
Exploring Contraindications for Thrombolysis: Risk of Hemorrhagic Transformation and Neurological Deterioration after Thrombolysis in Mice with Recent Ischemic Stroke and Hyperglycemia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
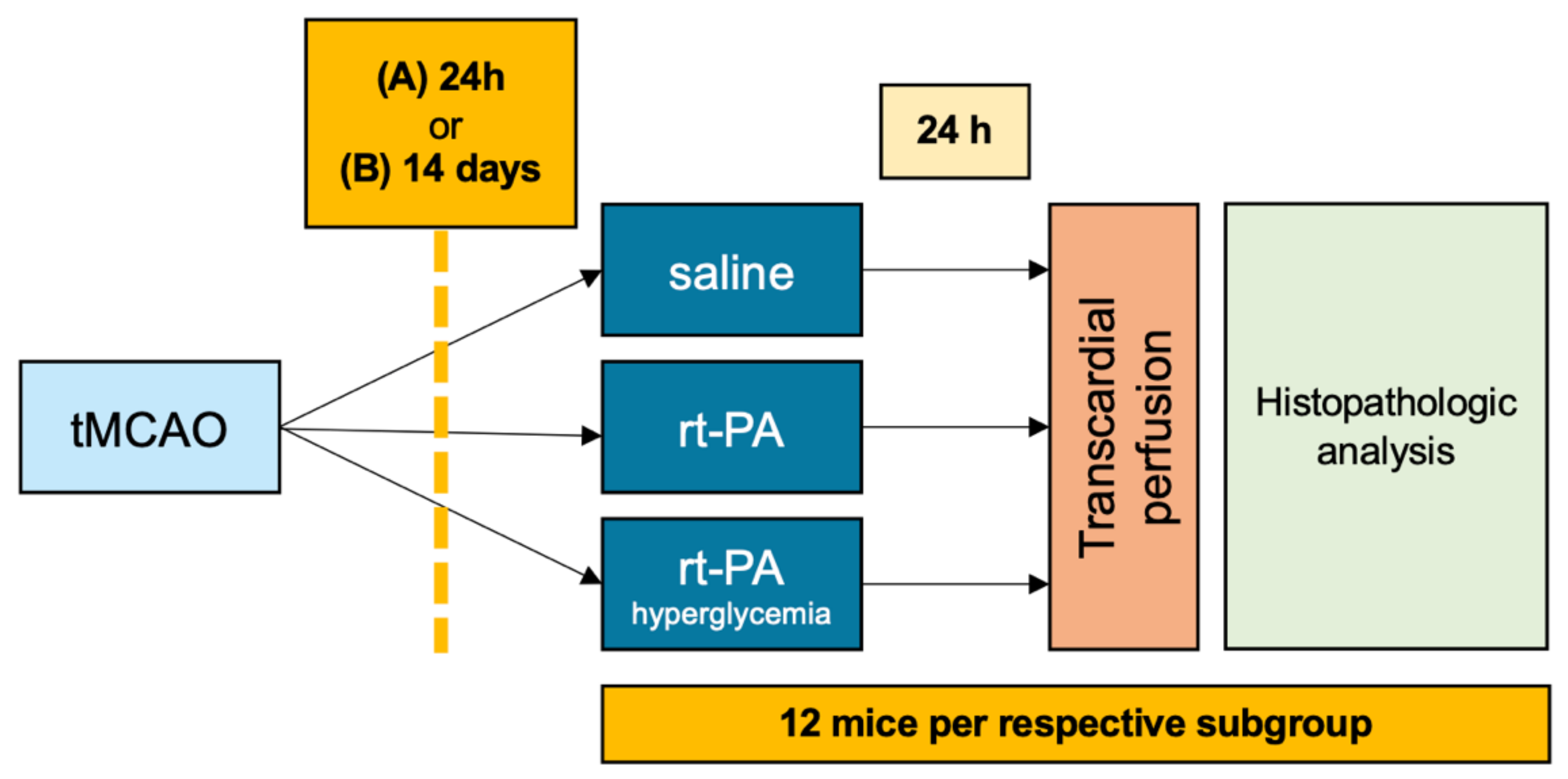
2.2. Experimental Design
2.3. Sample Size Calculation
2.4. Transient Middle Cerebral Artery Occlusion
2.5. Inducing Hyperglycemia
2.6. Quantifying the Neurological Deficit
2.7. Evaluation of Ischemic Lesion Size
2.8. Histopathological Analysis
2.9. Statistical Analyses
3. Results
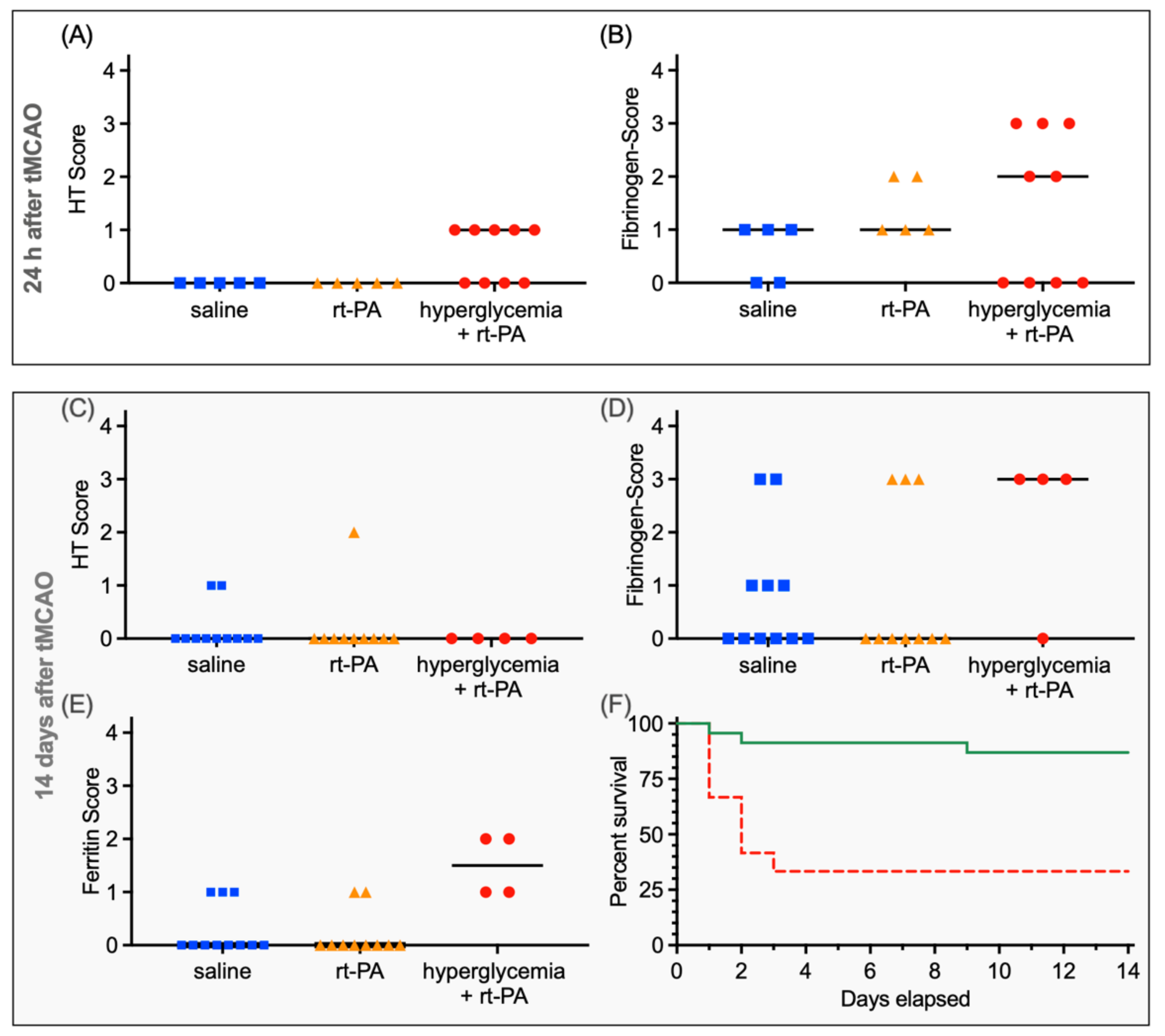
3.1. Functional Outcome and HT after Thrombolysis 24 h after Ischemic Stroke
3.2. Functional Outcome and HT after Thrombolysis 14 Days after Ischemic Stroke
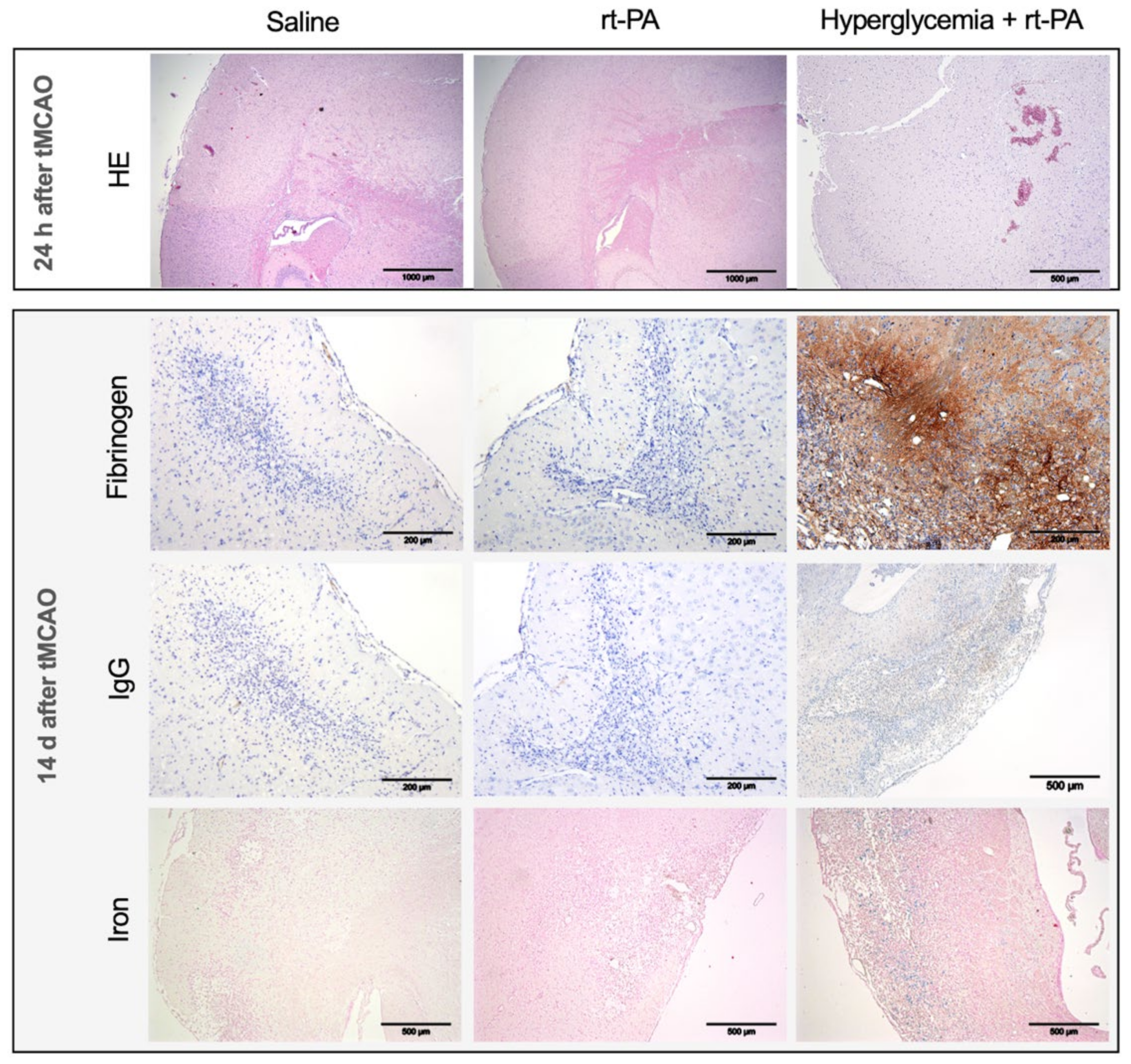
3.3. Further Histopathological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BBB | blood-brain-barrier |
| eSS | experimental Stroke Scale |
| HE | hematoxylin and eosin |
| HT | hemorrhagic transformation |
| ICH | intracerebral hemorrhage |
| IgG | immunoglobulin G |
| IQR | interquartile range |
| rt-PA | recombinant tissue plasminogen activator |
| STZ | streptozotocin |
| tMCAO | transient middle cerebral artery occlusion |
References
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S. Stroke: A global response is needed. Bull. World Health Organ. 2016, 94, 634A–635A. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001, Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke A. Stroke 2019, 50, E344–E418. [Google Scholar] [CrossRef]
- Coull, A.J.; Rothwell, P.M. Underestimation of the early risk of recurrent stroke: Evidence of the need for a standard definition. Stroke 2004, 35, 1925–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coull, A.J.; Lovett, J.K.; Rothwell, P.M. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: Implications for public education and organisation of services. Br. Med. J. 2004, 328, 326–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brass, L.M.; Lichtman, J.H.; Wang, Y. Intracranial hemorrhage associated with thrombolytic therapy for elderly patients with acute myocardial infarction: Results from the cooperative cardiovascular project. Stroke 2000, 31, 1802–1811. [Google Scholar] [CrossRef] [Green Version]
- Gurwitz, J.H.; Gore, J.M.; Goldberg, R.J.; Barron, H.V.; Breen, T.; Rundle, A.C.; Sloan, M.A.; French, W.; Rogers, W.J. Risk for intracranial hemorrhage after tissue plasminogen activator treatment for acute myocardial infarction. Ann. Intern. Med. 1998, 129, 597–604. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [Green Version]
- Laible, M.; Jenetzky, E.; Möhlenbruch, M.; Ringleb, P.A.; Rizos, T. Repeated Intravenous Treatment with Recombinant Tissue-Type Plasminogen Activator in Patients with Acute Ischemic Stroke. Eur. Neurol. 2015, 74, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Merkler, A.E.; Salehi Omran, S.; Gialdini, G.; Lerario, M.P.; Yaghi, S.; Elkind, M.S.; Navi, B.B. Safety Outcomes after Thrombolysis for Acute Ischemic Stroke in Patients with Recent Stroke. Stroke 2017, 48, 2282–2284. [Google Scholar] [CrossRef] [PubMed]
- Tisserand, M.; le Guennec, L.; Touzé, E.; Hess, A.; Charbonnier, C.; Devauchelle, A.D.; Bracard, S.; Mas, J.L.; Meder, J.F.; Oppenheim, C. Prevalence of MRI-defined recent silent ischemia and associated bleeding risk with thrombolysis. Neurology 2011, 76, 1288–1295. [Google Scholar] [CrossRef]
- Karlinski, M.; Kobayashi, A.; Czlonkowska, A.; Mikulik, R.; Vaclavik, D.; Brozman, M.; Gdovinova, Z.; Švigelj, V.; Csiba, L.; Fekete, K.; et al. Intravenous Thrombolysis for Stroke Recurring Within 3 Months from the Previous Event. Stroke 2015, 46, 3184–3189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrlich, M.E.; Liang, L.; Xu, H.; Kosinski, A.S.; Hernandez, A.F.; Schwamm, L.H.; Smith, E.E.; Fonarow, G.C.; Bhatt, D.L.; Peterson, E.D.; et