
Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland

 ,
,  ,
,  ,
,  , , , ,
, , , ,  , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analyses
3. Results
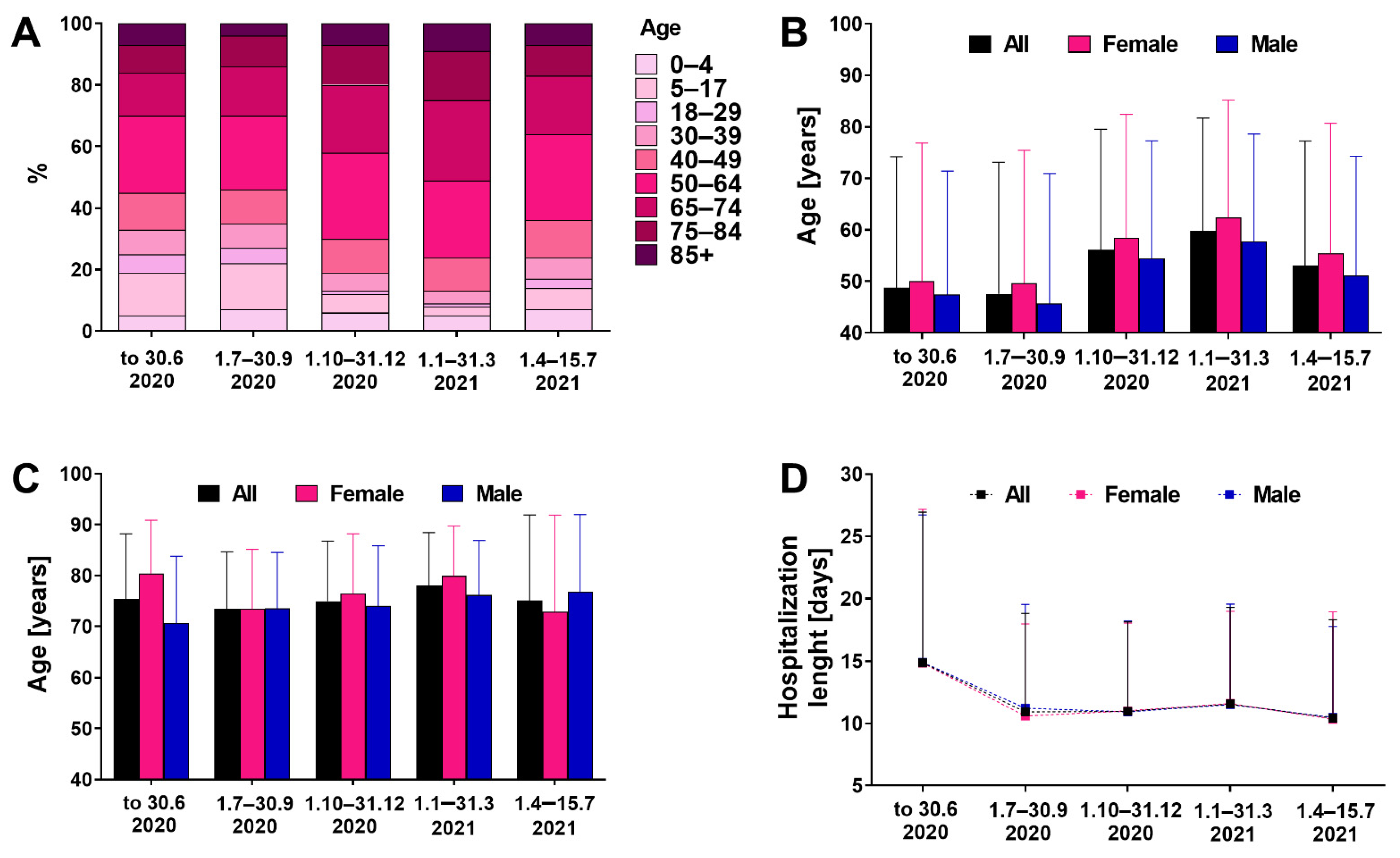
3.1. Demographic Characteristics
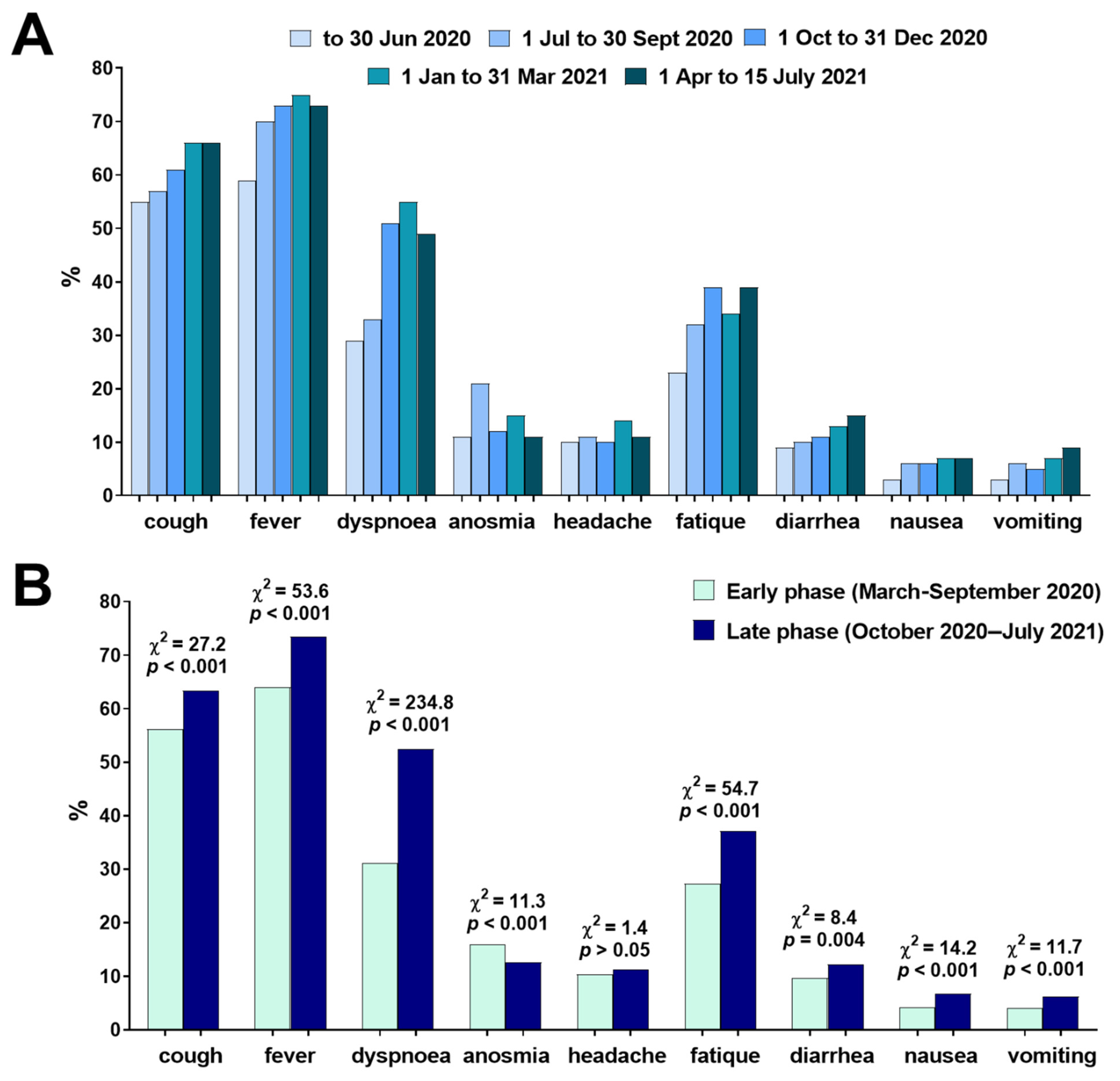
3.2. Early Symptoms of Infection
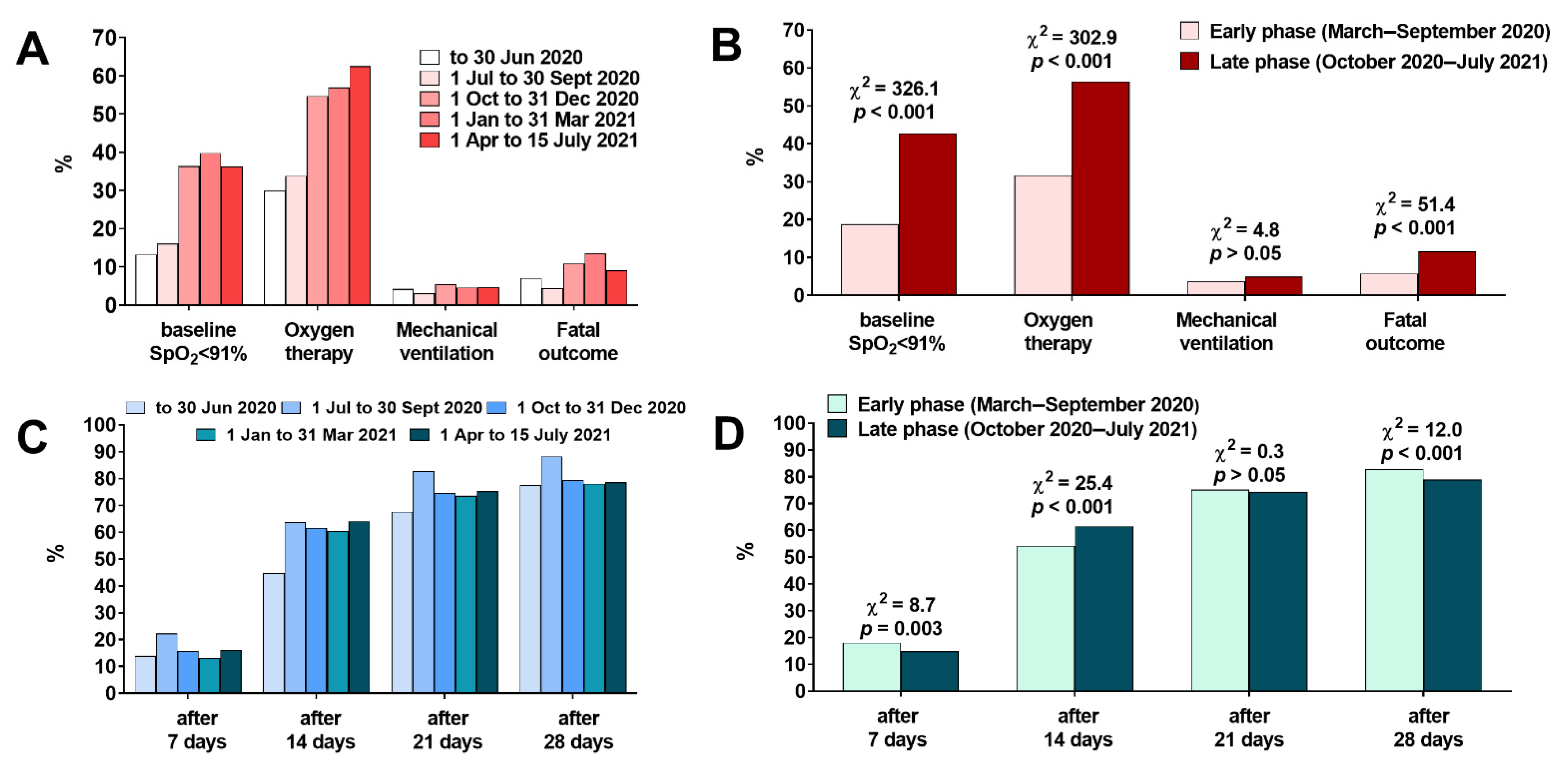
3.3. Laboratory and Clinical Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio-Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Gu, S.X.; Tyagi, T.; Jain, K.; Gu, V.W.; Lee, S.H.; Hwa, J.M.; Kwan, J.M.; Krause, D.S.; Lee, A.I.; Halene, S.; et al. Thrombocytopathy and endotheliopathy: Crucial contributors to COVID-19 thromboinflammation. Nat. Rev. Cardiol. 2021, 18, 194–209. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, P.R.M. Multiple organ dysfunction in SARS-CoV-2: MODS-CoV-2. Expert Rev. Respir. Med. 2020, 14, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Rochman, N.D.; Wolf, Y.I.; Faure, G.; Mutz, P.; Zhang, F.; Koonin, E.V. Ongoing global and regional adaptive evolution of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2021, 118, e2104241118. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Á.; Pongor, S.; Győrffy, B. Different mutations in SARS-CoV-2 associate with severe and mild outcome. Int. J. Antimicrob. Agents 2021, 57, 106272. [Google Scholar] [CrossRef]
- Horspool, A.M.; Ye, C.; Wong, T.Y.; Russ, B.P.; Lee, K.S.; Winters, M.T.; Bevere, J.R.; Kieffer, T.; Martinez, I.; Sourimant, J.; et al. SARS-CoV-2 B.1.1.7 and B.1.351 variants of concern induce lethal disease in K18-hACE2 transgenic mice despite convalescent plasma therapy. bioRxiv 2021. [Google Scholar] [CrossRef]
