
Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Inclusion Criteria and Variables
2.3. Statistical Analysis
3. Results
3.1. Normal Weight vs. Overweight Patients
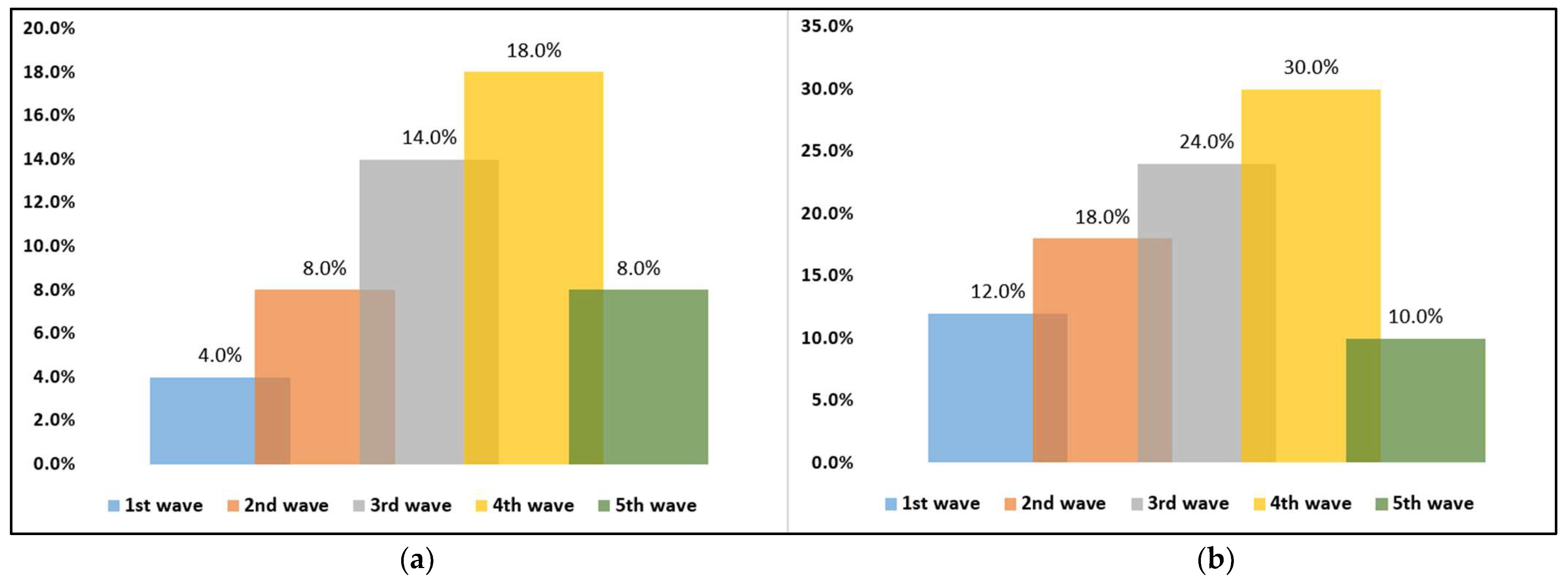
3.2. Dynamic Comparison of COVID-19 Pandemic Waves

{kind=link}
{kind=link}
| 1st Wave (n = 50) | 2nd Wave (n = 50) | 3rd Wave (n = 50) | 4th Wave (n = 50) | 5th Wave (n = 50) | p-Value * | |
|---|---|---|---|---|---|---|
| Severe COVID-19 | 7 (14.0%) | 15 (30.0%) | 12 (24.0%) | 20 (40.0%) | 7 (14.0%) | 0.004 |
| Severe imaging features | 8 (16.0%) | 15 (30.0%) | 13 (26.0%) | 21 (42.0%) | 9 (18.0%) | 0.012 |
| Oxygen saturation on admission (<92%) | 6 (12.0%) | 11 (22.0%) | 18 (36.0%) | 21 (42.0%) | 7 (14.0%) | 0.001 |
| Respiratory rate on admission (>20/min) | 9 (18.0%) | 14 (28.0%) | 22 (44.0%) | 26 (52.0%) | 12 (52.0%) | 0.001 |
| Heart rate on admission (>100 bpm) | 12 (24.0%) | 20 (40.0%) | 27 (54.0%) | 33 (66.0%) | 15 (30.0%) | 0.025 |
| Duration of hospital stay | 14 (11–18) | 9 (7–12) | 18 (11–23) | 21 (13–25) | 9 (7–13) | <0.001 |
| Duration from symptom onset until hospital admission | 2 (1–4) | 5 (2.2–8.3) | 6 (2.3–9.2) | 6 (2.1–9.0) | 5 (1.9–7.4) | <0.001 |
| Viral clearance | 8 (3–13) | 12 (4–16) | 15 (7–21) | 17 (11–23) | 9 (4–15) | <0.001 |
| ICU admission | 6 (12.0%) | 9 (18.0%) | 12 (24.0%) | 15 (30.0%) | 5 (10.0%) | 0.002 |
| Duration of ICU stay | 7 (3–11) | 12 (4–15) | 12 (5–16) | 14 (9–19) | 9 (4–12) | 0.009 |
| Severe in-hospital complications | 6 (12.0%) | 9 (18.0%) | 12 (24.0%) | 14 (30.0%) | 5 (10.0%) | 0.021 |
| Oxygen supplementation | 22 (44.0%) | 27 (54.0%) | 37 (74.0%) | 45 (90.0%) | 17 (34.0%) | <0.001 |
| Mortality | 2 (4.0%) | 4 (8.0%) | 7 (14.0%) | 9 (18.0%) | 4 (8.0%) | 0.001 |
| COVID-19 treatment | ||||||
| Antivirals | 50 (100%) | 50 (100%) | 46 (92.0%) | 48 (96.0%) | 45 (90.0%) | 0.693 |
| Corticosteroids | 46 (92.0%) | 43 (86.0%) | 44 (88.0%) | 40 (80.0%) | 38 (76.0%) | 0.184 |
| Antibiotics | 47 (94.0%) | 48 (96.0%) | 42 (84.0%) | 40 (80.0%) | 37 (74.0%) | 0.007 |
| Anticoagulant | 39 (78.0%) | 38 (76.0%) | 36 (72.0%) | 38 (76.0%) | 32 (64.0%) | 0.528 |
