
Radiological and Clinical Efficacy of Intra-Arterial 90Y-DOTATATE in Patients with Unresectable, Progressive, Liver Dominant Neuroendocrine Neoplasms

Abstract
:1. Introduction
The Aim of this Study
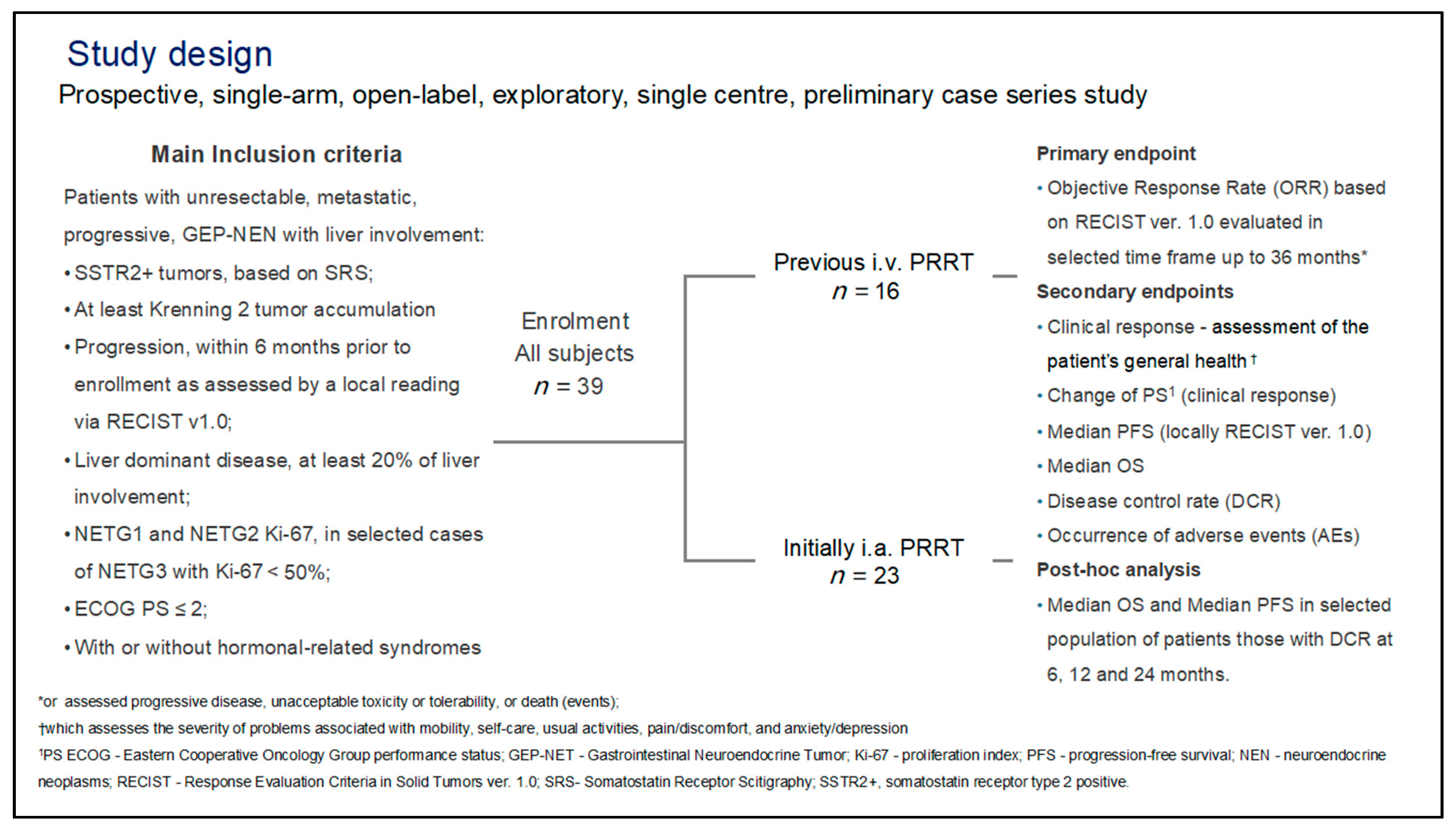
2. Materials and Methods
2.1. General
2.2. Patients
2.3. Therapy—Administration Protocol
2.4. Radiology
2.5. Biodistribution of the Radiotracer
3. Assessment of Effectiveness
3.1. Clinical Response and Performance Status
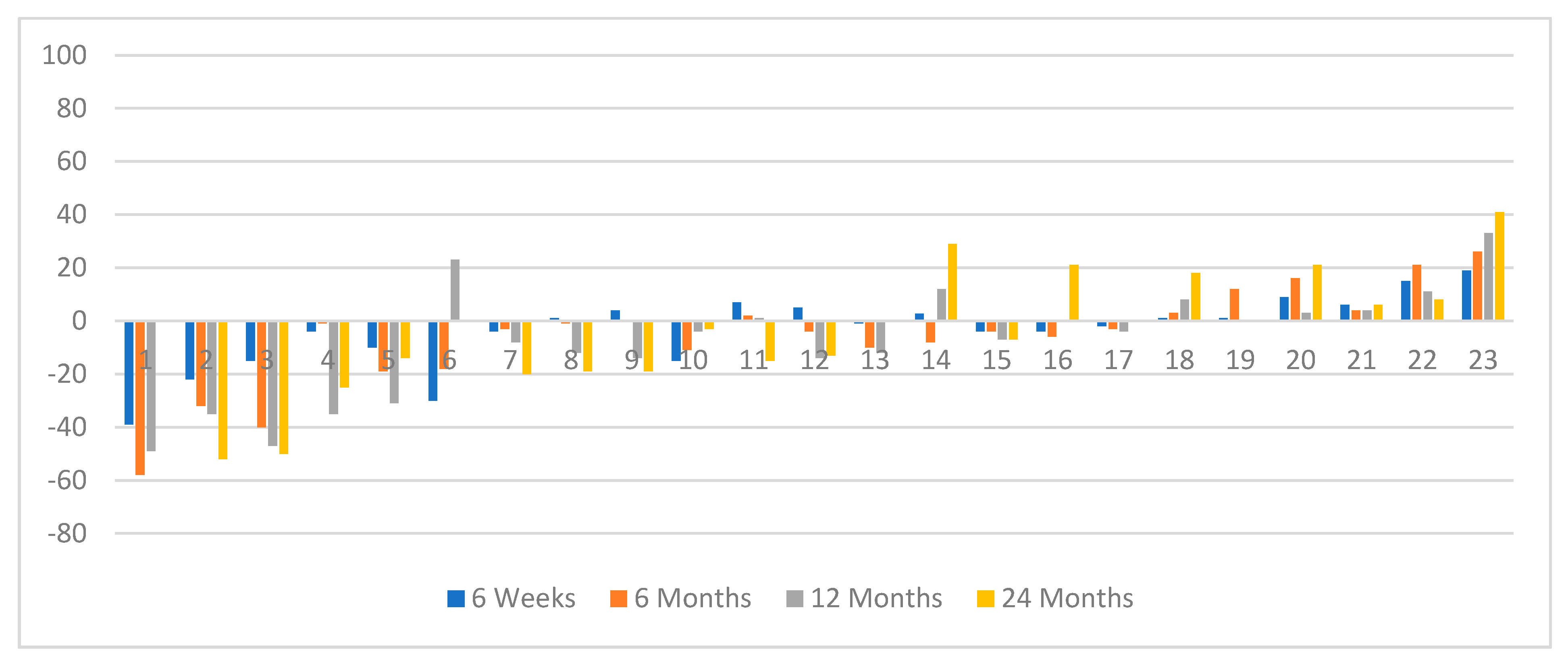
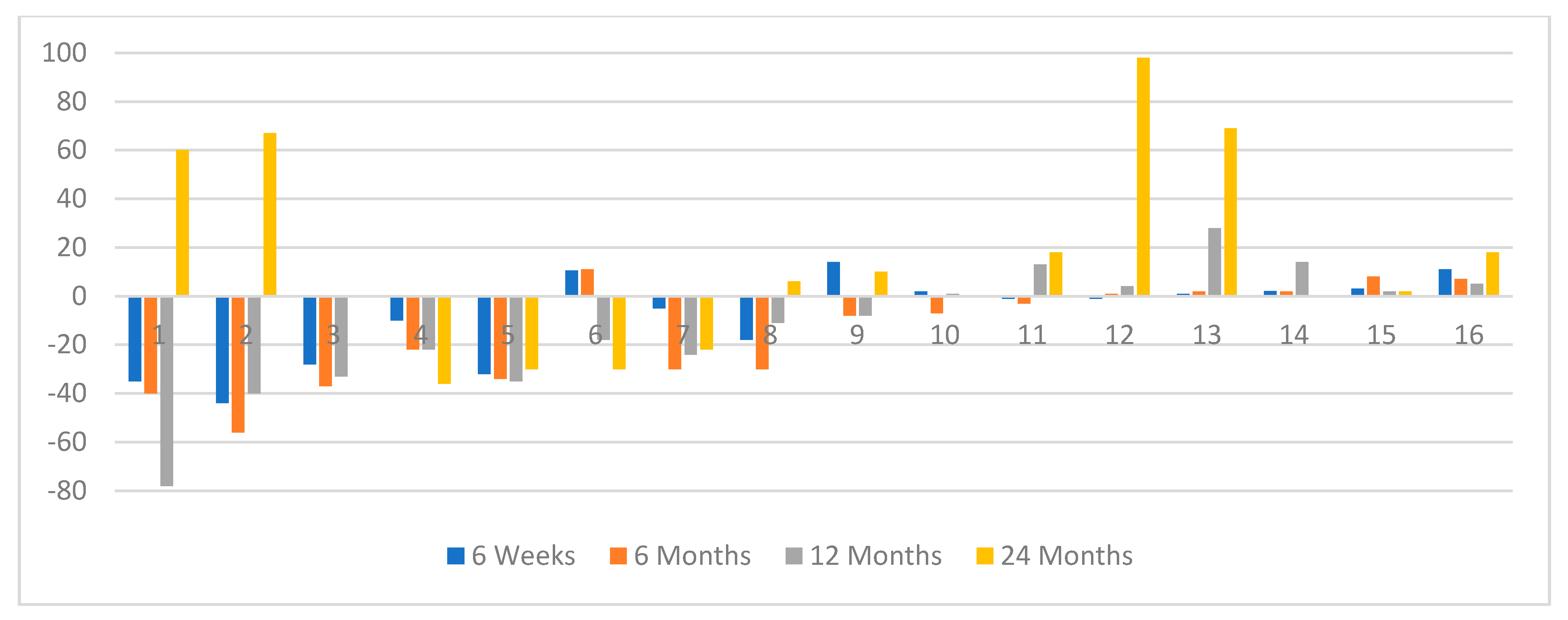
3.2. Image Analysis Radiological Response (RECIST v. 1.0)
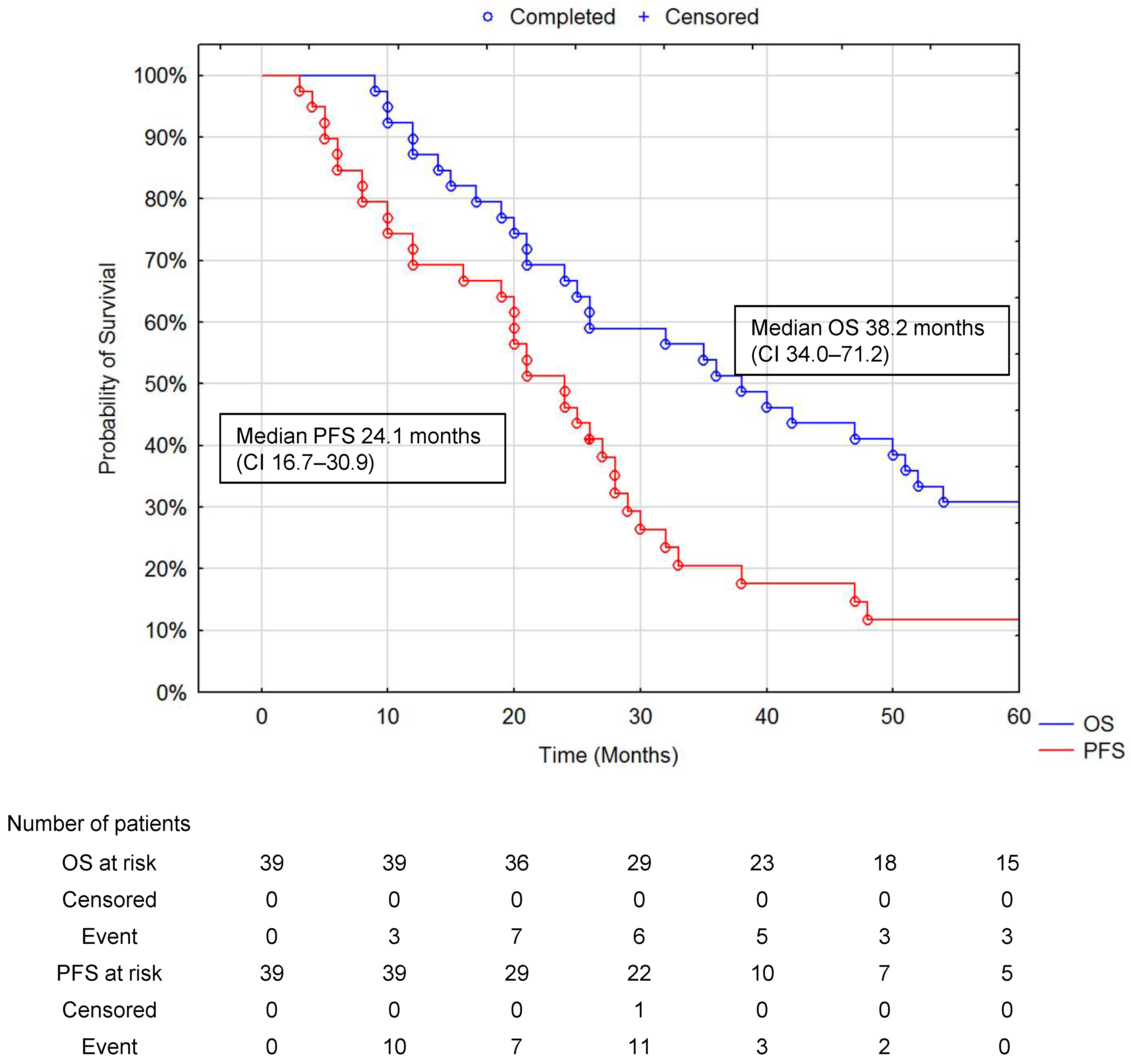
3.3. Statistical Analysis and Patient Survival Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caplin, M.E.; Buscombe, J.R.; Hilson, A.J.; Jones, A.L.; Watkinson, A.F.; Burroughs, A.K. Carcinoid tumour. Lancet 1998, 352, 799–805. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Ramage, J.K.; Ahmed, A.; Ardill, J.; Bax, N.; Breen, D.J.; Caplin, M.E.; Corrie, P.; Davar, J.; Davies, A.H.; Lewington, V.; et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut 2011, 61, 6–32. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.L.; Bang, Y.J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. Everolimus ofr the treatment of advanced non-functional neuroendocrine tumours of the lung or gastrointestinal tract (Radiant-4): A randomized, placebo-controlled phase 3 study. Lancet 2016, 387, 968–977. [Google Scholar] [CrossRef]
- Bodei, L.; Mueller-Brand, J.; Baum, R.P.; Pavel, M.E.; Hörsch, D.; O’Dorisio, M.S.; O’Dorisio, T.M.; Howe, J.R.; Cremonesi, M.; Kwekkeboom, D.J.; et al. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging. 2013, 40, 800–816. [Google Scholar] [CrossRef]
- Kwekkeboom, D.J.; Teunissen, J.J.; Bakker, W.H.; Kooij, P.P.; De Herder, W.W.; Feelders, R.A.; Van Eijck, C.H.; Esser, J.-P.; Kam, B.L.; Krenning, E.P. Radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate in patients with endocrine gastroenteropancreatic tumors. J. Clin. Oncol. 2005, 23, 2754–2762. [Google Scholar] [CrossRef] [Green Version]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M.A. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef]
