
Neutrophil-to-Lymphocyte Ratio, a Novel Inflammatory Marker, as a Predictor of Bipolar Type in Depressed Patients: A Quest for Biological Markers

 ,
,  , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hirschfeld, R. Differential diagnosis of bipolar disorder and major depressive disorder. J. Affect. Disord. 2014, 169, S12–S16. [Google Scholar] [CrossRef] [Green Version]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Merikangas, K.; Akiskal, H.; Angst, J.; Greenberg, P.; Hirschfeld, R.; Petukhova, M.; Kessler, R. Lifetime And 12-Month Prev-alence Of Bipolar Spectrum Disorder in The National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2007, 64, 543. [Google Scholar] [CrossRef]
- Grande, I.; Berk, M.; Birmaher, B.; Vieta, E. Bipolar Disorder. Lancet 2016, 387, 1561–1572. [Google Scholar] [CrossRef]
- Alonso, J.; Petukhova, M.; Vilagut, G.; Chatterji, S.; Heeringa, S.; Üstün, T.B.; Alhamzawi, A.O.; Viana, M.C.; Angermeyer, M.; Bromet, E.; et al. Days out of role due to common physical and mental conditions: Results from the WHO World Mental Health surveys. Mol. Psychiatry 2010, 16, 1234–1246. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Berk, M.; Schulze, T.G.; Carvalho, A.F.; Suppes, T.; Calabrese, J.R.; Gao, K.; Miskowiak, K.W.; Grande, I. Bipolar disorders. Nat. Rev. Dis. Prim. 2018, 4, 18008. [Google Scholar] [CrossRef]
- Dean, J.; Keshavan, M. The neurobiology of depression: An integrated view. Asian J. Psychiatry 2017, 27, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Kapczinski, F.; Andreazza, A.; Dean, O.; Giorlando, F.; Maes, M.; Yücel, M.; Gama, C.; Dodd, S.; Dean, B.; et al. Pathways underlying neuroprogression in bipolar disorder: Focus on inflammation, oxidative stress and neurotrophic factors. Neurosci. Biobehav. Rev. 2011, 35, 804–817. [Google Scholar] [CrossRef]
- Rosenblat, J.D.; McIntyre, R.S. Bipolar Disorder and Immune Dysfunction: Epidemiological Findings, Proposed Pathophysiology and Clinical Implications. Brain Sci. 2017, 7, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivković, M.; Pantović-Stefanović, M.; Dunjić-Kostić, B.; Jurišić, V.; Lačković, M.; Totić-Poznanović, S.; Jovanović, A.; Damjanović, A. Neutrophil-To-Lymphocyte Ratio Predicting Suicide Risk in Euthymic Patients with Bipolar Disorder: Moderatory Effect of Family History. Compr. Psychiatry 2016, 66, 87–95. [Google Scholar] [CrossRef]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef]
- Horstman, L.L.; Jy, W.; Ahn, Y.S.; Zivadinov, R.; Maghzi, A.H.; Etemadifar, M.; Alexander, J.S.; Minagar, A. Role of platelets in neuroinflammation: A wide-angle perspective. J. Neuroinflammation 2010, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Dietrich-Muszalska, A.; Wachowicz, B. Platelet haemostatic function in psychiatric disorders: Effects of antidepressants and antipsychotic drugs. World J. Biol. Psychiatry 2016, 18, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Baufeld, C.; O’Loughlin, E.; Calcagno, N.; Madore, C.; Butovsky, O. Differential contribution of microglia and monocytes in neurodegenerative diseases. J. Neural Transm. 2017, 125, 809–826. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, K.; Fornaguera-Trías, J.; Sheridan, J.F. Stress-Induced Microglia Activation and Monocyte Trafficking to the Brain Underlie the Development of Anxiety and Depression. In Inflammation-Associated Depression: Evidence, Mechanisms and Implications; Dantzer, R., Capuron, L., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 155–172. ISBN 978-3-319-51151-1. [Google Scholar]
