
Evaluation and Management of Cavus Foot in Adults: A Narrative Review

Abstract
:1. Introduction
2. Biomechanics, Etiology and Classification of Cavus Foot
2.1. Biomechanics
2.2. Etiology
2.3. Classification
- Causes classification
- Neuromuscular;
- Congenital;
- Acquired;
- Idiopathic.
- Deformity location classification
- Forefoot derived cavus: The apex of the deformity at the midfoot or forefoot, or plantar flexion of the first ray;
- Hindfoot derived cavus: Rigid varus and inclination increase of the calcaneus;
- Mixed cavus: A combination of the previous types.
- Flexible: Dynamic deformity that corrects with tendon transfers;
- Stiff: Structural deformity that corrects with soft tissue release and balance;
- Rigid: Structural deformity that requires osteotomies for correction.
3. Pathophysiology of Cavus Foot
4. Clinical Evaluation
4.1. Physical Examination
- A short assessment of the patient’s gait. You may be able to see an unstable foot drop gait, a weak push stance, or a weak dorsiflexion. Patients who have limb length discrepancies may have a limp gait. Patients with hip pathologies may also present with a Trendelenburg gait.
- Identify the deforming forces involved [27]. Although we cannot precisely calculate muscle strength through a physical examination, it is of great significance to help us to formulate the correct tendon release or transfer plan.
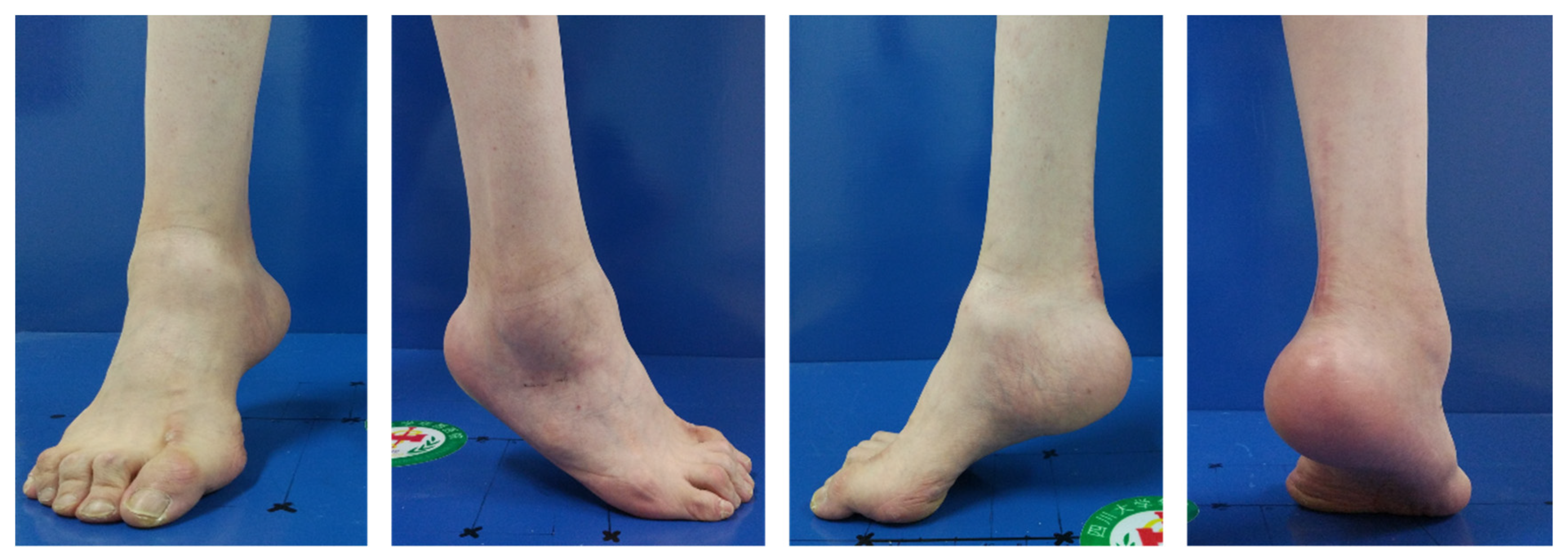
- Identify the source of the deformity. The Coleman block test [28] is the most popular method for assessing the flexibility of the hindfoot and for determining the source of the deformity. The patient is asked to stand with the heel and lateral border of the foot over a 1-inch-high block while the medial metatarsals are in contact with the floor (Figure 5). When the hindfoot is flexible, the heel will return to a neutral or valgus position. Meanwhile, we can further judge that the source of the deformity is the forefoot. A positive Coleman block sign implies that the hindfoot varus is due to the plantarflexed first ray and that the hindfoot is flexible. However, the Coleman block test cannot accurately reflect the flexibility of the hindfoot, especially when the patient has difficulty positing their foot on the block, which will mislead our judgment. Price et al. [29] described a method of evaluating the flexibility of the hindfoot. The patient lies prone on the examination bed, the examiner instructs the patient to bend the knee and corrects the calcaneal varus manually to see if the varus can be completely corrected and whether the first ray is decreased. Therefore, we need to make a comprehensive judgment by combining manual correction with the Coleman block test. If manual correction of the varus of the hindfoot is possible, we can also think that the hindfoot is flexible. More flexion of the first ray is usually observed after manual correction of the forefoot pronation and hindfoot varus (Figure 6).
- Assess the deformity in the coronal plane. The three-dimensional nature of cavus foot requires us to take into account all aspects during correction. We should estimate whether there is adduction or abduction of the forefoot after the manual correction of the hindfoot.
