1. Introduction
Low back pain is a health problem characterized by high prevalence in the general population, particularly in Western societies, with significant economic and social repercussions. Low back pain is one of the major reasons for medical treatment seeking and is one of the most challenging chronic pain disorders to treat [
1]. In addition, low back pain has become one of the first causes of work absenteeism [
2]. It is expected that between 60% and 80% of the world population will experience low back pain during their lifetime [
3], with 65% being recurrent and longstanding episodes. It becomes chronic by up to 5–10%, it evolves to chronic disability and consumes up to 75% of the total resources dedicated to lumbar disease [
4,
5,
6,
7,
8,
9]. Although low back pain can be caused by different muscle-skeletal etiologies (muscle overcharge, ligament strains, herniated discs, osteoarthritis, scoliosis, or osteoporosis-related fractures), in most cases (80%), the cause of low back pain cannot be attributed to any specific structural lesion [
4]. The pathophysiology of back pain is complex and, although mechanical and inflammatory responses are very frequent, peripheral and central neurological sensitization processes have a relevant role when the neuropathic component is predominant [
10,
11,
12]. Estimates of the proportion of chronic low back pain patients with a neuropathic component range from 17 to 54% and vary according to the diagnostic method used [
10,
12,
13,
14,
15]. However, the neuropathic component in chronic back pain may be underestimated [
16] because approximately 28% of patients had an uncertain diagnosis [
11].
Compared to inflammatory pain, neuropathic pain has a greater impact on sleep disturbances, anxiety, and reduction in quality of life and functional capacity [
15,
17,
18,
19], and from the economic point of view, a higher healthcare expenditure (high pharmaceutical cost, and increase in the number of emergencies, hospitalizations, and complications) [
15,
17,
20]. Despite the negative economic impact, therapies for neuropathic pain show only modest evidence of efficacy. Typically, no more than half of patients experience clinically significant pain relief with currently available pharmacotherapy, and these drugs are associated with a risk of significant adverse effects. Despite the variety of treatments available, no modality or therapeutic approach has stood out as a definitive solution [
21,
22]. Thus, there is still a demand for new approaches, less invasive and free of side effects. Non-pharmacological options for the management of chronic low back pain may also include noninvasive approaches, such as transcutaneous electrical nerve stimulation (TENS) and invasive procedures, including epidural steroid injections (ESIs) and spinal cord stimulation (SCS) [
23,
24].
Within the field of bioelectronics, the use of electromagnetic signals has had a notable increase in the past decade in acute and chronic rehabilitation treatments, and it provides a noninvasive, safe, and accurate method to stimulate therapeutic targets depending on the tissue, functional or structural location, and the type or mechanism of pain or disease [
25,
26,
27]. It has been reported that pulsed electromagnetic signals (PEMS) therapy yields several benefits into bone metabolism and osteogenesis, acute pain relief, wound healing, edema, and inflammation control, as well as in chronic pain associated with connective tissue injury and joint-associated soft tissue injury (such as in fibromyalgia and osteoarthritis) [
28,
29,
30,
31,
32]. In addition to its positive health effects, PEMS therapy has other benefits such as enhancing its potential of compliance (due to being noninvasive, low-risk level, and its absence of side effects), selectivity to act on physiological and therapeutic targets [
21], and positive results regardless of whether the low back pain is acute or chronic, or whether it has a muscular, discogenic, or complex origin [
33,
34,
35]. However, the number of studies available in the scientific literature investigating the effectiveness of PEMS on low back pain is still scarce, and even fewer if we consider low back pain subgroups [
36].
According to all the above mentioned, the present study aimed to evaluate the analgesic efficacy of PEMS therapy in patients with chronic non-specific low back pain associated with a neuropathic component using a noninvasive bioelectronic device (Physicalm®, Biotronic Advance Develop®, Granada, Spain), with a monopolar capacitive dielectric PEMS transmission.
The primary outcome of the study is analyzing the effectiveness of the PEMS therapy in reducing pain intensity and the neuropathic component. In addition, the effects of treatment on the amount and quality of sleep and health-related quality of life have been analyzed.