- Ćwikła, J.B.; Sankowski, A.J.; Seklecka, N.; Buscombe, J.R.; Nasierowska-Guttmejer, A.; Jeziorski, K.G.; Mikołajczak, R.; Pawlak, D.; Walecki, J. Efficacy of radionuclide treatment 90Y-DOTATATE in patients with progressive metastatic gastroenteropancreatic neuroendocrine carcinomas (GEP-NET). A phase II study. Ann. Oncol. 2010, 21, 787–794. [Google Scholar] [CrossRef]
- Bodei, L.; Cremonesi, M.; Grana, C.M.; Fazio, N.; Iodice, S.; Baio, S.M.; Bartolomei, M.; Lombardo, D.; Ferrari, M.E.; Sansovini, M.; et al. Peptide receptor radionuclide therapy with 177Lu-DOTATATE: The IEO phase I-II study. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 2125–2135. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 trail of 177Lu DOTATATE for midgut neuroendocrine tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Hicks, R.J.; Kwekkeboom, D.J.; Krenning, E.; Bodei, L.; Grozinsky-Glasberg, S.; Arnold, R.; Borbath, I.; Cwikla, J.; Toumpanakis, C.; Kaltsas, G.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors. Peptide Receptor Radionuclide Therapy with Radiolabeled Somatostatin Analogues. Neuroendocrinology 2017, 105, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.A.; Bodei, L.; Chan, J.A.; El-Haddad, G.; Fidelman, N.; Kunz, P.L.; Mailman, J.; Menda, Y.; Metz, D.C.; Mittra, E.S.; et al. NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy. J. Nucl. Med. 2020, 61, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.H.; Goldner, W.S.; Halfdanarson, T.R.; Bergsland, E.; Berlin, J.D.; Halperin, D.; Chan, J.; Kulke, M.H.; Benson, A.B.; Blaszkowsky, L.S.; et al. NCCN Clinical Practice Guidelines in Oncology: Neuroendocrine and Adrenal Tumors. J. Natl. Compr. Canc. Netw. 2018, 16, 693–702. [Google Scholar] [CrossRef]