- Minogue, A.M. Role of infiltrating monocytes/macrophages in acute and chronic neuroinflammation: Effects on cognition, learning and affective behaviour. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 79, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Pamer, E.G. Monocyte recruitment during infection and inflammation. Nat. Rev. Immunol. 2011, 11, 762–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, Y.; Yu, Z.; Sakai, M.; Tomita, H. Linking Activation of Microglia and Peripheral Monocytic Cells To The Patho-physiology Of Psychiatric Disorders. Front Cell Neurosci. 2016, 10, 144. [Google Scholar] [CrossRef]
- Wang, J.-R.; Chen, Z.; Yang, K.; Yang, H.-J.; Tao, W.-Y.; Li, Y.-P.; Jiang, Z.-J.; Bai, C.-F.; Yin, Y.-C.; Duan, J.-M.; et al. Association between neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and diabetic retinopathy among diabetic patients without a related family history. Diabetol. Metab. Syndr. 2020, 12, 55. [Google Scholar] [CrossRef]
- Imtiaz, F.; Shafique, K.; Mirza, S.; Ayoob, Z.; Vart, P.; Rao, S. Neutrophil Lymphocyte Ratio As A Measure Of Systemic In-flammation In Prevalent Chronic Diseases In Asian Population. Int. Arch. Med. 2012, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Zhou, P.; Liu, Y.; Wei, H.; Yang, X.; Chen, T.; Xiao, J. Platelet-to-lymphocyte ratio in advanced Cancer: Review and meta-analysis. Clin. Chim. Acta 2018, 483, 48–56. [Google Scholar] [CrossRef]
- Jung, J.; Lee, E.; Suh, C.; Kim, H. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio are associated with disease activity in Polymyalgia Rheumatica. J. Clin. Lab. Anal. 2019, 33, e23000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Z.; Cai, T.; Fan, L.; Lou, K.; Hua, X.; Huang, Z.; Gao, G. Clinical value of immune-inflammatory parameters to assess the severity of coronavirus disease 2019. Int. J. Infect. Dis. 2020, 95, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Zulfic, Z.; Weickert, C.; Weickert, T.; Liu, D.; Myles, N.; Galletly, C. Neutrophil–Lymphocyte Ratio—A Simple, Accessible Measure of Inflammation, Morbidity and Prognosis in Psychiatric Disorders? Australas. Psychiatry 2020, 28, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.-Q.; Huang, L.-D.; Dai, R.-J.; Chen, N.-D.; Hu, W.-J.; Shan, Y.-F. Neutrophil-lymphocyte ratio: A controversial marker in predicting Crohn’s disease severity. Int. J. Clin. Exp. Pathol. 2015, 8, 14779–14785. [Google Scholar]
- Islas-Vazquez, L.; Aguilar-Cazares, D.; Galicia-Velasco, M.; Rumbo-Nava, U.; Meneses-Flores, M.; Luna-Rivero, C.; Lopez-Gonzalez, J.S. IL-6, NLR, and SII Markers and Their Relation with Alterations in CD8+ T-Lymphocyte Subpopulations in Patients Treated for Lung Adenocarcinoma. Biology 2020, 9, 376. [Google Scholar] [CrossRef] [PubMed]
