
Undiagnosed Diabetes and Prediabetes in Patients with Chronic Coronary Syndromes—An Alarming Public Health Issue

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
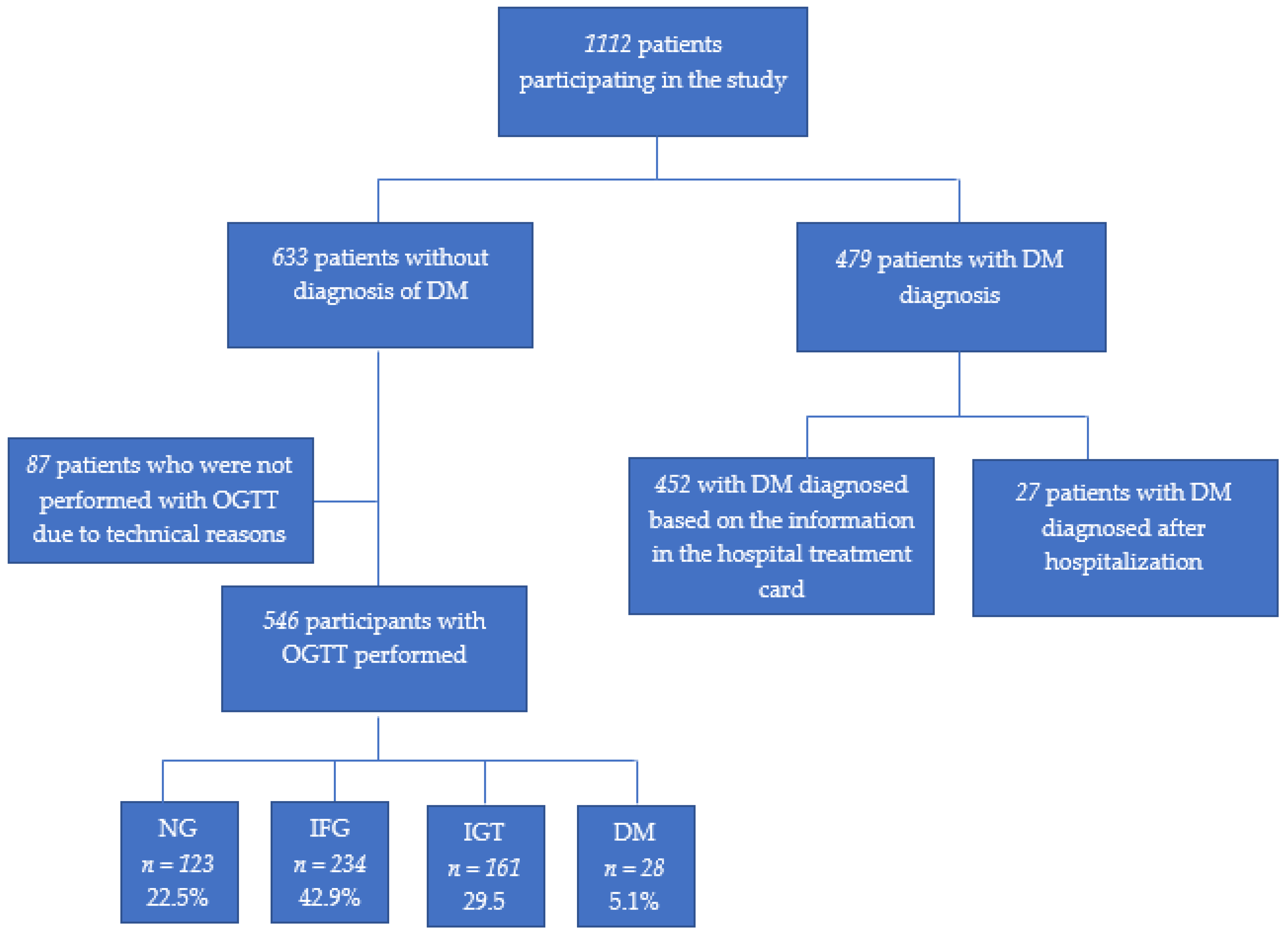
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuller, L.H.; Velentgas, P.; Barzilay, J.; Beauchamp, N.J.; O’Leary, D.H.; Savage, P.J. Diabetes Mellitus: Subclinical Cardiovascular Disease and Risk of Incident Cardiovascular Disease and All-Cause Mortality. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 823–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.M.M.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalska, I.; Prokop, J.; Bachórzewska-Gajewska, H.; Telejko, B.; Kinalskal, I.; Kochman, W.; Musial, W. Disturbances of glucose metabolism in men referred for coronary arteriography. Postload glycemia as predictor for coronary atherosclerosis. Diabetes Care 2001, 24, 897–901. [Google Scholar] [CrossRef] [Green Version]
- Cai, X.; Zhang, Y.; Li, M.; Wu, J.H.; Mai, L.; Li, J.; Yang, Y.; Hu, Y.; Huang, Y. Association between prediabetes and risk of all cause mortality and cardiovascular disease: Updated meta-analysis. BMJ 2020, 370, m2297. [Google Scholar] [CrossRef]
- Wang, T.; Lu, J.; Su, Q.; Chen, Y.; Bi, Y.; Mu, Y.; Chen, L.; Hu, R.; Tang, X.; Yu, X.; et al. Ideal Cardiovascular Health Metrics and Major Cardiovascular Events in Patients With Prediabetes and Diabetes. JAMA Cardiol. 2019, 4, 874–883. [Google Scholar] [CrossRef]
- American Diabetes Association. Prevention or delay of type 2 diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43 (Suppl. 1), S32–S36. [Google Scholar] [CrossRef] [Green Version]
