
Early Structural and Vascular Changes after Within-24 Hours Vitrectomy for Recent Onset Rhegmatogenous Retinal Detachment Treatment: A Pilot Study Comparing Bisected Macula and Not Bisected Macula

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. OCTA Imaging
2.3. Surgical Procedure
2.4. Statistical Analysis
2.5. Box Plot Analysis
2.6. Scatter Plot Analysis
3. Results
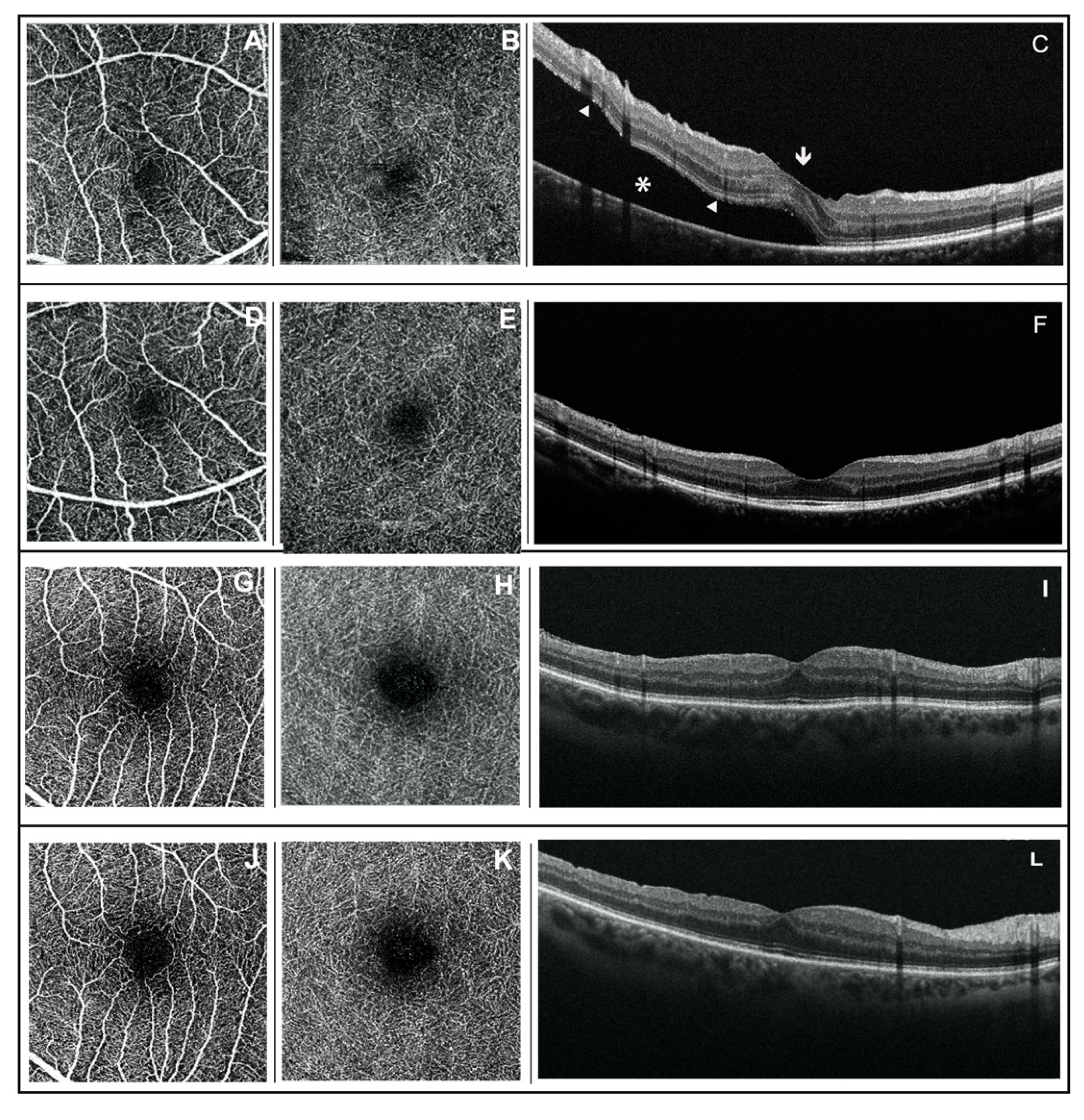
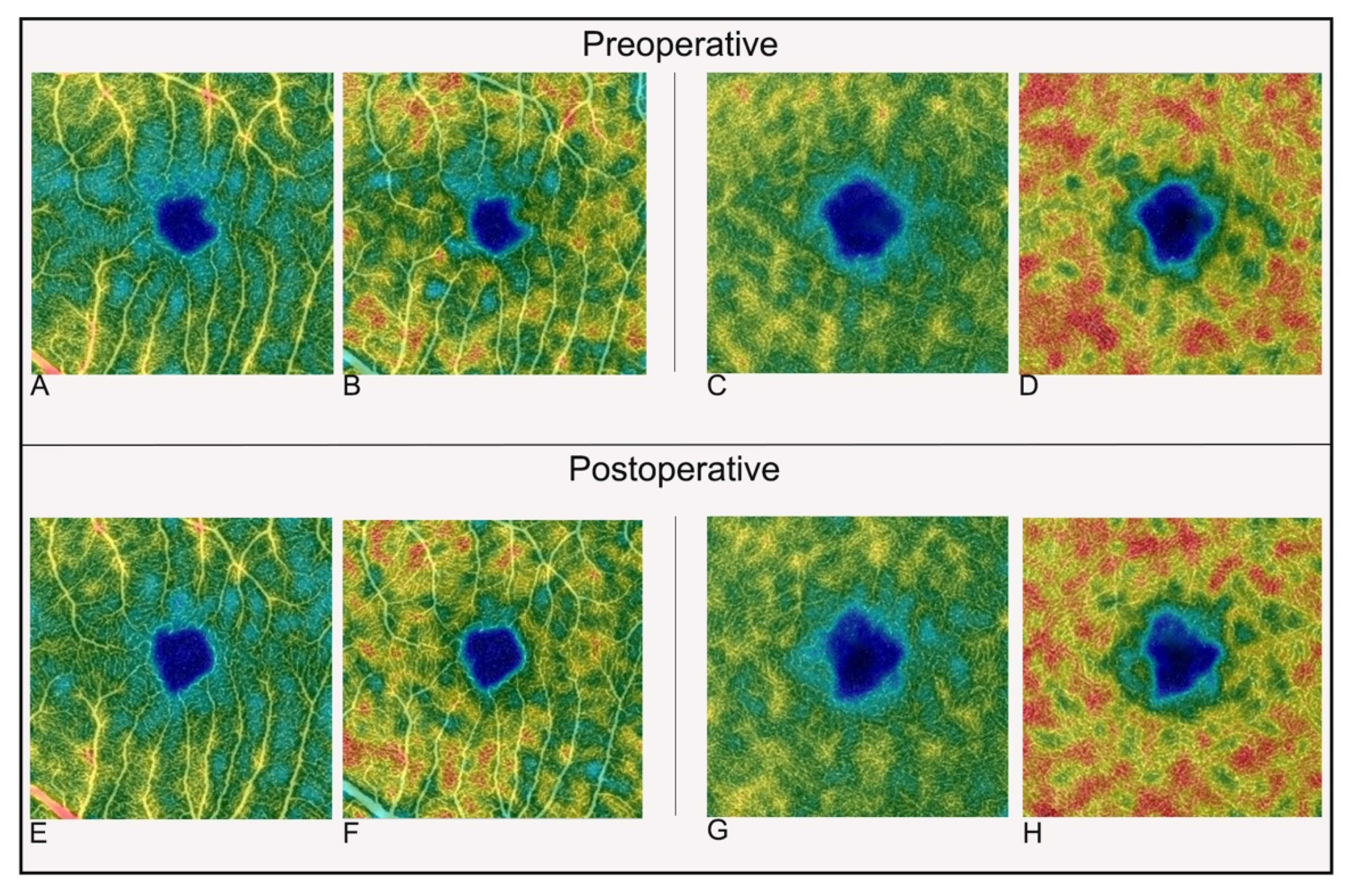
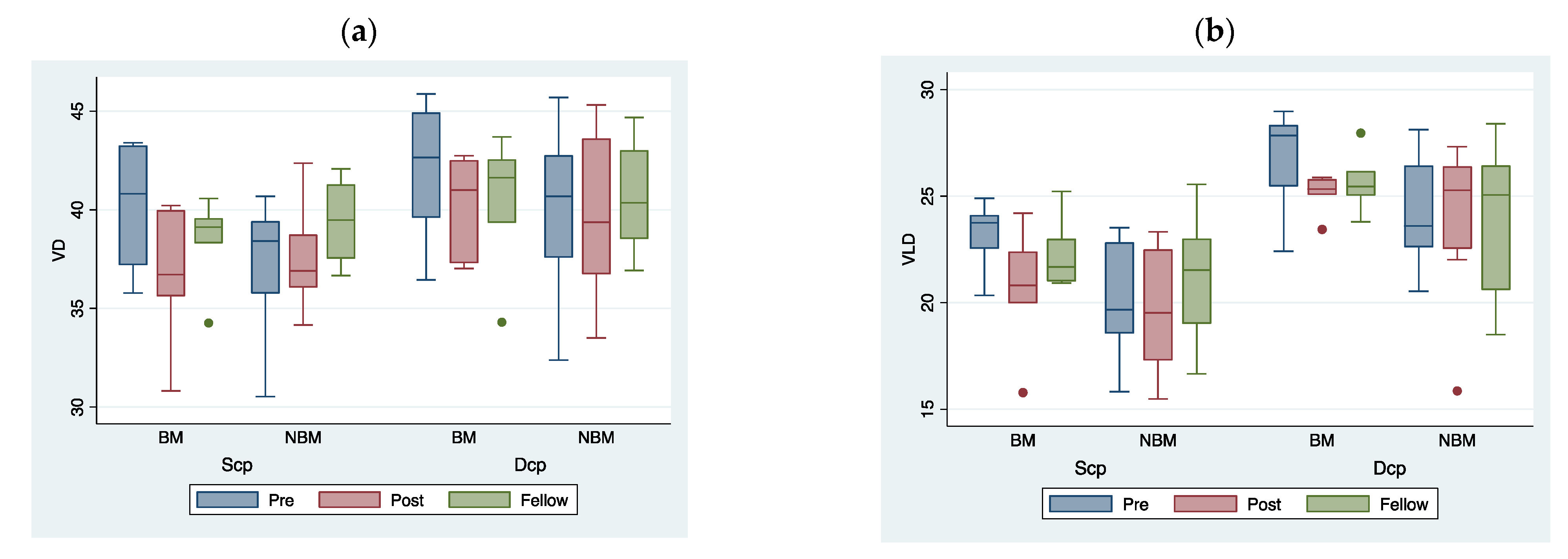
3.1. OCTA Findings
3.2. Visual Acuity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuhn, F.; Aylward, B. Rhegmatogenous retinal detachment: A reappraisal of its pathophysiology and treatment. Ophthalmic Res. 2014, 51, 15–31. [Google Scholar] [CrossRef]
- Nemet, A.; Moshiri, A.; Yiu, G.; Loewenstein, A.; Moisseiev, E. A Review of Innovations in Rhegmatogenous Retinal Detachment Surgical Techniques. J. Ophthalmol. 2017, 2017, 4310643. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.A.; Snead, M.P.; Billington, B.M.; Barrie, T.; Thompson, J.R.; Sparrow, J.M. National audit of the outcome of primary surgery for rhegmatogenous retinal detachment. II. Clinical outcomes. Eye 2002, 16, 771–777. [Google Scholar] [CrossRef]
- Dhoot, A.S.; Popovic, M.M.; Nichani, P.A.H.; Eshtiaghi, A.; Mihalache, A.; Sayal, A.P.; Yu, H.; Wykoff, C.C.; Kertes, P.J.; Muni, R.H. Pars plana vitrectomy versus scleral buckle: A comprehensive meta-analysis of 15,947 eyes. Surv. Ophthalmol. 2022, 67, 932–949. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, H.; Takano, M.; Yanagita, T.; Shiratani, T.; Wang, G.; Hoshi, K.; Shimizu, K. Scleral buckling and pars plana vitrectomy for rhegmatogenous retinal detachment: An analysis of 542 eyes. Curr. Eye Res. 2014, 39, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Orlin, A.; Hewing, N.J.; Nissen, M.; Lee, S.; Kiss, S.; D’Amico, D.J.; Chan, R.V.P. Pars plana vitrectomy compared with pars plana vitrectomy combined with scleral buckle in the primary management of noncomplex rhegmatogenous retinal detachment. Retina. 2014, 34, 1069–1075. [Google Scholar] [CrossRef]
