
Impact of Cardiac Troponin Elevation on Mortality of Patients with Acute Heart Failure: Insights from the Korea Acute Heart Failure (KorAHF) Registry

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. High-Sensitivity Troponin-I (TnI) Analysis
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patients
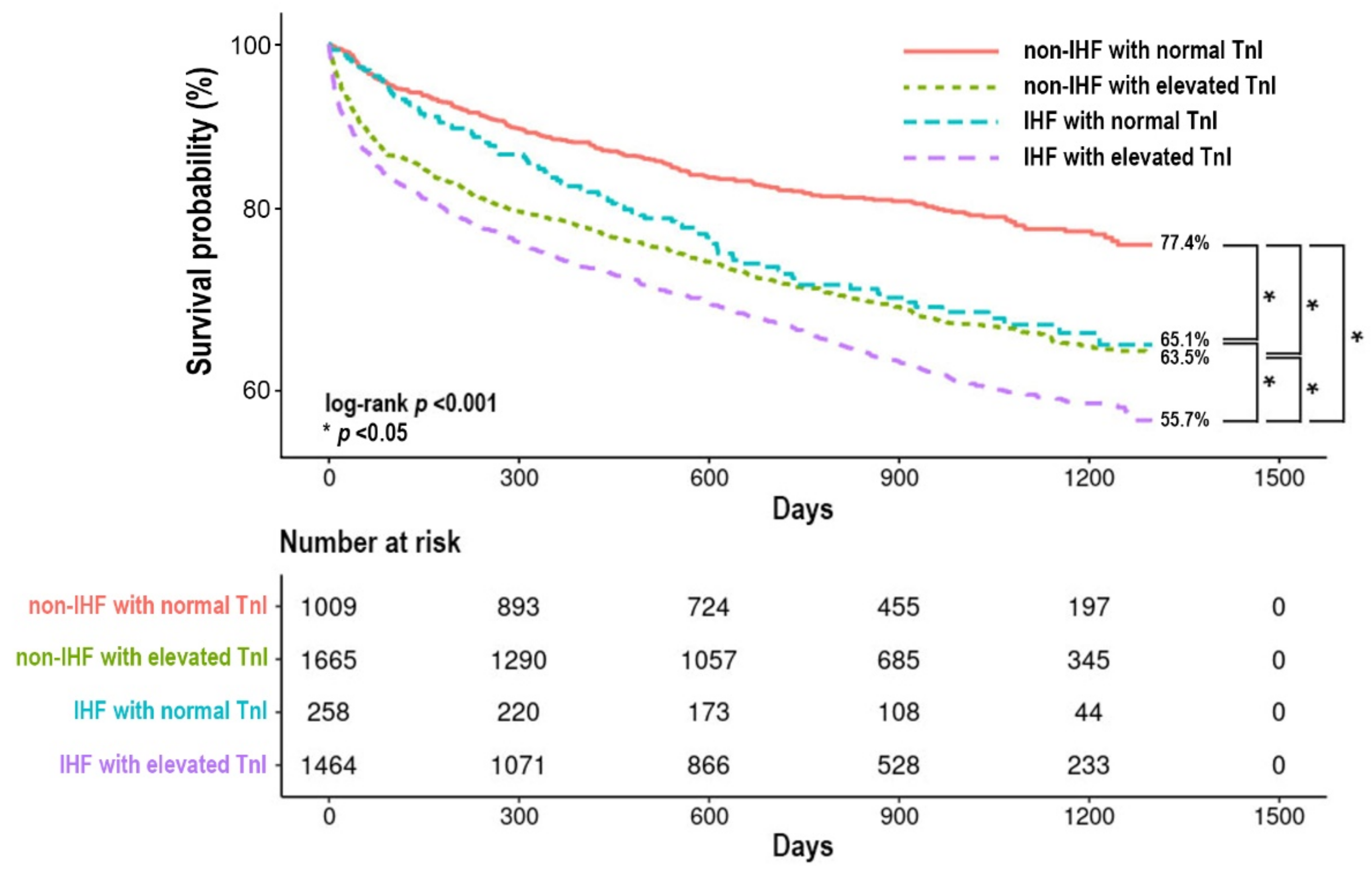
3.2. All-Cause Mortality According to the Etiology of AHF and the Status of TnI
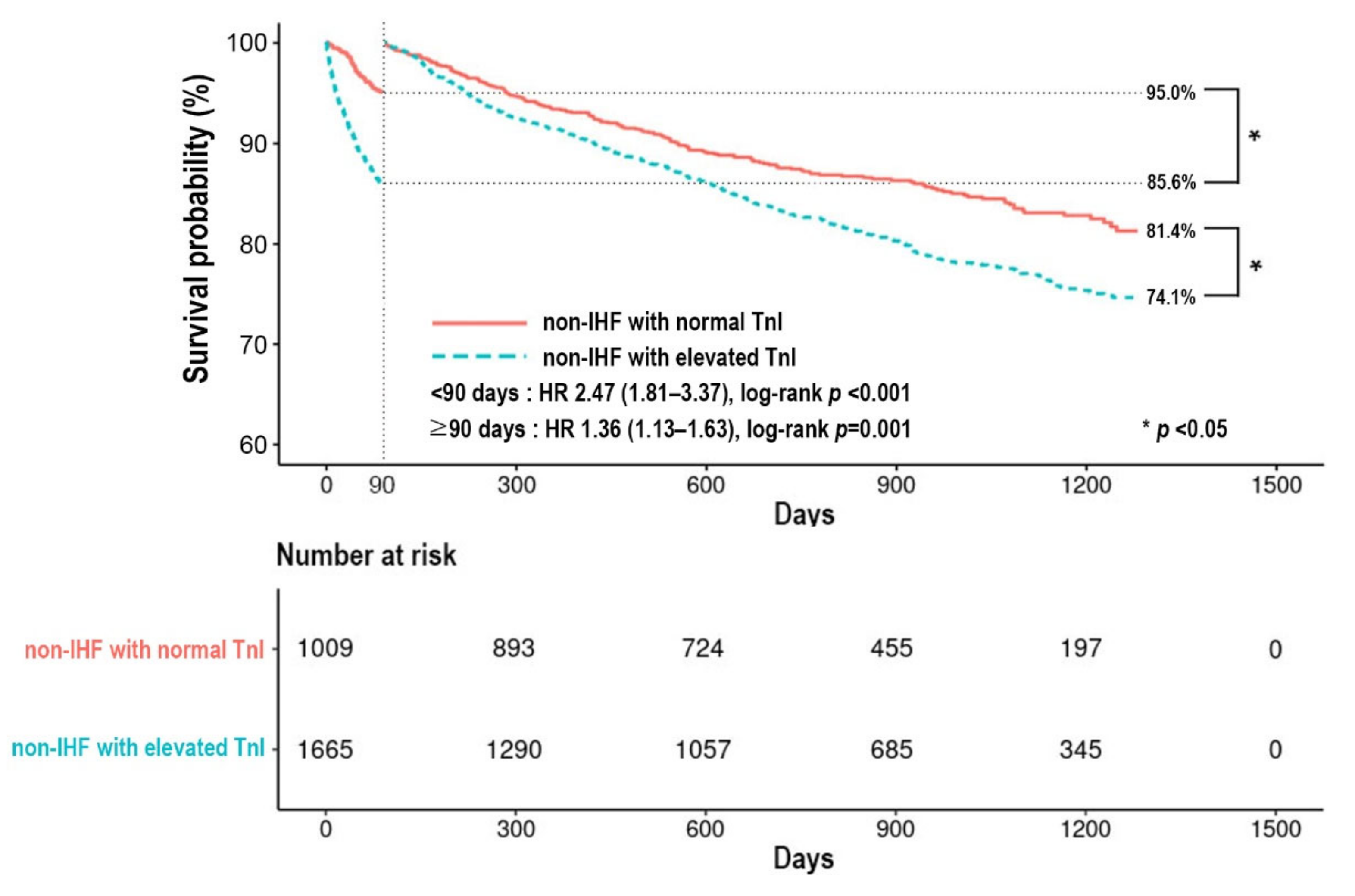
3.3. The 90-Day and Post-90-Day Mortality According to the Status of TnI in Non-IHF
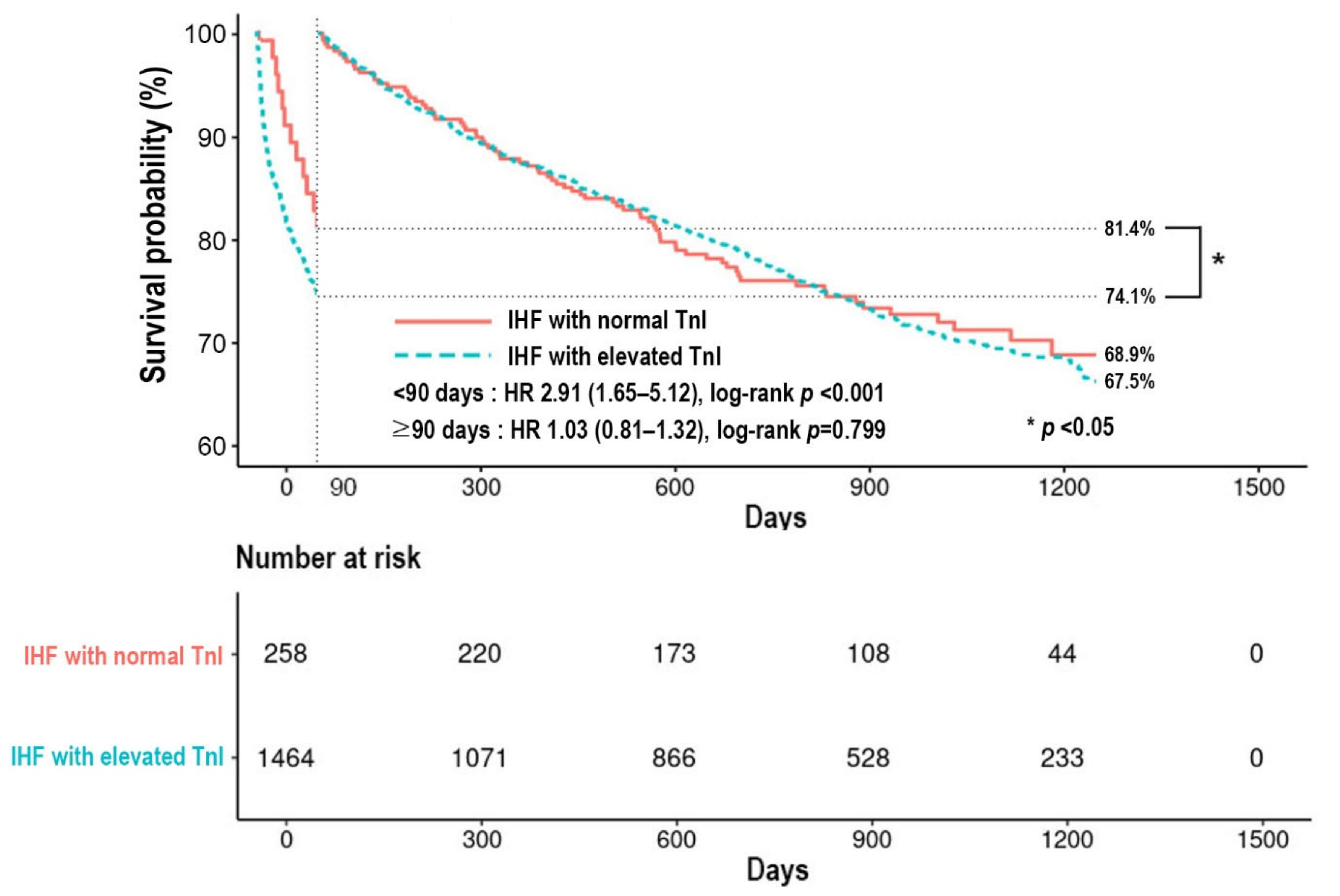
3.4. The 90-Day and Post-90-Day Mortality According to the Status of TnI in IHF
3.5. The Relationship between the Degree of TnI Elevation and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abraham, W.T.; Fonarow, G.C.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Predictors of in-hospital mortality in patients hospitalized for heart failure: Insights from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). J. Am. Coll. Cardiol. 2008, 52, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonarow, G.C.; Heywood, J.T.; Heidenreich, P.A.; Lopatin, M.; Yancy, C.W.; Committee, A.S.A.; Investigators. Temporal trends in clinical characteristics, treatments, and outcomes for heart failure hospitalizations, 2002 to 2004: Findings from Acute Decompensated Heart Failure National Registry (ADHERE). Am. Heart J. 2007, 153, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Francis, G.S.; Cogswell, R.; Thenappan, T. The heterogeneity of heart failure: Will enhanced phenotyping be necessary for future clinical trial success? J. Am. Coll. Cardiol. 2014, 64, 1775–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; et al. Clinical Characteristics and Outcome of Acute Heart Failure in Korea: Results from the Korean Acute Heart Failure Registry (KorAHF). Korean Circ. J. 2017, 47, 341–353. [Google Scholar] [CrossRef] [Green Version]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [Green Version]