- McStay, M.K.; Maudgil, D.; Williams, M.; Tibballs, J.M.; Watkinson, A.F.; Caplin, M.E.; Buscombe, J.R. Large-Volume Liver Metastases from Neuroendocrine Tumors: Hepatic Intraarterial 90Y-DOTA-Lanreotide as Effective Palliative Therapy. Radiology 2005, 237, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.C.; Schär, J.-C.; Waser, B.; Wenger, S.; Heppeler, A.; Schmitt, J.S.; Mäcke, H.R. Affinity profiles for human somatostatin receptor subtypes SST1-SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. Eur. J. Nucl. Med. Mol. Imaging 2000, 27, 273–282. [Google Scholar] [CrossRef]
- Kwekkeboom, D.J.; Bakker, W.H.; Kam, B.L.; Teunissen, J.J.M.; Kooij, P.P.M.; De Herder, W.W.; Feelders, R.A.; Van Eijck, C.H.J.; De Jong, M.; Srinivasan, A.; et al. Treatment of patients with gastro-entero-pancreatic (GEP) tumours with the novel radiolabelled somatostatin analogue [177Lu-DOTA0,Tyr3]octreotate. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 417–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esser, J.P.; Krenning, E.P.; Teunissen, J.J.M.; Kooij, P.P.M.; Van Gameren, A.L.H.; Bakker, W.H.; Kwekkeboom, D.J. Comparison of [177Lu-DOTA0,Tyr3]octreotate and [177Lu-DOTA0,Tyr3]octreotide: Which peptide is preferable for PRRT? Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Kwekkeboom, D.J.; de Herder, W.W.; Kam, B.L.; van Eijck, C.H.; van Essen, M.; Kooij, P.P.; Feelders, R.A.; van Aken, M.O.; Krenning, E.P. Treatment with the Radiolabeled Somatostatine Analog [177Lu-DOTA0Tyr3]octreotate: Toxicity, Efficacy and Survival. J. Clin. Oncol. 2008, 26, 2124–2130. [Google Scholar] [CrossRef] [Green Version]
- Valkema, R.; Pauwels, S.A.; Kvols, L.K.; Kwekkeboom, D.J.; Jamar, F.; De Jong, M.; Barone, R.; Walrand, S.; Kooij, P.P.M.; Bakker, W.H.; et al. Long term follow-up of renal function after peptide receptor radiation therapy with 90Y-DOTA, Tyr3-Octreotide and 177Lu-DOTA, Tyr3-Octreotate. J. Nucl. Med. 2005, 46, 83S–91S. [Google Scholar]