- Lumi, X.; Lužnik, Z.; Petrovski, G.; Petrovski, B.É.; Hawlina, M. Anatomical success rate of pars plana vitrectomy for treatment of complex rhegmatogenous retinal detachment. BMC Ophthalmol. 2016, 16, 216. [Google Scholar] [CrossRef] [Green Version]
- van Bussel, E.M.; van der Valk, R.; Bijlsma, W.R.; La Heij, E.C. Impact of duration of macula-off retinal detachment on visual outcome: A systematic review and meta-analysis of literature. Retina 2014, 34, 1917–1925. [Google Scholar] [CrossRef] [Green Version]
- Tee, J.J.L.; Veckeneer, M.; Laidlaw, D.A. Persistent subfoveolar fluid following retinal detachment surgery: An SD-OCT guided study on the incidence, aetiological associations, and natural history. Eye 2016, 30, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Ghassemi, F.; Karkhaneh, R.; Rezaei, M.; Nili-Ahmadabadi, M.; Ebrahimiadib, N.; Roohipoor, R.; Mohammadi, N. Foveal structure in macula-off rhegmatogenous retinal detachment after scleral buckling or vitrectomy. J. Ophthalmic Vis. Res. 2015, 10, 172–177. [Google Scholar] [CrossRef]
- Karacorlu, M.; Muslubas, I.S.; Hocaoglu, M.; Arf, S.; Ersoz, M.G. Correlation between morphological changes and functional outcomes of recent-onset macula-off rhegmatogenous retinal detachment: Prognostic factors in rhegmatogenous retinal detachment. Int. Ophthalmol. 2018, 38, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.M.; Lee, S.C.; Lee, C.S. Association of Spectral-Domain Optical Coherence Tomography Findings with Visual Outcome of Macula-Off Rhegmatogenous Retinal Detachment Surgery. Ophthalmologica 2015, 234, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, C.D.; Petersen, M.P.; Green, A.; Peto, T.; Grauslund, J. Fundus autofluorescence and spectral domain optical coherence tomography as predictors for long-term functional outcome in rhegmatogenous retinal detachment. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, R.; Xin, W.; Keane, P.A.; Chhablani, J.; Agarwal, A. Optical coherence tomography angiography: A non-invasive tool to image end-arterial system. Expert Rev. Med Devices 2016, 13, 519–521. [Google Scholar] [CrossRef] [Green Version]
- Satoh, Y. Retinal circulation in rhegmatogenous retinal detachment demonstrated by videofluorescence angiography and image analysis. I. The condition of retinal circulation before retinal detachment surgery. Nippon Ganka Gakkai Zasshi (Acta Soc. Ophthalmol. Jpn.) 1989, 93, 1002–1008. [Google Scholar]