- Sato, N.; Kajimoto, K.; Asai, K.; Mizuno, M.; Minami, Y.; Nagashima, M.; Murai, K.; Muanakata, R.; Yumino, D.; Meguro, T.; et al. Acute decompensated heart failure syndromes (ATTEND) registry. A prospective observational multicenter cohort study: Rationale, design, and preliminary data. Am. Heart J. 2010, 159, 949–955.e1. [Google Scholar] [CrossRef]
- West, R.; Liang, L.; Fonarow, G.C.; Kociol, R.; Mills, R.M.; O’Connor, C.M.; Hernandez, A.F. Characterization of heart failure patients with preserved ejection fraction: A comparison between ADHERE-US registry and ADHERE-International registry. Eur. J. Heart Fail. 2011, 13, 945–952. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Lim, N.K.; Cho, M.C.; Park, H.Y. Epidemiology of Heart Failure in Korea: Present and Future. Korean Circ. J. 2016, 46, 658–664. [Google Scholar] [CrossRef] [Green Version]
- Youn, J.C.; Han, S.; Ryu, K.H. Temporal Trends of Hospitalized Patients with Heart Failure in Korea. Korean Circ. J. 2017, 47, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-H.; Cho, S.M.J.; Lee, H.; Baek, J.; Bae, J.-H.; Chung, W.-J.; Kim, H.C. Korea Heart Disease Fact Sheet 2020: Analysis of Nationwide Data. Korean Circ. J. 2021, 51, 495–503. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Yancy, C.W. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Wettersten, N.; Maisel, A. Role of Cardiac Troponin Levels in Acute Heart Failure. Card. Fail. Rev. 2015, 1, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Horwich, T.B.; Patel, J.; MacLellan, W.R.; Fonarow, G.C. Cardiac troponin I is associated with impaired hemodynamics, progressive left ventricular dysfunction, and increased mortality rates in advanced heart failure. Circulation 2003, 108, 