- Buscombe, J.R. Interventional nuclear medicine in hepatoceullar cancers and other tumours. Nucl. Med. Commun. 2002, 23, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Baum, R.P.; Söldner, J.; Schmücking, M.; Niesen, A. Intravenous and Intra-arterial Peptide Receptor Radionuclide Therapy (PRRT) Using 90Y-DOTA-TYR3-OCTREOTATE (90Y DOTA-TATE) in Patients with Metastatic Neuroendocrine Tumors. In Proceedings of the Annual Congress of the European-Association-of-Nuclear-Medicine, Helsinki, Finland, 5–8 September 2004. [Google Scholar]
- Pettersson, O.; Fross-Baron, K.; Crona, J.; Dundin, A. Tumour Contrast-Enhancement of Monitoring of PRRT 177Lu DOTATATE in Pancreatic Neuroendocrine Tumour Patients. Front. Oncol. 2020, 10, 193. [Google Scholar] [CrossRef] [PubMed]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine and Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef] [PubMed]
- Gehan, E.A.; Tefft, M.C. Will there be resistance to the RECIST (Response Evaluation Criteria in Solid Tumours)? J. Natl. Cancer Inst. 2000, 92, 179–181. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation of solid tumours. Revised RECIST guidelines (RECIST1.1). Eur. J. Oncol. 2009, 45, 228–247. [Google Scholar]
- Waldherr, C.; Pless, M.; Maecke, H.R.; Schumacher, T.; Crazzolara, A.; Nitzsche, E.U.; Haldemann, A.; Mueller-Brand, J. Tumor response and clinical benefit in neuroendocrine tumors after 7.4 GBq 90Y-DOTATOC. J. Nucl. Med. 2002, 43, 610–616. [Google Scholar] [PubMed]
- Baum, R.; Wehrmann, C.; Zachert, C.; Prasad, V.; Wortmann, R. Long-term results of peptide receptor radionuclide therapy (PRRT): 5-year follow-up of 1,150 courses in 360 patients with progressive, somatostatin receptor positive neuroendocrine tumors in one clinical center. J. Nucl. Med. 2007, 48 (Suppl. S2), 37p. [Google Scholar]
- Chinol, M.; Bodei, L.; Cremonesi, M.; Paganelli, G. Receptor-mediated radiotherapy with 90Y-DOTA-DPhe-Tyr-octreotide: The experience of the European Institute of Oncology Group. Semin. Nucl. Med. 2002, 32, 141–147. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Lutetium 177Lu Oxodotreotide for Treating Unresectable or Metastatic Neuroendocrine Tumours 2018. Available online: https://www.nice.org.uk/guidance/TA539 (accessed on 12 April 2021).