- Piller, C. Dubious diagnosis. A war on “prediabetes” has created millions of new patients and a tempting opportunity for pharma. But how real is the condition? Science 2019, 363, 1026–1031. [Google Scholar] [CrossRef] [Green Version]
- Pasnoor, M.; Dimachkie, M.M.; Kluding, P.M.; Barohn, R.J. Diabetic Neuropathy Part 1. Neurol. Clin. 2013, 31, 425–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Donk, M.; Sandbæk, A.; Borch-Johnsen, K.; Lauritzen, T.; Simmons, R.K.; Wareham, N.J.; Rutten, G.E.H.M. Screening for type 2 diabetes: Lessons from the addition-Europe study. Diabet Med. 2011, 28, 1416–1424. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Diabetes Country Profiles; World Health Organization: Warsaw, Poland, 2016; Available online: https://www.who.int/diabetes/country-profiles/pol_en.pdf (accessed on 17 February 2021).
- Rutkowski, M.; Wojciechowska, A.; Śmigielski, W.; Drygas, W.; Piwońska, A.; Pająk, A.; Tykarski, A.; Kozakiewicz, K.; Waśniewska, M.K.; Zdrojewski, T. Prevalence of diabetes and impaired fasting glucose in Poland in 2005–2014: Results of the WOBASZ surveys. Diabet. Med. 2020, 37, 1528–1535. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network: Brussels, Belgium, 2017. [Google Scholar]
- Strojek, K.; Rokicka, D.; Szymborska-Kajanek, A.; Wróbel, M. Empagliflozin. Results of the EMPA-REG OUTCOME trial. A breakthrough in treatment of type 2 diabetes? Clin. Diabetol. 2016, 5, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Jankowski, P.; Kosior, D.A.; Sowa, P.; Szóstak-Janiak, K.; Kozieł, P.; Krzykwa, A.; Sawicka, E.; Haberka, M.; Setny, M.; Kamiński, K.; et al. Secondary prevention of coronary artery disease in Poland. Results from the POLASPIRE survey. Cardiol. J. 2020, 27, 533–540. [Google Scholar] [CrossRef]
- World Health Organization Definition. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 17 February 2021).