- Piccolino, C.; Piccolino, F. Vascular Changes in Rhegmatogenous Retinal Detachment. Ophthalmologica 1983, 186, 17–24. [Google Scholar] [CrossRef]
- Woo, J.E.; Yoon, Y.S.; Min, J.K. Foveal Avascular Zone Area Changes Analyzed Using OCT Angiography after Successful Rhegmatogenous Retinal Detachment Repair. Curr. Eye Res. 2018, 43, 674–678. [Google Scholar] [CrossRef]
- Sato, T.; Kanai, M.; Busch, C.; Wakabayashi, T. Foveal avascular zone area after macula-off rhegmatogenous retinal detachment repair: An optical coherence tomography angiography study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2071–2072. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Aggarwal, K.; Akella, M.; Agrawal, R.; Khandelwal, N.; Bansal, R.; Singh, R.; Gupta, V. Fractal Dimension and Optical Coherence Tomography Angiography Features of the Central Macula After Repair of Rhegmatogenous Rental Detachmnets. Retina 2019, 39, 2167–2177. [Google Scholar] [CrossRef]
- Yoshikawa, Y.; Shoji, T.; Kanno, J.; Ibuki, H.; Ozaki, K.; Ishii, H.; Ichikawa, Y.; Kimura, I.; Shinoda, K. Evaluation of microvascular changes in the macular area of eyes with rhegmatogenous retinal detachment without macular involvement using swept-source optical coherence tomography angiography. Clin. Ophthalmol. 2018, 12, 2059–2067. [Google Scholar] [CrossRef] [Green Version]
- Chatziralli, I.; Theodossiadis, G.; Parikakis, E.; Chatzirallis, A.; Dimitriou, E.; Theodossiadis, P. Inner retinal layers’ alterations and microvasculature changes after vitrectomy for rhegmatogenous retinal detachment. Int. Ophthalmol. 2020, 40, 3349–3356. [Google Scholar] [CrossRef] [PubMed]
- Bonfiglio, V.; Ortisi, E.; Scollo, D.; Reibaldi, M.; Russo, A.; Pizzo, A.; Faro, G.; Macchi, I.; Fallico, M.; Toro, M.D.; et al. Vascular changes after vitrectomy for rhegmatogenous retinal detachment: Optical coherence tomography angiography study. Acta Ophthalmol. 2019, 98, 563. [Google Scholar] [CrossRef] [PubMed]