- Assess the mobility of the first ray. The first metatarsal of the patient’s foot is grasped with the examiner’s hand and the rest of the foot is stabilized. The first metatarsal is then manipulated with the right thumb and forefinger. Motion in multiple directions should be evaluated [30]. In cases of cavus foot, the motion of the first ray is usually decreased.
- The Silfverskiold test [31,32,33] is essential. The clinician places the one hand at the level of the subtalar joint and the other around the midfoot, stabilizing the talonavicular joint and keeping the foot in a neutral position while dorsiflexing the ankle. The test is performed with the knee extended and flexed, respectively. If ankle dorsiflexion is not affected by knee flexion and extension, this indicates Achilles tendon contracture. If ankle dorsiflexion is increased during knee flexion, this indicates gastrocnemius contracture. We can choose gastrocnemius resection or Achilles tendon lengthening according to the result of this test.
4.2. Radiological Evaluation
5. Management of Cavus Foot
5.1. Conservative Treatment
5.2. Surgical Treatment
5.2.1. Soft-Tissue Release
5.2.2. Bony Reconstruction
Forefoot Driven Cavus Foot
Hindfoot Driven Cavus Foot
Mixed Cavus Foot
5.2.3. Soft-Tissue Balancing
5.2.4. Ancillary Procedures
6. What’s New
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pipis, M.; Rossor, A.M.; Laura, M.; Reilly, M.M. Next-generation sequencing in Charcot-Marie-Tooth disease: Opportunities and challenges. Nat. Rev. Neurol. 2019, 15, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Laura, M.; Singh, D.; Ramdharry, G.; Morrow, J.; Skorupinska, M.; Pareyson, D.; Burns, J.; Lewis, R.A.; Scherer, S.S.; Herrmann, D.N.; et al. Prevalence and orthopedic management of foot and ankle deformities in Charcot-Marie-Tooth disease. Muscle Nerve 2018, 57, 255–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkadesan, M.; Yawar, A.; Eng, C.M.; Dias, M.A.; Singh, D.K.; Tommasini, S.M.; Haims, A.H.; Bandi, M.M.; Mandre, S. Stiffness of the human foot and evolution of the transverse arch. Nature 2020, 579, 97–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, M.P.; Drought, A.B.; Kory, R.C. Walking patterns of normal men. J. Bone Jt. Surg. Am. 1964, 46, 335–360. [Google Scholar] [CrossRef]
- Di Gregorio, R.; Vocenas, L. Identification of Gait-Cycle Phases for Prosthesis Control. Biomimetics 2021, 6, 22. [Google Scholar] [CrossRef]
- Mayich, D.J.; Novak, A.; Vena, D.; Daniels, T.R.; Brodsky, J.W. Gait analysis in orthopedic foot and ankle surgery--topical review, part 1: Principles and uses of gait analysis. Foot Ankle Int. 2014, 35, 80–90. [Google Scholar] [CrossRef]
- Aminian, A.; Sangeorzan, B.J. The anatomy of cavus foot deformity. Foot Ankle Clin. 2008, 13, 191–198. [Google Scholar] [CrossRef]
- Biz, C.; Maso, G.; Malgarini, E.; Tagliapietra, J.; Ruggieri, P. Hypermobility of the First Ray: The Cinderella of the measurements conventionally assessed for correction of Hallux Valgus. Acta Bio-Med. Atenei Parm. 2020, 91, 47–59. [Google Scholar] [CrossRef]