- Kulaksizoglu, B.; Kulaksizoglu, S. Relationship Between Neutrophil/Lymphocyte Ratio with Oxidative Stress and Psycho-pathology in Patients with Schizophrenia. Neuropsychiatr. Dis. Treat. 2016, 12, 1999–2005. [Google Scholar] [CrossRef] [Green Version]
- Jacomb, I.; Stanton, C.; Vasudevan, R.; Powell, H.; O’Donnell, M.; Lenroot, R.; Bruggemann, J.; Balzan, R.; Galletly, C.; Liu, D.; et al. C-Reactive Protein: Higher During Acute Psychotic Episodes and Related to Cortical Thickness in Schizophrenia and Healthy Controls. Front. Immunol. 2018, 9, 2230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mert, D.G.; Terzi, H. Mean platelet volume in bipolar disorder: The search for an ideal biomarker. Neuropsychiatr. Dis. Treat. 2016, 12, 2057–2062. [Google Scholar] [CrossRef] [Green Version]
- Özdin, S.; Sarisoy, G.; Böke, Ö. A Comparison of The Neutrophil-Lymphocyte, Platelet-Lymphocyte and Monocyte-Lymphocyte Ratios in Schizophrenia And Bipolar Disorder Patients—A Retrospective File Review. Nord. J. Psychiatry 2017, 71, 509–512. [Google Scholar] [CrossRef]
- Özdin, S.; Usta, M.B. A comparison of inflammatory markers in manic and euthymic states of bipolar disorder. Nord. J. Psychiatry 2021, 75, 124–129. [Google Scholar] [CrossRef]
- Mayda, H.; Ahsen, A.; Bagcioglu, E.; Ozturk, A.; Bahceci, B.; Soyucok, E.; Baspinar, E.; Ulu, M. Effect of Increased Neutro-phil-To-Lymphocyte Ratio (NLR) And Decreased Mean Platelet Volume (MPV) Values on Inflammation in Acute Mania. Noro Psikiyatr. Ars. 2016, 53, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Kalelioglu, T.; Akkus, M.; Karamustafalioglu, N.; Genc, A.; Genc, E.S.; Cansiz, A.; Emul, M. Neutrophil-lymphocyte and platelet-lymphocyte ratios as inflammation markers for bipolar disorder. Psychiatry Res. 2015, 228, 925–927. [Google Scholar] [CrossRef] [PubMed]
- Inanli, I.; Aydin, M.; Çaliskan, A.M.; Eren, I. Neutrophil/lymphocyte ratio, monocyte/lymphocyte ratio, and mean platelet volume as systemic inflammatory markers in different states of bipolar disorder. Nord. J. Psychiatry 2019, 73, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, M.G.; Cicek, I.E.; Inanli, I.; Caliskan, A.M.; Ercan, S.K.; Eren, I. Neutrophil/lymphocyte and platelet/lymphocyte ratios in all mood states of bipolar disorder. Psychiatry Clin. Psychopharmacol. 2017, 27, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Mazza, M.G.; Lucchi, S.; Tringali, A.G.M.; Rossetti, A.; Botti, E.R.; Clerici, M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 84, 229–236. [Google Scholar] [CrossRef]
- Atli, A.; Demir, S.; Bulut, M.; Okan İbiloğlu, A.; Güneş, M.; Kaya, M.; Demirpençe, Ö.; Sır, A. Neutrophil-Lymphocyte Ratio In Patients With Major Depressive Disorder Undergoing No Pharmacological Therapy. Neuropsychiatr. Dis. Treat. 2015, 11, 2253–2258. [Google Scholar] [CrossRef] [Green Version]
- Kayhan, F.; Gündüz, Ş.; Ersoy, S.A.; Kandeğer, A.; Annagür, B.B. Relationships of neutrophil–lymphocyte and platelet–lymphocyte ratios with the severity of major depression. Psychiatry Res. 2017, 247, 332–335. [Google Scholar] [CrossRef]
