
Cyclic Metronomic Chemotherapy for Pediatric Tumors: Six Case Reports and a Review of the Literature



Abstract
:1. Introduction
1.1. Patient 1
1.2. Patient 2
1.3. Patient 3
1.4. Patient 4
1.5. Patient 5
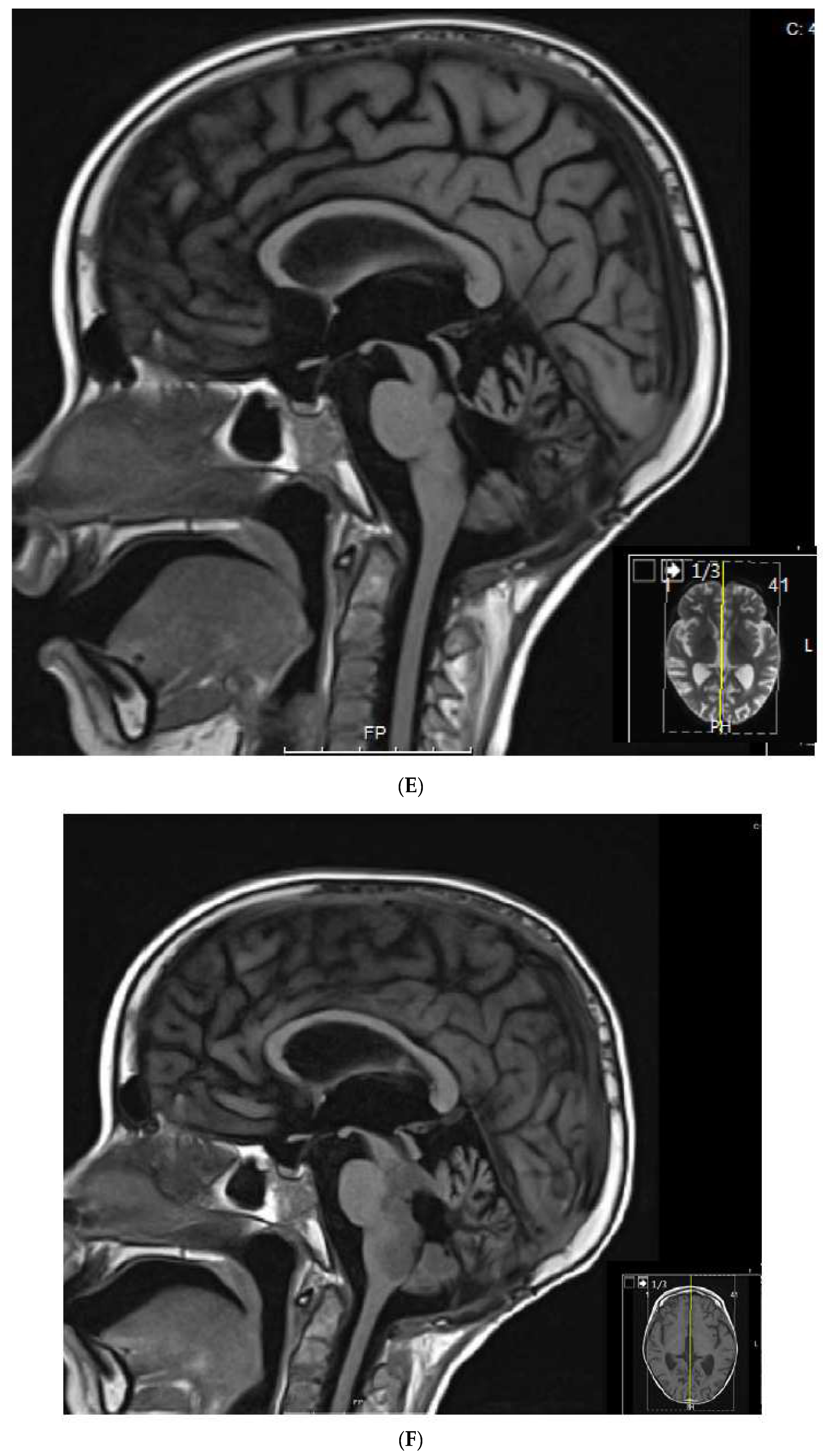
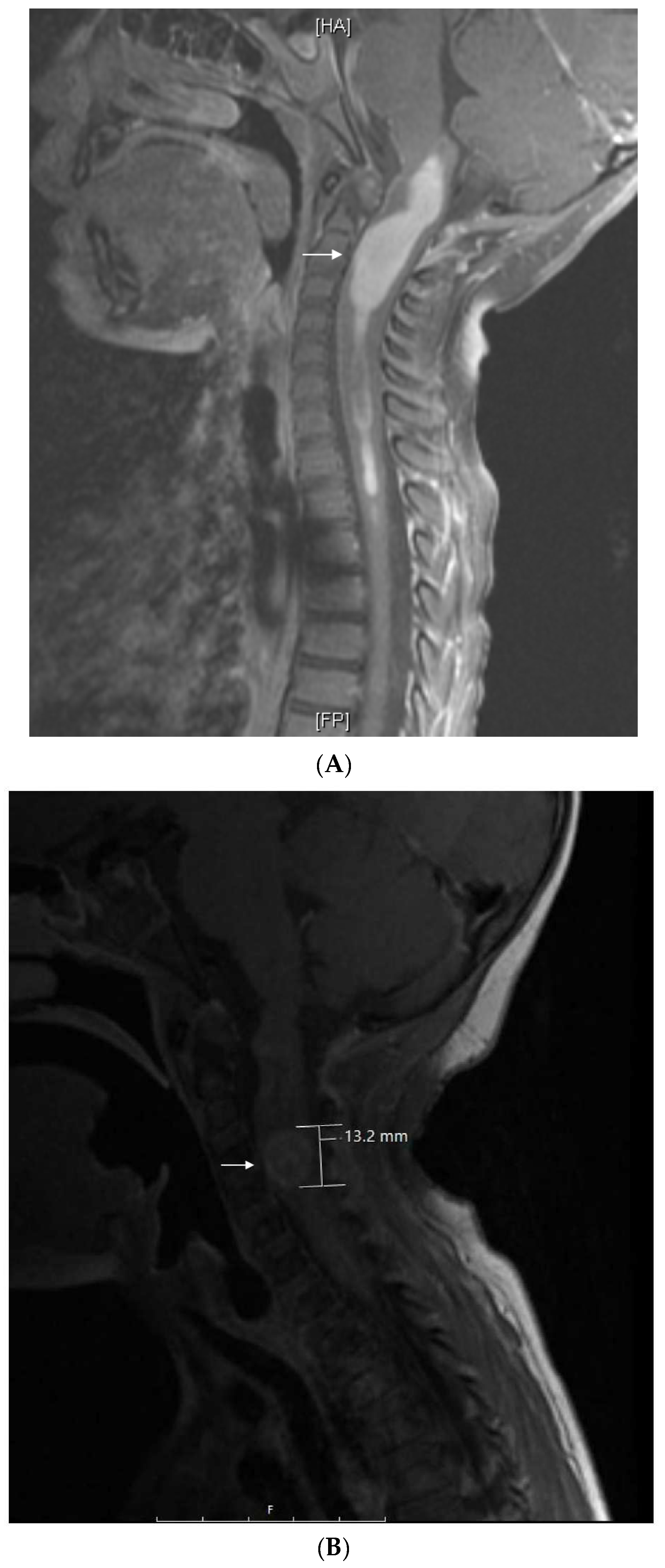
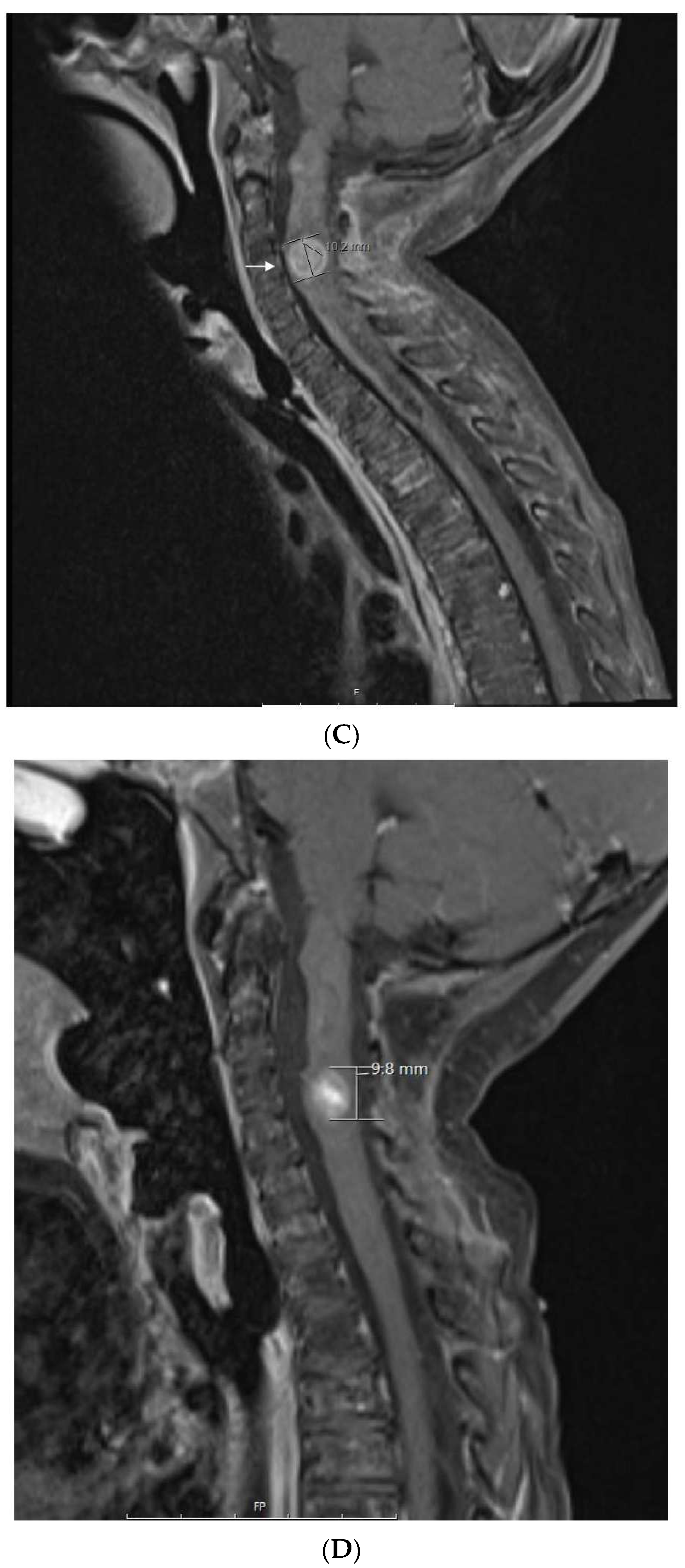
1.6. Patient 6
2. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kerbel, R.S.; Kamen, B.A. The anti-angiogenic basis of metronomic chemotherapy. Nat. Rev. Cancer 2004, 4, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Derosa, L.; Galli, L.; Orlandi, P.; Fioravanti, A.; Di Desidero, T.; Fontana, A.; Antonuzzo, A.; Biasco, E.; Farnesi, A.; Marconcini, R.; et al. Docetaxel plus oral metronomic cyclophosphamide: A phase II study with pharmacodynamic and pharmacogenetic analyses in castration-resistant prostate cancer patients. Cancer 2014, 120, 3923–3931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerbel, R.S.; Grothey, A. Gastrointestinal cancer: Rationale for metronomic chemotherapy in phase III trials. Nat. Rev. Clin. Oncol. 2015, 12, 313–314. [Google Scholar] [CrossRef]
- Bocci, G.; Kerbel, R.S. Pharmacokinetics of metronomic chemotherapy: A neglected but crucial aspect. Nat. Rev. Clin. Oncol. 2016, 11, 659–673. [Google Scholar] [CrossRef] [PubMed]
- Munzone, E.; Colleoni, M. Clinical overview of metronomic chemotherapy in breast cancer. Nat. Rev. Clin. Oncol. 2015, 12, 631–644. [Google Scholar] [CrossRef]
- Andre, N.; Banavali, S.; Pasquier, E. Paediatrics: Metronomics—Fulfilling unmet needs beyond level A evidence. Nat. Rev. Clin. Oncol. 2016, 13, 469–470. [Google Scholar] [CrossRef]
- Simkens, L.H.; van Tinteren, H.; May, A.; ten Tije, A.J.; Creemers, G.J.; Loosveld, O.J.; de Jongh, F.E.; Erdkamp, F.L.; Erjavec, Z.; van der Torren, A.M.; et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): A phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet 2015, 385, 1843–1852. [Google Scholar] [CrossRef]
- Rochlitz, C.; Bigler, M.; von Moos, R.; Bernhard, J.; Matter-Walstra, K.; Wicki, A.; Zaman, K.; Anchisi, S.; Kung, M.; Na, K.J.; et al. SAKK 24/09: Safety and tolerability of bevacizumab plus paclitaxel vs. bevacizumab plus metronomic cyclophosphamide and capecitabine as first-line therapy in patients with HER2-negative advanced stage breast cancer—A multicenter, randomized phase III trial. BMC Cancer 2016, 16, 780. [Google Scholar] [CrossRef] [Green Version]
- Robison, N.J.; Campigotto, F.; Chi, S.N.; Manley, P.E.; Turner, C.D.; Zimmerman, M.A.; Chordas, C.A.; Werger, A.M.; Allen, J.C.; Goldman, S.; et al. A phase II trial of a multi-agent oral antiangiogenic (metronomic) regimen in children with recurrent or progressive cancer. Pediatric Blood Cancer 2014, 61, 636–642. [Google Scholar] [CrossRef]