| Immune modulators | 0 (0.0%) | 0 (0.0%) | 28 (56.0%) | 29 (58.0%) | 26 (52.0%) | 0.827 |
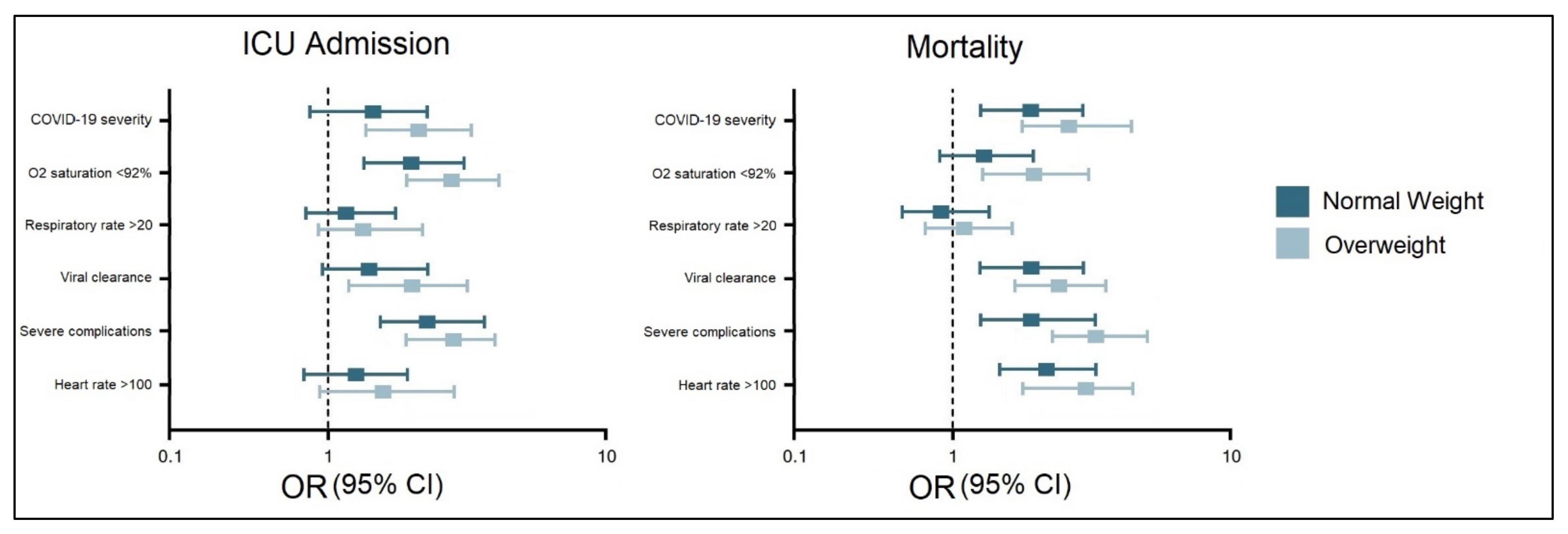
3.3. Risk Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, L.; Wang, K.; Zhong, H.; Zhao, N.; Xu, W.; Yang, Y.; He, Y.; Liu, S. The Effect of Coronavirus 2019 Disease Control Measures on the Incidence of Respiratory Infectious Disease and Air Pollutant Concentrations in the Yangtze River Delta Region, China. Int. J. Environ. Res. Public Health 2022, 19, 1286. [Google Scholar] [CrossRef] [PubMed]
- Cerbu, B.; Pantea, S.; Bratosin, F.; Vidican, I.; Turaiche, M.; Frent, S.; Borsi, E.; Marincu, I. Liver Impairment and Hematological Changes in Patients with Chronic Hepatitis C and COVID-19: A Retrospective Study after One Year of Pandemic. Medicina 2021, 57, 597. [Google Scholar] [CrossRef] [PubMed]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef] [PubMed]
- Farrag, M.A.; Amer, H.M.; Bhat, R.; Hamed, M.E.; Aziz, I.M.; Mubarak, A.; Dawoud, T.M.; Almalki, S.G.; Alghofaili, F.; Alnemare, A.K.; et al. SARS-CoV-2: An Overview of Virus Genetics, Transmission, and Immunopathogenesis. Int. J. Environ. Res. Public Health 2021, 18, 6312. [Google Scholar] [CrossRef]
- Kayode, A.J.; Banji-Onisile, F.O.; Olaniran, A.O.; Okoh, A.I. An Overview of the Pathogenesis, Transmission, Diagnosis, and Management of Endemic Human Coronaviruses: A Reflection on the Past and Present Episodes and Possible Future Outbreaks. Pathogens 2021, 10, 1108. [Google Scholar] [CrossRef]
- Salleh, M.Z.; Deris, Z.Z. In Silico Molecular Characterization of Human TMPRSS2 Protease Polymorphic Variants and Associated SARS-CoV-2 Susceptibility. Life 2022, 12, 231. [Google Scholar] [CrossRef]
- Pilut, C.N.; Citu, C.; Gorun, F.; Bratosin, F.; Gorun, O.M.; Burlea, B.; Citu, I.M.; Grigoras, M.L.; Manolescu, D.; Gluhovschi, A. The Utility of Laboratory Parameters for Cardiac Inflammation in Heart Failure Patients Hospitalized with SARS-CoV-2 Infection. Diagnostics 2022, 12, 824. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Neamtu, R.; Motoc, A.; Burlea, B.; Rosca, O.; Bratosin, F.; Hosin, S.; Manolescu, D.; et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. J. Clin. Med. 2022, 11, 1382. [Google Scholar] [CrossRef]