- Zdrojewski, T.; Rutkowski, M.; Bandosz, P.; Gaciong, Z.; Solnica, B.; Drygas, W.; Wyrzykowski, B. Ocena rozpowszechnienia i kontroli czynników ryzyka chorób serca i naczyń w Polsce—badania NATPOL 1997, 2002, 2011. In Epidemiologia i Prewencja Chorób Układu Krążenia; Medycyna Praktyczna: Kraków, Poland, 2015; pp. 57–64. [Google Scholar]
- National Diabetes Statistics Report. Estimates of Diabetes and Its Burden in the United State. 2017. Available online: https://dev.diabetes.org/sites/default/files/2019-06/cdc-statistics-report-2017 (accessed on 17 February 2021).
- Bartnik, M.; Ryden, L.; Ferrari, R.; Malmberg, K.; Pyörälä, K.; Simoons, M.; Öhrvik, J. The prevalence of abnormal glucose regulation in patients with coronary artery disease across Europe the Euro Heart Survey on diabetes and the heart. Eur. Heart J. 2004, 25, 1880–1890. [Google Scholar] [CrossRef] [PubMed]
- Abdulai, T.; Li, Y.; Zhang, H.; Tu, R.; Liu, X.; Zhang, L.; Dong, X.; Li, R.; Wang, Y.; Wang, C. Prevalence of impaired fasting glucose, type 2 diabetes and associated risk factors in undiagnosed Chinese rural population: The Henan Rural Cohort Study. BMJ Open 2019, 9, e029628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lüders, S.; Hammersen, F.; Kulschewski, A.; Venneklaas, U.; Züchner, C.; Gansz, A.; Schnieders, M.; Pfarr, E.; Sturm, C.D.; Paar, W.D.; et al. Diagnosis of impaired glucose tolerance in hypertensive patients in daily clinical practice. Int. J. Clin. Pr. 2005, 59, 632–638. [Google Scholar] [CrossRef]
- Makaroff, L.E. The need for international consensus on prediabetes. Lancet Diabetes Endocrinol. 2017, 5, 5–7. [Google Scholar] [CrossRef]
- Ferrannini, G.; De Bacquer, D.; De Backer, G.; Kotseva, K.; Mellbin, L.; Wood, D.; Rydén, L. Screening for Glucose Perturbations and Risk Factor Management in Dysglycemic Patients With Coronary Artery Disease—A Persistent Challenge in Need of Substantial Improvement: A Report From ESC EORP EUROASPIRE V. Diabetes Care 2020, 43, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Ali, I.; Kaleem, W.A.; Yasmeen, F. Correlation between Body Mass Index and Lipid Profile in patients with Type 2 Diabetes attending a tertiary care hospital in Peshawar. Pak. J. Med. Sci. 2019, 35, 591–597. [Google Scholar] [CrossRef] [Green Version]