al. Intravenous Tissue-Type Plasminogen Activator in Acute Ischemic Stroke Patients with History of Stroke Plus Diabetes Mellitus. Stroke 2019, 50, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Reiter, M.; Teuschl, Y.; Matz, K.; Seyfang, L.; Brainin, M. Diabetes and thrombolysis for acute stroke: A clear benefit for diabetics. Eur. J. Neurol. 2014, 21, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevationThe Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Respir. J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.; Cuthill, I.C. Editorial: Animal research: Reporting in vivo experiments-The ARRIVE Guidelines. J. Cereb. Blood Flow Metab. 2011, 31, 991–993. [Google Scholar] [CrossRef] [Green Version]
- Lourbopoulos, A.; Mamrak, U.; Roth, S.; Balbi, M.; Shrouder, J.; Liesz, A.; Hellal, F.; Plesnila, N. Inadequate food and water intake determine mortality following stroke in mice. J. Cereb. Blood Flow Metab. 2017, 37, 2084–2097. [Google Scholar] [CrossRef] [Green Version]
- Pfeilschifter, W.; Spitzer, D.; Pfeilschifter, J.; Steinmetz, H.; Foerch, C. Warfarin anticoagulation exacerbates the risk of hemorrhagic transformation after rt-PA treatment in experimental stroke: Therapeutic potential of PCC. PLoS ONE 2011, 6, e26087. [Google Scholar] [CrossRef]
- Fluri, F.; Schuhmann, M.K.; Kleinschnitz, C. Animal models of ischemic stroke and their application in clinical research. Drug Design Dev. Ther. 2015, 9, 3445–3454. [Google Scholar]
- Bohmann, F.; Mirceska, A.; Pfeilschifter, J.; Lindhoff-Last, E.; Steinmetz, H.; Foerch, C.; Pfeilschifter, W. No influence of dabigatran anticoagulation on hemorrhagic transformation in an experimental model of ischemic stroke. PLoS ONE 2012, 7, e40804. [Google Scholar] [CrossRef] [PubMed]
