
A Limited Course of Eculizumab in a Child with the Atypical Hemolytic Uremic Syndrome and Pre-B Acute Lymphoblastic Leukemia on Maintenance Therapy: Case Report and Literature Review

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
3. Treatment
4. Discussion and Conclusions
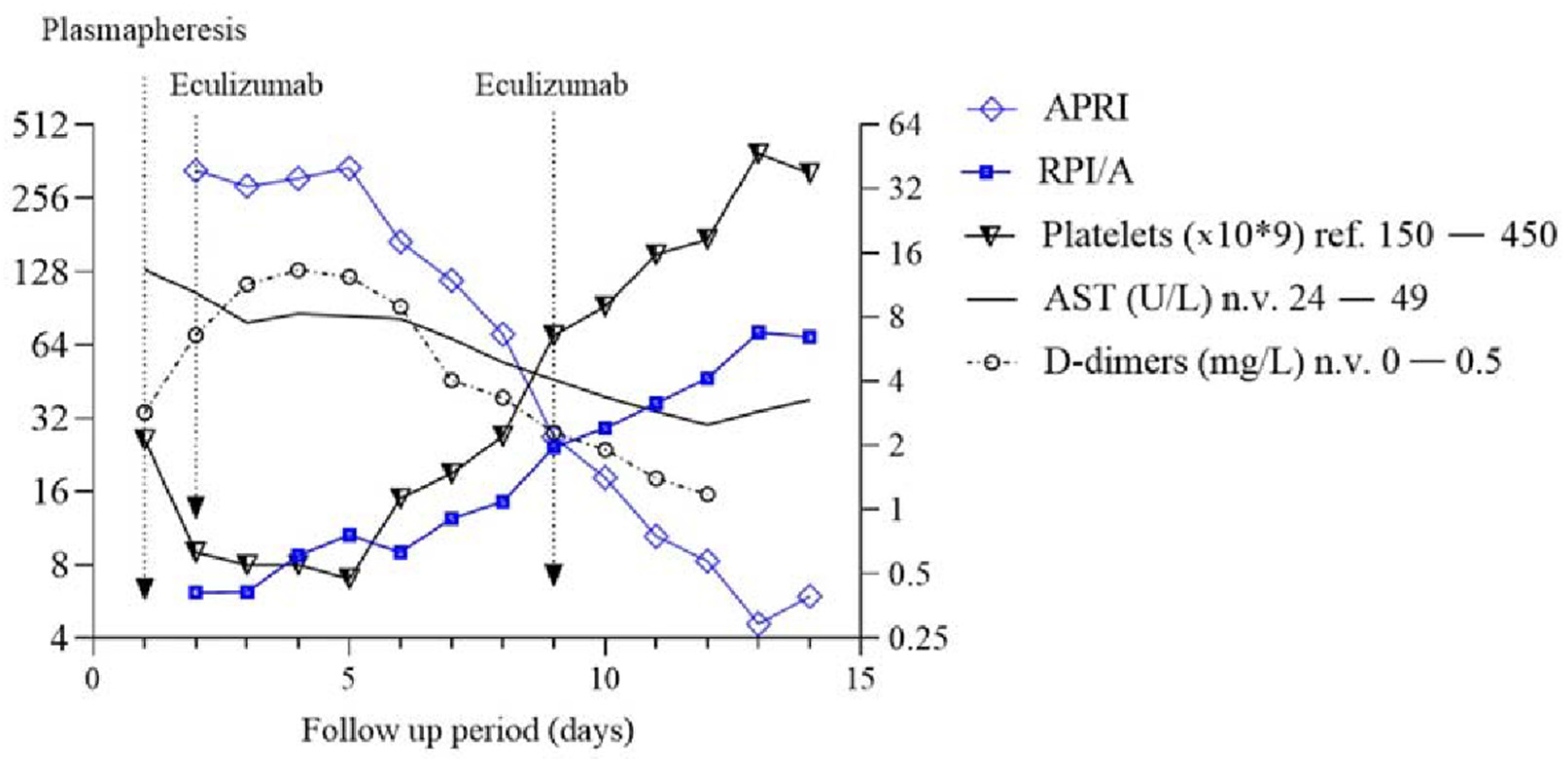
- Markers of bone marrow response to anemia;
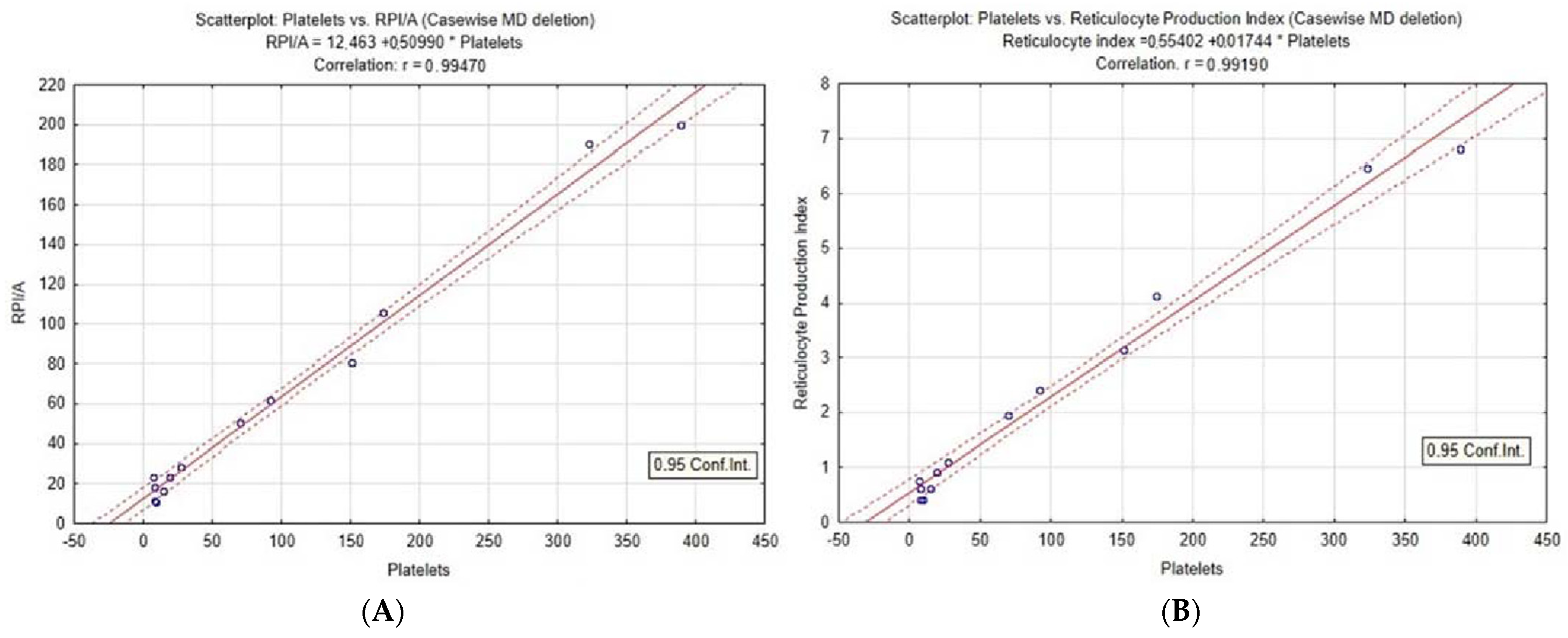
- Primarily serving as a marker of RBC and platelet recovery;
- Signifying a favorable response to treatment.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gordon, I.L.; Kwaan., H.C. Cancer-and drug-associated thrombotic thrombocytopenic purpura and hemolytic uremic syndrome. Semin. Hematol. 1997, 34, 140–147. [Google Scholar] [PubMed]
- Gordon, I.L.; Kwaan, H.C. Thrombotic microangiopathy manifesting as thrombotic thrombocytopenic purpura/hemolytic uremic syndrome in the cancer patient. Semin. Thromb. Hemost. 1999, 25, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, G.; Ozgonenel, B.; Bhambhani, K.; Kapur, G.; Smith, R.J.; Savaşan, S. Recurrent atypical hemolytic Uremic syndrome in children with acute lymphoblastic leukemia undergoing maintenance chemotherapy. J. Pediatr. Hematol. Oncol. 2018, 40, 560–562. [Google Scholar] [CrossRef] [PubMed]