- Biz, C.; Favero, L.; Stecco, C.; Aldegheri, R. Hypermobility of the first ray in ballet dancer. Muscles Ligaments Tendons J. 2012, 2, 282–288. [Google Scholar]
- Pfeffer, G.B.; Gonzalez, T.; Brodsky, J.; Campbell, J.; Coetzee, C.; Conti, S.; Guyton, G.; Herrmann, D.N.; Hunt, K.; Johnson, J.; et al. A Consensus Statement on the Surgical Treatment of Charcot-Marie-Tooth Disease. Foot Ankle Int. 2020, 41, 870–880. [Google Scholar] [CrossRef]
- Mosca, V.S. The cavus foot. J. Pediatr. Orthop. 2001, 21, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Maynou, C.; Szymanski, C.; Thiounn, A. The adult cavus foot. Effort. Open Rev. 2017, 2, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Eleswarapu, A.S.; Yamini, B.; Bielski, R.J. Evaluating the Cavus Foot. Pediatr. Ann. 2016, 45, e218–e222. [Google Scholar] [CrossRef]
- McCluskey, W.P.; Wood, L.W.; Cummings, R.J. The cavovarus foot deformity. Etiology and management. Clin. Orthop. Relat. Res. 1989, 247, 27–37. [Google Scholar] [CrossRef]
- Alexander, I.J.; Johnson, K.A. Assessment and management of pes cavus in Charcot-Marie-tooth disease. Clin. Orthop. Relat. Res. 1989, 246, 273–281. [Google Scholar] [CrossRef]
- Holmes, J.R.; Hansen, S.T., Jr. Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993, 14, 476–486. [Google Scholar] [CrossRef]
- Tenuta, J.; Shelton, Y.A.; Miller, F. Long-term follow-up of triple arthrodesis in patients with cerebral palsy. J. Pediatr. Orthop. 1993, 13, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Mosca, V.S. Foot and ankle deformities. In Priciples and Management of Pediatric Foot and Ankle Deformities and Malformations; Mosca, V.S., Ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2014; pp. 61–118. [Google Scholar]
- Randt, T.Q.; Wolfe, J.; Keeter, E.; Visser, H.J. Tendon Transfers and Their Role in Cavus Foot Deformity. Clin. Podiatr. Med. Surg. 2021, 38, 427–443. [Google Scholar] [CrossRef]
- Huber, M. What is the role of tendon transfer in the cavus foot? Foot Ankle Clin. 2013, 18, 689–695. [Google Scholar] [CrossRef]
- Kuo, K.N.; Wu, K.W.; Krzak, J.J.; Smith, P.A. Tendon Transfers Around the Foot: When and Where. Foot Ankle Clin. 2015, 20, 601–617. [Google Scholar] [CrossRef]
- Ryssman, D.B.; Myerson, M.S. Tendon transfers for the adult flexible cavovarus foot. Foot Ankle Clin. 2011, 16, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Dreher, T.; Wolf, S.I.; Heitzmann, D.; Fremd, C.; Klotz, M.C.; Wenz, W. Tibialis posterior tendon transfer corrects the foot drop component of cavovarus foot deformity in Charcot-Marie-Tooth disease. J. Bone Jt. Surg. Am. 2014, 96, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben Salem, A.K.; Maré, P.H.; Goodier, M.; Marais, L.C. Thompson DM. Polio-like deformity: A diagnostic dilemma. SA Orthop. J. 2021, 20, 93–97. [Google Scholar] [CrossRef]
- Shim, D.W.; Suh, J.W.; Park, K.H.; Lee, J.W.; Byun, J.; Han, S.H. Diagnosis and Operation Results for Chronic Lateral Ankle Instability with Subtle Cavovarus Deformity and a Peek-A-Boo Heel Sign. Yonsei. Med. J. 2020, 61, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Deben, S.E.; Pomeroy, G.C. Subtle cavus foot: Diagnosis and management. J. Am. Acad. Orthop. Surg. 2014, 22, 512–520. [Google Scholar] [CrossRef]