- Frampton, D.; Rampling, T.; Cross, A.; Bailey, H.; Heaney, J.; Byott, M.; Scott, R.; Sconza, R.; Price, J.; Margaritis, M.; et al. Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage in London, UK: A whole-genome sequencing and hospital-based cohort study. Lancet Infect. Dis. 2021, 21, 1246–1256. [Google Scholar] [CrossRef]
- Graham, M.S.; Sudre, C.H.; May, A.; Antonelli, M.; Murray, B.; Varsavsky, T.; Kläser, K.; Canas, L.S.; Molteni, E.; Modat, M.; et al. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: An ecological study. Lancet Public Health 2021, 6, e335–e345. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 31 March 2020. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists. Annex no. 1 as of 8 June 2020. Pol. Arch. Intern. Med. 2020, 130, 557–558. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Parczewski, M.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists. Annex no. 2 as of 13 October 2020. Pol. Arch. Intern. Med. 2020, 130, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 26 2April 021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef]
- Flisiak, R.; Jaroszewicz, J.; Rogalska, M.; Łapiński, T.; Berkan-Kawińska, A.; Bolewska, B.; Tudrujek-Zdunek, M.; Kozielewicz, D.; Rorat, M.; Leszczyński, P.; et al. Tocilizumab Improves the Prognosis of COVID-19 in Patients with High IL-6. J. Clin. Med. 2021, 10, 1583. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Pazgan-Simon, M.; Simon, K.; Łapiński, T.; Zarębska-Michaluk, D.; Szczepańska, B.; Chojnicki, M.; Mozer-Lisewska, I.; Flisiak, R. Clinical Characteristics of Hospitalized COVID-19 Patients Who Received at Least One Dose of COVID-19 Vaccine. Vaccines 2021, 9, 781. [Google Scholar] [CrossRef] [PubMed]