- Pfeilschifter, W.; Bohmann, F.; Baumgarten, P.; Mittelbronn, M.; Pfeilschifter, J.; Lindhoff-Last, E.; Steinmetz, H.; Foerch, C. Thrombolysis with recombinant tissue plasminogen activator under dabigatran anticoagulation in experimental stroke. Ann. Neurol. 2012, 71, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Rossini, A.A.; Like, A.A.; Chick, W.L.; Appel, M.C.; Cahill, G.F. Studies of streptozotocin induced insulitis and diabetes. Proc. Natl. Acad. Sci. USA 1977, 74, 2485–2489. [Google Scholar] [CrossRef] [Green Version]
- Tesch, G.H.; Allen, T.J. Rodent models of streptozotocin-induced diabetic nephropathy (methods in renal research). Nephrology 2007, 12, 261–266. [Google Scholar] [CrossRef]
- Bohmann, F.O.; Seiler, A.; Gelhard, S.; Stolz, L.; Brill, B.; Brunkhorst, R.; Steinmetz, H.; Harter, P.N.; Mittelbronn, M.; Foerch, C. Blood pressure lowering decreases intracerebral hemorrhage volume and improves behavioral outcomes in experimental animals. J. Stroke 2020, 22, 416–418. [Google Scholar] [CrossRef]
- Ploen, R.; Sun, L.; Zhou, W.; Heitmeier, S.; Zorn, M.; Jenetzky, E.; Veltkamp, R. Rivaroxaban does not increase hemorrhage after thrombolysis in experimental ischemic stroke. J. Cereb. Blood Flow Metab. 2014, 34, 495–501. [Google Scholar] [CrossRef]
- Choudhri, T.F.; Hoh, B.L.; Solomon, R.A.; Connolly, E.S., Jr.; Pinsky, D.J. Use of a spectrophotometric hemoglobin assay to objectively quantify intracerebral hemorrhage in mice. Stroke 1997, 28, 2296–2302. [Google Scholar] [CrossRef]
- Gibson-Corley, K.N.; Olivier, A.K.; Meyerholz, D.K. Principles for Valid Histopathologic Scoring in Research. Vet. Pathol. 2013, 50, 1007–1015. [Google Scholar] [CrossRef] [Green Version]
- Dirnagl, U. Standard operating procedures (SOP) in experimental stroke research: SOP for middle cerebral artery occlusion in the mouse. Nat. Preced. 2009, 1. [Google Scholar] [CrossRef]
