
Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors: A Randomised, Single-Blind, Controlled Trial with a 6-Month Follow-Up

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Sample Size Estimation
2.4. Randomisation and Blinding
2.5. Assessment and Data Collection
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Interventions
2.7. Data Analysis
3. Results
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doong, S.H.; Dhruva, A.; Dunn, L.B.; West, C.; Paul, S.M.; Cooper, B.A.; Elboim, C.; Abrams, G.; Merriman, J.D.; Langford, D.J.; et al. Associations between cytokine genes and a symptom cluster of pain, fatigue, sleep disturbance, and depression in patients prior to breast cancer surgery. Biol. Res. Nurs. 2015, 17, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Thong, M.S.Y.; van Noorden, C.J.F.; Steindorf, K.; Arndt, V. Cancer-Related Fatigue: Causes and Current Treatment Options. Curr. Treat. Options Oncol. 2020, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Arndt, V.; Stegmaier, C.; Ziegler, H.; Brenner, H. A population-based study of the impact of specific symptoms on quality of life in women with breast cancer 1 year after diagnosis. Cancer 2006, 107, 2496–2503. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.K.; Lee, D.T. Effects of pain, fatigue, insomnia, and mood disturbance on functional status and quality of life of elderly patients with cancer. Crit. Rev. Oncol./Hematol. 2011, 78, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Mustian, K.M.; Alfano, C.M.; Heckler, C.; Kleckner, A.S.; Kleckner, I.R.; Leach, C.R.; Mohr, D.; Palesh, O.G.; Peppone, L.J.; Piper, B.F.; et al. Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue: A Meta-analysis. JAMA Oncol. 2017, 3, 961–968. [Google Scholar] [CrossRef] [PubMed]
- O’Higgins, C.M.; Brady, B.; O’Connor, B.; Walsh, D.; Reilly, R.B. The pathophysiology of cancer-related fatigue: Current controversies. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2018, 26, 3353–3364. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: A meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E. Management of cancer-related fatigue. Clin. Adv. Hematol. Oncol. H&O 2006, 4, 828–829. [Google Scholar]
- Campos, M.P.O.; Hassan, B.J.; Riechelmann, R.; Del Giglio, A. Cancer-related fatigue: A practical review. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- del-Rosal-Jurado, A.; Romero-Galisteo, R.; Trinidad-Fernández, M.; González-Sánchez, M.; Cuesta-Vargas, A.; Ruiz-Muñoz, M. Therapeutic Physical Exercise Post-Treatment in Breast Cancer: A Systematic Review of Clinical Practice Guidelines. J. Clin. Med. 2020, 9, 1239. [Google Scholar] [CrossRef]
- Jiang, M.; Ma, Y.; Yun, B.; Wang, Q.; Huang, C.; Han, L. Exercise for fatigue in breast cancer patients: An umbrella review of systematic reviews. Int. J. Nurs. Sci. 2020, 7, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2015, 15, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Supervised exercise reduces cancer-related fatigue: A systematic review. J. Physiother. 2015, 61, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; American College of Sports Medicine: Indianapolis, IN, USA, 2018.