- Omotoye, F.E.; Fadupin, G.T. Effect of Body Mass Index on Lipid Profile of Type 2 Diabetic Patients at An Urban Tertiary Hospital In Nigeria. Iosr J. Dent. Med. Sci. 2016, 15, 65–70. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Armstrong, E.J.; Kim, G.; Oh, J.; Kang, S.-M.; Lee, B.-W.; Ahn, C.W.; Cha, B.S.; Lee, H.C.; Mantzoros, C.S.; et al. Undiagnosed diabetes is prevalent in younger adults and associated with a higher risk cardiometabolic profile compared to diagnosed diabetes. Am. Hear. J. 2015, 170, 760–769.e2. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.H.; Smith, F.B.; Lee, A.J.; Fowkes, F.G.R. Criteria for previously undiagnosed diabetes and risk of mortality: 15-year follow-up of the Edinburgh Artery Study cohort. Diabet. Med. 2005, 22, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Edwards, C.M.; Cusi, K. Prediabetes: A Worldwide Epidemic. Endocrinol. Metab. Clin. North Am. 2016, 45, 751–764. [Google Scholar] [CrossRef]
- Nichols, G.A.; Brown, J.B. Higher Medical Care Costs Accompany Impaired Fasting Glucose. Diabetes Care 2005, 28, 2223–2229. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Dall, T.M.; Chen, Y.; Baldwin, A.; Yang, W.; Mann, S.; Moore, V.; Le Nestour, E.; Quick, W.W. Medical Cost Associated with Prediabetes. Popul. Heal. Manag. 2009, 12, 157–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, B.H.; Song, X.; Andrews, L.M.; Purkayastha, D.; Princic, N.; Sedgley, R.; Rudolph, A.E. Progression to type 2 diabetes, healthcare utilization, and cost among pre-diabetic patients with or withoutcomorbid hypertension. Curr. Med. Res. Opin. 2011, 27, 809–819. [Google Scholar] [CrossRef]
- Haberka, M.; Jankowski, P.; Kosior, D.A.; Szpakowicz, M.; Szóstak-Janiak, K.; Kozieł, P.; Krzykwa, A.; Łapińska, M.; Setny, M.; Kamiński, K.; et al. Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus—Polish multicenter study POLASPIRE. Arch. Med. Sci. 2020, 16. [Google Scholar] [CrossRef]
- Kozieł, P.; Jankowski, P.; Mirek-Bryniarska, E.; Nessler, J.; Podolec, P.; De Bacquer, D.; Kotseva, K.; Wood, D.; Czarnecka, D.; Kawecka-Jaszcz, K.; et al. Obesity in patients with established coronary artery disease over a 20-year period (1997–2017). Pol. Arch. Intern. Med. 2021, 131, 26–32. [Google Scholar] [CrossRef]
- Niedziela, J.T.; Hiczkiewicz, J.; Kleinrok, A.; Pączek, P.; Leszek, P.; Lelonek, M.; Rozentryt, P.; Parma, Z.; Witkowski, A.; Bartuś, S.; et al. Prevalence, characteristics and prognostic implications of type 2 diabetes in patients with myocardial infarction: PL-ACS Registry annual report 2018. Kardiol. Pol. 2020, 78, 243–246. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| DM n = 47 | IQR 1 | No DM, OGTT Performed n = 546 | IQR 1 | No DM, OGTT Was Not Performed n = 87 | IQR 1 | p | ||
|---|---|---|---|---|---|---|---|---|
| Sex | M n (%) | 328 (68.5) | 399 (73.1%) | 63 (72.4%) | 0.258 | |||
| Age median | 70 a | 64.0–75.0 | 67 a | 62.0–73.0 | 67 | 63.0–75.0 | <0.01 | |
| BMI (kg/m2) median | 30.5 a,b | 27.5–33.6 | 28.64 a | 25.9–31.5 | 28.33 b | 25.3–30.5 | <0.01 | |