- Hryhorowicz, S.; Ustaszewski, A.; Kaczmarek-Ryś, M.; Lis, E.; Witt, M.; Pławski, A.; Ziętkiewicz, E. European context of the diversity and phylogenetic position of SARS-CoV-2 sequences from Polish COVID-19 patients. J. Appl. Genet. 2021, 62, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Volz, E.; Hill, V.; McCrone, J.T.; Price, A.; Jorgensen, D.; O’Toole, Á.; Southgate, J.; Johnson, R.; Jackson, B.; Nascimento, F.F.; et al. Evaluating the Effects of SARS-CoV-2 Spike Mutation D614G on Transmissibility and Pathogenicity. Cell 2021, 184, 64–75. [Google Scholar] [CrossRef]
- Hou, Y.J.; Chiba, S.; Halfmann, P.; Ehre, C.; Kuroda, M.; Dinnon, K.H., 3rd; Leist, S.R.; Schäfer, A.; Nakajima, N.; Takahashi, K.; et al. SARS-CoV-2 D614G variant exhibits efficient replication ex vivo and transmission in vivo. Science 2020, 370, 1464–1468. [Google Scholar] [CrossRef]
- Davies, N.G.; Jarvis, C.I.; van Zandvoort, K.; Clifford, S.; Sun, F.Y.; Funk, S.; Medley, G.; Jafari, Y.; Meakin, S.R.; Lowe, R.; et al. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature 2021, 593, 270–274. [Google Scholar] [CrossRef]
- Brookman, S.; Cook, J.; Zucherman, M.; Broughton, S.; Harman, K.; Gupta, A. Effect of the new SARS-CoV-2 variant B.1.1.7 on children and young people. Lancet Child Adolesc Health 2021, 5, e9–e10. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Ghimire, S.; Sharma, S.; Patel, A.; Budhathoki, R.; Chakinala, R.; Khan, H.; Lincoln, M.; Georgeston, M. Diarrhea Is Associated with Increased Severity of Disease in COVID-19: Systemic Review and Metaanalysis. SN Compr. Clin. Med. 2021, 3, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Talavera, B.; García-Azorín, D.; Martínez-Pías, E.; Trigo, J.; Hernández-Pérez, I.; Valle-Peñacoba, G.; Simón-Campo, P.; de Lera, M.; Chavarría-Miranda, A.; López-Sanz, C.; et al. Anosmia is associated with lower in-hospital mortality in COVID-19. J. Neurol. Sci. 2020, 419, 117163. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.J.; Jauregui, E.; Tajudeen, B.; Bishehsari, F.; Mahdavinia, M. Smell loss is a prognostic factor for lower severity of coronavirus disease 2019. Ann. Allergy Asthma Immunol. 2020, 125, 481–483. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 5199) | Female (n = 2376) | Male (n = 2823) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD (min–max) | 53.4 ± 24.5 (0–100) | 55.3 ± 25.4 (0–100) | 51.9 ± 23.6 (0–97) | p < 0.001 |
| BMI (kg/m2), mean ± SD (min–max) | 26.7 ± 6.4 (7.4–58.8) | 26.1 ± 6.6 (7.4–56.9) | 27.1 ± 6.3 (9.6–58.8) | p < 0.001 |
| Obese adults, % (n) | 23.2 (1207) | 22.4 (532) | 23.9 (675) | p > 0.05 |
| Comorbidities, % (n) | 67.0 (3481) | 68.6 (1629) | 65.6 (1852) | p = 0.02 |
| Need for oxygenation, % (n) | 44.9 (2333) | 40.1 (952) | 48.9 (1381) | p < 0.001 |
| Need for mechanical ventilation, % (n) | 4.5 (233) | 3.5 (84) | 5.3 (149) | p = 0.003 |
| Time of hospitalization (days), mean ± SD | 11.9 ± 8.9 | 11.9 ± 9.0 | 11.9 ± 8.8 | p > 0.05 |
| Fatality, % (n) | 9.2 (479) | 8.8 (208) | 9.6 (271) | p > 0.05 |
| Age of patients who died (years), mean ± SD (min–max) | 75.9 ± 12.0 | 77.9 ± 11.7 | 74.3 ± 12.0 | p < 0.001 |
| Symptom | Outcome | All (n = 5199) | Female (n = 2376) | Male (n = 2823) |
|---|---|---|---|---|
| Cough | Oxygen therapy | 2.0 (1.7–2.2) p < 0.001 | 1.8 (1.5–2.1) p < 0.001 | 2.1 (1.8–2.4) p < 0.001 |