- Bean, D.M.; Kraljevic, Z.; Searle, T.; Bendayan, R.; Kevin, O.; Pickles, A.; Folarin, A.; Roguski, L.; Noor, K.; Shek, A.; et al. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are not associated with severe COVID-19 infection in a multi-site UK acute hospital trust. Eur. J. Heart Fail. 2020, 22, 967–974. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Tirnea, L.; Avram, V.; Marincu, I. Exploring Pregnancy Outcomes Associated with SARS-CoV-2 Infection. Medicina 2021, 57, 796. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Tomescu, L.; Neamtu, R.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; et al. Immunogenicity Following Administration of BNT162b2 and Ad26.COV2.S COVID-19 Vaccines in the Pregnant Population during the Third Trimester. Viruses 2022, 14, 307. [Google Scholar] [CrossRef]
- Snider, B.; Patel, B.; McBean, E. Asymptomatic Cases, the Hidden Challenge in Predicting COVID-19 Caseload Increases. Infect. Dis. Rep. 2021, 13, 340–347. [Google Scholar] [CrossRef]
- Brandi, N.; Ciccarese, F.; Rimondi, M.R.; Balacchi, C.; Modolon, C.; Sportoletti, C.; Renzulli, M.; Coppola, F.; Golfieri, R. An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review. Diagnostics 2022, 12, 846. [Google Scholar] [CrossRef]
- Vîjîiac, A.; Stănciulescu, D.I.; Băetu, A.E.; Grigore, I.-A.; Vintilă, D.; Cojocaru, C.; Bădilă, E.; Moldovan, H.; Scafa-Udriște, A. The Impact of COVID-19 Era on Pulmonary Embolism Patients: Increased Incidence of Hospitalizations and Higher Mortality—What Can Be Done? COVID 2021, 1, 357–365. [Google Scholar] [CrossRef]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. A review of the 2019 novel coronavirus (COVID-19) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef]
- Sorbello, M.; El-Boghdadly, K.; Di Giacinto, I.; Cataldo, R.; Esposito, C.; Falcetta, S.; Merli, G.; Cortese, G.; Corso, R.M.; Bressan, F.; et al. The Italian coronavirus disease 2019 outbreak: Recommendations from clinical practice. Anaesthesia 2020, 75, 724–732. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Giudice, V.; Iannaccone, T.; Faiella, F.; Ferrara, F.; Aversano, G.; Coppola, S.; De Chiara, E.; Romano, M.G.; Conti, V.; Filippelli, A. Gender Differences in the Impact of COVID-19 Pandemic on Mental Health of Italian Academic Workers. J. Pers. Med. 2022, 12, 613. [Google Scholar] [CrossRef]