- Sunbul, E.A.; Sunbul, M.; Yanartas, O.; Cengiz, F.; Bozbay, M.; Sari, I.; Güleç, H. Increased Neutrophil/Lymphocyte Ratio in Patients with Depression is Correlated with the Severity of Depression and Cardiovascular Risk Factors. Psychiatry Investig. 2016, 13, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Arabska, J.; Łucka, A.; Magierski, R.; Sobów, T.; Wysokiński, A. Neutrophil-lymphocyte ratio is increased in elderly patients with first episode depression, but not in recurrent depression. Psychiatry Res. 2018, 263, 35–40. [Google Scholar] [CrossRef]
- Erdoğan, M.; Erdöl, M.; Öztürk, S.; Durmaz, T. Systemic Immune-Inflammation Index Is A Novel Marker to Predict Func-tionally Significant Coronary Artery Stenosis. Biomark. Med. 2020, 14, 1553–1561. [Google Scholar] [CrossRef]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of Systemic immune-inflammation index in cancer: A meta-analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef] [PubMed]
- Ruta, V.; Man, A.; Alexescu, T.; Motoc, N.; Tarmure, S.; Ungur, R.; Todea, D.; Coste, S.; Valean, D.; Pop, M. Neutrophil-To-Lymphocyte Ratio and Systemic Immune-Inflammation Index—Biomarkers in Interstitial Lung Disease. Medicina 2020, 56, 381. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, D.; Dai, Z.; Li, X. Association between Systemic Immune-Inflammation Index and Diabetic Depression. Clin. Interv. Aging 2021, 16, 97–105. [Google Scholar] [CrossRef]
- Zhou, L.; Ma, X.; Wang, W. Inflammation and Coronary Heart Disease Risk in Patients with Depression in China Mainland: A Cross-Sectional Study. Neuropsychiatr. Dis. Treat. 2020, 16, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedetti, F.; Mazza, M.; Cavalli, G.; Ciceri, F.; Dagna, L.; Rovere-Querini, P. Can Cytokine Blocking Prevent Depression in COVID-19 Survivors? J. Neuroimmune Pharmacol. 2021, 16, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; Feng, R.; Yang, Y. Changes in the serum levels of inflammatory cytokines in antidepressant drug-naïve patients with major depression. PLoS ONE 2018, 13, e0197267. [Google Scholar] [CrossRef]
- Osimo, E.; Pillinger, T.; Rodriguez, I.; Khandaker, G.; Pariante, C.; Howes, O. Inflammatory Markers in Depression: A Meta-Analysis of Mean Differences and Variability in 5166 Patients And 5083 Controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta-Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Munkholm, K.; Vinberg, M.; Kessing, L.V. Cytokines in bipolar disorder: A systematic review and meta-analysis. J. Affect. Disord. 2013, 144, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Guo, W.; Feng, Y.; Deng, H.; Li, G.; Nie, H.; Guo, G.; Yu, H.; Ma, Y.; Wang, J.; et al. Efficacy and safety of anti-inflammatory agents for the treatment of major depressive disorder: A systematic review and meta-analysis of randomised controlled trials. J. Neurol. Neurosurg. Psychiatry 2020, 91, 21–32. [Google Scholar] [CrossRef]
- Köhler-Forsberg, O.; Lydholm, N.C.; Hjorthøj, C.; Nordentoft, M.; Mors, O.; Benros, M. Efficacy of Anti-Inflammatory Treatment on Major Depressive Disorder or Depressive Symptoms: Meta-Analysis of Clinical Trials. Acta Psychiatr. Scand. 2019, 139, 404–419. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, J.; Kakar, R.; Berk, M.; Kessing, L.; Vinberg, M.; Baune, B.; Mansur, R.; Brietzke, E.; Goldstein, B.; McIntyre, R. Anti-Inflammatory Agents in The Treatment of Bipolar Depression: A Systematic Review and Meta-Analysis. Bipolar Disord. 2016, 18, 89–101. [Google Scholar] [CrossRef]