| Mechanical ventilation | 1.9 (1.4–2.5) p < 0.001 | 2.2 (1.3–3.5) p = 0.003 | 1.0 (0.8–1.4) p > 0.05 | |
| Death | 0.8 (0.6–0.9) p = 0.01 | 0.8 (0.6–1.1) p > 0.05 | 0.7 (0.6–1.0) p = 0.02 | |
| Dyspnea | Oxygen therapy | 6.3 (5.6–7.2) p < 0.001 | 5.3 (4.7–6.4) p < 0.001 | 7.2 (6.1–8.5) p < 0.001 |
| Mechanical ventilation | 6.0 (4.3–8.3) p < 0.001 | 7.9 (4.4–14.1) p < 0.001 | 4.9 (3.3–7.4) p < 0.001 | |
| Death | 3.7 (3.0–4.5) p < 0.001 | 3.5 (2.6–4.7) p < 0.001 | 3.8 (2.9–5.1) p < 0.001 | |
| Fever | Oxygen therapy | 2.0 (1.7–2.3) p < 0.001 | 1.7 (1.4–2.0) p < 0.001 | 2.2 (1.9–2.6) p < 0.001 |
| Mechanical ventilation | 2.2 (1.6–3.2) p < 0.001 | 1.6 (1.0–2.6) p > 0.05 | 2.8 (1.7–4.7) p < 0.001 | |
| Death | 0.9 (0.7–1.1) p > 0.05 | 0.8 (0.6–1.1) p > 0.05 | 0.9 (0.7–1.2) p > 0.05 | |
| Anosmia | Oxygen therapy | 0.8 (0.7–0.9) p = 0.003 | 0.7 (0.6–0.9) p = 0.005 | 0.9 (0.7–1.1) p > 0.05 |
| Mechanical ventilation | 0.7 (0.5–1.1) p > 0.05 | 0.5 (0.2–1.1) p > 0.05 | 0.9 (0.5–1.5) p > 0.05 | |
| Death | 0.4 (0.3–0.6) p < 0.001 | 0.3 (0.2–0.6) p < 0.001 | 0.5 (0.3–0.8) p = 0.004 | |
| Headache | Oxygen therapy | 0.7 (0.6–0.9) p = 0.003 | 0.6 (0.4–0.8) p < 0.001 | 0.9 (0.7–1.2) p > 0.05 |
| Mechanical ventilation | 1.1 (0.7–1.6) p > 0.05 | 0.6 (0.3–1.4) p > 0.05 | 1.5 (0.9–2.5) p > 0.05 | |
| Death | 0.7 (0.5–1.0) p > 0.05 | 0.7 (0.4–1.2) p > 0.05 | 0.7 (0.4–1.1) p > 0.05 | |
| Fatigue | Oxygen therapy | 1.6 (1.5–1.8) p < 0.001 | 1.4 (1.2–1.7) p < 0.001 | 1.9 (1.6–2.2) p < 0.001 |
| Mechanical ventilation | 1.4 (1.1–1.8) p = 0.02 | 1.2 (0.7–1.8) p > 0.05 | 1.6 (1.1–2.2) p = 0.007 | |
| Death | 1.2 (0.9–1.5) p > 0.05 | 1.0 (0.8–1.4) p > 0.05 | 1.1 (0.7–2.0) p > 0.05 | |
