
Perioperative Radiographic Predictors of Non-Union in Infra-Isthmal Femoral Shaft Fractures after Antegrade Intramedullary Nailing: A Case–Control Study


Abstract
:1. Introduction
2. Materials and Method
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiss, R.J.; Montgomery, S.M.; Al Dabbagh, Z.; Jansson, K.A. National Data of 6409 Swedish Inpatients with Femoral Shaft Fractures: Stable Incidence Between 1998 and 2004. Injury 2009, 40, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Agarwal-Harding, K.J.; Meara, J.G.; Greenberg, S.L.; Hagander, L.E.; Zurakowski, D.; Dyer, G.S. Estimating the Global Incidence of Femoral Fracture from Road Traffic Collisions: A Literature Review. J. Bone Jt. Surg. Am. 2015, 97, e31. [Google Scholar] [CrossRef] [PubMed]
- Taitsman, L.A.; Lynch, J.R.; Agel, J.; Barei, D.P.; Nork, S.E. Risk Factors for Femoral Nonunion after Femoral Shaft Fracture. J. Trauma 2009, 67, 1389–1392. [Google Scholar] [CrossRef] [PubMed]
- Pihlajamäki, H.K.; Salminen, S.T.; Böstman, O.M. The Treatment of Nonunions Following Intramedullary Nailing of Femoral Shaft Fractures. J. Orthop. Trauma 2002, 16, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Canadian Orthopaedic Trauma Society. Nonunion Following Intramedullary Nailing of the Femur with and without Reaming. Results of a Multicenter Randomized Clinical Trial. J. Bone Jt. Surg. Am. 2003, 85, 2093–2096. [Google Scholar] [CrossRef]
- Ricci, W.M.; Bellabarba, C.; Evanoff, B.; Herscovici, D.; DiPasquale, T.; Sanders, R. Retrograde Versus Antegrade Nailing of Femoral Shaft Fractures. J. Orthop. Trauma 2001, 15, 161–169. [Google Scholar] [CrossRef]
- Selvakumar, K.; Saw, K.Y.; Fathima, M. Comparison Study Between Reamed and Unreamed Nailing of Closed Femoral Fractures. Med. J. Malaysia 2001, 56, 24–28. [Google Scholar]