- Buscombe, J.R.; Navilkissoor, S. Molecular Radiotherapy. Clin. Med. 2012, 12, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Perren, A.; Couvelard, A.; Scoazec, J.Y.; Costa, F.; Borbath, I.; Delle Fave, G.; Gorbounova, V.; Gross, D.; Grossma, A.; Jense, R.T.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumours: Pathology Diagnosis and Prognostic Stratification. Neuroendocrinology 2017, 105, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Cwikla, J.B.; Mikolajczak, R.; Pawlak, D.; Buscombe, J.R.; Nasierowska-Guttmejer, A.; Bator, A.; Maecke, H.R.; Walecki, J. Initial direct comparison of 99mTc-[HYNIC-TOC] and 99mTc-[HYNIC-TATE] in identifying sites of disease in patients with proven GEP-NET tumors. J. Nucl. Med. 2008, 49, 1060–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, A.E.; Wanders, E.; Kaplan, J.; Rubinstein, R.; Verweij, L.; Van Glabbeke, J.; van Oosterom, M.; Christian, A.; et al. New guidelines to evaluate the response to treatment in solid tumors. J. Nat. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.; Valkema, R.; Jamar, F.; Kvols, L.K.; Kwekkeboom, D.J.; Breeman, W.A.; Bakker, W.H.; Smith, C.; Pauwels, S.; Krenning, E.P. Somatostatin receptor-targeted radionuclide therapy of tumors: Preclinical and clinical findings. Semin. Nucl. Med. 2002, 32, 133–140. [Google Scholar] [CrossRef]
- Goncalves, I.; Burbury, K.; Michael, M.; Iravani, A.; Ravi Kumar, A.S.; Akhurst, T.; Tiong, I.S.; Blombery, P.; Hofman, M.S.; Westerman, D.; et al. Characteristics and Outcomes of Therapy-Related Myeloid Neoplasms After Peptide Receptor radionuclide/chemoradionuclide Therapy (PRRT/PRCRT) for Metastatic Neuroendocrine Neoplasia: A Single-Institution Series. Eur. J. Nucl. Med. 2019, 46, 1902–1910. [Google Scholar] [CrossRef]
- McDermott, E.W.; Guduric, B.; Brennan, M.F. Prognostic variables in patients with gastrointestinal carcinoid tumours. Br. J. Surg. 1994, 81, 1007–1009. [Google Scholar] [CrossRef] [PubMed]