- Rosenblat, J.D. Targeting the immune system in the treatment of bipolar disorder. Psychopharmacology 2019, 236, 2909–2921. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, L.; Surace, T.; Vanella, A.; Meo, V.; Patania, F.; Furnari, R.; Signorelli, M.S.; Aguglia, E. The effect of adjunctive nutraceuticals in bipolar disorder: A systematic review of randomized placebo-controlled trials. J. Affect. Disord. 2019, 252, 334–349. [Google Scholar] [CrossRef]
- Rosenblat, J.D.; McIntyre, R.S. Bipolar Disorder and Inflammation. Psychiatr. Clin. North Am. 2016, 39, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Leboyer, M.; Soreca, I.; Scott, J.; Frye, M.; Henry, C.; Tamouza, R.; Kupfer, D. Can Bipolar Disorder Be Viewed as a Multi-System Inflammatory Disease? J. Affect. Disord. 2012, 141, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dionisie, V.; Filip, G.A.; Manea, M.C.; Manea, M.; Riga, S. The anti-inflammatory role of SSRI and SNRI in the treatment of depression: A review of human and rodent research studies. Inflammopharmacology 2021, 29, 75–90. [Google Scholar] [CrossRef]
- Nerurkar, L.; Siebert, S.; McInnes, I.B.; Cavanagh, J. Rheumatoid arthritis and depression: An inflammatory perspective. Lancet Psychiatry 2019, 6, 164–173. [Google Scholar] [CrossRef]
- Maes, M.; Kubera, M.; Obuchowiczwa, E.; Goehler, L.; Brzeszcz, J. Depression’s Multiple Comorbidities Explained By (Neuro) Inflammatory and Oxidative & Nitrosative Stress Pathways. Neuroendocr. Lett. 2011, 32, 7–24. [Google Scholar]
- Schaefer, M.; Engelbrechta, M.A.; Gut, O.; Fiebich, B.L.; Bauer, J.; Schmidt, F.; Grunze, H.; Lieb, K. Interferon alpha (IFNα) and psychiatric syndromes. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2002, 26, 731–746. [Google Scholar] [CrossRef]
- Mazza, M.; Tringali, A.; Rossetti, A.; Botti, R.; Clerici, M. Cross-Sectional Study of Neutrophil-Lymphocyte, Platelet-Lymphocyte and Monocyte-Lymphocyte Ratios in Mood Disorders. Gen Hosp. Psychiatry 2019, 58, 7–12. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Natale, A.; Amerio, A.; Cimpoesu, P.; Filioli, P.G.; Aguglia, E.; Amore, M.; Serafini, G.; Aguglia, A. Neutrophil-to-Lymphocyte, Platelet-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio in Bipolar Disorder. Brain Sci. 2021, 11, 58. [Google Scholar] [CrossRef]
- Fernandes, B.; Steiner, J.; Molendijk, M.; Dodd, S.; Nardin, P.; Gonçalves, C.; Jacka, F.; Köhler, C.; Karmakar, C.; Carvalho, A.; et al. C-Reactive Protein Concentrations Across the Mood Spectrum in Bipolar Disorder: A Systematic Review and Meta-Analysis. Lancet Psychiatry 2016, 3, 1147–1156. [Google Scholar] [CrossRef]
- Rowland, T.; Perry, B.; Upthegrove, R.; Barnes, N.; Chatterjee, J.; Gallacher, D.; Marwaha, S. Neurotrophins, Cytokines, Ox-idative Stress Mediators and Mood State in Bipolar Disorder: Systematic Review and Meta-Analyses. Br. J. Psychiatry 2018, 213, 514–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.-M.; Su, T.-P.; Li, C.-T.; Tsai, S.-J.; Chen, M.-H.; Tu, P.-C.; Chiou, W.-F. Comparison of pro-inflammatory cytokines among patients with bipolar disorder and unipolar depression and normal controls. Bipolar Disord. 