- Soriano, V.; Ganado-Pinilla, P.; Sanchez-Santos, M.; Gómez-Gallego, F.; Barreiro, P.; de Mendoza, C.; Corral, O. Main differences between the first and second waves of COVID-19 in Madrid, Spain. Int. J. Infect. Dis. 2021, 105, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A.R.; Fergusson, N.A.; Lloyd-Smith, E.; Wormsbecker, A.; Foster, D.; Karpov, A.; Crowe, S.; Haljan, G.; Chittock, D.R.; Kanji, H.D.; et al. Baseline characteristics and outcomes of patients with COVID-19 admitted to intensive care units in Vancouver, Canada: A case series. Can. Med. Assoc. J. 2020, 192, E694–E701. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Wilk-Sledziewska, K.; Sielatycki, P.J.; Uscinska, N.; Bujno, E.; Rosolowski, M.; Kakareko, K.; Sledziewski, R.; Rydzewska-Rosolowska, A.; Hryszko, T.; Zbroch, E. The Impact of Cardiovascular Risk Factors on the Course of COVID-19. J. Clin. Med. 2022, 11, 2250. [Google Scholar] [CrossRef]
- Gutierrez-Camacho, J.R.; Avila-Carrasco, L.; Murillo-Ruíz-Esparza, A.; Garza-Veloz, I.; Araujo-Espino, R.; Martinez-Vazquez, M.C.; Trejo-Ortiz, P.M.; Rodriguez-Sanchez, I.P.; Delgado-Enciso, I.; Castañeda-López, M.E.; et al. Evaluation of the Potential Risk of Mortality from SARS-CoV-2 Infection in Hospitalized Patients According to the Charlson Comorbidity Index. Healthcare 2022, 10, 362. [Google Scholar] [CrossRef]
- Silveira, E.A.; de Souza Rosa, L.P.; de Carvalho Santos, A.S.e.A.; de Souza Cardoso, C.K.; Noll, M. Type 2 Diabetes Mellitus in Class II and III Obesity: Prevalence, Associated Factors, and Correlation between Glycemic Parameters and Body Mass Index. Int. J. Environ. Res. Public Health 2020, 17, 3930. [Google Scholar] [CrossRef]
- Arias, A.; Rodríguez-Álvarez, C.; González-Dávila, E.; Acosta-Torrecilla, A.; Novo-Muñoz, M.M.; Rodríguez-Novo, N. Arterial Hypertension in Morbid Obesity after Bariatric Surgery: Five Years of Follow-Up, a Before-And-After Study. Int. J. Environ. Res. Public Health 2022, 19, 1575. [Google Scholar] [CrossRef]
- Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 3 April 2022).
- Sanyaolu, A.; Okorie, C.; Qi, X.; Locke, J.; Rehman, S. Childhood and Adolescent Obesity in the United States: A Public Health Concern. Glob. Pediatr. Health 2019, 6, 2333794X19891305. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Beydoun, M.A.; Min, J.; Xue, H.; Kaminsky, L.A.; Cheskin, L.J. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int. J. Epidemiol. 2020, 49, 810–823. [Google Scholar] [CrossRef]
- Haase, C.L.; Eriksen, K.T.; Lopes, S.; Satylganova, A.; Schnecke, V.; McEwan, P. Body mass index and risk of obesity-related conditions in a cohort of 2.9 million people: Evidence from a UK primary care database. Obes. Sci. Pract. 2020, 7, 137–147. [Google Scholar] [CrossRef]
- Agha, M.; Agha, R. The rising prevalence of obesity: Part A: Impact on public health. Int. J. Surg. Oncol. 2017, 2, e17. [Google Scholar] [CrossRef] [Green Version]
- Cai, Z.; Yang, Y.; Zhang, J. Obesity is associated with severe disease and mortality in patients with coronavirus disease 2019 (COVID-19): A meta-analysis. BMC Public Health 2021, 21, 1505. [Google Scholar] [CrossRef]
- Al-Benna, S. Association of high-level gene expression of ACE2 in adipose tissue with mortality of COVID-19 infection in obese patients. Obes. Med. 2020, 19, 100283. [Google Scholar] [CrossRef]
- Dixon, A.E.; Peters, U. The effect of obesity on lung function. Expert Rev. Respir. Med. 2018, 12, 755–767. [Google Scholar] [CrossRef]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, A.V.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and metabolic disease: Mechanisms and clinical management. Lancet Diabetes Endocrinol. 2021, 9, 786–798. [Google Scholar] [CrossRef]
- Ganji, R.; Reddy, P.H. Impact of COVID-19 on Mitochondrial-Based Immunity in Aging and Age-Related Diseases. Front. Aging Neurosci. 2021, 12, 614650. [Google Scholar] [CrossRef]
- Lazar, M.; Sequencing of the SARS-CoV-2 Virus Genome in Romania. National Institute of Medical-Military Research and Development “Cantacuzino”. Available online: https://cantacuzino.mapn.ro/pages/view/249 (accessed on 3 April 2022).