- Hong, E.H.; Cho, H.; Kim, D.R.; Kang, M.H.; Shin, Y.U.; Seong, M. Changes in Retinal Vessel and Retinal Layer Thickness After Vitrectomy in Retinal Detachment via Swept-Source OCT Angiography. Investig. Opthalmol. Vis. Sci. 2020, 61, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barca, F.; Bacherini, D.; Dragotto, F.; Tartaro, R.; Lenzetti, C.; Finocchio, L.; Rizzo, S.; Savastano, A.; Giansanti, F.; Caporossi, T.; et al. OCT Angiography Findings in Macula-ON and Macula-OFF Rhegmatogenous Retinal Detachment: A Prospective Study. J. Clin. Med. 2020, 9, 3982. [Google Scholar] [CrossRef]
- Baba, T.; Kakisu, M.; Nizawa, T.; Oshitari, T.; Yamamoto, S. Study of foveal avascular zone by OCTA before and after idiopathic epiretinal membrane removal. Spektrum Augenheilkd. 2017, 32, 31–38. [Google Scholar] [CrossRef]
- Lee, C.S.; Shaver, K.; Yun, S.H.; Kim, D.; Wen, S.; Ghorayeb, G. Comparison of the visual outcome between macula-on and macula-off rhegmatogenous retinal detachment based on the duration of macular detachment. BMJ Open Ophthalmol. 2021, 6, e000615. [Google Scholar] [CrossRef] [PubMed]
- Eshita, T.; Shinoda, K.; Kimura, I.; Kitamura, S.; Ishida, S.; Inoue, M.; Mashima, Y.; Katsura, H.; Oguchi, Y. Retinal Blood Flow in the Macular Area Before and After Scleral Buckling Procedures for Rhegmatogenous Retinal Detachment Without Macular Involvement. Jpn. J. Ophthalmol. 2004, 48, 358–363. [Google Scholar] [CrossRef]
- Chua, J.; Ke, M.; Tan, B.; Gan, A.T.L.; Lim, L.S.; Tan, G.S.; Lee, S.Y.; Wong, E.; Schmetterer, L.; Cheung, N. Association of macular and choroidal perfusion with long-term visual outcomes after macula-off rhegmatogenous retinal detachmen. Br. J. Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Yi, J.; Liu, W.; Chen, S.; Backman, V.; Sheibani, N.; Sorenson, C.M.; Fawzi, A.A.; Linsenmeier, R.A.; Zhang, H.F. Visible light optical coherence tomography measures retinal oxygen metabolic response to systemic oxygenation. Light. Sci. Appl. 2015, 4, e334. [Google Scholar] [CrossRef] [Green Version]
- Iandiev, I.; Uhlmann, S.; Pietsch, U.-C.; Biedermann, B.; Reichenbach, A.; Wiedemann, P.; Bringmann, A. Endothelin receptors in the detached retina of the pig. Neurosci. Lett. 2005, 384, 72–75. [Google Scholar] [CrossRef]