- Pollán, M.; Casla-Barrio, S.; Alfaro, J.; Esteban, C.; Segui-Palmer, M.A.; Lucia, A.; Martín, M. Exercise and cancer: A position statement from the Spanish Society of Medical Oncology. Clin Transl Oncol 2020, 22, 1710–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for enhancing adherence with physiotherapy: A systematic review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spathis, A.; Hatcher, H.; Booth, S.; Gibson, F.; Stone, P.; Abbas, L.; Barclay, M.; Brimicombe, J.; Thiemann, P.; McCabe, M.G.; et al. Cancer-Related Fatigue in Adolescents and Young Adults After Cancer Treatment: Persistent and Poorly Managed. J. Adolesc. Young Adult Oncol. 2017, 6, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Paul van Wilgen, C.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Cella, D.; Peterman, A.; Passik, S.; Jacobsen, P.; Breitbart, W. Progress toward guidelines for the management of fatigue. Oncology 1998, 12, 369–377. [Google Scholar]
- Cella, D.; Hernandez, L.; Bonomi, A.E.; Corona, M.; Vaquero, M.; Shiomoto, G.; Baez, L. Spanish language translation and initial validation of the functional assessment of cancer therapy quality-of-life instrument. Med. Care 1998, 36, 1407–1418. [Google Scholar] [CrossRef]
- Dapueto, J.J.; del Carmen Abreu, M.; Francolino, C.; Levin, R. Psychometric Assessment of the MSAS-SF and the FACIT-Fatigue Scale in Spanish-Speaking Patients With Cancer in Uruguay. J. Pain Symptom Manag. 2014, 47, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Nordin, Å.; Taft, C.; Lundgren-Nilsson, Å.; Dencker, A. Minimal important differences for fatigue patient reported outcome measures-a systematic review. BMC Med. Res. Methodol. 2016, 16, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.P.; Wang, W.; Potts, S.L.; Gould, E.M. Reliability and validity of individual and composite recall pain measures in patients with cancer. Pain Med. 2012, 13, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Harrington, S.; Gilchrist, L.; Sander, A. Breast Cancer EDGE Task Force Outcomes: Clinical Measures of Pain. Rehabil. Oncol. (Am. Phys. Ther. Assoc. Oncol. Sect.) 2014, 32, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, K.; Vogt, L.; Thiel, C.; Jäger, E.; Banzer, W. Validity of the six-minute walk test in cancer patients. Int. J. Sports Med. 2013, 34, 631–636. [Google Scholar] [CrossRef]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, B.; Arranz-Martín, B.; Navarro-Brazález, B.; Vergara-Pérez, F.; Bailón-Cerezo, J.; Torres-Lacomba, M. How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders. Int. J. Environ. Res. Public Health 2021, 18, 2377. [Google Scholar] [CrossRef]
- Torres-Lacomba, M.; Navarro-Brazález, B.; Bailón-Cerezo, J.; Vergara-Pérez, F.; de la Rosa-Díaz, I.; Prieto-Gómez, V. Assessment Tools of Patient Competences: The Spanish Version of the R-NPQ and Three Practical Cases in Women with Breast Cancer and Persistent Pain. Int. J. Environ. Res. Public Health 2021, 18, 4463. [Google Scholar] [CrossRef]