- Zide, J.R.; Myerson, M.S. Arthrodesis for the cavus foot: When, where, and how? Foot Ankle Clin. 2013, 18, 755–767. [Google Scholar] [CrossRef]
- Coleman, S.S.; Chesnut, W.J. A simple test for hindfoot flexibility in the cavovarus foot. Clin. Orthop. Relat. Res. 1977, 123, 60–62. [Google Scholar] [CrossRef]
- Price, B.D.; Price, C.T. A simple demonstration of hindfoot flexibility in the cavovarus foot. J. Pediatr. Orthop. 1997, 17, 18–19. [Google Scholar] [CrossRef]
- Myerson, M.S.; Badekas, A. Hypermobility of the first ray. Foot Ankle Clin. 2000, 5, 469–484. [Google Scholar]
- Symeonidis, P. The Silfverskiold Test. Foot Ankle Int. 2014, 35, 838. [Google Scholar] [CrossRef]
- Barouk, P.; Barouk, L.S. Clinical diagnosis of gastrocnemius tightness. Foot Ankle Clin. 2014, 19, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Molund, M.; Husebye, E.E.; Nilsen, F.; Hellesnes, J.; Berdal, G.; Hvaal, K.H. Validation of a New Device for Measuring Isolated Gastrocnemius Contracture and Evaluation of the Reliability of the Silfverskiold Test. Foot Ankle Int. 2018, 39, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. A protocol for classifying normal- and flat-arched foot posture for research studies using clinical and radiographic measurements. J. Foot Ankle Res. 2009, 2, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrara, C.; Caravaggi, P.; Belvedere, C.; Leardini, A. Radiographic angular measurements of the foot and ankle in weight-bearing: A literature review. Foot Ankle Surg. 2020, 26, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Michalski, M.P.; An, T.W.; Haupt, E.T.; Yeshoua, B.; Salo, J.; Pfeffer, G. Abnormal Bone Morphology in Charcot-Marie-Tooth Disease. Foot Ankle Int. 2022, 43, 576–581. [Google Scholar] [CrossRef] [PubMed]
- An, T.; Haupt, E.; Michalski, M.; Salo, J.; Pfeffer, G. Cavovarus With a Twist: Midfoot Coronal and Axial Plane Rotational Deformity in Charcot-Marie-Tooth Disease. Foot Ankle Int. 2022, 43, 676–682. [Google Scholar] [CrossRef]
- Fernandez-Seguin, L.M.; Heredia-Rizo, A.M.; Diaz-Mancha, J.A.; Gonzalez-Garcia, P.; Ramos-Ortega, J.; Munuera-Martinez, P.V. Immediate and short-term radiological changes after combining static stretching and transcutaneous electrical stimulation in adults with cavus foot: A randomized controlled trial. Medicine 2019, 98, e18018. [Google Scholar] [CrossRef]
- Fernández-Seguín, L.M.; Munuera, P.V.; Pena-Algaba, C.; Ortega, J.R.; Díaz-Morales, J.A.; Escamilla-Martínez, E. Effectiveness of neuromuscular stretching with symmetrical biphasic electric currents in the cavus foot. J. Am. Podiatr. Med. Assoc. 2013, 103, 191–196. [Google Scholar]
- Moisan, G.; Descarreaux, M.; Cantin, V. Biomechanical effects of foot orthoses with and without a lateral bar in individuals with cavus feet during comfortable and fast walking. PLoS ONE 2021, 16, e0248658. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.K.; Cha, E.J.; Kim, K.A.; Won, Y.; Kim, J.J. Effects of custom-made insoles on idiopathic pes cavus foot during walking. Biomed. Mater. Eng. 2015, 26 (Suppl. 1), S705–S715. [Google Scholar] [CrossRef] [Green Version]