- Sun, L.; Zhou, W.; Ploen, R. Anticoagulation with dabigatran does not increase secondary intracerebral haemorrhage after thrombolysis in experimental cerebral ischaemia. Thromb. Haemost. 2013, 110, 153–161. [Google Scholar] [PubMed]
- Strbian, D.; Durukan, A.; Pitkonen, M.; Marinkovic, I.; Tatlisumak, E.; Pedrono, E.; Abo-Ramadan, U. The blood-brain barrier is continuously open for several weeks following transient focal cerebral ischemia. Neuroscience 2008, 153, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Kraft, P.; Schuhmann, M.K.; Fluri, F.; Lorenz, K.; Zernecke, A.; Stoll, G.; Nieswandt, B.; Kleinschnitz, C. Efficacy and safety of platelet glycoprotein receptor blockade in aged and comorbid mice with acute experimental stroke. Stroke 2015, 46, 3502–3506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latour, L.L.; Kang, D.W.; Ezzeddine, M.A.; Chalela, J.A.; Warach, S. Early blood-brain barrier disruption in human focal brain ischemia. Ann. Neurol. 2004, 56, 468–477. [Google Scholar] [CrossRef]
- Wang, X.; Lee, S.R.; Arai, K.; Lee, S.-R.; Tsuji, K.; Rebeck, G.W.; Lo, E.H. Lipoprotein receptor-mediated induction of matrix metalloproteinase by tissue plasminogen activator. Nat. Med. 2003, 9, 1313–1317. [Google Scholar] [CrossRef]
- Kumari, R.; Willing, L.B.; Patel, S.D.; Baskerville, K.A.; Simpson, I.A. Increased cerebral matrix metalloprotease-9 activity is associated with compromised recovery in the diabetic db/db mouse following a stroke. J. Neurochem. 2011, 119, 1029–1040. [Google Scholar] [CrossRef] [Green Version]
- Kenna, J.E.; Anderton, R.S.; Knuckey, N.W.; Meloni, B.P. Assessment of recombinant tissue plasminogen activator (rtPA) toxicity in cultured neural cells and subsequent treatment with poly-arginine peptide R18D. Neurochem. Res. 2020, 45, 1215–1229. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 24 h Sub-Study | 14 d Sub-Study | |||||
|---|---|---|---|---|---|---|
