
Home-Measured Blood Pressure Is Associated with Handgrip Strength in Patients with Type 2 Diabetes: The KAMOGAWA-HBP Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
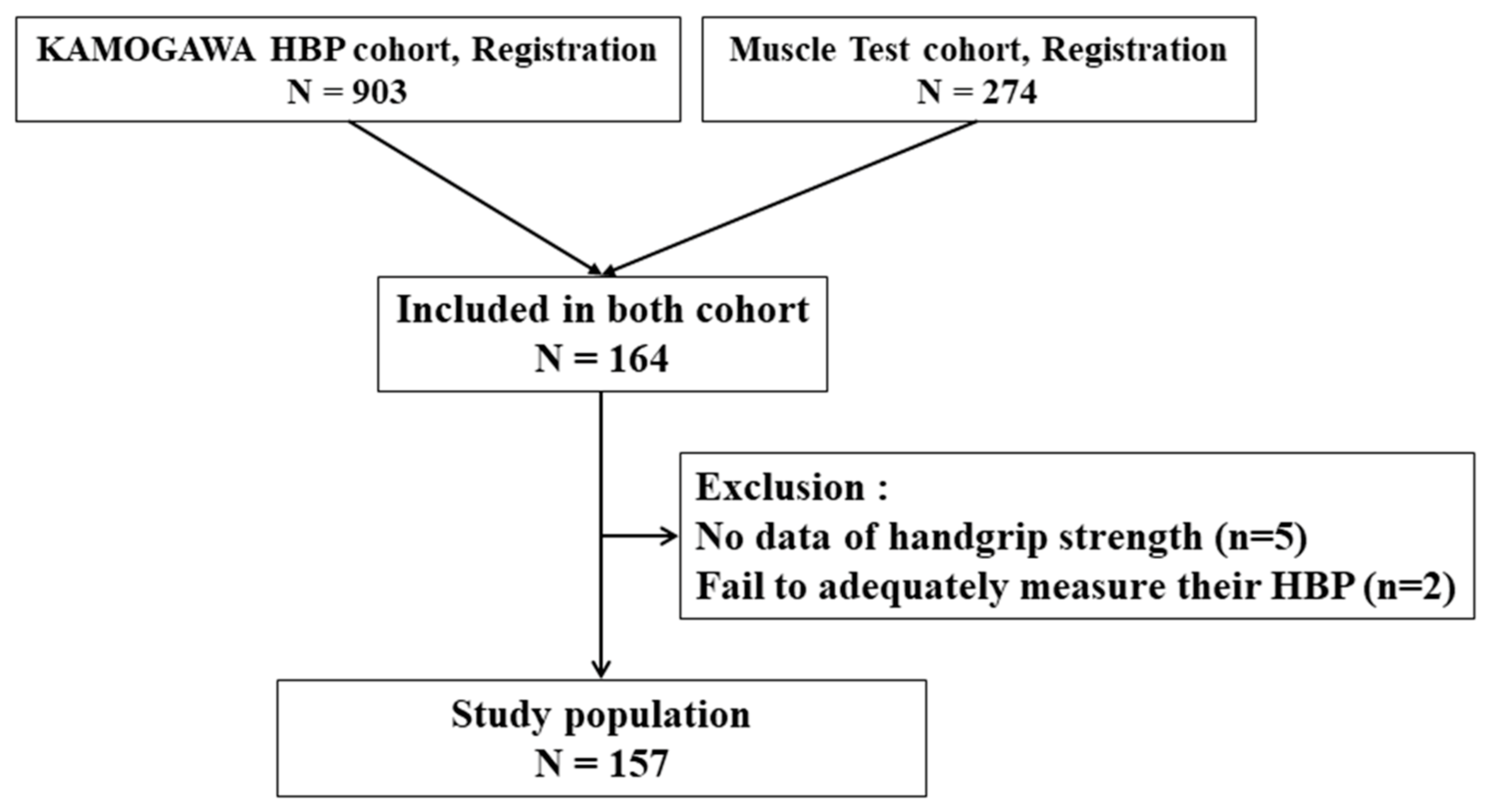
2.1. Study Design
2.2. Patients
2.3. BP Measurements
2.4. Measurements of Grip Strength
2.5. Data Collection
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Principal Findings
4.2. Interpretations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Ismail-Beigi, F.; Craven, T.; Banerji, M.A.; Basile, J.; Calles, J.; Cohen, R.M.; Cuddihy, R.; Cushman, W.C.; Genuth, S.; Grimm, R.; et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: An analysis of the accord randomised trial. Lancet 2010, 376, 419–430. [Google Scholar] [CrossRef] [Green Version]
- Ushigome, E.; Oyabu, C.; Tanaka, T.; Hasegawa, G.; Ohnishi, M.; Tsunoda, S.; Ushigome, H.; Yokota, I.; Nakamura, N.; Oda, Y.; et al. Impact of masked hypertension on diabetic nephropathy in patients with type II diabetes: A KAMOGAWA-HBP study. J. Am. Soc. Hypertens. 2018, 12, 364–371.e1. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, S.T.; Poulsen, P.L.; Hansen, K.W.; Ebbehøj, E.; Bek, T.; Mogensen, C.E. Pulse pressure and diurnal blood pressure variation: Association with micro- and macrovascular complications in type 2 diabetes. Am. J. Hypertens. 2002, 15, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Martone, A.M.; Bianchi, L.; Abete, P.; Bellelli, G.; Bo, M.; Cherubini, A.; Corica, F.; Di Bari, M.; Maggio, M.; Manca, G.M.; et al. The incidence of sarcopenia among hospitalized older patients: Results from the Glisten study. J. Cachexia Sarcopenia Muscle 2017, 8, 907–914. [Google Scholar] [CrossRef]
- Timpka, S.; Petersson, I.F.; Zhou, C.; Englund, M. Muscle strength in adolescent men and risk of cardiovascular disease events and mortality in middle age: A prospective cohort study. BMC Med. 2014, 12, 62. [Google Scholar] [CrossRef] [Green Version]
- Hess, N.C.; Carlson, D.J.; Inder, J.D.; Jesulola, E.; McFarlane, J.R.; Smart, N.A. Clinically meaningful blood pressure reductions with low intensity isometric handgrip exercise. A randomized trial. Physiol. Res. 2016, 65, 461–468. [Google Scholar] [CrossRef]
- Carlson, D.J.; Inder, J.; Palanisamy, S.K.; McFarlane, J.R.; Dieberg, G.; Smart, N.A. The efficacy of isometric resistance training utilizing handgrip exercise for blood pressure management: A randomized trial. Medicine 2016, 95, e5791. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.E.; Dennison, E.M.; Martin, H.J.; Phillips, D.I.; Cooper, C.; Byrne, C.D. Grip strength and the metabolic syndrome: Findings from the Hertfordshire cohort study. QJM 2007, 100, 707–713. [Google Scholar] [CrossRef] [Green Version]