- Myerson, M.S.; Myerson, C.L. Cavus Foot: Deciding Between Osteotomy and Arthrodesis. Foot Ankle Clin. 2019, 24, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.G.; Park, J.T.; Lee, S.H. Joint-sparing correction for idiopathic cavus foot: Correlation of clinical and radiographic results. Foot Ankle Clin. 2013, 18, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.; Shah, A.; Staggers, J.R.; Pinto, M.; Godoy-Santos, A.L.; Naranje, S.; de Cesar Netto, C. Anatomic Evaluation of Percutaneous Achilles Tendon Lengthening. Foot Ankle Int. 2018, 39, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Oesman, I.; Sari, C.M. Neglected neurogenic clubfoot treated with Achilles tendon lengthening using Z-plasty, total talectomy, and tibiocalcaneal arthrodesis. Int. J. Surg. Case Rep. 2021, 84, 106051. [Google Scholar] [CrossRef]
- Anderson, J.G.; Bohay, D.R.; Eller, E.B.; Witt, B.L. Gastrocnemius recession. Foot Ankle Clin. 2014, 19, 767–786. [Google Scholar] [CrossRef]
- Maes, R.; Safar, A.; Ghistelinck, B.; Labadens, A.; Hernigou, J. Percutaneous plantar fasciotomy: Radiological evolution of medial longitudinal arch and clinical results after one year. Int. Orthop. 2021, 46, 861–866. [Google Scholar] [CrossRef]
- Kiskaddon, E.M.; Meeks, B.D.; Roberts, J.G.; Laughlin, R.T. Plantar Fascia Release Through a Single Lateral Incision in the Operative Management of a Cavovarus Foot: A Cadaver Model Analysis of the Operative Technique. J. Foot Ankle Surg. 2018, 57, 681–684. [Google Scholar] [CrossRef]
- Kim, B.S. Reconstruction of Cavus Foot: A Review. Open Orthop. J. 2017, 11, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Ward, C.M.; Dolan, L.A.; Bennett, D.L.; Morcuende, J.A.; Cooper, R.R. Long-term results of reconstruction for treatment of a flexible cavovarus foot in Charcot-Marie-Tooth disease. J. Bone Jt. Surg. Am. 2008, 90, 2631–2642. [Google Scholar] [CrossRef]
- Singh, A.K.; Briggs, P.J. Metatarsal extension osteotomy without plantar aponeurosis release in cavus feet. The effect on claw toe deformity a radiographic assessment. Foot Ankle Surg. 2012, 18, 210–212. [Google Scholar] [CrossRef]
- Pirozzi, K.; Meyr, A.J. Using Geometry for the Dorsiflexory Wedge Osteotomy of the First Metatarsal. J. Foot Ankle Surg. 2014, 53, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Lui, T.H. Percutaneous sagittal plane closing wedge osteotomy of the first metatarsal. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Leeuwesteijn, A.E.; de Visser, E.; Louwerens, J.W. Flexible cavovarus feet in Charcot-Marie-Tooth disease treated with first ray proximal dorsiflexion osteotomy combined with soft tissue surgery: A short-term to mid-term outcome study. Foot Ankle Surg. 2010, 16, 142–147. [Google Scholar] [CrossRef]
- Kurar, L.; Nash, W.; Faroug, R.; Hussain, L.; Walker, R.; Abbasian, A.; Latif, A.; Singh, S. Making Things Easier: A Simple Novel Method to Fix a Dorsiflexion Osteotomy of the First Metatarsal. J. Med. Life 2020, 13, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Maskill, M.P.; Maskill, J.D.; Pomeroy, G.C. Surgical management and treatment algorithm for the subtle cavovarus foot. Foot Ankle Int. 2010, 31, 1057–1063. [Google Scholar] [CrossRef]