- Kieran, M.W.; Turner, C.D.; Rubin, J.B.; Chi, S.N.; Zimmerman, M.A.; Chordas, C.; Klement, G.; Laforme, A.; Gordon, A.; Thomas, A.; et al. A feasibility trial of antiangiogenic (metronomic) chemotherapy in pediatric patients with recurrent or progressive cancer. J. Pediatric Hematol. Oncol. 2005, 27, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Andre, N.; Cointe, S.; Barlogis, V.; Arnaud, L.; Lacroix, R.; Pasquier, E.; Dignat-George, F.; Michel, G.; Sabatier, F. Maintenance chemotherapy in children with ALL exerts metronomic-like thrombospondin-1 associated anti-endothelial effect. Oncotarget 2015, 6, 23008–23014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andre, N.; Abed, S.; Orbach, D.; Alla, C.A.; Padovani, L.; Pasquier, E.; Gentet, J.C.; Verschuur, A. Pilot study of a pediatric metronomic 4-drug regimen. Oncotarget 2011, 2, 960–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andre, N.; Rome, A.; Coze, C.; Padovani, L.; Pasquier, E.; Camoin, L.; Gentet, J.C. Metronomic etoposide/cyclophosphamide/celecoxib regimen given to children and adolescents with refractory cancer: A preliminary monocentric study. Clin. Ther. 2008, 30, 1336–1340. [Google Scholar] [CrossRef]
- Roux, C.; Revon-Rivière, G.; Gentet, J.C.; Verschuur, A.; Scavarda, D.; Saultier, P.; Appay, R.; Padovani, L.; André, N. Metronomic Maintenance With Weekly Vinblastine After Induction With Bevacizumab-Irinotecan in Children With Low-grade Glioma Prevents Early Relapse. J. Pediatric Hematol. Oncol. 2021, 43, e630–e634. [Google Scholar] [CrossRef] [PubMed]
- El Kababri, M.; Benmiloud, S.; Cherkaoui, S.; El Houdzi, J.; Maani, K.; Ansari, N.; Khoubila, N.; Kili, A.; El Khorassani, M.; Madani, A.; et al. Metro-SMHOP 01: Metronomics combination with cyclophosphamide-etoposide and valproic acid for refractory and relapsing pediatric malignancies. Pediatric Blood Cancer 2020, 67, e28508. [Google Scholar] [CrossRef]
- Verschuur, A.; Heng-Maillard, M.A.; Dory-Lautrec, P.; Truillet, R.; Jouve, E.; Chastagner, P.; Leblond, P.; Aerts, I.; Honoré, S.; Entz-Werle, N.; et al. Metronomic Four-Drug Regimen Has Anti-tumor Activity in Pediatric Low-Grade Glioma; The Results of a Phase II Clinical Trial. Front. Pharmacol. 2018, 9, 00950. [Google Scholar] [CrossRef]
- Berland, M.; Padovani, L.; Rome, A.; Pech-Gourg, G.; Figarella-Branger, D.; André, N. Sustained Complete Response to Metronomic Chemotherapy in a Child with Refractory Atypical Teratoid Rhabdoid Tumor: A Case Report. Front. Pharmacol. 2017, 8, 792. [Google Scholar] [CrossRef] [Green Version]