- Iandiev, I. Glial Cell Reactivity in a Porcine Model of Retinal Detachment. Investig. Opthalmol. Vis. Sci. 2006, 47, 2161–2171. [Google Scholar] [CrossRef] [PubMed]
- Gaucher, D.; Chiappore, J.-A.; Pâques, M.; Simonutti, M.; Boitard, C.; Sahel, J.A.; Massin, P.; Picaud, S. Microglial changes occur without neural cell death in diabetic retinopathy. Vis. Res. 2007, 47, 612–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roldán-Pallarés, M.; Musa, A.-S.; Hernández-Montero, J.; Llatas, C.B. Preoperative duration of retinal detachment and preoperative central retinal artery hemodynamics: Repercussion on visual acuity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 625–631. [Google Scholar] [CrossRef]
- Polak, K.; Luksch, A.; Frank, B.; Jandrasits, K.; Polska, E.; Schmetterer, L. Regulation of human retinal blood low by endothelin-1. Exp. Eye Res. 2003, 76, 633–640. [Google Scholar] [CrossRef]
- Williamson, T.H.; Shunmugam, M.; Rodrigues, I.; Dogramaci, M.; Lee, E. Characteristics of rhegmatogenous retinal detachment and their relationship to visual outcome. Eye 2013, 27, 1063–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salicone, A.; Smiddy, W.E.; Venkatraman, A.; Feuer, W. Visual recovery after scleral buckling procedure for retinal detachment. Ophthalmology 2006, 113, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Kontos, A.; Williamson, T.H. Rate and risk factors for the conversion of fovea-on to fovea-off rhegmatogenous retinal detachment while awaiting surgery. Br. J. Ophthalmol. 2017, 101, 1011–1015. [Google Scholar] [CrossRef]
- Angermann, R.; Bechrakis, N.E.; Rauchegger, T.; Casazza, M.; Nowosielski, Y.; Zehetner, C. Effect of Timing on Visual Outcomes in Fovea-Involving Retinal Detachments Verified by SD-OCT. J. Ophthalmol. 2020, 2020, 2307935. [Google Scholar] [CrossRef]
- Samara, W.A.; Say, E.A.T.; Khoo, C.T.L.; Higgins, T.P.; Magrath, G.; Ferenczy, S.; Shields, C.L. Correlation of foveal avascular zone size with foveal morphology in normal eyes using optical coherence tomography angiography. Retina 2015, 35, 2188–2195. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n = 14) | ||
|---|---|---|
| Mean Age (Years) | 52.6 ± 15.2 | |
| nNBM | 48.13 ± 17.36 | |
| nBM | 58.67 ± 10.01 | |
| Male: female (n) | 8:6 | |