4. Discussion
The current randomized trial was designed to evaluate the clinical improvement in a cohort of patients with non-specific chronic low back pain associated with a neuropathic component after treatment with PEMS by using a bioelectronic therapeutic device (Physicalm
®, Biotronic Advance Develops
®, Granada, Spain), via noninvasive transcutaneous to transmit electromagnetic signals through a dielectric, capacitive monopolar transmission. Pain intensity describes how much a patient is in pain [
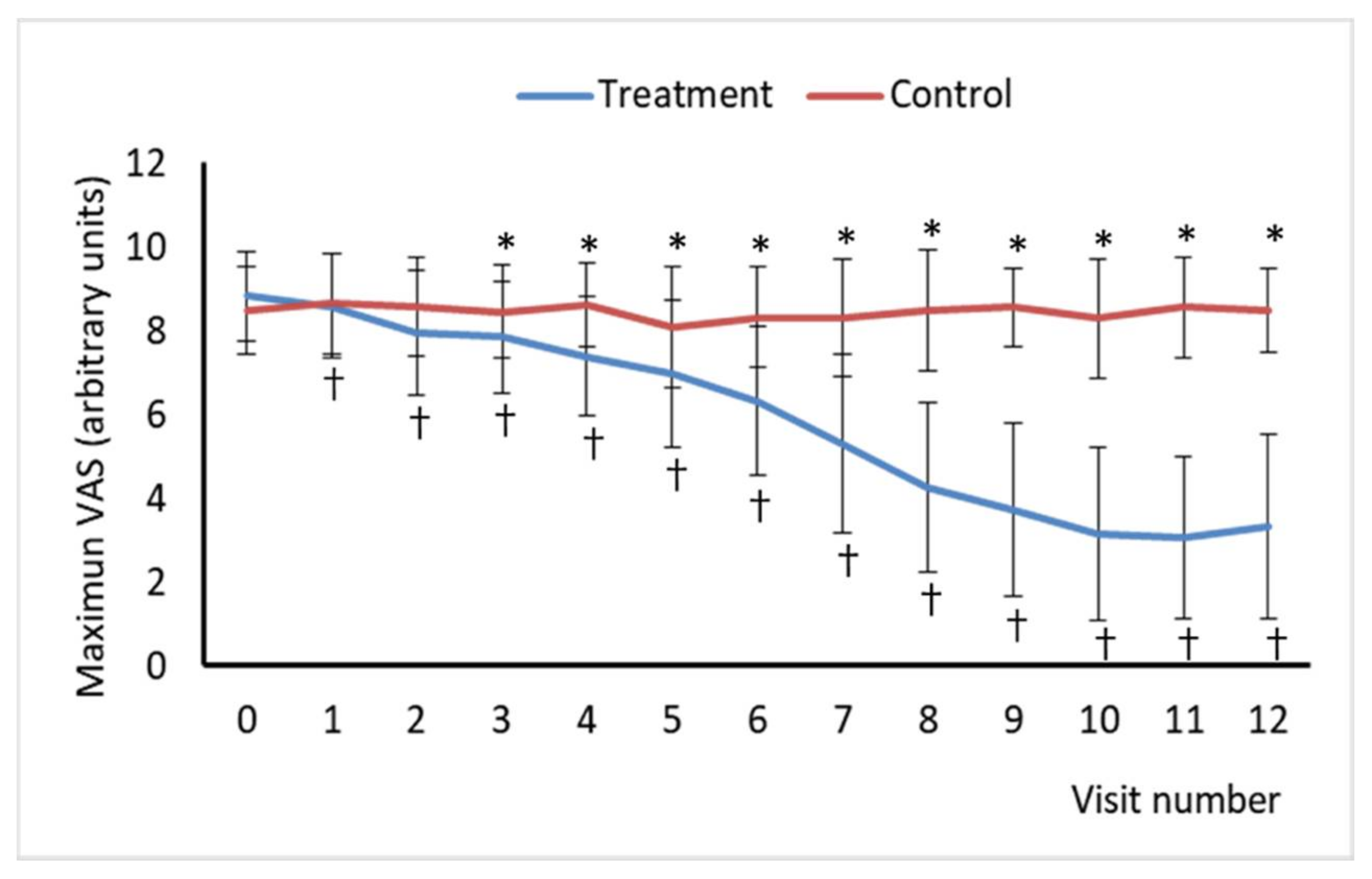
45] and is a critical component of pain experience and pain severity. Thus, the successive measurement of the intensity of low-back pain under different conditions is a key parameter for understanding the evolution of the patient’s recovery process. Pain VAS is a reliable and valid parameter [
46] that has been found to correlate positively with other self-reporting measures of pain intensity [
47,
48], and it has been demonstrated to be sensitive to treatment effect [
49]. Pain VAS scores showed a reduction in pain intensity through treatment sessions in the experimental group. In addition, the difference in pain intensity measured using VAS at two different time points represents the real difference in magnitude of pain, which seems to be the major advantage of this PEMS therapy compared to other treatments. However, the clinical importance of pain intensity is not always easy to determine [
50]. Several attempts have been made to identify the amount of change necessary to be clinically significant in pain VAS [
49]. Analgesic interventions providing a change of 10 units out of 100 in the VAS represents a clinically meaningful improvement or deterioration, and a VAS of 33 or less supposes an acceptable control of the pain. However, this ratio is more reliable at the group level than at the individual level. A change of approximately 20% for chronic back pain and 12% for acute pain is considered clinically significant [
51]. In the present study, the average difference in pain VAS score compared to the baseline was 77.1 (V11) and 66.8 (V12) in the treatment group, whereas it was 23.5 (V11) and 11.7 (V12) in the control group. These results are particularly important considering that they were obtained from visits 11 and 12, one and three months after the end of treatment, respectively, showing that the beneficial effect is still maintained in the medium term.