- Hahn, H.; Ha, I.S.; Choi, H.S.; Shin, H.Y.; Cheong, H.I.; Ahn, H.S.; Choi, Y. Acute leukemia: An association with atypical hemolytic uremic syndrome. Pediatric Nephrol. 2003, 18, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Hee, B.; Youngkuk, C.; Chan, K.; Myung, S.; Hoon, K.; Tai, H. A case of atypical hemolytic uremic syndrome as an early manifestation of acute lymphoblastic leukemia. Korean J. Pediatr. 2010, 53, 253. [Google Scholar] [CrossRef]
- Piel, B.; Brittain, C.; Dixon, A. Haemolytic uraemic syndrome preceding acute lymphoblastic leukaemia. BMJ Case Rep. 2011, 4, bcr0520114285. [Google Scholar] [CrossRef] [Green Version]
- Salcedo, J.R.; Fusner, J. Hemolytic uremic syndrome followed by acute lymphocytic leukemia. Int. J. Pediatr. Nephrol. 1986, 7, 169–172. [Google Scholar]
- Martini, G.; Dall’Amico, R.; Murer, L.; Montini, G.; D’Avino, A.; Zacchello, G. Hemolytic-uremic syndrome as a presenting form of acute lymphocytic leukemia. Ann. Hematol. 2000, 79, 452–454. [Google Scholar] [CrossRef]
- Sinha, R.; AlAbbas, A.; Dionne, J.M.; Hurley, R.M. Simultaneous occurrence of atypical hemolytic uremic syndrome and acute lymphoblastic leukemia: A case report and literature review. Pediatr. Nephrol. 2008, 23, 835–839. [Google Scholar] [CrossRef]
- Chandra, D.; Lawson, S.; Ramani, P. Atypical haemolytic uraemic syndrome as a complication of induction chemotherapy for acute lymphoblastic leukaemia. J. Clin. Pathol. 2004, 57, 667–669. [Google Scholar] [CrossRef] [Green Version]