- Vyleta, M.; Coldwell, D. Radioembolization in the Treatment of Neuroendocrine Tumor Metastases to the Liver. Int. J. Hepatol. 2011, 2011, 785315. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, A.; Bester, L.; Salem, R.; Sharma, R.A.; Parks, R.W.; Ruszniewski, P. Role of hepatic intra-arteria therapies in metastatic neuroendocrine tumours (NET): Guidelines from the NET-Liver -Metastases Cnsensus Conference. HPB 2015, 17, 29–37. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All n = 39 | Previous i.v. PRRT n = 16 (%) | Only i.a. n = 23 (%) | |
|---|---|---|---|
| Male to female | 22/17 | 12/4 | 12/11 |
| Age in years (mean, SD) | 56.4 (9.2) | 55.4 (8.2) | 57.5 (9.9) |
| Primary site NEN origin | |||
| Pancreas | 14 (36) | 7 (44) | 7 (30) |
| Small Bowel | 13 (33) | 5 (31) | 8 (35) |
| Large Bowel/Rectum | 4 (10) | 1 (6) | 3 (13) |
| CUP (Cancer of Unknown Primary) | 8 (21) | 3 (19) | 5 (22) |
| Secretor tumors | 19 (49) | 9 (56) | 10 (43) |
| Tumor grade | |||
| NETG1 (Ki-67 ≤ 2%) | 8 (22) | 4 (27) | 4 (17) |
| NEG2 (2 < Ki-67 ≤ 20%) | 28 (73) | 10 (67) | 18 (78) |
| NETG3 (20% < Ki-67 < 50%) | 2 (5) | 1 (6) | 1 (5) |
| Hepatic load (tuVolume/liverVolume) | 0.41% | 45% | 38% |
| ≤25% | 8 (21) | 3 (19) | 5 (22) |
| < 25% x ≤ 50% | 18 (46) | 6 (38) | 12 (52) |
| >50% | 13 (33) | 7 (43) | 6 (26) |
| WHO Performance status (PS) initial | All n = 39 | Previous iv. PRRT n = 16 (%) | Only i.a. n = 23 (%) |
| 0—normal activity | 1 (3) | 1 (5) | |
| 1—restricted activity | 29 (74) | 11 (69) | 18 (78) |
| 2—in bed ≤ 50% of the time | 9 (23) | 5 (31) | 4 (17) |
| Initial basic hematology and kidney creatinine level | All n = 39 | Previous iv. PRRT n = 16 | Only i.a. n = 23 mean value |
| WBC (×109/L) | 6.78 | 7.34 | 6.37 |
| Hb (g/dL) | 12.8 | 12.0 | 13.4 |
| Platelet (×106/L) | 288 | 297 | 282 |
| Creatinine level mg/dL | 0.97 | 1.24 | 0.78 |
| CgA x ULN; mean (95% CI) | 34.5 (19.8–49.2) | 48.8 (11.6–81.9) | 27.6 (13.9–41.3) |