- Sharp, J.R.; Bouffet, E.; Stempak, D.; Gammon, J.; Stephens, D.; Johnston, D.L.; Eisenstat, D.; Hukin, J.; Samson, Y.; Bartels, U.; et al. A multi-centre Canadian pilot study of metronomic temozolomide combined with radiotherapy for newly diagnosed paediatric brainstem glioma. Eur. J. Cancer 2010, 46, 3271–3279. [Google Scholar] [CrossRef]
- Bocci, G.; Francia, G.; Man, S.; Lawler, J.; Kerbel, R.S. Thrombospondin 1, a mediator of the antiangiogenic effects of low-dose metronomic chemotherapy. Proc. Natl. Acad. Sci. USA 2003, 100, 12917–12922. [Google Scholar] [CrossRef] [Green Version]
- Francia, G.; Shaked, Y.; Hashimoto, K.; Sun, J.; Yin, M.; Cesta, C.; Xu, P.; Man, S.; Hackl, C.; Stewart, J.; et al. Low-dose metronomic oral dosing of a prodrug of gemcitabine (LY2334737) causes antitumor effects in the absence of inhibition of systemic vasculogenesis. Mol. Cancer Ther. 2012, 11, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Ghiringhelli, F.; Menard, C.; Puig, P.E.; Ladoire, S.; Roux, S.; Martin, F.; Solary, E.; Le Cesne, A.; Zitvogel, L.; Chauffert, B. Metronomic cyclophosphamide regimen selectively depletes CD4+CD25+ regulatory T cells and restores T and NK effector functions in end stage cancer patients. Cancer Immunol. Immunother. CII 2007, 56, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Allegrini, G.; Di Desidero, T.; Barletta, M.T.; Fioravanti, A.; Orlandi, P.; Canu, B.; Chericoni, S.; Loupakis, F.; Di Paolo, A.; Masi, G.; et al. Clinical, pharmacokinetic and pharmacodynamic evaluations of metronomic UFT and cyclophosphamide plus celecoxib in patients with advanced refractory gastrointestinal cancers. Angiogenesis 2012, 15, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, G.; De Salvo, G.L.; Bergeron, C.; Gallego Melcón, S.; Merks, J.H.; Kelsey, A.; Martelli, H.; Minard-Colin, V.; Orbach, D.; Glosli, H.; et al. Vinorelbine and continuous low-dose cyclophosphamide as maintenance chemotherapy in patients with high-risk rhabdomyosarcoma (RMS 2005): A multicentre, open-label, randomised, phase 3 trial. Lancet. Oncol. 2019, 20, 1566–1575. [Google Scholar] [CrossRef]
- Peyrl, A.; Chocholous, M.; Kieran, M.W.; Azizi, A.A.; Prucker, C.; Czech, T.; Dieckmann, K.; Schmook, M.T.; Haberler, C.; Leiss, U.; et al. Antiangiogenic metronomic therapy for children with recurrent embryonal brain tumors. Pediatric Blood Cancer 2012, 59, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Zapletalova, D.; André, N.; Deak, L.; Kyr, M.; Bajciova, V.; Mudry, P.; Dubska, L.; Demlova, R.; Pavelka, Z.; Zitterbart, K.; et al. Metronomic chemotherapy with the COMBAT