- Park, J.; Kim, S.G.; Yoon, H.K.; Yang, K.H. The Treatment of Nonisthmal Femoral Shaft Nonunions with IM Nail Exchange Versus Augmentation Plating. J. Orthop. Trauma 2010, 24, 89–94. [Google Scholar] [CrossRef]
- Song, S.H. Radiologic Outcomes of Intramedullary Nailing in Infraisthmal Femur-Shaft Fracture with or without Poller Screws. Biomed. Res. Int. 2019, 2019, 9412379. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Yoon, Y.C.; Oh, C.W.; Han, S.B.; Sim, J.A.; Oh, J.K. Exchange Nailing with Enhanced Distal Fixation is Effective for the Treatment of Infraisthmal Femoral Nonunions. Arch. Orthop. Trauma Surg. 2018, 138, 27–34. [Google Scholar] [CrossRef]
- Yang, T.C.; Tzeng, Y.H.; Wang, C.S.; Lin, C.C.; Chang, M.C.; Chiang, C.C. “Ratio of fracture site diameter to isthmus femoral canal diameter” as a predictor of complication following treatment of infra-isthmal femoral shaft fracture with antegrade intramedullary nailing. Injury 2021, 52, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Takenaka, N.; Kobayashi, M.; Matsushita, T. Infra-isthmal Fracture is a Risk Factor for Nonunion After Femoral Nailing: A Case-Control Study. J. Orthop. Sci. 2013, 18, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.H.; Kim, J.R.; Park, J. Nonisthmal Femoral Shaft Nonunion as a Risk Factor for Exchange Nailing Failure. J. Trauma Acute Care Surg. 2012, 72, E60–E64. [Google Scholar] [CrossRef] [PubMed]
- Frölke, J.P.; Patka, P. Definition and Classification of Fracture Non-unions. Injury 2007, 38, S19–S22. [Google Scholar] [CrossRef]
- Weber, B.G.; Brunner, C. The Treatment of Nonunions without Electrical Stimulation. Clin. Orthop. Relat. Res. 1981, 161, 24–32. [Google Scholar] [CrossRef]