- Jahss, M.H. Tarsometatarsal truncated-wedge arthrodesis for pes cavus and equinovarus deformity of the fore part of the foot. J. Bone Jt. Surg. Am. 1980, 62, 713–722. [Google Scholar] [CrossRef]
- Grady, J.F.; Schumann, J.; Cormier, C.; LaViolette, K.; Chinn, A. Management of Midfoot Cavus. Clin. Podiatr. Med. Surg. 2021, 38, 391–410. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.S.; Jones, K.; Jonah, D.; Dicintio, M.S. Management of the rigid cavus foot in children and adolescents. Foot Ankle Clin. 2013, 18, 727–741. [Google Scholar] [CrossRef]
- Saunders, J. Etiology and treatment of clawfoot. Arch. Surg. 1935, 30, 2. [Google Scholar] [CrossRef]
- Cole, W.H. The treatment of claw foot. J. Bone Jt. Surg. Am. 1940, 22, 895–908. [Google Scholar]
- Tullis, B.L.; Mendicino, R.W.; Catanzariti, A.R.; Henne, T.J. The Cole midfoot osteotomy: A retrospective review of 11 procedures in 8 patients. J. Foot Ankle Surg. 2004, 43, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Ergun, S.; Yildirim, Y. The Cole Midfoot Osteotomy: Clinical and Radiographic Retrospective Review of Five Patients (Six Feet) with Different Etiologies. J. Am. Podiatr. Med. Assoc. 2019, 109, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Japas, L.M. Surgical treatment of pes cavus by tarsal V-osteotomy. Preliminary report. J. Bone Jt. Surg. Am. 1968, 50, 927–944. [Google Scholar] [CrossRef]
- Giannini, S.; Ceccarelli, F.; Benedetti, M.G.; Faldini, C.; Grandi, G. Surgical treatment of adult idiopathic cavus foot with plantar fasciotomy, naviculocuneiform arthrodesis, and cuboid osteotomy. A review of thirty-nine cases. J. Bone Jt. Surg. Am. 2002, 84-A (Suppl. 2), 62–69. [Google Scholar]
- Chatterjee, P.; Sahu, M.K. A prospective study of Japas’ osteotomy in paralytic pes cavus deformity in adolescent feet. Indian J. Orthop. 2009, 43, 281–285. [Google Scholar] [CrossRef]
- Wilcox, P.G.; Weiner, D.S. The Akron midtarsal dome osteotomy in the treatment of rigid pes cavus: A preliminary review. J. Pediatr. Orthop. 1985, 5, 333–338. [Google Scholar] [CrossRef]
- Weiner, D.S.; Morscher, M.; Junko, J.T.; Jacoby, J.; Weiner, B. The Akron dome midfoot osteotomy as a salvage procedure for the treatment of rigid pes cavus: A retrospective review. J. Pediatr. Orthop. 2008, 28, 68–80. [Google Scholar] [CrossRef]
- Boquan, Q.; Yi, R.; Tingjiang, G.; Xi, L.; Hui, Z. Complex foot deformities associated with lower limb deformities: A new therapeutic strategy for simultaneous correction using Ilizarov procedure together with osteotomy and soft tissue release. J. Orthop. Surg. Res. 2020, 15, 492. [Google Scholar] [CrossRef]
- Jeong, B.O.; Kim, T.Y.; Song, W.J. Use of Ilizarov External Fixation Without Soft Tissue Release to Correct Severe, Rigid Equinus Deformity. J. Foot Ankle Surg. 2015, 54, 821–825. [Google Scholar] [CrossRef] [Green Version]