- Hodcroft, E.B.; Zuber, M.; Nadeau, S.; Vaughan, T.G.; Crawford, K.H.D.; Althaus, C.L.; Reichmuth, M.L.; Bowen, J.E.; Walls, A.C.; Corti, D.; et al. Spread of a SARS-CoV-2 variant through Europe in the summer of 2020. Nature 2021, 595, 707–712. [Google Scholar] [CrossRef]
- National Institute of Public Health. Epidemiological Analysis of the First 136 COVID-19 Cases in Romania Confirmed with New Variants of SARS-CoV-2. Available online: https://www.cnscbt.ro/index.php/analiza-cazuri-confirmate-covid19/2291-cazuri-covid-19-cu-noi-variante-analiza-epidemiologica-a-primelor-136-cazuri/file (accessed on 3 April 2022).
- National Committee for Coordination of Activities on Vaccination against COVID-19. What We Need to Know about the Delta Variant of the SARS-CoV-2 Virus. Available online: https://vaccinare-covid.gov.ro/wp-content/uploads/2021/07/Varianta-Delta-informare-de-presa-07.07.2021-1.pdf (accessed on 3 April 2022).
- Ministry of Health in Romania. Update of Infection Cases with the OMICRON Strain of SARS-CoV-2 Virus. Available online: https://www.ms.ro/2022/01/05/update-cazuri-de-infectare-cu-tulpina-omicron-a-virusului-sars-cov-2-2/ (accessed on 3 April 2022).
- Legislative Portal. Order no. 533 of 22 April 22 2021 on the Amendment of the Annex to the Order of the Minister of Health No. 487/2020 for the Approval of the Protocol for the Treatment of SARS-CoV-2 Virus Infection. Romanian Ministry of Health. Available online: https://www.dsptimis.ro/data_files/content/legislatie-covid/files/ordin-nr-533-27-04-2021.pdf (accessed on 3 April 2022).
- Liang, S.T.; Liang, L.T.; Rosen, J.M. COVID-19: A comparison to the 1918 influenza and how we can defeat it. Postgrad. Med. J. 2021, 97, 273–274. [Google Scholar] [CrossRef]
- Cacciapaglia, G.; Cot, C.; Sannino, F. Multiwave pandemic dynamics explained: How to tame the next wave of infectious diseases. Sci. Rep. 2021, 11, 6638. [Google Scholar] [CrossRef]
- Hâncean, M.G.; Perc, M.; Lerner, J. Early spread of COVID-19 in Romania: Imported cases from Italy and human-to-human transmission networks. R. Soc. Open Sci. 2020, 7, 200780. [Google Scholar] [CrossRef]
- Zhou, T.; Liu, Q.; Yang, Z.; Liao, J.; Yang, K.; Bai, W.; Lu, X.; Zhang, W. Preliminary prediction of the basic reproduction number of the Wuhan novel coronavirus 2019-nCoV. J. Evid. Based Med. 2020, 13, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Seong, H.; Hyun, H.J.; Yun, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Song, J.Y. Comparison of the second and third waves of the COVID-19 pandemic in South Korea: Importance of early public health intervention. Int. J. Infect. Dis. 2021, 104, 742–745. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Sawadogo, W.; Tsegaye, M.; Gizaw, A.; Adera, T. Overweight and obesity as risk factors for COVID-19-associated hospitalisations and death: Systematic review and meta-analysis. BMJ Nutr. Prev. Health 2022, e000375. [Google Scholar] [CrossRef]