regimen in advanced pediatric malignancies: A multicenter experience. Oncology 2012, 82, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Colleoni, M.; Rocca, A.; Sandri, M.T.; Zorzino, L.; Masci, G.; Nolè, F.; Peruzzotti, G.; Robertson, C.; Orlando, L.; Cinieri, S.; et al. Low-dose oral methotrexate and cyclophosphamide in metastatic breast cancer: Antitumor activity and correlation with vascular endothelial growth factor levels. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2002, 13, 73–80. [Google Scholar] [CrossRef]
- Chen, C.L.; Fuscoe, J.C.; Liu, Q.; Pui, C.H.; Mahmoud, H.H.; Relling, M.V. Relationship between cytotoxicity and site-specific DNA recombination after in vitro exposure of leukemia cells to etoposide. J. Natl. Cancer Inst. 1996, 88, 1840–1847. [Google Scholar] [CrossRef] [Green Version]
- Ashley, D.M.; Meier, L.; Kerby, T.; Zalduondo, F.M.; Friedman, H.S.; Gajjar, A.; Kun, L.; Duffner, P.K.; Smith, S.; Longee, D. Response of recurrent medulloblastoma to low-dose oral etoposide. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1996, 14, 1922–1927. [Google Scholar] [CrossRef]
- Khan, Z.; Khan, N.; Tiwari, R.P.; Sah, N.K.; Prasad, G.B.; Bisen, P.S. Biology of Cox-2: An application in cancer therapeutics. Curr. Drug Targets 2011, 12, 1082–1093. [Google Scholar] [CrossRef]
- Gately, S.; Li, W.W. Multiple roles of COX-2 in tumor angiogenesis: A target for antiangiogenic therapy. Semin. Oncol. 2004, 31, 2–11. [Google Scholar] [CrossRef]
- Kerbel, R.S. Improving conventional or low dose metronomic chemotherapy with targeted antiangiogenic drugs. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2007, 39, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Shu, Q.; Antalffy, B.; Su, J.M.; Adesina, A.; Ou, C.N.; Pietsch, T.; Blaney, S.M.; Lau, C.C.; Li, X.N. Valproic Acid prolongs survival time of severe combined immunodeficient mice bearing intracerebellar orthotopic medulloblastoma xenografts. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2006, 12, 4687–4694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, Y.; Liu, K.W.; Wang, J.; Garancher, A.; Tao, R.; Esparza, L.A.; Maier, D.L.; Udaka, Y.T.; Murad, N.; Morrissy, S.; et al. HDAC and PI3K Antagonists Cooperate to Inhibit Growth of MYC-Driven Medulloblastoma. Cancer Cell 2016, 29, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenberghe, E.A.; Mecucci, C.; Delannoy, A.; Van den Berghe, H. Deletion of 5q by t(5;17) in therapy-related myelodysplastic syndrome. Cancer Genet. Cytogenet. 1990, 48, 49–52. [Google Scholar] [CrossRef]