- Bariteau, J.T.; Blankenhorn, B.D.; Tofte, J.N.; DiGiovanni, C.W. What is the role and limit of calcaneal osteotomy in the cavovarus foot? Foot Ankle Clin. 2013, 18, 697–714. [Google Scholar] [CrossRef]
- Boffeli, T.J.; Collier, R.C. Surgical technique for combined Dwyer calcaneal osteotomy and peroneal tendon repair for correction of peroneal tendon pathology associated with cavus foot deformity. J. Foot Ankle Surg. 2012, 51, 135–140. [Google Scholar] [CrossRef] [PubMed]
- An, T.W.; Michalski, M.; Jansson, K.; Pfeffer, G. Comparison of Lateralizing Calcaneal Osteotomies for Varus Hindfoot Correction. Foot Ankle Int. 2018, 39, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Krause, F.G.; Sutter, D.; Waehnert, D.; Windolf, M.; Schwieger, K.; Weber, M. Ankle joint pressure changes in a pes cavovarus model after lateralizing calcaneal osteotomies. Foot Ankle Int. 2010, 31, 741–746. [Google Scholar] [CrossRef]
- Pfeffer, G.B.; Michalski, M.P.; Basak, T.; Giaconi, J.C. Use of 3D Prints to Compare the Efficacy of Three Different Calcaneal Osteotomies for the Correction of Heel Varus. Foot Ankle Int. 2018, 39, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Barg, A.; Ruiz, R.; Hintermann, B. Triple arthrodesis for correction of cavovarus deformity. Oper. Orthop. Traumatol. 2017, 29, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Krause, F.G.; Wing, K.J.; Younger, A.S. Neuromuscular issues in cavovarus foot. Foot Ankle Clin. 2008, 13, 243–258. [Google Scholar] [CrossRef]
- Steinau, H.U.; Tofaute, A.; Huellmann, K.; Goertz, O.; Lehnhardt, M.; Kammler, J.; Steinstraesser, L.; Daigeler, A. Tendon transfers for drop foot correction: Long-term results including quality of life assessment, and dynamometric and pedobarographic measurements. Arch Orthop. Trauma. Surg. 2011, 131, 903–910. [Google Scholar] [CrossRef]
- Sugathan, H.K.; Sherlock, D.A. A modified Jones procedure for managing clawing of lesser toes in pes cavus: Long-term follow-up in 8 patients. J Foot Ankle Surg. 2009, 48, 637–641. [Google Scholar] [CrossRef]
- Faldini, C.; Traina, F.; Nanni, M.; Mazzotti, A.; Calamelli, C.; Fabbri, D.; Pungetti, C.; Giannini, S. Surgical treatment of cavus foot in Charcot-Marie-tooth disease: A review of twenty-four cases: AAOS exhibit selection. J Bone Jt. Surg. Am. 2015, 97, e30. [Google Scholar] [CrossRef] [Green Version]
- Grambart, S.T. Hibbs Tenosuspension. Clin. Podiatr. Med. Surg. 2016, 33, 63–69. [Google Scholar] [CrossRef]
- Dagneaux, L.; Canovas, F. 3D Printed Patient-Specific Cutting Guide for Anterior Midfoot Tarsectomy. Foot Ankle Int. 2020, 41, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Sobron, F.B.; Dos Santos-Vaquinhas, A.; Alonso, B.; Parra, G.; Perez-Mananes, R.; Vaquero, J. Technique tip: 3D printing surgical guide for pes cavus midfoot osteotomy. Foot Ankle Surg. 2021, 28, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Michalski, M.P.; Gonzalez, T.A.; Metzger, M.F.; Nelson, T.J.; Eberlein, S.; Pfeffer, G.B. Biomechanical Comparison of Achilles Tendon Pullout Strength Following Midline Tendon-Splitting and Endoscopic Approaches for Calcaneoplasty. Foot Ankle Int. 2019, 40, 1219–1225. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Congenital | Friedreich’s ataxia Traumatic brain injury Spina bifida Syringomyelia Filum terminale lipoma Tethered cord syndrome |