| RE: LE (n) | 7:7 | |
| NBM | 4:4 | |
| BM | 3:3 | |
| PPV (SF6: C3F8) (n) | 11:3 | |
| NBM: BM (n) | 8:6 | |
| Diabetes mellitus † (n, %) | 2 (14.3%) | |
| nNBM (%) | 1 (12.5%) | |
| nBM (%) | 1 (16.7%) | |
| High blood pressure† (n, %) | 5 (35.7%) | |
| nNBM (%) | 3 (37.5%) | |
| nBM (%) | 2 (33.3%) | |
| Axial length (mm) | 24.8 ± 1.1 | |
| nNBM | 25.5 ± 1.0 | |
| nBM | 24.3 ± 1.1 | |
| Phakic (n) | 13 | |
| NBM: BM (n) | 7:6 | |
| Pseudophakic (n) | 1 | |
| NBM: BM (n) | 1:0 | |
| PPV + PHACO + IOL % (n) | 54.5% (6/11) | |
| NBM: BM (n) | 3:3 | |
| Surgery Duration (min) | 85.36 ± 24.40 | |
| NBM | 93.75 ± 24.07 | |
| BM | 74.17 ± 21.78 | |
| 360° laser photocoagulation % (n) | 21.43% (3/14) | |
| NBM | 25% (2/8) | |
| BM | 16.67% (1/6) | |
| Detachment extension % (n) | ||
| S (only) | 7% (1) | |
| NBM/BM | 1/0 | |
| S-N | 7% (1) | |
| NBM/BM | 1/0 | |
| N (only) | 0% (0) | |
| N-I | 0% (0) | |
| I (only) | 7% (1) | |
| NBM/BM | 1/0 | |
| I-T | 21% (3) | |
| NBM/BM | 0/3 | |
| T (only) | 14% (2) | |
| NBM/BM | 0/2 | |
| T-S | 43% (6) | |
| NBM/BM | 5/1 | |
| Preoperative | Postoperative | Fellow Eye | p-Value | |||
|---|---|---|---|---|---|---|
| Pre. vs. Post. | Pre. vs. Fellow | |||||
| BCVA (logMAR) | 0.114 ± 0.2 | 0.089 ± 0.184 | 0.016 ± 0.059 | 0.3644 | 0.1144 | |
| (Snellen) | 20/26 | 20/25 | 20/20 | |||
| CMT (µm) | 307.50 ± 35.56 | 302.64 ± 33.84 | 284.64 ± 26.47 | 0.5914 | 0.0067 | |
| FAZ (mm2) | ||||||
| Scp | 0.24 ± 0.08 | 0.33 ± 0.13 | 0.24 ± 0.09 | 0.0003 | 0.8739 | |
| Dcp | 0.35 ± 0.16 | 0.45 ± 0.24 | 0.36 ± 0.15 | 0.0107 | 0.0941 | |
| Central Area | ||||||
| VD (%) Scp | 32.24 ± 4.55 | 29.54 ± 4.79 | 30.62 ± 4.35 | 0.1298 | 0.0758 | |
| VD (%) Dcp | 32.63 ± 9.81 | 30.70 ± 6.77 | 29.63 ± 6.83 | 0.4378 | 0.1486 | |
| VLD (mm−1) Scp | 18.22 ± 3.11 | 16.29 ± 2.72 | 17.6 ± 2.60 | 0.1074 | 0.3980 | |
| VLD (mm−1) Dcp | 19.67 ± 6.35 | 18.44 ± 4.27 | 17.77 ± 4.86 | 0.4443 | 0.1773 | |
| Quadrant I | ||||||
| VD (%) Scp | 41.58 ± 3.93 | 42.01 ± 2.15 | 42.06 ± 3.45 | 0.6224 | 0.7051 | |
| VD (%) Dcp | 42.72 ± 3.69 | 44.1 ± 2.42 | 43.96 ± 3.4 | 0.0357 | 0.2991 | |
| VLD (mm−1) Scp | 22.94 ± 3.15 | 22.07 ± 2.89 | 22.99 ± 3.25 | 0.2841 | 0.9500 | |