- Merchant, T.E.; Bendel, A.E.; Sabin, N.D.; Burger, P.C.; Shaw, D.W.; Chang, E.; Wu, S.; Zhou, T.; Eisenstat, D.D.; Foreman, N.K.; et al. Conformal Radiation Therapy for Pediatric Ependymoma, Chemotherapy for Incompletely Resected Ependymoma, and Observation for Completely Resected, Supratentorial Ependymoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 974–983. [Google Scholar] [CrossRef] [Green Version]
- Esbenshade, A.J.; Kocak, M.; Hershon, L.; Rousseau, P.; Decarie, J.C.; Shaw, S.; Burger, P.; Friedman, H.S.; Gajjar, A.; Moghrabi, A. A Phase II feasibility study of oral etoposide given concurrently with radiotherapy followed by dose intensive adjuvant chemotherapy for children with newly diagnosed high-risk medulloblastoma (protocol POG 9631): A report from the Children’s Oncology Group. Pediatric Blood Cancer 2017, 64, e26373. [Google Scholar] [CrossRef]
- Michalski, J.M.; Janss, A.J.; Vezina, L.G.; Smith, K.S.; Billups, C.A.; Burger, P.C.; Embry, L.M.; Cullen, P.L.; Hardy, K.K.; Pomeroy, S.L.; et al. Children’s Oncology Group Phase III Trial of Reduced-Dose and Reduced-Volume Radiotherapy With Chemotherapy for Newly Diagnosed Average-Risk Medulloblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 2685–2697. [Google Scholar] [CrossRef]
- Seif, A.E.; Naranjo, A.; Baker, D.L.; Bunin, N.J.; Kletzel, M.; Kretschmar, C.S.; Maris, J.M.; McGrady, P.W.; von Allmen, D.; Cohn, S.L.; et al. A pilot study of tandem high-dose chemotherapy with stem cell rescue as consolidation for high-risk neuroblastoma: Children’s Oncology Group study ANBL00P1. Bone Marrow Transplant. 2013, 48, 947–952. [Google Scholar] [CrossRef]
- Slavc, I.; Peyrl, A.; Gojo, J.; Holm, S.; Blomgren, K.; Sehested, A.M.; Leblond, P.; Czech, T. MBCL-43. Recurrent Medulloblastoma—Long-term survival with a “MEMMAT” based antiangiogenic approach. Neuro-Oncol. 2020, 22, iii397. [Google Scholar] [CrossRef]
- Corbacioglu, S.; Steinbach, D.; Lode, H.; Gruhn, B.; Fruehwald, M.; Broeckelmann, M. The RIST design: A molecularly targeted multimodal approach for the treatment of patients with relapsed and refractory neuroblastoma. J. Clin. Oncol. 2013, 31, 10017. [Google Scholar] [CrossRef]
- Sun, X.; Zhen, Z.; Guo, Y.; Gao, Y.; Wang, J.; Zhang, Y.; Zhu, J.; Lu, S.; Sun, F.; Huang, J.; et al. Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies. Cancers 2021, 13, 3494. [Google Scholar] [CrossRef] [PubMed]
- Carcamo, B.; Bista, R.; Wilson, H.; Reddy, P.; Pacheco, J. Rapid Response to Lorlatinib in a Patient With TFG-ROS1 Fusion Positive Inflammatory Myofibroblastic Tumor of the Chest Wall Metastatic to the Brain and Refractory to First and Second Generation ROS1 Inhibitors. J. Pediatric Hematol. Oncol. 2021, 43, e718–e722. [Google Scholar] [CrossRef] [PubMed]