PEMS therapy has been investigated in many studies searching for its effects in alleviating acute and chronic pain in musculoskeletal disorders [
52]. These conditions include low back pain with different etiologies, such as generalized low back pain [
33]; acute non-specific low back pain [
21]; discogenic lumbar radiculopathy [
34], and chronic low back pain [
53]. All the mentioned studies reported a decrease in pain intensity compared to the baseline, with a mean difference in pain intensity from baseline to the endpoint from 21 to 64 points out of 100 on the VAS [
36]. Moreover, the studies on discogenic lumbar radiculopathy and lumbar myalgia showed a large effect size [
34,
35]. In addition, no differences in such improvement between the PEMS-treated group and the sham group were found in one of the studies [
21]. The inconsistent results of the PEMS treatment effect found in the literature could be a consequence of the high heterogeneity between the PEMS therapy protocols of the different studies. Overall, it can be suggested that PEMS greatly reduces the pain intensity in low back patients when used alone, independently of the low back pain condition. However, some studies found no additional benefits [
36,
52] when added to other standard therapies such as standard physiotherapy [
21] or analgesic therapy [
33], probably due to the presence of a predominant neuropathic component in the patients studied. In our study, all patients followed the usual pharmacological treatment for their painful condition (first and second step of the treatment guidelines: antiepileptics, antidepressants, weak opioids), having had poor analgesic effects. The analgesic improvement in our study may be due to the novel technique used to transmit PEMS (dielectric, capacitive and monopolar). This type of transmission adds important advantages because of the selectivity of the energy deposits on the therapeutic targets and its lack of side effects. Dielectric capacitive PEMS transmission [
37] allows energy to be transferred noninvasively to deeper tissues in a more controlled and accurate manner than conventional electrotherapy or thermotherapy systems [
38]. This system is based on tissue dielectric charge capacity [
54] to deeply transport high-frequency energy and a higher degree of focalization and density of energy applied while avoids warming the surface [
38].
The neuropathic component of low back pain was assessed using the DN4 questionnaire, whose discriminant validity for identifying neuropathic components, particularly in low back pain patients, has been confirmed in previous studies [
14,
39]. According to DN4 scores, PEMS treatment led to a clear improvement in this condition compared with placebo, with a very reduced number of individuals showing DN4 scores enough to consider that they have neuropathic pain. This is consistent with the decrease in pain intensity found in both groups, but no previous studies have evaluated the effect of PEMS on this component in patients with different low back pain conditions.
Besides pain intensity, pain-related interference with daily or at-work activities (i.e., disability) is also an important pain severity component. The SF-12 instrument was used to evaluate the increase in the quality of life perceived by the patients. This SF-12 is subdivided into two separate health constructs: the physical component summary score (PCS) and the mental component summary score (MCS). As the SF-12 is a reduced version of the MOS, it does not contain sleep behavior items. The MOS–Sleep scale, a face valid index of sleep disturbance with adequate established reliability with objective sleep measures, was also administered to evaluate the effects on sleep quality and quantity.