- Fracture and Dislocation Compendium. Orthopaedic Trauma Association Committee for Coding and Classification. J. Orthop. Trauma 1996, 10 (Suppl. 1: V-ix), 1–154. [Google Scholar]
- Nicholson, J.A.; Makaram, N.; Simpson, A.; Keating, J.F. Fracture Nonunion in Long Bones: A Literature Review of Risk Factors and Surgical Management. Injury 2021, 52, S3–S11. [Google Scholar] [CrossRef]
- Zura, R.; Mehta, S.; Della Rocca, G.J.; Steen, R.G. Biological Risk Factors for Nonunion of Bone Fracture. JBJS Rev. 2016, 4, e5. [Google Scholar] [CrossRef]
- Reis, N.D.; Hirschberg, E. The Infra-isthmal Fracture of the Shaft of the Femur. Injury 1977, 9, 8–16. [Google Scholar] [CrossRef]
- Ha, S.S.; Oh, C.W.; Jung, J.W.; Kim, J.W.; Park, K.H.; Kim, S.M. Exchange Nailing for Aseptic Nonunion of the Femoral Shaft after Intramedullary Nailing. J. Trauma Inj. 2020, 33, 104–111. [Google Scholar] [CrossRef]
- Zhang, X.; Zhong, B.; Sui, S.; Yu, X.; Jiang, Y. Treatment of Distal Femoral Nonunion and Delayed Union by Using a Retrograde Intramedullary Interlocking Nail. Chin. J. Traumatol. 2001, 4, 180–184. [Google Scholar] [PubMed]
- Van Dyke, B.; Colley, R.; Ottomeyer, C.; Palmer, R.; Pugh, K. Effect of Blocking Screws on Union of Infraisthmal Femur Fractures Stabilized With a Retrograde Intramedullary Nail. J. Orthop. Trauma 2018, 32, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Brinker, M.R.; O’Connor, D.P. Exchange Nailing of Ununited Fractures. J. Bone Jt. Surg Am. 2007, 89, 177–188. [Google Scholar] [CrossRef]
- Auston, D.; Donohue, D.; Stoops, K.; Cox, J.; Diaz, M.; Santoni, B.; Mir, H. Long Segment Blocking Screws Increase the Stability of Retrograde Nail Fixation in Geriatric Supracondylar Femur Fractures: Eliminating the “Bell-Clapper Effect”. J. Orthop. Trauma 2018, 32, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.K.; Singh, V.A.; Mariapan, S.; Chong, S.T. Antegrade