| Diarrhea | Oxygen therapy | 1.1 (0.9–1.3) p > 0.05 | 1.2 (0.9–1.5) p > 0.05 | 1.1 (0.9–1.5) p > 0.05 |
| Mechanical ventilation | 1.1 (0.7–1.6) p > 0.05 | 1.0 (0.5–1.9) p > 0.05 | 1.1 (0.7–1.9) p > 0.05 | |
| Death | 1.1 (0.8–1.5) p > 0.05 | 1.0 (0.7–1.5) p > 0.05 | 1.2 (0.8–1.8) p > 0.05 | |
| Nausea | Oxygen therapy | 1.0 (0.8–1.2) p > 0.05 | 1.0 (0.7–1.4) p > 0.05 | 1.0 (0.7–1.5) p > 0.05 |
| Mechanical ventilation | 0.8 (0.4–1.5) p > 0.05 | 0.7 (0.2–1.8) p > 0.05 | 0.9 (0.4–2.2) p > 0.05 | |
| Death | 0.8 (0.5–1.3) p > 0.05 | 1.0 (0.6–1.8) p > 0.05 | 0.6 (0.3–1.2) p > 0.05 | |
| Vomiting | Oxygen therapy | 0.9 (0.7–1.2) p > 0.05 | 1.0 (0.7–1.4) p > 0.05 | 0.9 (0.6–1.6) p > 0.05 |
| Mechanical ventilation | 0.7 (0.4–1.4) p > 0.05 | 0.8 (0.3–2.0) p > 0.05 | 0.7 (0.3–2.0) p > 0.05 | |
| Death | 0.8 (0.5–1.2) p > 0.05 | 0.8 (0.4–1.4) p > 0.05 | 0.8 (0.4–1.7) p > 0.05 |
| All (n = 5199) | Female (n = 2376) | Male (n = 2823) | p-Value | Early Phase (n = 2145) | Late Phase (n = 3054) | p-Value | |
|---|---|---|---|---|---|---|---|
| CRP, mg/L | 70.2 ± 76.1 | 57.0 ± 68.9 | 81.3 ± 80.2 | <0.001 | 50.4 ± 68.0 | 83.8 ± 78.5 | <0.001 |
| PCT, ng/mL | 0.5 ± 3.5 | 0.4 ± 2.9 | 0.6 ± 3.9 | >0.05 | 0.5 ± 4.7 | 0.5 ± 2.6 | >0.05 |
| IL-6, pg/mL | 67.7 ± 175.2 | 58.9 ± 200.3 | 75.2 ± 150.3 | <0.001 | 44.5 ± 150.1 | 80.1 ± 186.1 | <0.001 |
| d-dimer, ng/mL | 1964.0 ± 6153.7 | 1865.5 ± 5309.3 | 2046.4 ± 6779.5 | >0.05 | 1331.6 ± 4345.1 | 2361.7 ± 7029.2 | <0.001 |
| ALT, IU/L | 40.6 ± 56.2 | 34.0 ± 50.1 | 46.2 ± 60.3 | <0.001 | 34.9 ± 54.6 | 44.6 ± 56.9 | <0.001 |
| WBC, ×103/µL | 7.0 ± 4.4 | 6.7 ± 3.8 | 7.2 ± 4.7 | <0.001 | 6.6 ± 4.2 | 7.3 ± 4.4 | <0.001 |