- Ji, C.; Zheng, L.; Zhang, R.; Wu, Q.; Zhao, Y. Handgrip strength is positively related to blood pressure and hypertension risk: Results from the national health and nutrition examination survey. Lipids Health Dis. 2018, 17, 86. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, Y.; Kaji, A.; Sakai, R.; Hamaguchi, M.; Okada, H.; Ushigome, E.; Asano, M.; Yamazaki, M.; Fukui, M. Sarcopenia is associated with blood pressure variability in older patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort study. Geriatr. Gerontol. Int. 2018, 18, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003, 26, 5–20. [CrossRef] [Green Version]
- Imai, Y.; Otsuka, K.; Kawano, Y.; Shimada, K.; Hayashi, H.; Tochikubo, O.; Miyakawa, M.; Fukiyama, K. Japanese society of hypertension (JSH) guidelines for self-monitoring of blood pressure at home. Hypertens. Res. 2003, 26, 771–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chilima, D.M.; Ismail, S.J. Nutrition and handgrip strength of older adults in rural Malawi. Public Health Nutr. 2001, 4, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Kallman, D.A.; Plato, C.C.; Tobin, J.D. The role of muscle loss in the age-related decline of grip strength: Cross-sectional and longitudinal perspectives. J. Gerontol. 1990, 45, 82–88. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Petr, M.; Kohlikova, E.; Holmerova, I. Relation between cigarette smoking and sarcopenia: Meta-analysis. Physiol. Res. 2015, 64, 419–426. [Google Scholar] [CrossRef]
- Srikanthan, P.; Hevener, A.L.; Karlamangla, A.S. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: Findings from the national health and nutrition examination survey III. PLoS ONE 2010, 5, e10805. [Google Scholar] [CrossRef] [PubMed]
- Kohara, K. Sarcopenic obesity in aging population: Current status and future directions for research. Endocrine 2014, 45, 15–25. [Google Scholar] [CrossRef]
- Chamoit-Clerc, P.; Renaud, J.F.; Safar, M.E. Pulse pressure, aortic reactivity, and endothelium dysfunction in old hypertensive rats. Hypertension 2001, 37, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Higashi, Y.; Sasaki, S.; Kurisu, S.; Yoshimizu, A.; Sasaki, N.; Matsuura, H.; Kajiyama, G.; Oshima, T. Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects: Role of endothelium-derived nitric oxide. Circulation 1999, 100, 1194–1202. [Google Scholar] [CrossRef] [Green Version]
- Samengo, G.; Avik, A.; Fedor, B.; Whittaker, D.; Myung, K.H.; Wehling-Henricks, M.; Tidball, J.G. Age-related loss of nitric oxide synthase in skeletal muscle causes reductions in calpain S-nitrosylation that increase myofibril degradation and sarcopenia. Aging Cell 2012, 11, 1036–1045. [Google Scholar] [CrossRef] [Green Version]