833–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metra, M.; Nodari, S.; Parrinello, G.; Specchia, C.; Brentana, L.; Rocca, P.; Fracassi, F.; Bordonali, T.; Milani, P.; Danesi, R.; et al. The role of plasma biomarkers in acute heart failure. Serial changes and independent prognostic value of NT-proBNP and cardiac troponin-T. Eur. J. Heart Fail. 2007, 9, 776–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunwald, E. Biomarkers in heart failure. N. Engl. J. Med. 2008, 358, 2148–2159. [Google Scholar] [CrossRef] [Green Version]
- Logeart, D.; Beyne, P.; Cusson, C.; Tokmakova, M.; Leban, M.; Guiti, C.; Bourgoin, P.; Solal, A.C. Evidence of cardiac myolysis in severe nonischemic heart failure and the potential role of increased wall strain. Am. Heart J. 2001, 141, 247–253. [Google Scholar] [CrossRef]
- Narula, J.; Haider, N.; Virmani, R.; DiSalvo, T.G.; Kolodgie, F.D.; Hajjar, R.J.; Schmidt, U.; Semigran, M.J.; Dec, G.W.; Khaw, B.A. Apoptosis in myocytes in end-stage heart failure. N. Engl. J. Med. 1996, 335, 1182–1189. [Google Scholar] [CrossRef]
- Kociol, R.D.; Pang, P.S.; Gheorghiade, M.; Fonarow, G.C.; O’Connor, C.M.; Felker, G.M. Troponin elevation in heart failure prevalence, mechanisms, and clinical implications. J. Am. Coll. Cardiol. 2010, 56, 1071–1078. [Google Scholar] [CrossRef] [Green Version]
- Lim, N.K.; Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; et al. Risk prediction for 30-day heart failure-specific readmission or death after discharge: Data from the Korean Acute Heart Failure (KorAHF) registry. J. Cardiol. 2019, 73, 108–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peacock, W.F.T.; De Marco, T.; Fonarow, G.C.; Diercks, D.; Wynne, J.; Apple, F.S.; Wu, A.H.; Investigators, A. Cardiac troponin and outcome in acute heart failure. N. Engl. J. Med. 2008, 358, 2117–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y. Clinical characteristics of Korean patients with congestive heart failure. Korean J. Med. 1998, 55, 446–452. [Google Scholar]