| Lymphocytes, ×103/µL | 1.4 ± 1.8 | 1.5 ± 1.4 | 1.4 ± 2.0 | >0.05 | 1.6 ± 2.0 | 1.4 ± 1.6 | <0.001 |
| Neutrophils, ×103/µL | 4.9 ± 3.7 | 4.6 ± 3.2 | 5.1 ± 4.2 | <0.001 | 4.2 ± 2.8 | 5.3 ± 4.2 | <0.001 |
| Platelets, ×103/µL | 227.2 ± 102.4 | 235.2 ± 98.7 | 220.5 ± 104.9 | 0.003 | 231.3 ± 98.0 | 224.8 ± 105.2 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flisiak, R.; Rzymski, P.; Zarębska-Michaluk, D.; Rogalska, M.; Rorat, M.; Czupryna, P.; Lorenc, B.; Ciechanowski, P.; Kozielewicz, D.; Piekarska, A.; et al. Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland. J. Clin. Med. 2022, 11, 117. https://doi.org/10.3390/jcm11010117
Flisiak R, Rzymski P, Zarębska-Michaluk D, Rogalska M, Rorat M, Czupryna P, Lorenc B, Ciechanowski P, Kozielewicz D, Piekarska A, et al. Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland. Journal of Clinical Medicine. 2022; 11(1):117. https://doi.org/10.3390/jcm11010117
Chicago/Turabian StyleFlisiak, Robert, Piotr Rzymski, Dorota Zarębska-Michaluk, Magdalena Rogalska, Marta Rorat, Piotr Czupryna, Beata Lorenc, Przemysław Ciechanowski, Dorota Kozielewicz, Anna Piekarska, and et al. 2022. "Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland" Journal of Clinical Medicine 11, no. 1: 117. https://doi.org/10.3390/jcm11010117
APA StyleFlisiak, R., Rzymski, P., Zarębska-Michaluk, D., Rogalska, M., Rorat, M., Czupryna, P., Lorenc, B., Ciechanowski, P., Kozielewicz, D., Piekarska, A., Pokorska-Śpiewak, M., Sikorska, K., Tudrujek, M., Bolewska, B., Angielski, G., Kowalska, J., Podlasin, R., Mazur, W., Oczko-Grzesik, B., ... Grabowski, H. (2022). Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland. Journal of Clinical Medicine, 11(1), 117. https://doi.org/10.3390/jcm11010117