2014, 17, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.-M.; Chen, M.-H.; Hsu, J.-W.; Huang, K.-L.; Tu, P.-C.; Chang, W.-C.; Su, T.-P.; Li, C.T.; Lin, W.-C.; Tsai, S.-J. A comparison study of metabolic profiles, immunity, and brain gray matter volumes between patients with bipolar disorder and depressive disorder. J. Neuroinflammation 2020, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.-H.; Chang, W.-C.; Hsu, J.-W.; Huang, K.-L.; Tu, P.-C.; Su, T.-P.; Li, C.-T.; Lin, W.-C.; Bai, Y.-M. Correlation of proinflammatory cytokines levels and reduced gray matter volumes between patients with bipolar disorder and unipolar depression. J. Affect. Disord. 2019, 245, 8–15. [Google Scholar] [CrossRef]
- Bowden, C.L. A different depression: Clinical distinctions between bipolar and unipolar depression. J. Affect. Disord. 2005, 84, 117–125. [Google Scholar] [CrossRef]
- Gitlin, M.J. Antidepressants in bipolar depression: An enduring controversy. Int. J. Bipolar Disord. 2018, 6, 25. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, B.S.; Gama, C.S.; Kauer-Sant’Anna, M.; Lobato, M.I.; Belmonte-De-Abreu, P.; Kapczinski, F. Serum brain-derived neurotrophic factor in bipolar and unipolar depression: A potential adjunctive tool for differential diagnosis. J. Psychiatr. Res. 2009, 43, 1200–1204. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Supasitthumrong, T.; Teixeira, A.L.; Vieira, E.L.; Gattaz, W.F.; Benseñor, I.M.; Lotufo, P.A.; Lafer, B.; Berk, M.; Carvalho, A.F.; et al. Differences in the immune-inflammatory profiles of unipolar and bipolar depression. J. Affect. Disord. 2020, 262, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Wang, T.; Lee, I.; Lee, S.; Chen, K.; Huang, S.; Yang, Y.; Lu, R.; Chen, P. C-Reactive Protein: A Differential Biomarker For Major Depressive Disorder and Bipolar II Disorder. World J. Biol. Psychiatry 2016, 18, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Zhang, C.; Chen, J.; Zhao, G.; Zhou, R.; Wang, F.; Xu, J.; Yang, T.; Su, Y.; Huang, J.; et al. Different levels of pro- and anti-inflammatory cytokines in patients with unipolar and bipolar depression. J. Affect. Disord. 2018, 237, 65–72. [Google Scholar] [CrossRef]
- Wollenhaupt-Aguiar, B.; Librenza-Garcia, D.; Bristot, G.; Przybylski, L.; Stertz, L.; Burque, R.K.; Ceresér, K.M.; Spanemberg, L.; Caldieraro, M.A.; Frey, B.N.; et al. Differential biomarker signatures in unipolar and bipolar depression: A machine learning approach. Aust. New Zealand J. Psychiatry 2019, 54, 393–401. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Sample (N = 182) | BD Manic Episode (N = 65) | BD Depressive Episode (N = 34) | MDD (N = 83) | p | |
|---|---|---|---|---|---|
| Gender, N (%) | 0.925 1 | ||||
| Males | 84 (46.2) | 31 (47.7) | 16 (47.1) | 37 (44.6) | |
| Females | 98 (53.8) | 34 (52.3) | 18 (52.9) | 46 (56.4) | |
| Age (years), mean ± SD | 44.41 ± 12.29 | 41.25 ± 11.6 | 47.59 ± 12.02 | 45.58 ± 12.45 | 0.0152 |
| Level of education, N (%) | 0.0242 | ||||
| ≤8 years | 38 (20.9) | 7 (10.8) | 7 (20.6) | 24 (28.9) | |
| 9–12 years | 93 (51.1) | 35 (53.8) | 17 (50.0) | 41 (49.4) | |
| >12 years | 51 (28) | 23 (35.4) | 10 (29.4) | 18 (21.7) | |
| Marital status, N (%) | 0.062 2 | ||||
