbing time (s), (3) Swimming time (s) 2. OFT (1) Entries in center, (2) Travel distance (cm) 3. EPM (1) Entries in open arms, (2) Entries in closed arms, (3) Time spent in open arms (open/total), (4) Anxiety index | Experiment (A) 1. (1) ↓ †, (2) ↑ †, (3) N.S. 2. (1) ↑ †, (2) N.S. 3. (1) ↑ †, (2) N.S., (3) ↑ †, (4) ↑ † 4. ↓ † 5. ↓ † 6. (1) N.S., (2) ↑ †, (3) ↑ *, (4) ↑ †, (5) ↑ †, (6) ↑ † 7. (1) ↑ †, (2) ↑ †, (3) ↑ *, (4) ↑ † Experiment (B) 1. (1) ↓ †, (2) ↑ †, (3) N.S. 2. (1) ↑ †, (2) ↑ * 3. (1) ↑ †, (2) ↑ *, (3) ↑ †, (4) ↑ † |
| Wei 2018 [45] | SD rats (male) | 6 weeks old/180 ± 20 g | SPS & S | 1. MWM (1) Daily latency during positioning navigation experiment (sec), (2) Space exploration experiment-times crossing platform, 3) Space exploration experiment-times crossing the effective areas 2. EEG power spectrum values of bilateral cerebral hemispheres (left/right) (1) α-wave, (2) β-wave, (3) δ’-wave, (4) θ-wave | 1. (1) ↓ *, (2) ↑ *, (3) ↑ * 2. (1) ↑ †, (2) ↓ †, (3) ↓ †, (4) ↓ † |
| Zhang 2018 [46] | SD rats (male) | 6 weeks old/180 ± 20 g | SPS & S | 1. fNIRs (1) Oxy-Hb, (2) Deoxy-Hb, (3) Total-Hb | 1. (1) ↓ *, (2) ↑ *, (3) ↓ * |
| Zhao 2018 [47] | SD rats (male) | 6 weeks old/180 ± 20 g | SPS & S | 1. OFT (1) Horizontal crossing grid number, (2) Vertical frequency, (3) Number of fecal particle 2. MWM (1) Location navigation (escape latency), (2) Special probe tests (platform quadrant crossing times) 3. Discrimination index | 1. (1) ↑ *, (2) ↑ *, (3) ↓ * 2. (1) ↓ *, (2) ↑ * 3. ↑ * |
| Zhao 2018 [48] | SD rats (male) | 2 month old/200 ± 20 g | SPS & S | 1. Discharge frequency of hippocampal (1) CA1 and (2) CA3 regions (Hz) 2. Wave amplitude of hippocampal (1) CA1 and (2) CA3 regions (μV) | 1. (1) ↑ †, (2) ↑ † 2. (1) ↑ †, (2) ↑ † |
| Yu 2019 [49] | Wistar rats (male) | 8 weeks old/203.47 ± 6.29 g | SPS & S | 1. Non-REMS latency (min) 2. REMS latency (min) 3. Amplitude and ultrastructure of the neurons in the hippocampal (1) CA1 and (2) CA3 regions | 1. ↓ * 2. ↓ * 3. (1) ↑ *, (2) ↑ * |
| Zhao 2019 [50] | SD rats (male) | 2 month old/200 ± 20 g | SPS & S | 1. Interspike interval of hippocampal (1) CA1 and (2) CA3 regions 2. Power spectral densities of hippocampal (1) CA1 and (2) CA3 regions | 1. (1) ↓ *, (2) ↓ † 2. (1) ↓ *, (2) ↓ † |
| Study | Target Symptom | Proposed Mechanism |
|---|---|---|
| Electro-Acupuncture | ||
| Fang 2012 [27] | Anxiety symptom | Downregulation of HPA axis activity |
| Hou 2013a [28] | Spatial learning and memory * | Downregulation of hippocampal nNOS expression |
| Hou 2013b [29] | Spatial learning and memory | Upregulation of hippocampal mineralocorticoid receptor expression Downregulation of hippocampal glucocorticoid receptor expression |
| Li 2014 [30] | Spatial learning and memory | NR |
| Xie 2015 [31] | Excessive stress response * | Downregulation of nNOS expression in locus coeruleus |
| Li 2016 [32] | Anxiety symptom | Upregulation of hippocampal Trx expression (relieve the nerve injury) |
| Li 2017 [33] | Conditioned fear | Restoration of the mRNA level of Sirt1 and MAO-A in the hippocampus |