| VLD (mm−1) Dcp | 26.82 ± 3.12 | 26.91 ± 2.76 | 26.47 ± 3.19 | 0.9294 | 0.6561 | |
| Quadrant N | ||||||
| VD (%) Scp | 37.3 ± 7.07 | 37.34 ± 3.77 | 39.27 ± 2.42 | 0.9838 | 0.3395 | |
| VD (%) Dcp | 41.51 ± 4.16 | 41.03 ± 3.70 | 43.06 ± 2.44 | 0.7448 | 0.1063 | |
| VLD (mm−1) Scp | 21.13 ± 4.89 | 20.54 ± 3.55 | 21.95 ± 2.73 | 0.6137 | 0.4177 | |
| VLD (mm−1) Dcp | 25.63 ± 3.26 | 25.19 ± 2.77 | 26.28 ± 2.36 | 0.6562 | 0.3093 | |
| Quadrant S | ||||||
| VD (%) Scp | 41.29 ± 3.90 | 39.04 ± 4.76 | 42.84 ± 2.15 | 0.1884 | 0.2025 | |
| VD (%) Dcp | 44.59 ± 2.68 | 41.88 ± 5.2 | 43.67 ± 2.53 | 0.0748 | 0.1279 | |
| VLD (mm−1) Scp | 22.74 ± 3.22 | 20.91 ± 3.92 | 23.34 ± 3.28 | 0.0779 | 0.2915 | |
| VLD (mm−1) Dcp | 27.93 ± 2.92 | 25.84 ± 4.27 | 26.79 ± 3.56 | 0.1959 | 0.2436 | |
| Quadrant T | ||||||
| VD (%) Scp | 40.34 ± 4.13 | 37.78 ± 2.72 | 40.3 ± 1.78 | 0.0749 | 0.9774 | |
| VD (%) Dcp | 42.96 ± 2.96 | 42.24 ± 2.3 | 42.75 ± 1.57 | 0.4299 | 0.8184 | |
| VLD (mm−1) Scp | 22.41 ± 2.78 | 20.69 ± 2.95 | 22.29 ± 2.47 | 0.1130 | 0.8921 | |
| VLD (mm−1) Dcp | 26.68 ± 2.75 | 25.91 ± 3.05 | 25.89 ± 2.65 | 0.5471 | 0.3824 | |
| Whole Macular Area | ||||||
| VD (%) Scp | 38.55 ± 3.50 | 37.14 ± 2.88 | 39.02 ± 2.10 | 0.2855 | 0.5915 | |
| VD (%) Dcp | 40.89 ± 4.00 | 39.99 ± 3.47 | 40.61 ± 2.92 | 0.3868 | 0.7796 | |
| VLD (mm−1) Scp | 21.49 ± 2.72 | 20.1 ± 2.88 | 21.63 ± 2.50 | 0.0980 | 0.7796 | |
| VLD (mm−1) Dcp | 25.35 ± 2.76 | 24.46 ± 2.85 | 24.64 ± 2.98 | 0.3633 | 0.2758 | |
| Parafoveal Macular Area | ||||||
| VD (%) Scp | 40.13 ± 3.82 | 39.04 ± 2.88 | 41.12 ± 1.81 | 0.3981 | 0.3580 | |
| VD (%) Dcp | 42.94 ± 2.77 | 42.31 ± 2.91 | 43.36 ± 2.11 | 0.4068 | 0.5140 | |
| VLD (mm−1) Scp | 22.31 ± 2.92 | 21.05 ± 3.19 | 22.64 ± 2.70 | 0.1231 | 0.5150 | |
| VLD (mm−1) Dcp | 26.76 ± 2.55 | 25.97 ± 2.89 | 26.36 ± 2.80 | 0.4472 | 0.5205 | |
| BM | NBM | |||||
|---|---|---|---|---|---|---|
| Preoperative | Postoperative | Fellow Eye | Preoperative | Postoperative | Fellow Eye | |
| BCVA (logMAR) | 0.24 ± 0.26 | 0.16 ± 0.27 | 0.04 ± 0.08 | 0.01 ± 0.03 # | 0.03 ± 0.03 | 0.0 ± 0.0 |
| FAZ (mm2) | ||||||
| Scp | 0.24 ± 0.09 | 0.35 ± 0.15 * | 0.25 ± 0.11 | 0.24 ± 0.08 | 0.31 ± 0.12 ° | 0.23 ± 0.07 |