- Hartman, L.L.R.; Oaxaca, D.M.; Carcamo, B.; Wilson, H.L.; Ross, J.A.; Robles-Escajeda, E.; Kirken, R.A. Integration of a Personalized Molecular Targeted Therapy into the Multimodal Treatment of Refractory Childhood Embryonal Tumor with Multilayered Rosettes (ETMR). Case Rep. Oncol. 2019, 12, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Doloff, J.C.; Waxman, D.J. VEGF receptor inhibitors block the ability of metronomically dosed cyclophosphamide to activate innate immunity-induced tumor regression. Cancer Res. 2012, 72, 1103–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francia, G.; Emmenegger, U.; Lee, C.R.; Shaked, Y.; Folkins, C.; Mossoba, M.; Medin, J.A.; Man, S.; Zhu, Z.; Witte, L.; et al. Long-term progression and therapeutic response of visceral metastatic disease non-invasively monitored in mouse urine using beta-human choriogonadotropin secreting tumor cell lines. Mol. Cancer Ther. 2008, 7, 3452–3459. [Google Scholar] [CrossRef] [Green Version]
- Tang, T.C.; Man, S.; Xu, P.; Francia, G.; Hashimoto, K.; Emmenegger, U.; Kerbel, R.S. Development of a resistance-like phenotype to sorafenib by human hepatocellular carcinoma cells is reversible and can be delayed by metronomic UFT chemotherapy. Neoplasia 2010, 12, 928–940. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.J.; Singleton, W.G.; Lowis, S.P.; Malik, K.; Kurian, K.M. Therapeutic Targeting of Histone Modifications in Adult and Pediatric High-Grade Glioma. Front. Oncol. 2017, 7, 45. [Google Scholar] [CrossRef] [Green Version]
- Browder, T.; Butterfield, C.E.; Kraling, B.M.; Shi, B.; Marshall, B.; O’Reilly, M.S.; Folkman, J. Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res. 2000, 60, 1878–1886. [Google Scholar]
- Shaked, Y.; Ciarrocchi, A.; Franco, M.; Lee, C.R.; Man, S.; Cheung, A.M.; Hicklin, D.J.; Chaplin, D.; Foster, F.S.; Benezra, R.; et al. Therapy-induced acute recruitment of circulating endothelial progenitor cells to tumors. Science 2006, 313, 1785–1787. [Google Scholar] [CrossRef]
- Emmenegger, U.; Francia, G.; Chow, A.; Shaked, Y.; Kouri, A.; Man, S.; Kerbel, R.S. Tumors that acquire resistance to low-dose metronomic cyclophosphamide retain sensitivity to maximum tolerated dose cyclophosphamide. Neoplasia (New York N.Y.) 2011, 13, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Klement, G.; Baruchel, S.; Rak, J.; Man, S.; Clark, K.; Hicklin, D.J.; Bohlen, P.; Kerbel, R.S. Continuous low-dose therapy with vinblastine and VEGF receptor-2 antibody induces sustained tumor regression without overt toxicity. J. Clin. Investig. 