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Abdool Karim, S.S.; Sridhar, D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef]
- Townsend, J.P.; Hassler, H.B.; Wang, Z.; Miura, S.; Singh, J.; Kumar, S.; Ruddle, N.H.; Galvani, A.P.; Dornburg, A. The durability of immunity against reinfection by SARS-CoV-2: A comparative evolutionary study. Lancet Microbe 2021, 2, e666–e675. [Google Scholar] [CrossRef]
- Lazarevic, I.; Pravica, V.; Miljanovic, D.; Cupic, M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt So Far? Viruses 2021, 13, 1192. [Google Scholar] [CrossRef]
- Diarra, M.; Kebir, A.; Talla, C.; Barry, A.; Faye, J.; Louati, D.; Opatowski, L.; Diop, M.; White, L.J.; Loucoubar, C. Non-pharmaceutical interventions and COVID-19 vaccination strategies in Senegal: A modelling study. BMJ Glob. Health 2022, 7, e007236. [Google Scholar] [CrossRef]
- Kovács, G.; Kaló, Z.; Jahnz-Rozyk, K.; Kyncl, J.; Csohan, A.; Pistol, A.; Leleka, M.; Kipshakbaev, R.; Durand, L.; Macabeo, B. Medical and economic burden of influenza in the elderly population in central and eastern European countries. Hum. Vaccin. Immunother. 2014, 10, 428–440. [Google Scholar] [CrossRef] [Green Version]


| Variables * | BMI 18.5–24.9 (n = 113) | BMI > 24.9 (n = 250) | p-Value |
|---|---|---|---|
| Background data | |||
| Age | 0.407 | ||
| 18–40 years | 21 (18.6%) | 33 (13.2%) | |
| 40–65 years | 54 (47.8%) | 129 (51.6%) | |
| >65 years | 38 (33.6%) | 88 (35.2%) | |
| Gender (men) | 62 (54.9%) | 137 (54.8%) | 0.990 |
| Area of residence (urban) | 68 (60.2%) | 143 (57.2%) | 0.594 |
| Occupation (employed) | 66 (58.4%) | 124 (49.6%) | 0.119 |
| Smoking | 43 (38.1%) | 129 (51.6%) | 0.016 |
| Alcohol use disorder | 9 (8.0%) | 17 (6.8%) | 0.690 |
| Comorbidities | |||
| Malignancy | 7 (6.2%) | 26 (10.4%) | 0.196 |
| Chronic lung disease | 11 (9.7%) | 39 (15.6%) | 0.133 |
| Cardiovascular disease | 51 (45.1%) | 114 (45.6%) | 0.934 |
| Cerebrovascular disease | 8 (7.1%) | 33 (13.2%) | 0.088 |
| Diabetes mellitus | 14 (12.4%) | 56 (22.4%) | 0.025 |
| Autoimmune disease | 3 (2.7%) | 12 (4.8%) | 0.341 |
| Chronic kidney disease | 4 (3.5%) | 14 (5.6%) | 0.402 |
| Digestive and liver disease | 11 (9.7%) | 51 (20.4%) | 0.012 |
| COVID-19 treatment | |||
| Antivirals | 103 (91.2%) | 239 (95.6%) | 0.092 |
| Corticosteroids | 99 (87.6%) | 211 (84.4%) | 0.422 |
| Antibiotics | 87 (77.0%) | 214 (85.6%) | 0.043 |
| Anticoagulants | 75 (66.4%) | 183 (73.2%) | 0.184 |
| Immune modulators | 28 (24.8%) | 83 (33.2%) | 0.106 |
| Variables * | Normal Range | BMI 18.5–24.9 (n = 113) | BMI > 24.9 (n = 250) | p-Value |
|---|---|---|---|---|
| RBC (millions/mm3) | 4.35–5.65 | 61 (54.0%) | 164 (65.6%) | 0.034 |
| WBC (thousands/mm3) | 4.5–11.0 | 68 (60.2%) | 179 (71.6%) | 0.030 |
| Hemoglobin (g/dL) | 13.0–17.0 | 59 (52.2%) | 155 (62.0%) | 0.079 |
| Hematocrit (%) | 36–48 | 31 (27.4%) | 123 (49.2%) | <0.001 |