| Therapy Approach before i.a. PRRT | All n = 39 (%) | Previous iv. PRRT n = 16 (%) | Only i.a. PRRT n = 23 (%) |
|---|---|---|---|
| Analogs SST (long-acting) | 32 (82) | 13 (81) | 19 (83) |
| Chemotherapy any type | 12 (31) | 9 (56) | 3 (13) |
| Previous i.v. PRRT | 16 (41) | 16 (100) | |
| Local Liver therapy TA, surgery | 9 (23) | 4 (25) | 5 (22) |
| Parameter | All Subjects n = 39 | Previous i.v. PRRT n = 16 (%) | Native i.a. n = 23 (%) |
|---|---|---|---|
| Mean activity (GBq of 90Y DOTATATE) per session | 1.15 | 1.12 | 1.16 |
| Mean Cumulative activity (GBq of 90Y) per therapy (range) | 3.13 (1.4–4.1) | 2.8 (2.0–4.1) | 3.4 (1.4–4.1) |
| Mean (range) time between each therapy sessions (weeks) | 9.2 (6–12) | 10 (8–12) | 8.4 (6–10) |
| Response | RECIST 6W, n (%) | Clinical Response 6 W | RECIST; 6 M n (%) | Clinical Response 6 M | RECIST 12 M, n (%) | Clinical Response 12 M | RECIST 24 M n (%) | Clinical Response 24 M | RECIST 36 M n (%) | Clinical Response 36 M |
|---|---|---|---|---|---|---|---|---|---|---|
| All subjects n = 39 | ||||||||||
| PR | 5 (13) | 29 (74) | 9 (24) | 27(70) | 9 (24) | 24 (63) | 5 (16) | 15 (46) | 2 (13) | 7 (39) |
| SD | 34 (87) | 8 (21) | 27 (71) | 6 (15) | 25 (68) | 4 (11) | 18 (58) | 6 (18) | 6 (40) | 4 (22) |
| DP | 2 (5) | 2 (5) | 6 (15) | 3 (8) | 10 (26) | 8 (26) | 12 (36) | 7 (47) | 7 (39) | |
| Previous i.v. PRRT n = 16 | ||||||||||
| PR | 3 (19) | 12 (75) | 6 (38) | 10 (63) | 4 (25) | 7 (44) | 3 (23) | 3 (23) | 2 (40) | 2 (40) |
| SD | 13 (81) | 3 (19) | 10 (62) | 4 (25) | 11 (69) | 2 (12) | 6 (46) | 1 (8) | ||
| DP | 1 (6) | 2 (12) | 1 (6) | 7 (44) | 4 (31) | 9 (69) | 3 (60) | 3 (60) | ||
| Initially i.a. PRRT n = 23 | ||||||||||
| PR | 2 (9) | 17 (74) | 3 (14) | 17 (74) | 5 (23) | 17 (77) | 2 (11) | 12 (23) | 5 (38) | |
| SD | 21 (91) | 5 (22) | 17 (77) | 2 (9) | 14 (67) | 2 (9) | 12 (67) | 5 (8) | 6 (60) | 4 (31) |
| 1 (4) | 2 (9) | 4 (17) | 2 (10) | 3 (14) | 4 (22) | 3 (69) | 4 (40) | 4 (31) | ||