| Single | 68 (37.4) | 35 (53.8) | 10 (29.4) | 23 (27.7) | |
| Married | 62 (34.1) | 15 (23.1) | 12 (35.3) | 35 (42.2) | |
| Divorced | 26 (14.3) | 6 (9.2) | 8 (23.5) | 12 (14.5) | |
| Widowed | 6 (3.3) | 0 | 0 | 6 (7.2) | |
| Domestic Partnership | 20 (11.0) | 9 (13.8) | 4 (11.8) | 7 (8.4) | |
| Smoking status, N (%) | 0.011 1 | ||||
| Yes | 105 (57.7) | 47 (72.3) | 18 (52.9) | 40 (48.2) | |
| No | 77 (42.3) | 18 (27.7) | 16 (47.1) | 43 (51.8) | |
| Psychotic symptoms, N (%) | <0.0011 | ||||
| Yes | 64 (35.2) | 43 (66.2) | 28 (82.4) | 15 (18.1) | |
| No | 118 (64.8) | 22 (33.8) | 6 (17.6) | 68 (81.9) | |
| BMI (kg/m2), mean ± SD | 24.92 ± 2.86 | 25.17 ± 2.56 | 25.47 ± 2.25 | 24.51 ± 3.25 | 0.449 2 |
| Total Sample | BD Manic Episode | BD Depressive Episode | MDD | p | |
|---|---|---|---|---|---|
| White blood cells (103 cells/mm3) | 7.5 ± 1.87 | 8.13 ± 2 | 7.38 ± 1.78 | 7.05 ± 1.66 | 0.0021 |
| Neutrophils (103 cells/mm3) | 4.34 ± 1.61 | 5.13 ± 1.63 | 4.40 ± 1.68 | 3.68 ± 1.24 | 0.0002 |
| Lymphocytes (103 cells/mm3) | 2.38 ± 0.73 | 2.25 ± 0.67 | 2.24 ± 0.63 | 2.54 ± 0.77 | 0.0222 |
| Monocytes (103 cells/mm3) | 0.61 ± 0.17 | 0.64 ± 0.18 | 0.57 ± 0.13 | 0.61 ± 0.18 | 0.072 2 |
| Platelets (103 cells/mm3) | 264.76 ± 59.05 | 264.65 ± 52.26 | 255.35 ± 52.93 | 268.7 ± 65.63 | 0.683 2 |
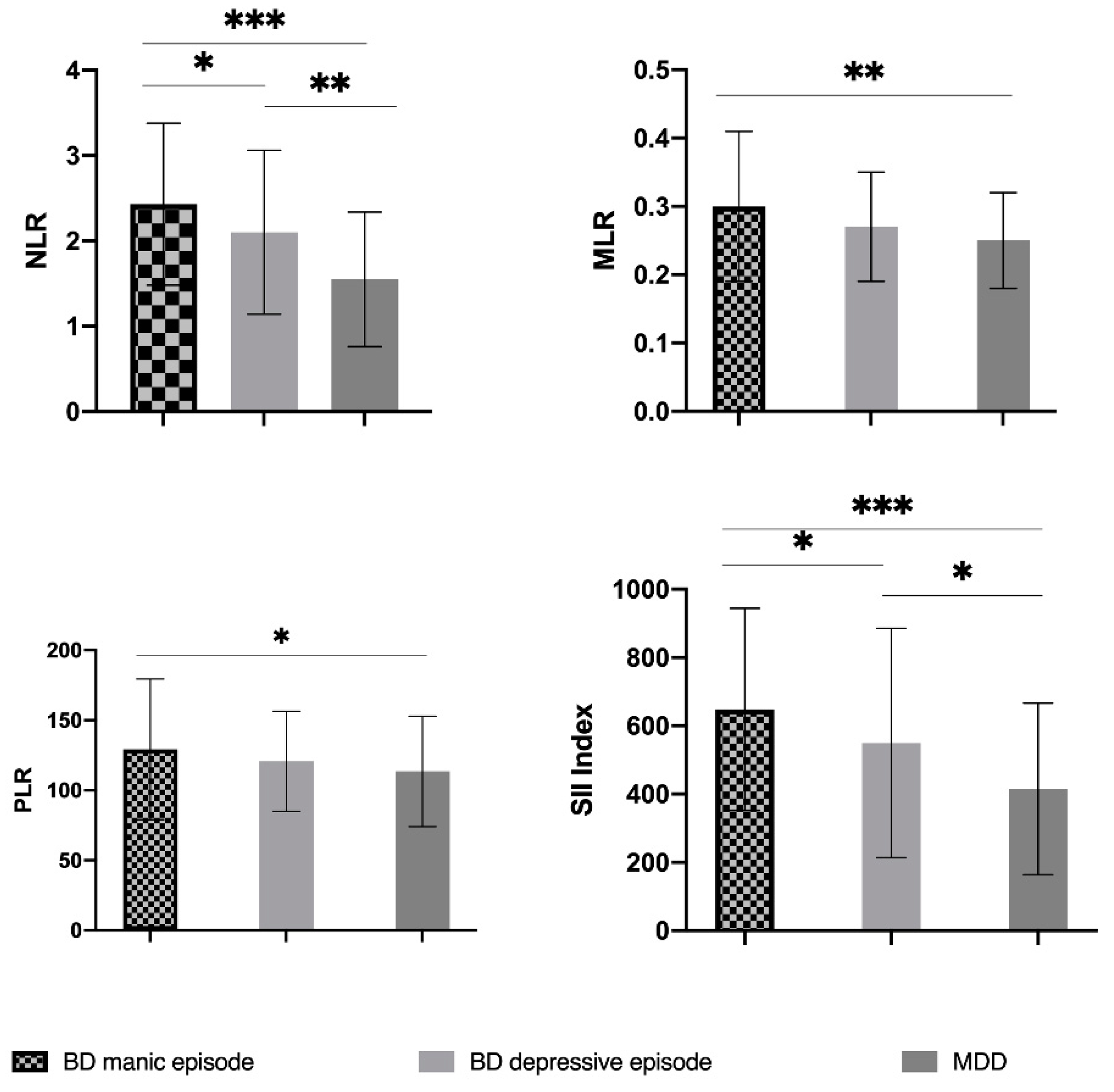
| NLR | 1.97 ± 0.97 | 2.43 ± 0.95 | 2.10 ± 0.96 | 1.55 ± 0.79 | 0.0002 |
| PLR | 120.47 ± 43.56 | 129.21 ± 50.19 | 120.78 ± 35.66 | 113.5 ± 39.47 | 0.068 2 |
| MLR | 0.27 ± 0.09 | 0.30 ± 0.11 | 0.27 ± 0.08 | 0.25 ± 0.07 | 0.0032 |
| SII Index | 523.53 ± 303.58 | 648.21 ± 295.79 | 549.40 ± 335.78 | 415.13 ± 251.45 | 0.0002 |
| Glycemia (mg/dL) | 92.03 ± 11.78 | 91.58 ± 12.16 | 94.5 ± 12.32 | 91.06 ± 11.41 | 0.158 1 |
| Total Cholesterol (mg/dL) | 189.42 ± 45.80 | 177.18 ± 47.49 | 193.32 ± 49.30 | 197.40 ± 41.26 | 0.0072 |
| Triglycerides (mg/dL) | 131.0 ± 79.90 | 138.40 ± 101.95 | 135.68 ± 78.41 | 123.29 ± 58.25 | 0.919 2 |
| BD Mania vs. BD Depression | BD Mania vs. MDD | BD Depression vs. MDD | |
|---|---|---|---|
| White blood cells (103 cells/mm3) 1 | 0.072 | <0.001 | 0.344 |
| Neutrophils (103 cells/mm3) 2 | 0.009 | <0.001 | 0.038 |
| Lymphocytes (103 cells/mm3) 2 | 0.754 | 0.030 | 0.016 |
| Monocytes (103 cells/mm3) 2 | 0.023 | 0.126 | 0.368 |
| Platelets (103 cells/mm3) 2 | 0.470 | 0.951 | 0.391 |
| NLR 2 | 0.047 | <0.001 | 0.001 |
| PLR 2 | 0.635 | 0.034 | 0.113 |
| MLR 2 | 0.095 | 0.001 | 0.368 |
| SII index 2 | 0.033 | <0.001 | 0.015 |
| Binary logistic regression: NLR Univariate analysis, R2 Nagelkerke = 0.108, p = 0.002 | ||||||||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| 0.778 | 0.301 | 6.692 | 1 | 0.010 | 2.178 | 1.208 | 3.927 | |
| Binary logistic regression: SII Index Univariate analysis, R2 Nagelkerke = 0.059, p = 0.026 | ||||||||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| SII Index | 0.002 | 0.001 | 3.950 | 1 | 0.047 | 1.002 | 1.000 | 1.003 |
| Binary logistic regression: Multivariate analysis, Model 2, R2 Nagelkerke = 0.235, p = 0.021, Method: Enter | ||||||||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| NLR | 0.914 | 0.328 | 7.780 | 1 | 0.005 | 2.495 | 1.312 | 4.744 |