- Han, S.W.; Ryu, K.H.; Chae, S.C.; Yang, D.H.; Shin, M.S.; Lee, S.H.; Ahn, Y.G. Multicenter analysis of clinical characteristics and prognostic factors of patients with congestive heart failure in Korea. Korean Circ. J. 2005, 35, 357–361. [Google Scholar] [CrossRef]
- Choi, D.J.; Han, S.; Jeon, E.S.; Cho, M.C.; Kim, J.J.; Yoo, B.S.; Ryu, K.H. Characteristics, outcomes and predictors of long-term mortality for patients hospitalized for acute heart failure: A report from the Korean Heart Failure Registry. Korean Circ. J. 2011, 41, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.E.; Cho, H.J.; Lee, H.Y.; Yang, H.M.; Choi, J.O.; Jeon, E.S.; Oh, B.H. A multicentre cohort study of acute heart failure syndromes in Korea: Rationale, design, and interim observations of the Korean Acute Heart Failure (KorAHF) registry. Eur. J. Heart Fail. 2014, 16, 700–708. [Google Scholar] [CrossRef]
- Mohammed, A.A.; Januzzi, J.L., Jr. Clinical applications of highly sensitive troponin assays. Cardiol. Rev. 2010, 18, 12–19. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Group, E.S.D. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2018, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.; Schaus, B.J.; Fallavollita, J.A.; Lee, T.C.; Canty, J.M., Jr. Preload induces troponin I degradation independently of myocardial ischemia. Circulation 2001, 103, 2035–2037. [Google Scholar] [CrossRef] [Green Version]
- de Lemos, J.A.; Drazner, M.H.; Omland, T.; Ayers, C.R.; Khera, A.; Rohatgi, A.; Hashim, I.; Berry, J.D.; Das, S.R.; Morrow, D.A.; et al. Association of troponin T detected with a highly sensitive assay and cardiac structure and mortality risk in the general population. JAMA 2010, 304, 2503–2512. [Google Scholar] [CrossRef]