2000, 105, R15–R24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochlitz, C.; von Moos, R.; Bigler, M.; Zaman, K.; Anchisi, S.; Küng, M.; Jae Na, K.; Baertschi, D.; Borner, M.M.; Rordorf, T.; et al. SAKK 24/09: Safety and tolerability of bevacizumab plus paclitaxel versus bevacizumab plus metronomic cyclophosphamide and capecitabine as first-line therapy in patients with HER2-negative advanced stage breast cancer—A multicenter, randomized phase III trial. J. Clin. Oncol. 2014, 32, 518. [Google Scholar]
- Traore, F.; Togo, B.; Pasquier, E.; Dembele, A.; Andre, N. Preliminary evaluation of children treated with metronomic chemotherapy and valproic acid in a low-income country: Metro-Mali-02. Indian J. Cancer 2013, 50, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Pramanik, R.; Agarwala, S.; Sreenivas, V.; Dhawan, D.; Bakhshi, S. Quality of life in paediatric solid tumours: A randomised study of metronomic chemotherapy versus placebo. BMJ Supportive Palliat. Care 2021. [Google Scholar] [CrossRef]
- Qayed, M.; Cash, T.; Tighiouart, M.; MacDonald, T.J.; Goldsmith, K.C.; Tanos, R.; Kean, L.; Watkins, B.; Suessmuth, Y.; Wetmore, C.; et al. A phase I study of sirolimus in combination with metronomic therapy (CHOAnome) in children with recurrent or refractory solid and brain tumors. Pediatric Blood Cancer 2020, 67, e28134. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Diagnosis | Regimen | Age at Initial Diagnosis | Best Response | Clinical Course |
|---|---|---|---|---|---|
| 1 | Rhabdoid tumor of the kidney (RTK) with lung and BM metastasis. Malignant myeloid clone at end of primary treatment. RTK relapse to bone marrow +/− lungs. | VP16-CTX, Celecoxib, VA | 34 months | CR | Developed Treatment-related myeloid neoplasia and died from BMT complications in CR. CR 18 months at death. OS 3 years |
| 2 | Supratentorial Anaplastic Ependymoma. Local and distant relapse to spine. | VP16-CTX, Celecoxib, VA | 6 years | CR | CR 5.5 years at last encounter Alive 8 years at last encounter |
| 3 | Medulloblastoma Infratentorial Microscopic leptomeningeal relapse | VP16 alone (VA added later) | 10 months | CR | CR 5 years at last encounter Alive 7 years at last encounter |
| 4 | Medulloblastoma Infratentorial Second relapse | TMZ-CTX, VA, Celecoxib (TMZ changed to VP later) | 5 years | PR | PR at 8 months lasted 2 months. Died of disease at 12 months |
| 5 | Metastatic neuroblastoma Retroperitoneal relapse | VP16-CTX, Sulindac (Sulindac changed to Celecoxib later) | 9 years | PR | PR at 5 months lasted 6 months. Died of upper GI bleeding at 13 months. |
| 6 | Spinal cord neurocytoma Unresectable progressive tumor. | TMZ-CTX, VA, BV, Celecoxib | 3 years | PR | PR at 3 months. Treatment stopped after 4 years of stable disease. PD 10 months later. She remains AWD on treatment |