- Cavagnaro, F.; Barriga, F. Hemolytic uremic syndrome in a child with leukemia and cytomegalovirus infection. Pediatr. Nephrol. 2000, 14, 1118–1120. [Google Scholar] [CrossRef] [PubMed]
- Kanchi, H.; Webb, N.J.; Eden, O.B. Hemolytic uremic syndrome secondary to the treatment of acute lymphoblastic leukemia. J. Pediatr. Hematol. Oncol. 2000, 22, 483–484. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.A.; Pinkel, D.; Meehan, M.A.; Verani, R.R.; Ashkenazi, S.; Eftekhari, F.; Moake, J.L.; Portman, R.J. Acute renal failure in a female adolescent with leukemia in remission. J. Pediatr. 1991, 119, 999–1006. [Google Scholar] [CrossRef]
- Alparslan, C.; Yavaşcan, Ö.; Kasap, D.B.; Atmiş, B.; Karabay Bayazit, A.; Leblebisatan, G.; Öncel, E.P.; Alaygut, D.; Mutlubaş, F.; Aksu, N. Successful Management of a Rare Cause of Hemolytic Uremic Syndrome With Eculizumab in a Child. J. Pediatr. Hematol. Oncol. 2018, 40, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Shiari, R.; Parvaneh, V.J.; Dalirani, R.; Farivar, S.; Shiva, M.R. Atypical hemolytic-uremic syndrome associated with antiphospholipid antibodies and antiphospholipid syndrome: A novel presentation. Pediatr. Rheumatol. Online J. 2014, 12 (Suppl. 1), 363. [Google Scholar] [CrossRef] [Green Version]
- TIBCO Statistica. v. 12.5.0; TIBCO Software Inc.: Palo Alto, CA, USA, 2017; Available online: https://www.tibco.com/products/tibco-statistica (accessed on 18 February 2022).