Health-related quality of life instruments have been widely recommended as an outcome measurement for patients with low back pain [
55,
56], and, interestingly, their reliability and validity are well established. In contrast, many physical impairments measurements have been found to be lacking in reliability and validity [
57]. In this context, generic instruments such as the SF-12 questionnaire are designed for broad use in various patient populations to broadly assess the concepts of health, disability, and quality of life. Although generic health status measures are often less responsive to changes in specific conditions than disease-specific instruments, they are important for broad comparisons of the relative impact of different conditions or treatments on the health of the population. In addition, both instruments, the MOS SF-36 and its short-form, the SF-12, have been widely used to evaluate low back pain [
58]. It is worth highlighting the excellent validity of the SF-12 criteria compared to the SF-36, because the SF-12 can explain, for both components, more than 90% of the variability of the summary scores of the original version of the questionnaire. Regarding reliability, the estimates were very high for the SF-36, close to 0.9, and lower for the SF-12, although they exceeded the expected standard of 0.7 for group comparisons [
59]. In contrast to the original dimensions of the SF-36, CSF and CSM of the SF-12 are standardized and that their interpretation is based on standards. In addition, summary components allow the number of statistical comparisons to be reduced and presenting a more symmetric distribution eliminating the ceiling and floor effects [
43]. This offers the advantage of providing a direct interpretation of the general Spanish population scores, which has a mean of 50 and a SD of 10. To calculate summary components of the SF-12, we used the weights calculated for Spain by Vilagut et al. [
43] whose values for the different dimensions are very similar to those obtained for the different language versions of the questionary [
60]. In the present study, both groups showed average components at baseline that indicated a worse state of health than the general Spanish population. Treatment improved the state of health, but it continued to be worse than in the general population.
Regarding the evaluation of the recovery of function, the authors use specific scales depending on the musculoskeletal diseases. Several scoring systems are frequently used in the clinical environment to measure the disability related to the low back condition. Up to date, studies investigating the effect of PEMS therapies on back pain did not evaluate the health-related quality of life by using the SF-12 questionnaire. However, the SF-12 tool was developed as an abbreviated version of the SF-36, containing a subset of 12 identical questions embedded in the SF-36 eight constructs [
41]. In this sense, Park et al. [
35] reported significant improvements in SF-36 prior to and following treatment in lumbar myalgia patients and no significant difference between the PEMS-treated group and the group receiving sham treatment. For these reasons, it was assumed that there was no significant difference between the two groups following the treatment [
35]. Other scales and indexes used to evaluate and quantify the recovery of participant’s function in studies assessing PEMS therapy effect on back pain are the EuroQol-5 Dimension (EQ-5D) [
35], the Modified Oswestry Low Back Pain Disability Questionnaire (OSW) [
34], the Korean version of Oswestry Disability Index (ODI) [
21,
35] and Modified Version Functional Activity Scale [
21]. In general, previous studies have demonstrated the effectiveness of PEMS in reducing the disability related to low back pain [
33,
34,
35,
53]. However, a study reported no significant improvements in the PEMS-treated group when compared to the control group [
21]. The study conducted by Omar et al. [
34] was an exception, achieving a large effect size, a 42% mean reduction after daily applications of PEMS therapy for 3 weeks. However, some caution should be taken when considering this study since they used an adapted score.
Lastly, no significant differences in the demographic information and the physical examination provided before the trial, including gender, age, studies, civil status, or economic activity, were found between the two experimental groups. In addition, no significant differences between the two experimental groups in terms of the values of VAS, DN4, SF-12, MOS sleep scale score were found at baseline. Thus, the extent of pain and disability and the quality of life due to low back pain and the physical characteristics of the subjects in the PEMS-treated group and the sham group were similar at baseline.
Importantly, neither group showed side or abnormal effects throughout the trial. Although PEMS is safe, its safety needs to be furtherly evaluated for its use in long-term treatment, because a 2-weeks treatment with a three-month follow-up shows only medium-term results. Additional investigations and clinical trial studies are needed.
Notwithstanding, it is worth noting some limitations that might have influenced the results of our study. VAS has some disadvantages. In particular, it seems to be more difficult to understand than other measurement methods and hence, more susceptible to misinterpretations or “zero-values.” However, this is particularly true in elderly patients and when respondents are given good instructions and the limitations are borne in mind, the VAS is still a valuable instrument to assess pain intensity and changes due to therapy. Likewise, SF-12 summary component scores could be an oversimplification of the information collected by the individual dimensions because they are calculated from the original 8 dimensions. However, summary components can be interpreted together with the profile provided by the 8 dimensions to avoid possible errors in interpreting the results. The use of SF-12 in conjunction with a disability scale has been recommendable because each tool measures unique aspects of disability and health-related quality of life. However, there is some overlap between both instruments, particularly concerning physical-function assessment. Regarding the MOS sleep scale, the lack of a cut-off score undermines its utility as a clinical tool. Nevertheless, the MOS scale may be more useful in studies where the focus is general health status assessment, but information on sleep parameters is of interest. This study also has several strengths: it is a randomized double-blind placebo-controlled treatment study; all the patients, outcome assessors, and the statistician were blinded to the group assignment, the sample size was large enough, and compliance was high.



 ,
, 





{kind=link}
{kind=link}
{kind=link}