| Study | Metronomic Regimen |
|---|---|
| Kieran 2005 [10] | Thalidomide 3 mg/kg oral daily days 1–42, |
| Celecoxib 100–400 mg bid oral days 1–42 | |
| VP-16 50 mg/m2/day oral days 1–21 | |
| CTX 2.5 mg/kg/day to a maximum of 100 mg oral days 22–42. | |
| Kieran 2014 [9] | Celecoxib 100–400 mg bid oral days 1–42 |
| Thalidomide 3 mg/kg oral daily days 1–42, | |
| Fenofibrate 90 mg/m2 oral daily | |
| CTX 2.5 mg/kg/day to a max of 100 mg per day) days 1–21 | |
| VP16 50 mg/m2/day days 22–42 | |
| Andre et al. 2008 [13] | VP-16 25 mg/m2/day days 1–14 |
| CTX 25 mg/m2/day days 15–28 | |
| Celecoxib 100–400 mg/day days 1–28 | |
| MEMMAT Slavc et al. 2020 [39] | Etoposide 35–50 mg/m2/day oral on days 1–21 of 42 day cycles |
| CTX 2.5 mg/kg/day oral on days 22–42 of 42 day cycles | |
| Intrathecal Liposomal cytarabine 16–30 mg days 1, 4, 8, 11 of 28-day cycles | |
| Intrathecal VP16 0.5 mg days 18, 19, 20, 21, 21 of 28-day cycles. | |
| Bevacizumab 10 mg/kg IV every other week | |
| Thalidomide 3 mg/kg daily 1 year | |
| Celecoxib 50–400 mg oral daily 1 year | |
| Fenofibrate 90 mg/m2 oral daily 1 year | |
| Sun et al. 2021 [41] | VP16 25 mg/m2 oral days 1–21 of 56–day cycles |
| Topotecan 1.4 mg/m2 oral daily on days 29–33 of 56-day cycles | |
| CTX 25–50 mg/m2 oral daily days 1–56 of 56-day cycles. | |
| Vinorelbine 40 mg/m2 oral weekly weeks 1–3 every 4 weeks | |
| Celecoxib 200 mg/m2 oral twice a day 1 year | |
| This manuscript | VP-16 50 mg/m2/day days 1–21 |
| CTX 2.5 mg/kg/day days 22–42 | |
| Celecoxib 250 mg/m2/dose twice a day days 1–42 | |
| Valproic acid 7.5 mg/kg/dose twice a day days 1–42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carcamo, B.; Francia, G. Cyclic Metronomic Chemotherapy for Pediatric Tumors: Six Case Reports and a Review of the Literature. J. Clin. Med. 2022, 11, 2849. https://doi.org/10.3390/jcm11102849
Carcamo B, Francia G. Cyclic Metronomic Chemotherapy for Pediatric Tumors: Six Case Reports and a Review of the Literature. Journal of Clinical Medicine. 2022; 11(10):2849. https://doi.org/10.3390/jcm11102849
Chicago/Turabian StyleCarcamo, Benjamin, and Giulio Francia. 2022. "Cyclic Metronomic Chemotherapy for Pediatric Tumors: Six Case Reports and a Review of the Literature" Journal of Clinical Medicine 11, no. 10: 2849. https://doi.org/10.3390/jcm11102849
APA StyleCarcamo, B., & Francia, G. (2022). Cyclic Metronomic Chemotherapy for Pediatric Tumors: Six Case Reports and a Review of the Literature. Journal of Clinical Medicine, 11(10), 2849. https://doi.org/10.3390/jcm11102849