- deFilippi, C.R.; de Lemos, J.A.; Christenson, R.H.; Gottdiener, J.S.; Kop, W.J.; Zhan, M.; Seliger, S.L. Association of serial measures of cardiac troponin T using a sensitive assay with incident heart failure and cardiovascular mortality in older adults. JAMA 2010, 304, 2494–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, J.T.; Nambi, V.; de Lemos, J.A.; Chambless, L.E.; Virani, S.S.; Boerwinkle, E.; Hoogeveen, R.C.; Liu, X.; Astor, B.C.; Mosley, T.H.; et al. Cardiac troponin T measured by a highly sensitive assay predicts coronary heart disease, heart failure, and mortality in the Atherosclerosis Risk in Communities Study. Circulation 2011, 123, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felker, G.M.; Thompson, R.E.; Hare, J.M.; Hruban, R.H.; Clemetson, D.E.; Howard, D.L.; Baughman, K.L.; Kasper, E.K. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N. Engl. J. Med. 2000, 342, 1077–1084. [Google Scholar] [CrossRef]
- Felker, G.M.; Hasselblad, V.; Tang, W.H.; Hernandez, A.F.; Armstrong, P.W.; Fonarow, G.C.; Voors, A.A.; Metra, M.; McMurray, J.J.; Butler, J.; et al. Troponin I in acute decompensated heart failure: Insights from the ASCEND-HF study. Eur. J. Heart Fail. 2012, 14, 1257–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arenja, N.; Reichlin, T.; Drexler, B.; Oshima, S.; Denhaerynck, K.; Haaf, P.; Potocki, M.; Breidthardt, T.; Noveanu, M.; Stelzig, C.; et al. Sensitive cardiac troponin in the diagnosis and risk stratification of acute heart failure. J. Intern. Med. 2012, 271, 598–607. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Non-IHF with Normal TnI (n = 1009) | Non-IHF with Elevated TnI (n = 1665) | IHF with Normal TnI (n = 258) | IHF with Elevated TnI (n = 1464) | p |
|---|---|---|---|---|---|
| Median age—yr | 72 (59–78) | 70 (56–78) | 72 (66–79) †,§ | 74 (66–80) ‡,* | <0.001 |
| Male sex—no. (%) | 446 (44.2) | 812 (48.8) | 159 (61.6) †,§ | 895 (61.1) ‡,* | <0.001 |