- Bracho, F.J.; Osorio, I.A. Evaluation of the reticulocyte production index in the pediatric population. Am. J. Clin. Pathol. 2020, 8, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Piva, E.; Brugnara, C.; Spolaore, F.; Plebani, M. Clinical utility of reticulocyte parameters. Clin. Lab. Med. 2015, 35, 133–163. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Yonal, O.; Kurt, R.; Bayrak, M.; Aktas, B.; Ozdogan, O. Noninvasive assessment of liver fibrosis with the aspartate transaminase to platelet ratio index (APRI): Usefulness in patients with chronic liver disease: APRI in chronic liver disease. Hepat. Mon. 2011, 11, 103–116. [Google Scholar]
- Clarke, R.T.; Mitchell, C. Haemolytic uraemic syndrome in a patient with acute lymphoblastic leukemia. Pediatr. Blood Cancer 2010, 55, 1402–1405. [Google Scholar] [CrossRef]
- Bilic, E.; Bilic, E. Amino acid sequence homology of thrombopoietin and erythropoietin may explain thrombocytosis in children with iron deficiency anemia. J. Pediatr. Hematol. Oncol. 2003, 25, 675–676. [Google Scholar] [CrossRef]
- Xavier-Ferrucio, J.; Krause, D.S. Concise review: Bipotent megakaryocytic-erythroid progenitors: Concepts and controversies. Stem Cells. 2018, 36, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hukkinen, M.; Kivisaari, R.; Lohi, J.; Heikkilä, P.; Mutanen, A.; Merras-Salmio, L.; Pakarinen, M.P. Transient elastography and aspartate aminotransferase to platelet ratio predict liver injury in paediatric intestinal failure. Liver Int. 2016, 36, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Seok, J.Y.; Han, S.J.; Koh, H. Assessment of liver fibrosis and cirrhosis by aspartate aminotransferase-to-platelet ratio index in children with biliary atresia. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 198–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, J.J.; Gura, K.M.; Roda, J.; Perez-Atayde, A.R.; Duggan, C.; Jaksic, T.; Lo, C.W. Aspartate aminotransferase to platelet ratio index correlates with hepatic cirrhosis but not with fibrosis in pediatric patients with intestinal failure. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 367–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, W.G.; Park, S.H.; Jang, M.K.; Hahn, T.H.; Kim, J.B.; Lee, M.S.; Kim, D.J.; Jun, S.Y.; Park, C.K. Aspartate aminotransferase to platelet ratio index (APRI) can predict liver fibrosis in chronic hepatitis B. Dig. Liver Dis. 2008, 40, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Kirnake, V.; Arora, A.; Sharma, P.; Goyal, M.; Chawlani, R.; Toshniwal, J.; Kumar, A. Non-invasive aspartate aminotransferase to platelet ratio index correlates well with invasive hepatic venous pressure gradient in cirrhosis. Indian J. Gastroenterol. 2018, 37, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Sert, A.; Pirgon, O.; Aypar, E.; Yılmaz, H.; Dündar, B. Relationship between aspartate aminotransferase-to-platelet ratio index and carotid intima-media thickness in obese adolescents with non-alcoholic fatty liver disease. J. Clin. Res. Pediatr. Endocrinol. 2013, 10, 182–188. [Google Scholar] [CrossRef]
- De Matteis, C.; Cariello, M.; Graziano, G.; Battaglia, S.; Suppressa, P.; Piazzolla, G.; Sabbà, C.; Moschetta, A. AST to Platelet ratio Index (APRI) is an easy-to-use predictor score for cardiovascular risk in metabolic subjects. Sci. Rep. 2021, 11, 14834. [Google Scholar] [CrossRef]
- Siberry, G.K.; Cohen, R.A.; Harris, D.R.; Cruz, M.L.; Oliveira, R.; Peixoto, M.F.; Cervi, M.C.; Hazra, R.; Pinto, J.A. NISDI PLACES Protocol. Prevalence and predictors of elevated aspartate aminotransferase-to-platelet ratio index in Latin American perinatally HIV-infected children. Pediatr. Infect. Dis. J. 2014, 33, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Guedes, K.S.; Sanchez, B.A.M.; Gomes, L.T.; Fontes, C.J.F. Aspartate aminotransferase-to-platelet ratio index (APRI): A potential marker for diagnosis in patients at risk of severe malaria caused by Plasmodium vivax. PLoS ONE 2019, 14, e0224877. [Google Scholar] [CrossRef]