| Clubfoot Tarsal Coalition | |
| Peripheral nervous system | |
| Charcot-Marie-Tooth disease Guillain-Barre syndrome Peripheral neuropathy | |
| Central nervous system | Traumatic |
| Cerebral palsy Spinal cord tumor Stroke Amyotrophic lateral sclerosis Poliomyelitis Huntington’s chorea | Crush injury Postburn contracture Talar neck fracture malunion Peroneal nerve injury Crush injury |
| Forefoot |
| Metatarsalgia |
| Stress fracture of the fifth metatarsal |
| Callus under first, fifth metatarsal heads |
| Claw-toes |
| Metatarsus adductus |
| Midfoot |
| Midfoot arthritis |
| Talar subluxation |
| Hindfoot |
| Plantar fasciitis |
| Achilles tendinitis |
| Subtalar unstable |
| Peroneal tendons subluxation |
| Peroneal tendon problems (tear or split, rupture, tendinopathy) |
| Ankle |
| Chronic lateral ankle instability |
| Varus ankle arthritis |
| Gait |
| Limp |
| Soft-Tissue Release | ||
| Contracture of the plantar fascia | → | Open or Percutaneous plantar fasciotomy |
| Overpull of the intrinsic muscle | → | Steindler stripping |
| Ankle varus deformity | → | Lateral ankle ligament reconstruction |
| Deltoid ligament release | ||
| Ankle equinus deformity | → | Gastrocnemius recession |
| Achilles tendon lengthening | ||
| Severe rigid deformity | → | Combined with other tendon release |
| Bony Reconstruction | ||
| Forefoot deformity | ||
| The first TMT equinus | → | First metatarsal dorsiflexion osteotomy |
| The multiple metatarsals equinus | → | Jahss osteotomy |
| Midfoot deformity | ||
| The apex at the NC joint or cuneiforms | → | Cole/Japas/Akron/Myerson osteotomy * |
| Ilizarov external fixation | ||
| Hindfoot deformity | ||
| Nonreducible mild heel varus | → | Dwyer osteotomy |
| Nonreducible severe heel varus | → | Z-shaped osteotomy |
| Mixed deformity | ||
| Rigid deformity with osteoarthritis | → | Double or Triple arthrodesis |
| Naviculocuneiform arthrodesis | ||
| Soft-tissue Balancing | ||
| Weakness of the peroneus brevis | → | Peroneus longus to brevis transfer |
| Overpower of the posterior tibial tendon | → | Posterior tibial tendon transfer |
| The claw-toes | → | Jones procedure |
| Hibbs procedure | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, B.; Wu, S.; Zhang, H. Evaluation and Management of Cavus Foot in Adults: A Narrative Review. J. Clin. Med. 2022, 11, 3679. https://doi.org/10.3390/jcm11133679
Qin B, Wu S, Zhang H. Evaluation and Management of Cavus Foot in Adults: A Narrative Review. Journal of Clinical Medicine. 2022; 11(13):3679. https://doi.org/10.3390/jcm11133679
Chicago/Turabian StyleQin, Boquan, Shizhou Wu, and Hui Zhang. 2022. "Evaluation and Management of Cavus Foot in Adults: A Narrative Review" Journal of Clinical Medicine 11, no. 13: 3679. https://doi.org/10.3390/jcm11133679
APA StyleQin, B., Wu, S., & Zhang, H. (2022). Evaluation and Management of Cavus Foot in Adults: A Narrative Review. Journal of Clinical Medicine, 11(13), 3679. https://doi.org/10.3390/jcm11133679