| Body weight (kg) median | 86.00 a,b | 77.0–97.0 | 81.28 a | 73.0–91.0 | 79.0 b | 71.0–90.0 | <0.01 | |
| Waist circumference (cm) median | 105.0 a,b | 98.0–113.0 | 100.0 a | 95.0–108.0 | 99 b | 90.0–104.0 | <0.01 | |
| Total cholesterol (mg/dL) median | 145.0 a,b | 123.4–177.9 | 153 a | 132.1–181.7 | 160 b | 141.5–193.3 | <0.01 | |
| LDL (mg/dL) median | 70.69 a,b | 54.1–92.8 | 80.72 a | 64.8–101.7 | 83.20 b | 66.0–109.3 | <0.01 | |
| HDL-C (mg/dL L) median | 46 a,b | 38.7–56.5 | 50 a | 42.9–60.5 | 50.66 b | 44.7–58.9 | <0.01 | |
| TG (mg/dL) median | 126.4 a,b | 89.5–169.2 | 105 a | 78.9–143.7 | 105.1 b | 74.0–138.0 | <0.01 | |
| HbA1C (%) median | 6.5 a,b | 6.0–7.4 | 5.70 a | 5.5–6.0 | 5.6 b | 5.4–5.9 | <0.01 | |
| Index event n (%) | CABG | 17 (3.5%) | 23(4.2%) | 6(6.9%) | <0.01 | |||
| PCI | 185(38.6%) a | 208(38.1%) b | 12(13.8%) a,b | |||||
| STEMI | 62(12.9%) a | 88(16.1%) b | 27(31%) a,b | |||||
| NSTEMI | 121(25.3%) | 105(19.2%) | 24(27.6%) | |||||
| Unstable angina | 94(19.6%) | 122(22.3%) | 18(20.7%) | |||||
| lifestyle change n (%) | reduction in salt consumption | 272(71.6%) | 352(66.3%) | 51(59.3%) | 0.08 | |||
| reduction in fat consumption | 303(79.5%) a,b | 365(67.8%) a | 55(64%) b | <0.01 | ||||
| reduction in calories consumption | 250(65.8%) a | 323(60.3%) | 38(44.2%) a | <0.01 | ||||
| more fruits and vegetables consumption | 291(76.4%) | 378(70.1%) | 62(72.1%) | 0.266 | ||||
| more fishes consumption | 174(45.7%) | 240(44.8%) | 41(47.7%) | 0.610 | ||||
| reduction in sugar consumption | 307(80.6%) a,b | 320(59.5%) a | 48(55.8%) b | <0.01 | ||||
| reduction in alcohol consumption | 247(65.2%) a,b | 299(55.8%) a | 38(44.2%) b | 0.03 | ||||
| compliance with dietary recommendations | 258(67.7%) a | 273(50.8%) a | 47(54,7%) | <0.01 | ||||
| Categories of Diagnosis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NGT n = 123 | IQR | IFG n = 234 | IQR | IGT n = 161 | IQR | Newly Diagnosed DM n = 28 | IQR * | p | ||
| sex | M n (%) | 85 (69.1%) | 181 (77.4%) | 112 (69.6%) | 21 (75%) | 0.239 | ||||
| Age median | 67.0 | 60.0–73.0 | 65.0 a,b | 61.0–62.0 | 69.0 a | 63.0–75.0 | 69.0 b | 66.0–73.0 | <0.05 | |
| BMI (kg/m2) median | 27.5 a,b,c | 24.5–29.9 | 28.6 a | 25.9–31.5 | 29.4 b | 26.6–32.6 | 29.3 c | 27.2–30.7 | <0.05 | |
| Body weight (kg) median | 80.0 a,b | 67.0–88.5 | 82.0 b | 75.0–93.0 | 81.2 a | 74.0–92.2 | 81.0 | 74.3–90.5 | <0.05 | |
| Waist circumference (cm) median | 99.0 a,b,c | 92.0–105.0 | 100.0 a | 95.0–108.0 | 103.0 b | 95.0–110.0 | 102.5 c | 99.0–107.0 | <0.01 | |
| Total cholesterol (mg/dL) median | 155.5 | 134.0–187.0 | 150.8 | 131.5–180.0 | 154.0 | 132.0–181.5 | 144.5 | 132.5–170.0 | ||