- Position Stand. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Domaszewska, K.; Pienkowski, T.; Janiak, A.; Bukowska, D.; Laurentowska, M. The Influence of Soft Tissue Therapy on Respiratory Efficiency and Chest Mobility of Women Suffering from Breast Cancer. Int. J. Environ. Res. Public Health 2019, 16, 5092. [Google Scholar] [CrossRef] [Green Version]
- Vieira, D.S.R.; Mendes, L.P.S.; Elmiro, N.S.; Velloso, M.; Britto, R.R.; Parreira, V.F. Breathing exercises: Influence on breathing patterns and thoracoabdominal motion in healthy subjects. Braz. J. Phys. Ther. 2014, 18, 544–552. [Google Scholar] [CrossRef] [Green Version]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K.; Brosseau, L.; Costa, L.; Cramp, F.; Cup, E.; et al. Consensus on Exercise Reporting Template (CERT): Modified Delphi Study. Phys. Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef]
- Aboagye, E.; Hagberg, J.; Axén, I.; Kwak, L.; Lohela-Karlsson, M.; Skillgate, E.; Dahlgren, G.; Jensen, I. Individual preferences for physical exercise as secondary prevention for non-specific low back pain: A discrete choice experiment. PLoS ONE 2017, 12, e0187709. [Google Scholar] [CrossRef] [Green Version]
- Collado-Mateo, D.; Lavín-Pérez, A.M.; Peñacoba, C.; Del Coso, J.; Leyton-Román, M.; Luque-Casado, A.; Gasque, P.; Fernández-del-Olmo, M.Á.; Amado-Alonso, D. Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 2023. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Lai, J.S.; Chang, C.H.; Peterman, A.; Slavin, M. Fatigue in cancer patients compared with fatigue in the general United States population. Cancer 2002, 94, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Montan, I.; Löwe, B.; Cella, D.; Mehnert, A.; Hinz, A. General Population Norms for the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue Scale. Value Health J. Int. Soc. Pharm. Outcomes Res. 2018, 21, 1313–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- But-Hadzic, J.; Dervisevic, M.; Karpljuk, D.; Videmsek, M.; Dervisevic, E.; Paravlic, A.; Hadzic, V.; Tomazin, K. Six-Minute Walk Distance in Breast Cancer Survivors—A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2591. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, J.L.; Byers, T.; DiGuiseppi, C.; Dabelea, D.; Denberg, T.D. Cardiovascular disease competes with breast cancer as the leading cause of death for older females diagnosed with breast cancer: A retrospective cohort study. Breast Cancer Res 2011, 13, R64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.M.; Murthy, J.N.; Wollak, I.D.; Jackson, A.S. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm. Med. 