| Previous admission due to HF | 279 (27.7) | 529 (31.8) | 109 (42.2) †,§ | 418 (28.6) ♭ | <0.001 |
| Medical conditions—no. (%) | |||||
| Hypertension | 550 (54.5) | 863 (51.8) | 178 (69.0) †,§ | 1043 (71.2) ‡,* | <0.001 |
| Diabetes | 253 (25.1) | 421 (25.3) | 133 (51.6) †,§ | 755 (51.6) ‡,* | <0.001 |
| Chronic kidney disease | 72 (7.1) | 209 (12.6) ¶ | 35 (13.6) † | 285 (19.5) ‡,* | <0.001 |
| Chronic obstructive pulmonary disease | 124 (12.3) | 200 (12.0) | 28 (10.9) | 146 (10.0) | 0.216 |
| Cerebrovascular accident | 125 (12.4) | 224 (13.5) | 47 (18.2) | 272 (18.6) ‡,* | <0.001 |
| Prior coronary artery disease | 101 (10.0) | 149 (8.9) | 196 (76.0) †,§ | 837 (57.2) ‡,*,♭ | <0.001 |
| Prior myocardial infarction | 36 (3.6) | 55 (3.3) | 141 (54.7) †,§ | 513 (35.1) ‡,*,♭ | <0.001 |
| Heart failure | 398 (39.5) | 731 (43.9) | 141 (54.7) †,§ | 556 (38.0) *,♭ | <0.001 |
| Malignancy | 89 (8.8) | 151 (9.1) | 18 (7.0) | 100 (6.8) | 0.095 |
| Initial clinical findings | |||||
| Median SBP—mmHg | 130 (112–150) | 129 (109–151) | 132 (113–153) | 132 (113–153) * | 0.004 |
| Median LVEF—% | 43.0 (28.0–57.1) | 36.0 (24.6–52.0) ¶ | 36.0 (26.4–49.2) † | 34.4 (26.0–44.0) ‡,* | <0.001 |
| Median TnI—ng/mL | 0.02 (0.01–0.04) | 0.10 (0.05–0.25) ¶ | 0.02 (0.01–0.04) § | 0.20 (0.20–1.74) ‡,*,♭ | <0.001 |
| Median serum Na—mEq/L | 139 (136–141) | 138 (135–140) ¶ | 138 (136–141) § | 138 (135–140) ‡ | <0.001 |
| Median serum Cr—mg/dL | 0.94 (0.75–1.23) | 1.08 (0.81–1.52) ¶ | 1.10 (0.86–1.44) † | 1.21 (0.90–1.80) ‡,*,♭ | <0.001 |
| Atrial fibrillation at admission | 533 (52.8) | 628 (37.7) ¶ | 92 (35.7) † | 231 (15.8) ‡,*,♭ | <0.001 |
| Procedures during the index hospitalization—no. (%) | |||||
| Coronary revascularization | 1 (0.1) | 25 (1.5) | 28 (10.9) †§ | 570 (39.0) ‡,*,♭ | <0.001 |
| Medication at discharge—no. (%) | |||||