| LDL (mg/dL) median | 85.8 | 66.8–106.0 | 77.3 | 65.0–100.5 | 78.9 | 64.8–101.3 | 80.2 | 56.8–106.1 | ||
| HDL-C (mg/dL L) median | 52.5 | 43.0–63.1 | 49 | 42.1–58.4 | 51.0 | 43.0–61.0 | 67.6 | 42.0–54.0 | ||
| TG (mg/dL) median | 101.9 | 76.0–135.0 | 107.0 | 80.0–145.0 | 109.0 | 78.0–144.4 | 120.5 | 98.8–195.3 | ||
| HbA1C (%) median | 5.6 a,b,c | 5.4–5.8 | 5.7 a,d,e | 5.5–5.9 | 5.8 b,d,f | 5.6–6.1 | 6.1 c,e,f | 5.7–6.4 | <0.01 | |
| NGT n = 123 | IFG n = 234 | IGT n = 161 | Newly Diagnosed DM n = 28 | p | ||
|---|---|---|---|---|---|---|
| Indexe vent n (%) | CABG | 6(4.9%) | 12(5.1%) | 4(2.5%) | 1(3.6%) | |
| PCI | 52(42.3%) | 84(35.9%) | 61(37.9%) | 11(39.3%) | ||
| STEMI | 22(17.9%) | 38(16.2%) | 21(13%) | 7(25%) | 0.579 | |
| NSTEMI | 19(15.4%) | 50(21.4%) | 34(21.1%) | 2(7.1%) | ||
| Unstable angina | 24(19.5%) | 50(21.4%) | 41(25.5%) | 7(25%) | ||
| lifestyle change n (%) | reduction in salt consumption | 79(65.8%) | 151(66.2%) | 108(69.2%) | 14(51.9%) | 0.607 |
| reduction in fat consumption | 83(67.5%) | 156(68.1%) | 112(70.9%) | 14(50%) | 0.228 | |
| reduction in calories consumption | 72(58.5%) | 143(63%) | 92(58.2%) | 16(57.1%) | 0.191 | |
| more fruits and vegetables consumption | 92(74.8%) | 160(69.6%) | 108(68.4%) | 18(64.3%) | 0.199 | |
| more fishes consumption | 52(42.3%) | 98(43%) | 77(49%) | 13(46.4%) | 0.534 | |
| reduction in sugar consumption | 74(60.7%) a | 137(59.6%) b | 100(63.3%) c | 9(32.1%) a,b,c | 0.034 | |
| reduction in alcohol consumption | 68(56.2%) | 131(57.2%) | 87(55.1%) | 13(46.4%) | 0.584 | |
| compliance with dietary recommendations | 56(45.5%) | 117(51.3%) | 84(53.2%) | 16(57.1%) | 0.787 |
| Reported during Hospitalization n = 452 | IQR | After Hospital Discharge n = 27 | IQR | Newly Diagnosed n = 28 | IQR | p | |
|---|---|---|---|---|---|---|---|
| Sex | 307 (67.9%) | 21 (77.8%) | 21 (75%) | 0.432 | |||
| Age median | 70.0 | 65.0–75.0 | 64.0 | 61.0–74.0 | 70.0 | 66.0–73.0 | 0.053 |
| BMI (kg/m2) median | 30.6 | 27.4–33.5 | 29.4 | 27.4–35.6 | 30.6 | 27.2–30.7 | 0.260 |
| Body weight (kg) median | 86.0 | 77.0–96.5 | 85.9 | 76.6–99.5 | 86.0 | 74.3–90.5 | 0.264 |
| Waist circumference (cm) median | 105.0 | 98.0–113.0 | 103.0 | 99.0–120.0 | 105.0 | 99.0–107.0 | 0.450 |
| Total cholesterol (mg/dL) median | 145.0 | 123.7–177.8 | 143.3 | 123.7–170.0 | 145.0 | 132.5–170.0 | 0.886 |
| LDL (mg/dL) median | 70.6 | 54.1–93.9 | 71.7 | 54.1–83.0 | 70.6 | 56.8–106.1 | 0.468 |
| HDL-C (mg/dL L) median | 46.0 | 38.7–56.8 | 43.0 | 37.0–47.0 | 46.0 | 42.0–54.0 | 0.236 |
| TG (mg/dL) median | 124.9 | 89.0–166.0 | 168 | 93.0–213.3 | 124.9 | 98.8–195.3 | 0.119 |