- Yamanashi, H.; Kulkarni, B.; Edwards, T.; Kinra, S.; Koyamatsu, J.; Nagayoshi, M.; Shimizu, Y.; Maeda, T.; Cox, S.E. Association between atherosclerosis and handgrip strength in non-hypertensive populations in India and Japan. Geriatr. Gerontol. Int. 2018, 18, 1071–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baber, R.J.; Panay, N.; Fenton, A.; Baber, R.J.; Panay, N.; Fenton, A.; Pérez López, F.R.; Storch, E.; Villaseca, P.; Llaneza, P. 2016 IMS recommendations on women’s midlife health and menopause hormone therapy. Climacteric 2016, 19, 109–150. [Google Scholar] [CrossRef]
- Valenti, G. Adrenopause: An imbalance between dehydroepiandrosterone (DHEA) and cortisol secretion. J. Endocrinol. Invest. 2002, 25, 29–35. [Google Scholar] [PubMed]
- Greising, S.M.; Baltgalvis, K.A.; Lowe, D.A.; Warren, G.L. Hormone therapy and skeletal muscle strength: A meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.E.; McArdle, A.; Griffiths, R.D. The role of hormones, cytokines and heat shock proteins during age-related muscle loss. Clin. Nutr. 2007, 26, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.C.; Laakkonen, E.K.; Lowe, D.A. Aging of the musculoskeletal system: How the loss of estrogen impacts muscle strength. Bone 2019, 123, 137–144. [Google Scholar] [CrossRef]
- Taekema, D.G.; Maier, A.B.; Westendorp, R.G.J.; de Craen, A.J.M. Higher blood pressure is associated with higher handgrip strength in the oldest old. Am. J. Hypertens. 2011, 24, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, M.A.; John, A.; Weir, M.R.; Smith, S.R.; Hunsicker, L.; Kasiske, B.L.; Kusek, J.W.; Bostom, A.; Ivanova, A.; Levey, A.S.; et al. Cardiovascular disease, and death in the folic acid for vascular outcome reduction in transplantation trial. J. Am. Soc. Nephrol. 2014, 25, 1554–1562. [Google Scholar] [CrossRef] [Green Version]
- Franklin, S.S.; Larson, M.G.; Khan, S.A.; Wong, N.D.; Leip, E.P.; Kannel, W.B.; Levy, D. Does the relation of blood pressure to coronary heart disease risk change with aging? The framingham heart study. Circulation 2001, 103, 1245–1249. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All | Men | Women | p | |
|---|---|---|---|---|
| N | 157 | 94 | 63 | - |
| Age (year) | 70.5 (8.5) | 69.8 (8.9) | 71.5 (7.8) | 0.201 |
| BMI (kg/m2) | 23.7 (3.8) | 24.0 (3.1) | 23.2 (4.4) | 0.263 |
| Handgrip strength (kg) | 27.0 (9.2) | 32.4 (7.4) | 18.8 (4.1) | <0.0001 |
| Smoking (never/past or current) | 52/105 | 14/80 | 38/25 | <0.0001 |
| Regular exercise (yes/no) | 102/53 | 47/45 | 55/8 | <0.0001 |
| Antihypertensive drug use (yes/no) | 88/69 | 59/35 | 29/34 | 0.539 |