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlSaeed, E.F.; Balaraj, F.K.; Tunio, M.A. Changes in pulmonary function tests in breast carcinoma patients treated with locoregional post-mastectomy radiotherapy: Results of a pilot study. Breast Cancer 2017, 9, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.H.; Hsieh, C.C.; Chang, C.S.; Chen, M.F. A Retrospective Analysis of Dose Distribution and Toxicity in Patients with Left Breast Cancer Treated with Adjuvant Intensity-Modulated Radiotherapy: Comparison with Three-Dimensional Conformal Radiotherapy. Cancer Manag. Res. 2020, 12, 9173–9182. [Google Scholar] [CrossRef]
- Anzic, M.; Marinko, T. Effect of Adjuvant Hormonal Therapy on the Development of Pulmonary Fibrosis after Postoperative Radiotherapy for Breast Cancer. J. Breast Cancer 2020, 23, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Suesada, M.M.; Carvalho, H.A.; Albuquerque, A.L.P.; Salge, J.M.; Stuart, S.R.; Takagaki, T.Y. Impact of thoracic radiotherapy on respiratory function and exercise capacity in patients with breast cancer. J. Bras. Pneumol. Publicacao Off. Soc. Bras. Pneumol. Tisilogia 2018, 44, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Juhl, A.A.; Christiansen, P.; Damsgaard, T.E. Persistent Pain after Breast Cancer Treatment: A Questionnaire-Based Study on the Prevalence, Associated Treatment Variables, and Pain Type. J. Breast Cancer 2016, 19, 47–454. [Google Scholar] [CrossRef] [Green Version]
- Andersen, K.G.; Kehlet, H. Persistent pain after breast cancer treatment: A critical review of risk factors and strategies for prevention. J. Pain 2011, 12, 725–746. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 2011, 63 (Suppl. 11), S240–S252. [Google Scholar]
- Vaegter, H.B.; Handberg, G.; Graven-Nielsen, T. Similarities between exercise-induced hypoalgesia and conditioned pain modulation in humans. Pain 2014, 155, 158–167. [Google Scholar] [CrossRef]
- O’Leary, S.; Falla, D.; Hodges, P.W.; Jull, G.; Vicenzino, B. Specific therapeutic exercise of the neck induces immediate local hypoalgesia. J. Pain 2007, 8, 832–839. [Google Scholar] [CrossRef]
- Koltyn, K.F.; Brellenthin, A.G.; Cook, D.B.; Sehgal, N.; Hillard, C. Mechanisms of exercise-induced hypoalgesia. J. Pain 2014, 15, 1294–1304. [Google Scholar] [CrossRef] [Green Version]
- Dong, L.; Lee, J.Y.; Harvey, A.G. Do improved patient recall and the provision of memory support enhance treatment adherence? J. Behav. Ther. Exp. Psychiatry 2017, 54, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Baumann, F.T.; Reike, A.; Reimer, V.; Schumann, M.; Hallek, M.; Taaffe, D.R.; Newton, R.U.; Galvao, D.A. Effects of physical exercise on breast cancer-related secondary lymphedema: A systematic review. Breast Cancer Res. Treat. 2018, 170, 1–13. [Google Scholar] [CrossRef]
- Naghibi, S.; Varshouei Tabrizi, F. Exercise Training and Breast Cancer-Related Lymphedema: A Systematic Review. Razavi Int. J. Med. 2018, 6, e11967. [Google Scholar] [CrossRef]