| Age | 0.032 | 0.022 | 2.204 | 1 | 0.138 | 1.033 | 0.990 | 1.078 |
| Gender | 0.077 | 0.478 | 0.026 | 1 | 0.872 | 1.080 | 0.423 | 2.753 |
| BMI | 0.172 | 0.092 | 3.520 | 1 | 0.061 | 1.188 | 0.992 | 1.421 |
| Smoking status | −0.350 | 0.482 | 0.527 | 1 | 0.468 | 0.705 | 0.274 | 1.812 |
| Glycemia | 0.019 | 0.020 | 0.926 | 1 | 0.336 | 1.020 | 0.980 | 1.061 |
| Total Cholesterol | −0.014 | 0.006 | 4.552 | 1 | 0.033 | 0.987 | 0.974 | .999 |
| Triglycerides | 0.005 | 0.004 | 1.597 | 1 | 0.206 | 1.005 | 0.997 | 1.012 |
| Level of education | 0.601 | 0.341 | 3.104 | 1 | 0.078 | 1.824 | 0.935 | 3.559 |
| Marital status | 0.141 | 0.199 | 0.503 | 1 | 0.478 | 1.151 | 0.780 | 1.699 |
| Constant | −9.503 | 3.461 | 7.540 | 1 | 0.006 | 0.000 | ||
| Binary logistic regression: Multivariate analysis, Model 3, R2 Nagelkerke = 0.248, p = 0.022, Method: Enter | ||||||||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| NLR | 1.670 | 0.768 | 4.730 | 1 | 0.030 | 5.311 | 1.179 | 23.919 |
| SII Index | −0.003 | 0.002 | 1.221 | 1 | 0.269 | 0.997 | 0.993 | 1.002 |
| Age | 0.035 | 0.022 | 2.455 | 1 | 0.117 | 1.035 | 0.991 | 1.081 |
| Gender | 0.112 | 0.482 | 0.054 | 1 | 0.816 | 1.119 | 0.435 | 2.877 |
| Smoking status | −0.202 | 0.502 | 0.162 | 1 | 0.687 | 0.817 | 0.306 | 2.184 |
| BMI | 0.171 | 0.093 | 3.423 | 1 | 0.064 | 1.187 | 0.990 | 1.423 |
| Glycemia | 0.024 | 0.021 | 1.342 | 1 | 0.247 | 1.025 | 0.983 | 1.068 |
| Total Cholesterol | −0.012 | 0.006 | 3.630 | 1 | 0.057 | 0.988 | 0.975 | 1.000 |
| Triglycerides | 0.004 | 0.004 | 1.094 | 1 | 0.295 | 1.004 | 0.996 | 1.012 |
| Level of Education | 0.544 | 0.345 | 2.493 | 1 | 0.114 | 1.723 | 0.877 | 3.385 |
| Marital status | 0.162 | 0.202 | 0.648 | 1 | 0.421 | 1.176 | 0.792 | 1.747 |
| Constant | −10.33 | 3.607 | 8.206 | 1 | 0.004 | 0.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dionisie, V.; Filip, G.A.; Manea, M.C.; Movileanu, R.C.; Moisa, E.; Manea, M.; Riga, S.; Ciobanu, A.M. Neutrophil-to-Lymphocyte Ratio, a Novel Inflammatory Marker, as a Predictor of Bipolar Type in Depressed Patients: A Quest for Biological Markers. J. Clin. Med. 2021, 10, 1924. https://doi.org/10.3390/jcm10091924
Dionisie V, Filip GA, Manea MC, Movileanu RC, Moisa E, Manea M, Riga S, Ciobanu AM. Neutrophil-to-Lymphocyte Ratio, a Novel Inflammatory Marker, as a Predictor of Bipolar Type in Depressed Patients: A Quest for Biological Markers. Journal of Clinical Medicine. 2021; 10(9):1924. https://doi.org/10.3390/jcm10091924
Chicago/Turabian StyleDionisie, Vlad, Gabriela Adriana Filip, Mihnea Costin Manea, Robert Constantin Movileanu, Emanuel Moisa, Mirela Manea, Sorin Riga, and Adela Magdalena Ciobanu. 2021. "Neutrophil-to-Lymphocyte Ratio, a Novel Inflammatory Marker, as a Predictor of Bipolar Type in Depressed Patients: A Quest for Biological Markers" Journal of Clinical Medicine 10, no. 9: 1924. https://doi.org/10.3390/jcm10091924
APA StyleDionisie, V., Filip, G. A., Manea, M. C., Movileanu, R. C., Moisa, E., Manea, M., Riga, S., & Ciobanu, A. M. (2021). Neutrophil-to-Lymphocyte Ratio, a Novel Inflammatory Marker, as a Predictor of Bipolar Type in Depressed Patients: A Quest for Biological Markers. Journal of Clinical Medicine, 10(9), 1924. https://doi.org/10.3390/jcm10091924