- Şaşmaz, M.İ.; Ayvaz, M.A.; Dülger, A.C.; Kuday Kaykısız, E.K.; Güven, R. Aspartate-aminotransferase to platelet ratio index score for predicting HELLP syndrome. Am. J. Emerg. Med. 2020, 38, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Nsiah, K.; Dzogbefia, V.P.; Ansong, D.; Akoto, A.O.; Boateng, H.; Ocloo, D. Pattern of AST and ALT changes in relation to hemolysis in sickle cell disease. Clinical Medicine. Blood Disord. 2011, 4, CMBD-S3969. [Google Scholar] [CrossRef]
- Arya, M.; Anvari, B.; Romo, G.M.; Cruz, M.A.; Dong, J.F.; McIntire, L.V.; Moake, J.L.; López, J.A. Ultralarge multimers of von Willebrand factor form spontaneous high-strength bonds with the platelet glycoprotein Ib-IX complex: Studies using optical tweezers. Blood 2002, 99, 3971–3977. [Google Scholar] [CrossRef] [PubMed]
- Galic, S.; Csuka, D.; Prohászka, Z.; Turudic, D.; Dzepina, P.; Milosevic, D. A case report of a child with sepsis induced multiorgan failure and massive complement consumption treated with a short course of Eculizumab: A case of crosstalk between coagulation and complement? Medicine 2019, 98, E14105. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.M.; Merin, N.; Burwick, R.M.; Abdelnour, L.; Selamet, U.; Yanny, B.; Bui, P.; Fouad, M.; Kurtz, I. Successful use of eculizumab to treat atypical hemolytic uremic syndrome in patients with inflammatory bowel disease. Thromb. J. 2019, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Øzbay, L.A. Eculizumab treatment of thrombotic microangiopathy in a patient with ulcerative colitis. Clin. J. Gastroenterol. 2020, 13, 344–348. [Google Scholar] [CrossRef]
- Lokki, A.I.; Haapio, M.; Heikkinen-Eloranta, J. Eculizumab Treatment for Postpartum HELLP Syndrome and aHUS-Case Report. Front Immunol. 2020, 11, 548. [Google Scholar] [CrossRef]
- Sakurai, S.; Kato, H.; Yoshida, Y.; Sugawara, Y.; Fujisawa, M.; Yasumoto, A.; Matsumoto, M.; Fujimura, Y.; Yatomi, Y.; Nangaku, M. Profiles of Coagulation and Fibrinolysis Activation-Associated Molecular Markers of Atypical Hemolytic Uremic Syndrome in the Acute Phase. J. Atheroscler. Thromb. 2020, 27, 353–362. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turudic, D.; Milosevic, D.; Bilic, K.; Prohászka, Z.; Bilic, E. A Limited Course of Eculizumab in a Child with the Atypical Hemolytic Uremic Syndrome and Pre-B Acute Lymphoblastic Leukemia on Maintenance Therapy: Case Report and Literature Review. J. Clin. Med. 2022, 11, 2779. https://doi.org/10.3390/jcm11102779
Turudic D, Milosevic D, Bilic K, Prohászka Z, Bilic E. A Limited Course of Eculizumab in a Child with the Atypical Hemolytic Uremic Syndrome and Pre-B Acute Lymphoblastic Leukemia on Maintenance Therapy: Case Report and Literature Review. Journal of Clinical Medicine. 2022; 11(10):2779. https://doi.org/10.3390/jcm11102779
Chicago/Turabian StyleTurudic, Daniel, Danko Milosevic, Katarina Bilic, Zoltán Prohászka, and Ernest Bilic. 2022. "A Limited Course of Eculizumab in a Child with the Atypical Hemolytic Uremic Syndrome and Pre-B Acute Lymphoblastic Leukemia on Maintenance Therapy: Case Report and Literature Review" Journal of Clinical Medicine 11, no. 10: 2779. https://doi.org/10.3390/jcm11102779
APA StyleTurudic, D., Milosevic, D., Bilic, K., Prohászka, Z., & Bilic, E. (2022). A Limited Course of Eculizumab in a Child with the Atypical Hemolytic Uremic Syndrome and Pre-B Acute Lymphoblastic Leukemia on Maintenance Therapy: Case Report and Literature Review. Journal of Clinical Medicine, 11(10), 2779. https://doi.org/10.3390/jcm11102779