| Initial Week 0 n = 38 | Week 6 after PRRT, n = 38 | 6 Months n = 35 | 12 Months n = 29 | 24 Months n = 20 | |
|---|---|---|---|---|---|
| WBC | |||||
| Grade 1 | 5 (13) | 12 (32) | 9 (26) | 7 (24) | 1 (6) |
| Grade 2 | 1 (3) | 1 (3) | |||
| Grade 3 | 1 (6) | ||||
| Hb | |||||
| Grade 1 | 10 (26) | 15 (39) | 6 (21) | 6 (21) | 3 (15) |
| Grade 2 | 2 (5) | 2 (5) | 2 (7) | 2 (7) | 1 (5) |
| Grade 3 | 1 (3) | 1 (3) | 1 (3) | ||
| Creatinine | |||||
| Grade 1 | 2 (5) | 2 (6) | 4 (14) | ||
| Grade 2 | 2 (5) | 3 (8) | 2 (6) | 2 (7) | |
| Grade 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolasińska-Ćwikła, A.; Nowicki, M.L.; Sankowski, A.J.; Pałucki, J.M.; Buscombe, J.R.; Glinka, L.; Ćwikła, J.B. Radiological and Clinical Efficacy of Intra-Arterial 90Y-DOTATATE in Patients with Unresectable, Progressive, Liver Dominant Neuroendocrine Neoplasms. J. Clin. Med. 2021, 10, 1794. https://doi.org/10.3390/jcm10081794
Kolasińska-Ćwikła A, Nowicki ML, Sankowski AJ, Pałucki JM, Buscombe JR, Glinka L, Ćwikła JB. Radiological and Clinical Efficacy of Intra-Arterial 90Y-DOTATATE in Patients with Unresectable, Progressive, Liver Dominant Neuroendocrine Neoplasms. Journal of Clinical Medicine. 2021; 10(8):1794. https://doi.org/10.3390/jcm10081794
Chicago/Turabian StyleKolasińska-Ćwikła, Agnieszka, Mirosław L. Nowicki, Artur J. Sankowski, Jakub M. Pałucki, John R. Buscombe, Lidia Glinka, and Jarosław B. Ćwikła. 2021. "Radiological and Clinical Efficacy of Intra-Arterial 90Y-DOTATATE in Patients with Unresectable, Progressive, Liver Dominant Neuroendocrine Neoplasms" Journal of Clinical Medicine 10, no. 8: 1794. https://doi.org/10.3390/jcm10081794
APA StyleKolasińska-Ćwikła, A., Nowicki, M. L., Sankowski, A. J., Pałucki, J. M., Buscombe, J. R., Glinka, L., & Ćwikła, J. B. (2021). Radiological and Clinical Efficacy of Intra-Arterial 90Y-DOTATATE in Patients with Unresectable, Progressive, Liver Dominant Neuroendocrine Neoplasms. Journal of Clinical Medicine, 10(8), 1794. https://doi.org/10.3390/jcm10081794