| Dcp | 0.32 ± 0.18 | 0.42 ± 0.29 * | 0.34 ± 0.16 | 0.36 ± 0.14 | 0.46 ± 0.22 | 0.37 ± 0.15 |
| Whole Macular Area | ||||||
| VD (%) Scp | 40.21 ± 3.19 | 36.67 ± 3.43 | 38.49 ± 2.21 | 37.30 ± 3.36 | 37.49 ± 2.58 | 39.41 ± 2.05 |
| VD (%) Dcp | 42.03 ± 3.78 | 40.26 ± 2.51 | 40.52 ± 3.38 | 40.02 ± 4.17 | 39.78 ± 4.20 | 40.67 ± 2.76 |
| VLD (mm−1) Scp | 23.23 ± 1.62 | 20.66 ± 2.84 | 22.25 ± 1.66 | 20.18 ± 2.70 | 19.67 ± 3.01 | 21.16 ± 3.01 |
| VLD (mm−1) Dcp | 26.81 ± 2.46 | 25.14 ± 0.89 | 25.64 ± 1.40 | 24.24 ± 2.56 | 23.95 ± 3.72 | 23.88 ± 2.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Aloisio, R.; Gironi, M.; Verdina, T.; Vivarelli, C.; Leonelli, R.; Mariotti, C.; Kaleci, S.; Toto, L.; Mastropasqua, R. Early Structural and Vascular Changes after Within-24 Hours Vitrectomy for Recent Onset Rhegmatogenous Retinal Detachment Treatment: A Pilot Study Comparing Bisected Macula and Not Bisected Macula. J. Clin. Med. 2022, 11, 3498. https://doi.org/10.3390/jcm11123498
D’Aloisio R, Gironi M, Verdina T, Vivarelli C, Leonelli R, Mariotti C, Kaleci S, Toto L, Mastropasqua R. Early Structural and Vascular Changes after Within-24 Hours Vitrectomy for Recent Onset Rhegmatogenous Retinal Detachment Treatment: A Pilot Study Comparing Bisected Macula and Not Bisected Macula. Journal of Clinical Medicine. 2022; 11(12):3498. https://doi.org/10.3390/jcm11123498
Chicago/Turabian StyleD’Aloisio, Rossella, Matteo Gironi, Tommaso Verdina, Chiara Vivarelli, Riccardo Leonelli, Cesare Mariotti, Shaniko Kaleci, Lisa Toto, and Rodolfo Mastropasqua. 2022. "Early Structural and Vascular Changes after Within-24 Hours Vitrectomy for Recent Onset Rhegmatogenous Retinal Detachment Treatment: A Pilot Study Comparing Bisected Macula and Not Bisected Macula" Journal of Clinical Medicine 11, no. 12: 3498. https://doi.org/10.3390/jcm11123498
APA StyleD’Aloisio, R., Gironi, M., Verdina, T., Vivarelli, C., Leonelli, R., Mariotti, C., Kaleci, S., Toto, L., & Mastropasqua, R. (2022). Early Structural and Vascular Changes after Within-24 Hours Vitrectomy for Recent Onset Rhegmatogenous Retinal Detachment Treatment: A Pilot Study Comparing Bisected Macula and Not Bisected Macula. Journal of Clinical Medicine, 11(12), 3498. https://doi.org/10.3390/jcm11123498