| Ding 2018 [34] | Anxiety symptom | Upregulation of BDNF, TrkB, p-MEK, and p-ERK expression in the amygdala Activating BDNF-TrkB-ERK signaling pathway |
| Chen 2019 [35] | Anxiety symptom | Increasing CB1R and DAGLα expression in the PFC |
| Li 2019 [36] | Fear memory | Repair of synaptic plasticity in amygdala and hippocampus |
| Liu 2019 [37] | Fear memory | Increasing Fos expression in the ACC |
| Wei 2019 [38] | Sleep disturbance | Regulation TNF-α and IL-4 levels in the hypothalamus |
| Xue 2019 [39] | Anxiety symptom and fear learning | Improvement of hippocampal synaptic plasticity Increasing BDNF, DAGLα, and CB1R expression |
| Zhou 2019 [40] | Anxiety symptom | Improvement of hippocampal neurogenesis Upregulation of the molecular mechanism associated with protection against oxidative damage and of BDNF expression |
| Zhu 2019 [41] | Fear learning * | Prevention TH from increasing and BDNF from decreasing in amygdala |
| Manual Acupuncture | ||
| Zhao 2016 [42] | Sleep disturbance | Restoring the hippocampal neural structure |
| Han 2017 [43] | Spatial learning and memory | Improvement of the abnormal EEG power spectrum value |
| Oh 2018 [44] | Depression and anxiety symptom | Increasing protein synthesis required for synaptic plasticity via the mTOR pathway in the hippocampus |
| Wei 2018 [45] | Spatial learning and memory | Improvement of the abnormal EEG activity |
| Zhang 2018 [46] | Not specific (abnormal neuron activity) * | Regulatory effect on the blood-oxygen concentration in cerebral cortex |
| Zhao 2018 [47] | Anxiety and learning-memory ability | NR |
| Zhao 2018 [48] | Fear memory * | Regulation of abnormal neuron cluster electrical activity of hippocampal CA1 and CA3 regions. |
| Yu 2019 [49] | Sleep disturbance | Reversing the discharge activity of neurons in hippocampus and restoring the structure of neuron cells |
| Zhao 2019 [50] | Excessive stress response * | Regulation of the neuro-electrophysiology activity of hippocampal CA1 and CA3 regions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.-Y.; Lee, B.; Kim, S.-H. Efficacy and Underlying Mechanism of Acupuncture in the Treatment of Posttraumatic Stress Disorder: A Systematic Review of Animal Studies. J. Clin. Med. 2021, 10, 1575. https://doi.org/10.3390/jcm10081575
Kwon C-Y, Lee B, Kim S-H. Efficacy and Underlying Mechanism of Acupuncture in the Treatment of Posttraumatic Stress Disorder: A Systematic Review of Animal Studies. Journal of Clinical Medicine. 2021; 10(8):1575. https://doi.org/10.3390/jcm10081575
Chicago/Turabian StyleKwon, Chan-Young, Boram Lee, and Sang-Ho Kim. 2021. "Efficacy and Underlying Mechanism of Acupuncture in the Treatment of Posttraumatic Stress Disorder: A Systematic Review of Animal Studies" Journal of Clinical Medicine 10, no. 8: 1575. https://doi.org/10.3390/jcm10081575
APA StyleKwon, C. -Y., Lee, B., & Kim, S. -H. (2021). Efficacy and Underlying Mechanism of Acupuncture in the Treatment of Posttraumatic Stress Disorder: A Systematic Review of Animal Studies. Journal of Clinical Medicine, 10(8), 1575. https://doi.org/10.3390/jcm10081575