| ACEI/ARB | 692 (68.6) | 1016 (61.0) ¶ | 196 (76.0) § | 964 (65.8) *,♭ | <0.001 |
| Beta-blocker | 567 (56.2) | 743 (44.6) ¶ | 159 (61.6) § | 804 (54.9) * | <0.001 |
| Aldosterone antagonist | 513 (50.8) | 703 (42.2) ¶ | 122 (47.3) | 523 (35.7) ‡,*,♭ | <0.001 |
| Factor | Crude Hazard Ratio on Univariate Analysis (95% CI) | p | Adjusted Hazard Ratio on Multivariate Analysis (95% CI) | p |
|---|---|---|---|---|
| Groups | <0.001 | <0.001 | ||
| Non-IHF with normal TnI | 1.00 | 1.00 | ||
| Non-IHF with elevated TnI | 1.77 (1.52–2.07) | <0.001 | 1.60 (1.36–1.88) | <0.001 |
| IHF with normal TnI | 1.61 (1.26–2.06) | <0.001 | 1.44 (1.12–1.85) | 0.005 |
| IHF with elevated TnI | 2.29 (1.97–2.66) | <0.001 | 1.88 (1.60–2.21) | <0.001 |
| Demographics | ||||
| Age ≥ 65 year | 2.59 (2.27–2.96) | <0.001 | 2.61 (2.25–3.02) | <0.001 |
| Male sex | 1.01 (0.91–1.11) | 0.892 | ||
| Comorbidities | ||||
| Hypertension | 1.38 (1.24–1.53) | <.0.001 | 1.10 (0.97–1.23) | 0.128 |
| Diabetes | 1.32 (1.19–1.46) | <0.001 | ||
| Previous admission due to HF | 1.74 (1.58–1.93) | <0.001 | 1.34 (1.20–1.49) | <0.001 |
| Prior coronary artery disease | 1.53 (1.38–1.69) | <0.001 | ||
| Prior myocardial infarction | 1.52 (1.35–1.71) | <0.001 | ||
| Chronic kidney disease | 2.01 (1.78–2.26) | <0.001 | 1.32 (1.12–1.55) | 0.001 |
| Chronic obstructive pulmonary disease | 1.46 (1.27–1.68) | <0.001 | 1.27 (1.09–1.47) | 0.002 |
| Cerebrovascular accident | 1.54 (1.36–1.74) | <0.001 | 1.23 (1.08–1.40) | 0.002 |
| Malignancy | 1.67 (1.43–1.95) | <0.001 | 1.51 (1.28–1.77) | <0.001 |
| Findings at admission | ||||
| SBP < 110 mmHg | 1.31 (1.17–1.47) | <0.001 | 1.27 (1.12–1.44) | <0.001 |
| LVEF < 40% | 1.12 (1.01–1.24) | 0.033 | 1.26 (1.13–1.41) | <0.001 |
| Serum Na < 135 mEq/L | 1.80 (1.61–2.01) | <0.001 | 1.56 (1.39–1.75) | <0.001 |
| Serum Cr ≥ 2.0 mg/dL | 1.95 (1.73–2.20) | <0.001 | 1.28 (1.09–1.50) | 0.003 |