| Platelets (thousands/mm3) | 150–450 | 38 (33.6%) | 104 (41.6%) | 0.149 |
| Ferritin (ng/mL) | 20–250 | 33 (29.2%) | 96 (38.4%) | 0.090 |
| ESR (mm/h) | 0–22 mm/hr | 75 (66.4%) | 177 (70.8%) | 0.369 |
| CRP (mg/L) | 0–10 mg/L | 72 (63.7%) | 170 (68.0%) | 0.422 |
| Fibrinogen (g/L) | 2–4 g/L | 69 (61.1%) | 171 (68.4%) | 0.171 |
| Procalcitonin (ug/L) | 0–0.25 ug/L | 20 (17.7%) | 69 (27.6%) | 0.042 |
| D-dimers (ng/mL) | <250 | 13 (11.5%) | 44 (17.6%) | 0.139 |
| IL-6 (pg/mL) | 0–16 pg/mL | 32 (28.3%) | 98 (39.2%) | 0.045 |
| Variables * | BMI 18.5–24.9 (n = 113) | BMI > 24.9 (n = 250) | p-Value |
|---|---|---|---|
| Signs and Symptoms | |||
| Cough | 72 (63.7%) | 188 (75.2%) | 0.024 |
| Fever | 66 (58.4%) | 172 (68.8%) | 0.053 |
| Dyspnea | 13 (11.5%) | 56 (22.4%) | 0.014 |
| Headache | 9 (8.0%) | 42 (16.8%) | 0.024 |
| Digestive symptoms | 18 (15.9%) | 57 (22.8%) | 0.134 |
| Anosmia/ageusia | 34 (30.1%) | 81 (32.4%) | 0.661 |
| Fatigue | 82 (72.6%) | 217 (86.8%) | <0.001 |
| Myalgia/arthralgia | 36 (31.9%) | 95 (38.0%) | 0.259 |
| Dysphagia | 7 (6.2%) | 49 (19.6%) | 0.001 |
| COVID-19 Outcomes | |||
| Severe COVID-19 | 13 (11.5%) | 61 (24.4%) | 0.004 |
| Severe imaging features | 19 (16.8%) | 66 (26.4%) | 0.045 |
| Oxygen saturation on admission (<92%) | 14 (12.4%) | 63 (25.2%) | 0.005 |
| Respiratory rate on admission (>20/min) | 27 (23.9%) | 83 (33.2%) | 0.074 |
| Heart rate on admission (>100 bpm) | 35 (31.0%) | 107 (42.8%) | 0.032 |
| Duration of hospital stay | 14 (9–16) | 18 (8–25) | <0.001 |
| Duration from symptom onset until hospital admission | 5 (2–8) | 5 (1–7) | 0.319 |
| Viral clearance | 12 (7–19) | 15 (6–21) | <0.001 |
| ICU admission | 11 (9.7%) | 47 (18.8%) | 0.029 |
| Duration of ICU stay | 7 (3–14) | 11 (7–19) | <0.001 |
| Severe in-hospital complications | 11 (9.7%) | 46 (18.4%) | 0.035 |
| Oxygen supplementation | 42 (37.2%) | 148 (59.2%) | <0.001 |
| Mortality | 4 (3.5%) | 26 (10.4%) | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fericean, R.M.; Citu, C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Tudorache, E.; Oancea, C. Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves. J. Clin. Med. 2022, 11, 2916. https://doi.org/10.3390/jcm11102916
Fericean RM, Citu C, Manolescu D, Rosca O, Bratosin F, Tudorache E, Oancea C. Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves. Journal of Clinical Medicine. 2022; 11(10):2916. https://doi.org/10.3390/jcm11102916
Chicago/Turabian StyleFericean, Roxana Manuela, Cosmin Citu, Diana Manolescu, Ovidiu Rosca, Felix Bratosin, Emanuela Tudorache, and Cristian Oancea. 2022. "Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves" Journal of Clinical Medicine 11, no. 10: 2916. https://doi.org/10.3390/jcm11102916
APA StyleFericean, R. M., Citu, C., Manolescu, D., Rosca, O., Bratosin, F., Tudorache, E., & Oancea, C. (2022). Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves. Journal of Clinical Medicine, 11(10), 2916. https://doi.org/10.3390/jcm11102916