| HbA1c (%) | 7.1 (0.8) | 7.1 (0.8) | 7.1 (0.8) | 0.572 |
| Average of morning SBP (mmHg) | 133.6 (19.9) | 133.4 (18.2) | 133.8 (22.4) | 0.914 |
| Average of morning DBP (mmHg) | 75.4 (11.0) | 76.8 (10.9) | 73.2 (10.8) | 0.043 |
| Average of morning PP (mmHg) | 58.2 (15.0) | 56.6 (13.6) | 60.6 (16.7) | 0.107 |
| Average of evening SBP (mmHg) | 129.2 (17.9) | 128.1 (16.5) | 130.8 (19.8) | 0.342 |
| Average of evening DBP (mmHg) | 70.3 (9.8) | 70.7 (10.1) | 69.7 (9.4) | 0.548 |
| Average of evening PP (mmHg) | 58.9 (14.0) | 57.4 (12.9) | 61.1 (15.4) | 0.104 |
| Men | Women | |||
|---|---|---|---|---|
| Unadjusted | Adjusted † | Unadjusted | Adjusted † | |
| Morning systolic blood pressure | 0.04 (−0.05, 0.12) | 0.09 (−0.01, 0.19) | −0.08 (−0.12, −0.03) | −0.09 (−0.15, −0.04) |
| Morning diastolic blood pressure | 0.21 (0.08, 0.34) | 0.20 (0.03, 0.37) | −0.01 (−0.11, 0.09) | −0.04 (−0.15, 0.08) |
| Morning pulse pressure | −0.07 (−0.18, 0.04) | 0.02 (−0.10, 0.19) | −0.13 (−0.19, −0.08) | −0.14 (−0.21, −0.08) |
| Evening systolic blood pressure | 0.02 (−0.08, 0.11) | 0.04 (−0.06, 0.14) | −0.07 (−0.12, −0.02) | −0.06 (−0.12, −0.002) |
| Evening diastolic blood pressure | 0.19 (0.04, 0.34) | 0.10 (−0.08, 0.28) | 0.04 (−0.07, 0.16) | 0.04 (−0.09, 0.17) |
| Evening pulse pressure | −0.09 (−0.21, 0.03) | 0.01 (−0.13, 0.15) | −0.13 (−0.19, −0.07) | −0.12 (−0.19, −0.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, T.; Ushigome, E.; Hashimoto, Y.; Nakanishi, N.; Hamaguchi, M.; Asano, M.; Yamazaki, M.; Fukui, M. Home-Measured Blood Pressure Is Associated with Handgrip Strength in Patients with Type 2 Diabetes: The KAMOGAWA-HBP Study. J. Clin. Med. 2021, 10, 1913. https://doi.org/10.3390/jcm10091913
Kimura T, Ushigome E, Hashimoto Y, Nakanishi N, Hamaguchi M, Asano M, Yamazaki M, Fukui M. Home-Measured Blood Pressure Is Associated with Handgrip Strength in Patients with Type 2 Diabetes: The KAMOGAWA-HBP Study. Journal of Clinical Medicine. 2021; 10(9):1913. https://doi.org/10.3390/jcm10091913
Chicago/Turabian StyleKimura, Tomonori, Emi Ushigome, Yoshitaka Hashimoto, Naoko Nakanishi, Masahide Hamaguchi, Mai Asano, Masahiro Yamazaki, and Michiaki Fukui. 2021. "Home-Measured Blood Pressure Is Associated with Handgrip Strength in Patients with Type 2 Diabetes: The KAMOGAWA-HBP Study" Journal of Clinical Medicine 10, no. 9: 1913. https://doi.org/10.3390/jcm10091913
APA StyleKimura, T., Ushigome, E., Hashimoto, Y., Nakanishi, N., Hamaguchi, M., Asano, M., Yamazaki, M., & Fukui, M. (2021). Home-Measured Blood Pressure Is Associated with Handgrip Strength in Patients with Type 2 Diabetes: The KAMOGAWA-HBP Study. Journal of Clinical Medicine, 10(9), 1913. https://doi.org/10.3390/jcm10091913