| Atrial fibrillation | 0.93 (0.83–1.03) | 0.160 | ||
| Medication at discharge | ||||
| ACEI/ARB | 0.56 (0.51–0.62) | <0.001 | 0.65 (0.58–0.72) | <0.001 |
| Beta-blocker | 0.60 (0.55–0.67) | <0.001 | 0.69 (0.62–0.77) | <0.001 |
| Aldosterone antagonist | 0.82 (0.74–0.91) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Cho, J.Y.; Kim, K.H.; Kim, H.Y.; Cho, H.-J.; Lee, H.-Y.; Jeon, E.-S.; Kim, J.-J.; Cho, M.-C.; Chae, S.C.; et al. Impact of Cardiac Troponin Elevation on Mortality of Patients with Acute Heart Failure: Insights from the Korea Acute Heart Failure (KorAHF) Registry. J. Clin. Med. 2022, 11, 2800. https://doi.org/10.3390/jcm11102800
Lee N, Cho JY, Kim KH, Kim HY, Cho H-J, Lee H-Y, Jeon E-S, Kim J-J, Cho M-C, Chae SC, et al. Impact of Cardiac Troponin Elevation on Mortality of Patients with Acute Heart Failure: Insights from the Korea Acute Heart Failure (KorAHF) Registry. Journal of Clinical Medicine. 2022; 11(10):2800. https://doi.org/10.3390/jcm11102800
Chicago/Turabian StyleLee, Nuri, Jae Yeong Cho, Kye Hun Kim, Hyung Yoon Kim, Hyun-Jai Cho, Hae-Young Lee, Eun-Seok Jeon, Jae-Joong Kim, Myeong-Chan Cho, Shung Chull Chae, and et al. 2022. "Impact of Cardiac Troponin Elevation on Mortality of Patients with Acute Heart Failure: Insights from the Korea Acute Heart Failure (KorAHF) Registry" Journal of Clinical Medicine 11, no. 10: 2800. https://doi.org/10.3390/jcm11102800
APA StyleLee, N., Cho, J. Y., Kim, K. H., Kim, H. Y., Cho, H. -J., Lee, H. -Y., Jeon, E. -S., Kim, J. -J., Cho, M. -C., Chae, S. C., Baek, S. H., Kang, S. -M., Choi, D. -J., Yoo, B. -S., Oh, B. -H., & on behalf of the KorAHF Investigators. (2022). Impact of Cardiac Troponin Elevation on Mortality of Patients with Acute Heart Failure: Insights from the Korea Acute Heart Failure (KorAHF) Registry. Journal of Clinical Medicine, 11(10), 2800. https://doi.org/10.3390/jcm11102800