| HbA1C (%) median | 6.6 | 6.0–7.5 | 6.0 | 5.8–6.8 | 6.6 | 5.7–6.4 | <0.01 |
| Reported during Hospitalization n = 452 | After Hospital Discharge n = 27 | Newly Diagnosed n = 28 | p | ||
|---|---|---|---|---|---|
| Index event n (%) | CABG | 14(3.1%) | 3(11.1%) | 1(3.6%) | 0.030 |
| PCI | 179(39.6%) | 6(22.2%) | 11(39.3%) | ||
| STEMI | 55(12.2%) | 7(25.9) | 7(25%) | ||
| NSTEMI | 114(25.2%) | 7(25.9%) | 2(7.1%) | ||
| Unstable angina | 90(19.9%) | 4(14.8%) | 7(25%) | ||
| lifestyle change n (%) | reduction in salt consumption | 255(72%) | 17(65.4%) | 14(51.9%) | 0.131 |
| reduction in fat consumption | 286(80.6%) a | 17(65.4%) | 14(50%) a | <0.01 | |
| reduction in calories consumption | 234(66.1%) | 16(61.5%) | 16(57.1%) | 0.449 | |
| more fruits and vegetables consumption | 270(76.1%) | 21(80.8%) | 18(64.3%) | 0.556 | |
| more fishes consumption | 165(46.5%) | 9(34.6%) | 13(46.4%) | 0.748 | |
| reduction in sugar consumption | 290(81.7%) b | 17(65.4%) a | 9(32.1%) a,b | <0.01 | |
| reduction in alcohol consumption | 230(65.2%) | 17(65.4%) | 13(46.4%) | 0.378 | |
| compliance with dietary recommendations | 243(68.5%) | 15(57.7%) | 16(57.1%) | 0.162 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drobek, N.; Sowa, P.; Jankowski, P.; Haberka, M.; Gąsior, Z.; Kosior, D.; Czarnecka, D.; Pająk, A.; Szostak-Janiak, K.; Krzykwa, A.; et al. Undiagnosed Diabetes and Prediabetes in Patients with Chronic Coronary Syndromes—An Alarming Public Health Issue. J. Clin. Med. 2021, 10, 1981. https://doi.org/10.3390/jcm10091981
Drobek N, Sowa P, Jankowski P, Haberka M, Gąsior Z, Kosior D, Czarnecka D, Pająk A, Szostak-Janiak K, Krzykwa A, et al. Undiagnosed Diabetes and Prediabetes in Patients with Chronic Coronary Syndromes—An Alarming Public Health Issue. Journal of Clinical Medicine. 2021; 10(9):1981. https://doi.org/10.3390/jcm10091981
Chicago/Turabian StyleDrobek, Natalia, Paweł Sowa, Piotr Jankowski, Maciej Haberka, Zbigniew Gąsior, Dariusz Kosior, Danuta Czarnecka, Andrzej Pająk, Karolina Szostak-Janiak, Agnieszka Krzykwa, and et al. 2021. "Undiagnosed Diabetes and Prediabetes in Patients with Chronic Coronary Syndromes—An Alarming Public Health Issue" Journal of Clinical Medicine 10, no. 9: 1981. https://doi.org/10.3390/jcm10091981
APA StyleDrobek, N., Sowa, P., Jankowski, P., Haberka, M., Gąsior, Z., Kosior, D., Czarnecka, D., Pająk, A., Szostak-Janiak, K., Krzykwa, A., Setny, M., Kozieł, P., Paniczko, M., Jamiołkowski, J., Kowalska, I., & Kamiński, K. (2021). Undiagnosed Diabetes and Prediabetes in Patients with Chronic Coronary Syndromes—An Alarming Public Health Issue. Journal of Clinical Medicine, 10(9), 1981. https://doi.org/10.3390/jcm10091981