- Olsson Möller, U.; Beck, I.; Rydén, L.; Malmström, M. A comprehensive approach to rehabilitation interventions following breast cancer treatment—A systematic review of systematic reviews. BMC Cancer 2019, 19, 472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tendero-Ruiz, L.; Palomo-Carrión, R.; Megía-García-Carpintero, Á.; Pérez-Nombela, S.; López-Muñoz, P.; Bravo-Esteban, E. The effect of therapeutic exercise in the prevention of lymphoedema secondary to breast cancer: A systematic review. Arch. Med. Sci. 2020, 16. [Google Scholar] [CrossRef]
- Donovan, K.A.; Boyington, A.R.; Ismail-Khan, R.; Wyman, J.F. Urinary symptoms in breast cancer: A systematic review. Cancer 2012, 118, 582–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Córdoba-de Juan, C.; Arranz-Martín, B.; Torres-Lacomba, M. Disfunción sexual en mujeres diagnosticadas y tratadas de cáncer de mama. Estudio descriptivo longitudinal. Fisioterapia 2019, 41, 73–82. [Google Scholar] [CrossRef]
- Stabile, C.; Goldfarb, S.; Baser, R.E.; Goldfrank, D.J.; Abu-Rustum, N.R.; Barakat, R.R.; Dickler, M.N.; Carter, J. Sexual health needs and educational intervention preferences for women with cancer. Breast Cancer Res. Treat. 2017, 165, 77–84. [Google Scholar] [CrossRef]
- Bø, K.; Mørkved, S.; Frawley, H.; Sherburn, M. Evidence for benefit of transversus abdominis training alone or in combination with pelvic floor muscle training to treat female urinary incontinence: A systematic review. Neurourol. Urodyn. 2009, 28, 368–373. [Google Scholar] [CrossRef]
- Danforth, K.N.; Townsend, M.K.; Lifford, K.; Curhan, G.C.; Resnick, N.M.; Grodstein, F. Risk factors for urinary incontinence among middle-aged women. Am. J. Obstet. Gynecol. 2006, 194, 339–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | STE Group (n = 40) | UE Group (n = 40) | Total Sample (n = 80) | p-Value |
|---|---|---|---|---|
| Age years, Median (IQI) | 53.5 (58.8–47.0) | 54.5 (63.0–48.5) | 54.0 (62.0–47.3) | 0.846 |
| Education level, frequency (%) | ||||
| Basic | 1 (2.5) | 0 (0) | 1 (1.3) | 0.626 |
| Primary education | 13 (32.5) | 11 (27.5) | 24 (30.0) | |
| Secondary education | 16 (40.0) | 16 (40.0) | 32 (40.0) | |
| Pre-university | 5 (12.5) | 9 (22.5) | 14 (17.5) | |
| University or HNUE | 5 (12.5) | 4 (10.0) | 9 (11.3) | |
| Currently employed, frequency (%) | 16 (40.0) | 18 (45.0) | 34 (42.5) | 0.821 |
| Surgical procedure, frequency (%) | ||||
| Mastectomy | 0 (0) | 1 (2.5) | 1 (1.3) | 0.542 |
| Quadrantectomy | 11 (27.5) | 5 (12.5) | 16 (20) | |
| Tumorectomy | 29 (72.5) | 34 (85) | 63 (78.8) | |
| Axillary dissection procedure frequency (%) | ||||
| ALND | 38 (95) | 40 (100) | 78 (97.5) | 0.473 |
| SLNB | 2 (5) | 0 (0) | 2 (2.5) | 0.472 |
| Postoperative complications frequency (%) | ||||
| Seroma | 0 (0) | 1 (2.5) | 1 (1.3) | 0.999 |
| SLT | 37 (92.5) | 33 (82.5) | 70 (87.5) | 0.310 |
| Lymphedema | 4 (10) | 2 (5) | 6 (7.5) | 0.671 |
| Postoperative therapy frequency (%) | ||||