Versus Retrograde Locked Intramedullary Nailing for Femoral Fractures: Which Is Better? Eur. J. Trauma Emerg. Surg. 2007, 33, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Tornetta, P.; Tiburzi, D. Antegrade or Retrograde Reamed Femoral Nailing. A Prospective, Randomised Trial. J. Bone Jt. Surg. Br. 2000, 82, 652–654. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Union (n = 31) | Union (n = 62) | p-Value | |
|---|---|---|---|
| Age, years (95% CI) | 28.6 (20–34) | 28.2 (20–35) | 0.687 |
| Male, n (%) | 23 (74.2) | 47 (75.8) | 0.672 |
| Right laterality, n (%) | 18 (58.1) | 40 (64.5) | 0.514 |
| BMI, kg/m2 (95% CI) | 23.6 (18.4–33.8) | 24.1 (18.8–34.2) | 0.761 |
| AO/OTA classification | 0.004 | ||
| Type A, n (%) | 11 (35.5) | 42 (67.7) | |
| Type B and C, n (%) | 20 (64.5) | 20 (32.3) | |
| Postoperative coronal deformity, degree (95% CI) | 7.0 (2–10) | 6.7 (3–9) | 0.341 |
| Postoperative sagittal deformity, degree (95% CI) | 3.6 (2–9) | 2.8 (2–10) | 0.412 |
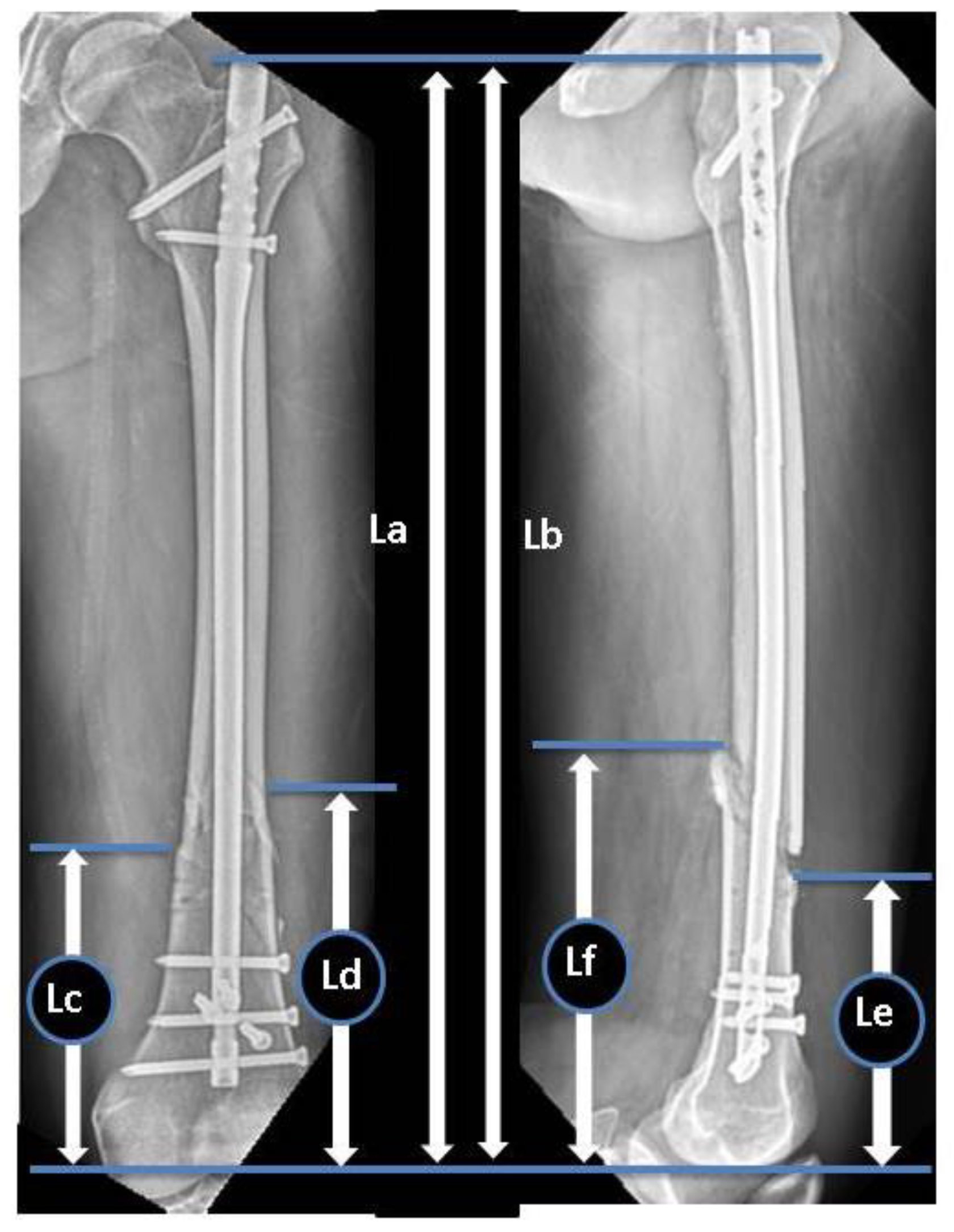
| Ratio of the distal fragment, % (95% CI) | 34.6 (28–40) | 44.5 (37–47) | 0.021 |
| Ratio of the unfixed distal fragment, % (95% CI) | 32.3 (24.1–41.8) | 23.8 (16.4–28.7) | 0.013 |
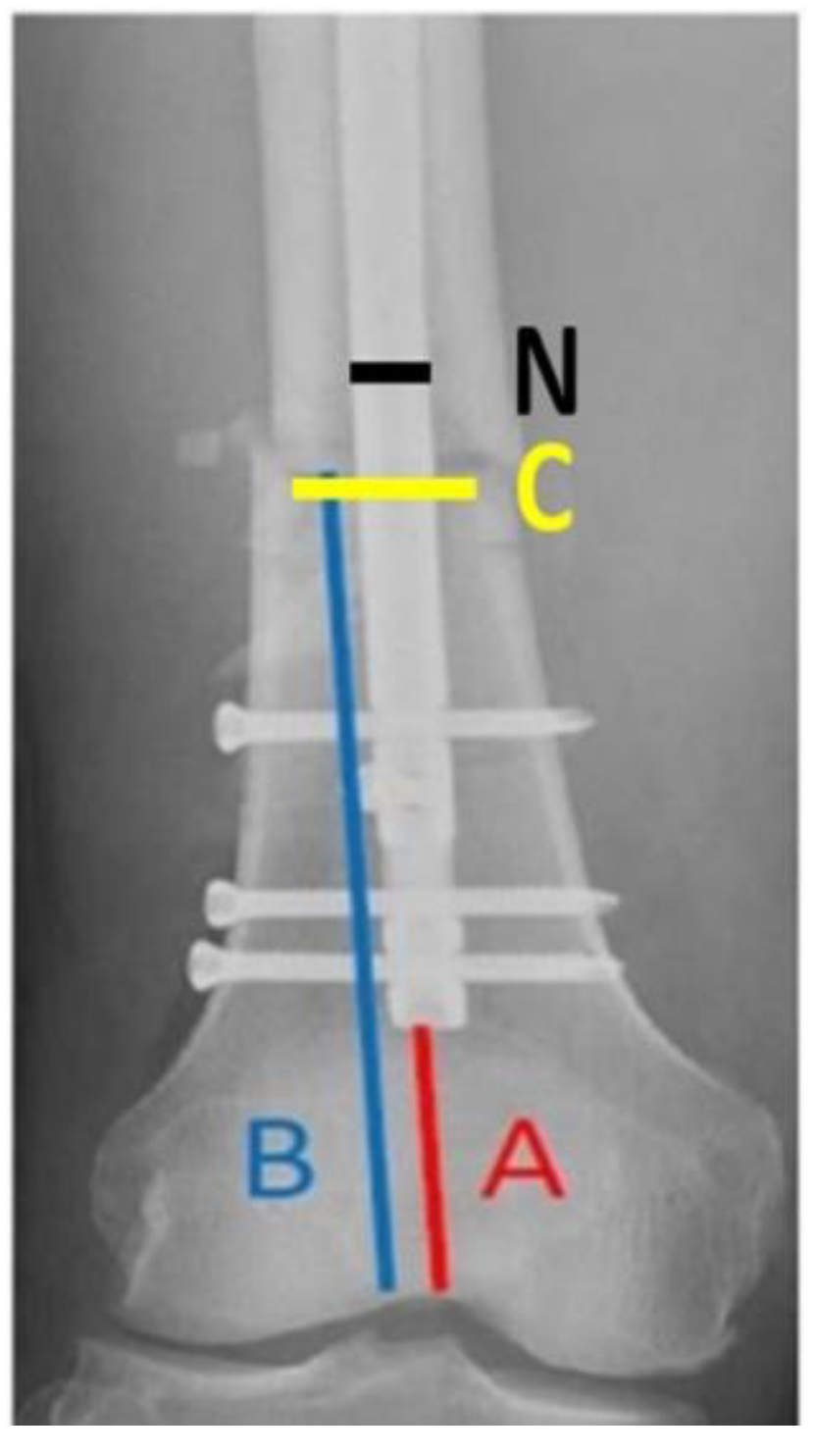
| C/N ratio, (95% CI) | 2.2 (1.9–2.4) | 1.9 (1.8–2.1) | 0.028 |
| Distal locking screws, n (95% CI) | 2.1(2–4) | 3.4 (2–4) | 0.033 |
| Poller screws, n (95% CI) | 0.69 (0–2) | 0.93 (0–4) | 0.086 |
| Risk Factor | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| AO/OTA classification type B and C | 2.87 (0.67–5.84) | 0.028 |
| Ratio of the distal fragment < 43% | 5.41 (2.09–10.65) | 0.002 |
| Ratio of the unfixed distal fragment > 32.5% | 9.23 (3.44–24.06) | <0.001 |