| Experimental Group | Control | rt-PA | rt-PA + Hyperglycemia | Control | rt-PA | rt-PA + Hyperglycemia |
| In total | 12 | 12 | 12 | 12 | 12 | 12 |
| Excluded mice (total) | 3 | 3 | 3 | 1 | 2 | 8 |
| Excluded—Died during operation | 1 | 2 | 1 | 0 | 1 | 0 |
| Excluded—weight loss > 20% | 0 | 0 | 1 | 0 | 0 | 3 |
| Excluded—spontanously died during observation | 2 * | 1 * | 1 * | 1 * | 1 * | 5 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gelhard, S.; Kestner, R.-I.; Armbrust, M.; Steinmetz, H.; Foerch, C.; Bohmann, F.O. Exploring Contraindications for Thrombolysis: Risk of Hemorrhagic Transformation and Neurological Deterioration after Thrombolysis in Mice with Recent Ischemic Stroke and Hyperglycemia. J. Clin. Med. 2022, 11, 3343. https://doi.org/10.3390/jcm11123343
Gelhard S, Kestner R-I, Armbrust M, Steinmetz H, Foerch C, Bohmann FO. Exploring Contraindications for Thrombolysis: Risk of Hemorrhagic Transformation and Neurological Deterioration after Thrombolysis in Mice with Recent Ischemic Stroke and Hyperglycemia. Journal of Clinical Medicine. 2022; 11(12):3343. https://doi.org/10.3390/jcm11123343
Chicago/Turabian StyleGelhard, Sarah, Roxane-Isabelle Kestner, Moritz Armbrust, Helmuth Steinmetz, Christian Foerch, and Ferdinand O. Bohmann. 2022. "Exploring Contraindications for Thrombolysis: Risk of Hemorrhagic Transformation and Neurological Deterioration after Thrombolysis in Mice with Recent Ischemic Stroke and Hyperglycemia" Journal of Clinical Medicine 11, no. 12: 3343. https://doi.org/10.3390/jcm11123343
APA StyleGelhard, S., Kestner, R. -I., Armbrust, M., Steinmetz, H., Foerch, C., & Bohmann, F. O. (2022). Exploring Contraindications for Thrombolysis: Risk of Hemorrhagic Transformation and Neurological Deterioration after Thrombolysis in Mice with Recent Ischemic Stroke and Hyperglycemia. Journal of Clinical Medicine, 11(12), 3343. https://doi.org/10.3390/jcm11123343