| Radiotherapy | 40 (100) | 40 (100) | 80 (100) | |
| Chemotherapy | 38 (95) | 40 (100) | 78 (97.5) | 0.473 |
| Hormonal therapy | 32 (80) | 26 (65) | 58 (72.5) | 0.210 |
| Time (months) since treatment, Median (IQI) | 9 (5) | 7.5 (3.75) | 8 (5) | 0.110 |
| VAS (mm), (SD) | 5.60 (1.6) | 5.55 (1.5) | 5.57 (1.5) | 0.885 |
| 6MWD (m), (SD) | 349.50 (114.1) | 304.5 (113.2) | 327 (115.1) | 0.080 |
| FACIT-F, (SD) | 7.03 (1.7) | 6.33 (1.9) | 6.63 (1.8) | 0.086 |
| Supervised Therapeutic Exercise Group | Unsupervised Exercise Group | Supervised Therapeutic Exercise Group vs. Unsupervised Exercise Group | ||||
|---|---|---|---|---|---|---|
| Outcome | Mean Difference | 95%CI | Mean Difference | 95%CI | p-Value | |
| VAS (mm) | V1 | −2.05 | −2.58 to −1.51 | −1.62 | −2.16 to −1.08 | 0.258 |
| VAS (mm) | V2 | −2.50 | −3.04 to −1.95 | −2.73 | −3.23 to −2.21 | 0.543 |
| VAS (mm) | V3 | −3.08 | −3.54 to −2.60 | −3.72 | −3.72 to −2.72 | 0.661 |
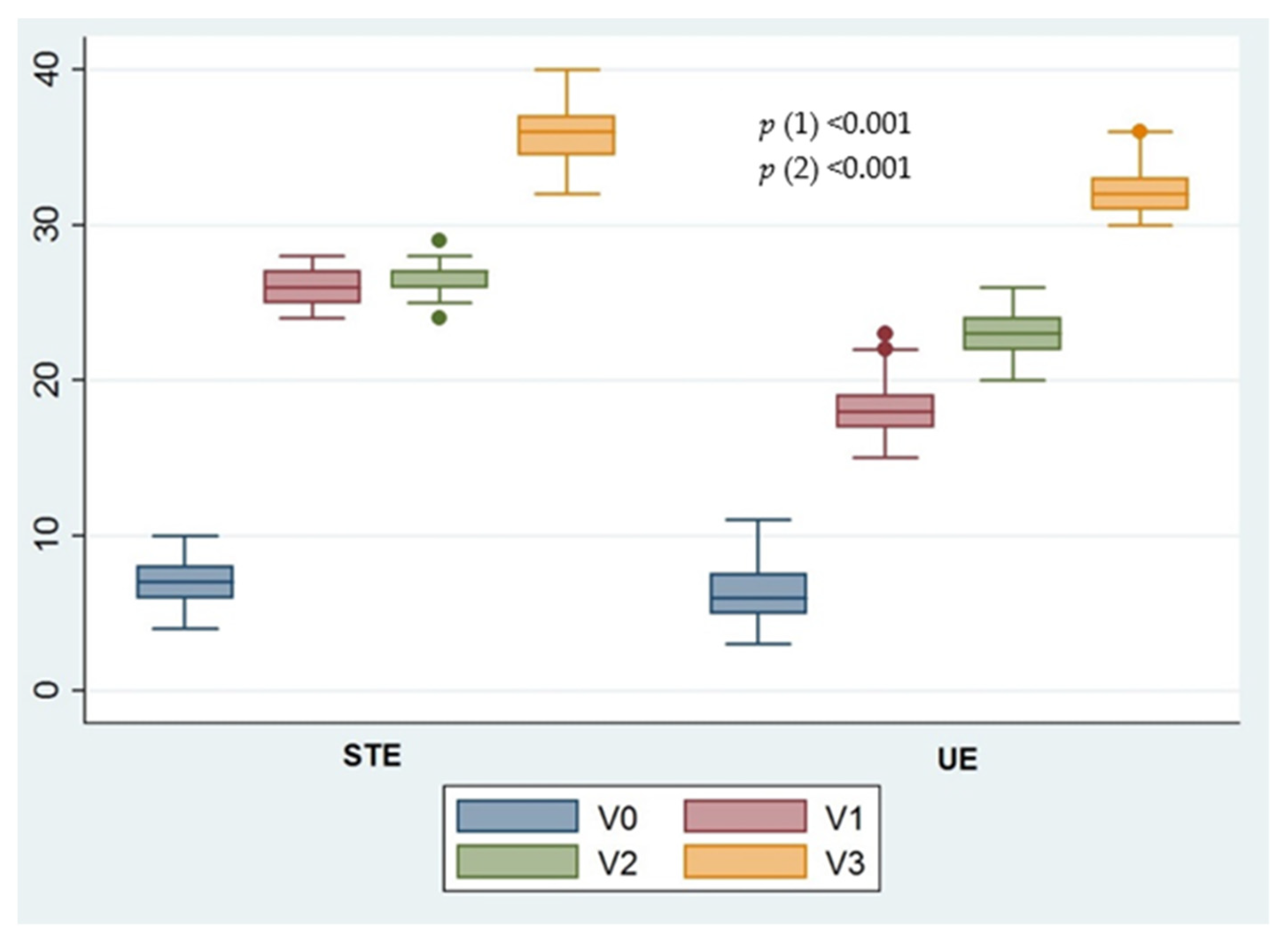
| FACIT-F | V1 | 19.17 | 18.68 to 19.67 | 11.92 | 11.10 to 12.74 | <0.001 |
| FACIT-F | V2 | 19.70 | 19.20 to 20.19 | 17.10 | 16.33 to 17.86 | <0.001 |
| FACIT-F | V3 | 28.77 | 27.94 to 29.60 | 26.10 | 25.17 to 27.02 | <0.001 |
| 6MWD (m) | V1 | 207.37 | 190.37 to 224.37 | 132.37 | 119.03 to 145.72 | <0.001 |
| 6MWD (m) | V2 | 288.00 | 265.10 to 310.89 | 186.37 | 163.23 to 209.51 | <0.001 |
| 6MWD (m) | V3 | 306.75 | 275.35 to 338.14 | 200.25 | 172.69 to 227.31 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prieto-Gómez, V.; Yuste-Sánchez, M.J.; Bailón-Cerezo, J.; Romay-Barrero, H.; de la Rosa-Díaz, I.; Lirio-Romero, C.; Torres-Lacomba, M. Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors: A Randomised, Single-Blind, Controlled Trial with a 6-Month Follow-Up. J. Clin. Med. 2022, 11, 269. https://doi.org/10.3390/jcm11010269
Prieto-Gómez V, Yuste-Sánchez MJ, Bailón-Cerezo J, Romay-Barrero H, de la Rosa-Díaz I, Lirio-Romero C, Torres-Lacomba M. Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors: A Randomised, Single-Blind, Controlled Trial with a 6-Month Follow-Up. Journal of Clinical Medicine. 2022; 11(1):269. https://doi.org/10.3390/jcm11010269
Chicago/Turabian StylePrieto-Gómez, Virginia, María José Yuste-Sánchez, Javier Bailón-Cerezo, Helena Romay-Barrero, Irene de la Rosa-Díaz, Cristina Lirio-Romero, and María Torres-Lacomba. 2022. "Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors: A Randomised, Single-Blind, Controlled Trial with a 6-Month Follow-Up" Journal of Clinical Medicine 11, no. 1: 269. https://doi.org/10.3390/jcm11010269
APA StylePrieto-Gómez, V., Yuste-Sánchez, M. J., Bailón-Cerezo, J., Romay-Barrero, H., de la Rosa-Díaz, I., Lirio-Romero, C., & Torres-Lacomba, M. (2022). Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors: A Randomised, Single-Blind, Controlled Trial with a 6-Month Follow-Up. Journal of Clinical Medicine, 11(1), 269. https://doi.org/10.3390/jcm11010269