| C/N ratio > 2.1 | 8.71 (2.07–21.27) | 0.001 |
| Distal locking screws < 3 | 3.16 (1.94–9.17) | 0.004 |
| Risk Factor | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|
| AO/OTA classification type B and C | 2.20 (0.47–4.13) | 0.037 |
| Ratio of the distal fragment < 43% | 4.05 (1.43–7.12) | 0.018 |
| Ratio of the unfixed distal fragment > 32.5% | 7.16 (2.37–17.96) | 0.031 |
| C/N ratio > 2.1 | 6.23 (1.94–17.38) | 0.017 |
| Distal locking screws < 3 | 2.31 (1.08–6.18) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, W.-C.; Hsu, C.-J.; Kumar, A.; Tsai, C.-H.; Chang, H.-W.; Lin, T.-L. Perioperative Radiographic Predictors of Non-Union in Infra-Isthmal Femoral Shaft Fractures after Antegrade Intramedullary Nailing: A Case–Control Study. J. Clin. Med. 2022, 11, 3664. https://doi.org/10.3390/jcm11133664
Hung W-C, Hsu C-J, Kumar A, Tsai C-H, Chang H-W, Lin T-L. Perioperative Radiographic Predictors of Non-Union in Infra-Isthmal Femoral Shaft Fractures after Antegrade Intramedullary Nailing: A Case–Control Study. Journal of Clinical Medicine. 2022; 11(13):3664. https://doi.org/10.3390/jcm11133664
Chicago/Turabian StyleHung, Wei-Cheng, Chin-Jung Hsu, Abhishek Kumar, Chun-Hao Tsai, Hao-Wei Chang, and Tsung-Li Lin. 2022. "Perioperative Radiographic Predictors of Non-Union in Infra-Isthmal Femoral Shaft Fractures after Antegrade Intramedullary Nailing: A Case–Control Study" Journal of Clinical Medicine 11, no. 13: 3664. https://doi.org/10.3390/jcm11133664
APA StyleHung, W. -C., Hsu, C. -J., Kumar, A., Tsai, C. -H., Chang, H. -W., & Lin, T. -L. (2022). Perioperative Radiographic Predictors of Non-Union in Infra-Isthmal Femoral Shaft Fractures after Antegrade Intramedullary Nailing: A Case–Control Study. Journal of Clinical Medicine, 11(13), 3664. https://doi.org/10.3390/jcm11133664