
Which Explanatory Variables Contribute to the Classification of Good Visual Acuity over Time in Patients with Branch Retinal Vein Occlusion with Macular Edema Using Machine Learning?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Treatment Regimen
2.2. Grouping into Two Groups Based on Visual Acuity over Time
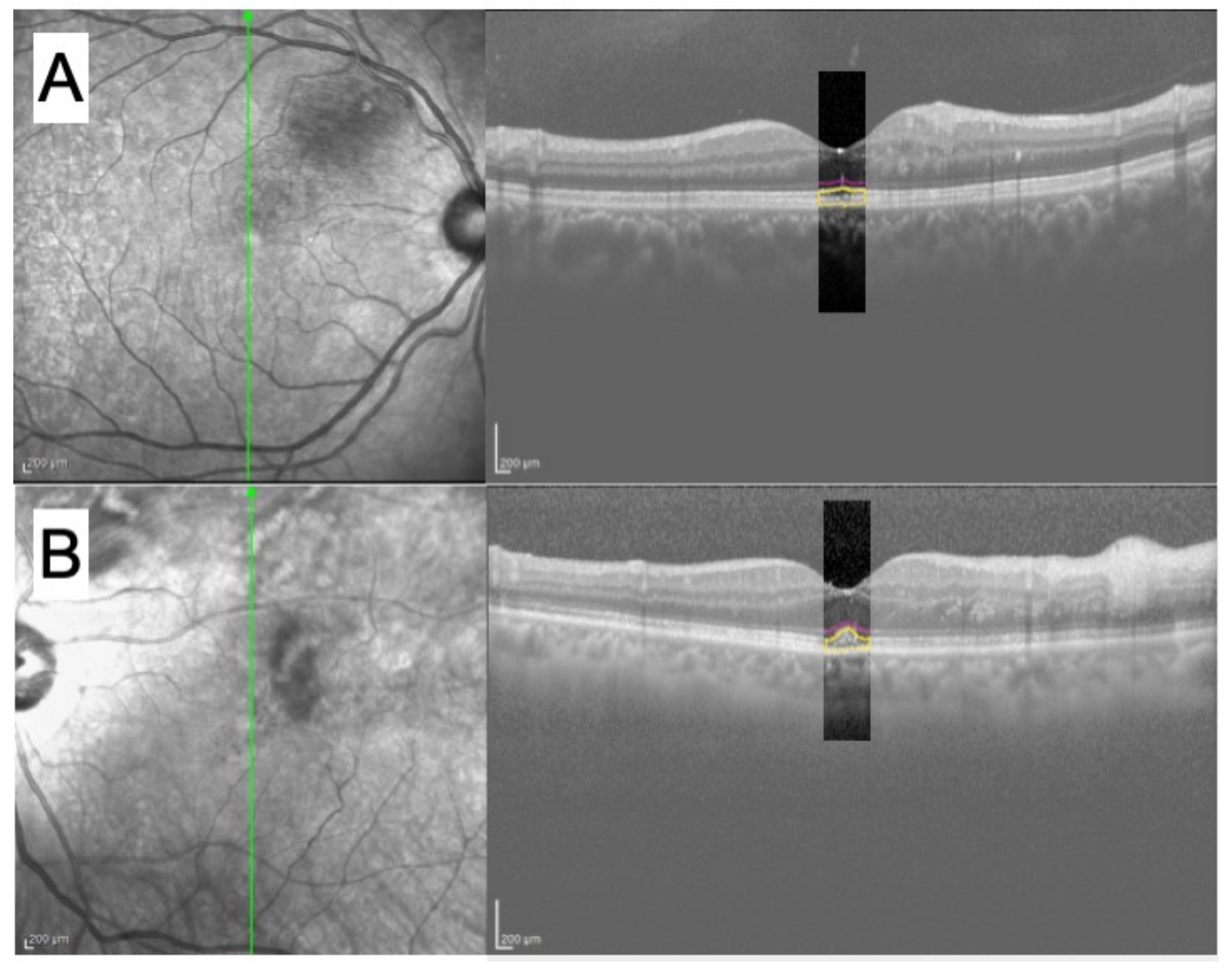
2.3. Preprocessing of OCT Images and Features from OCT Images
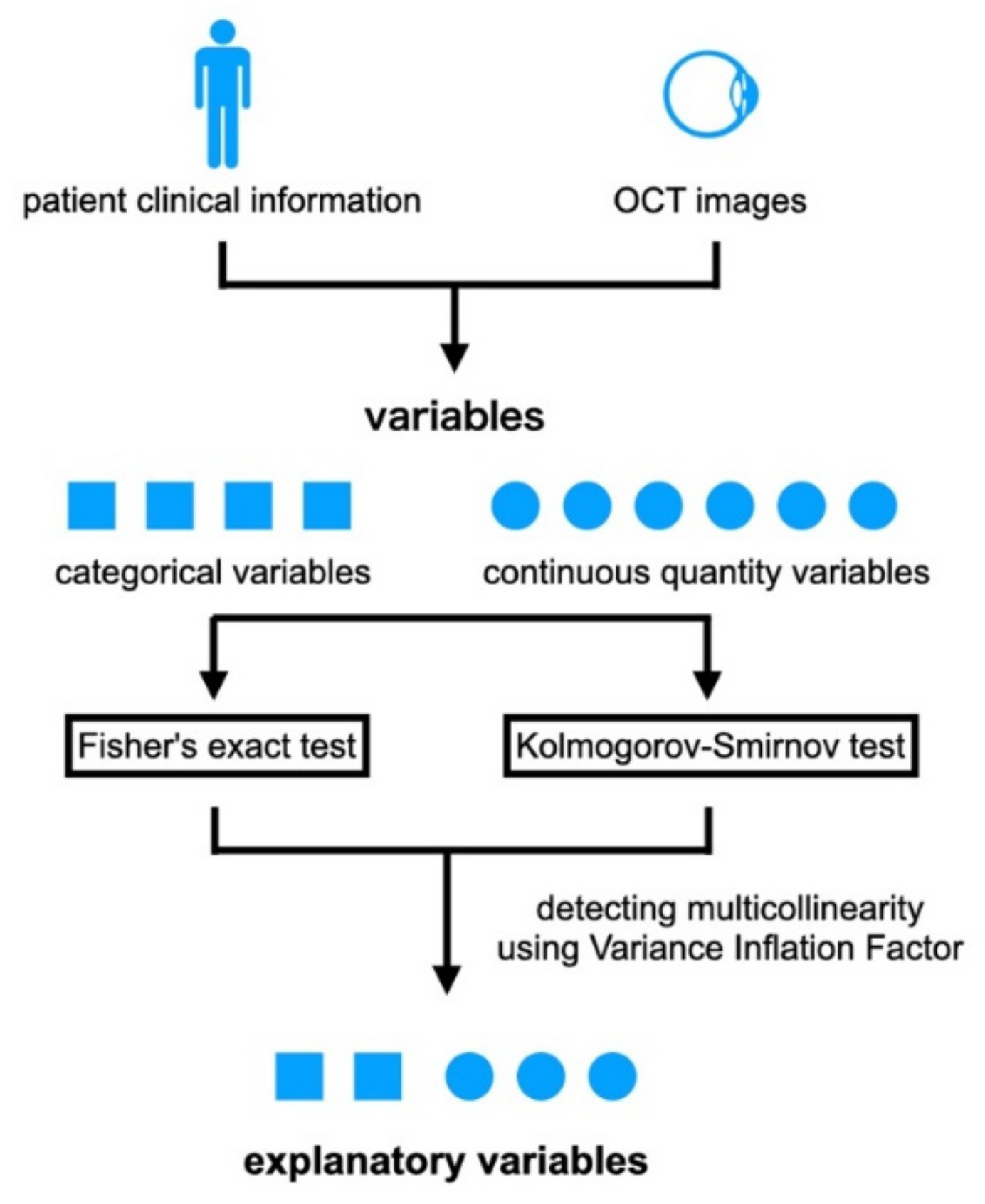
2.4. Selection of Explanatory Variables
2.5. Machine-Learning Algorithm
3. Results
3.1. Demographics of Each Group
3.2. Explanatory Variables
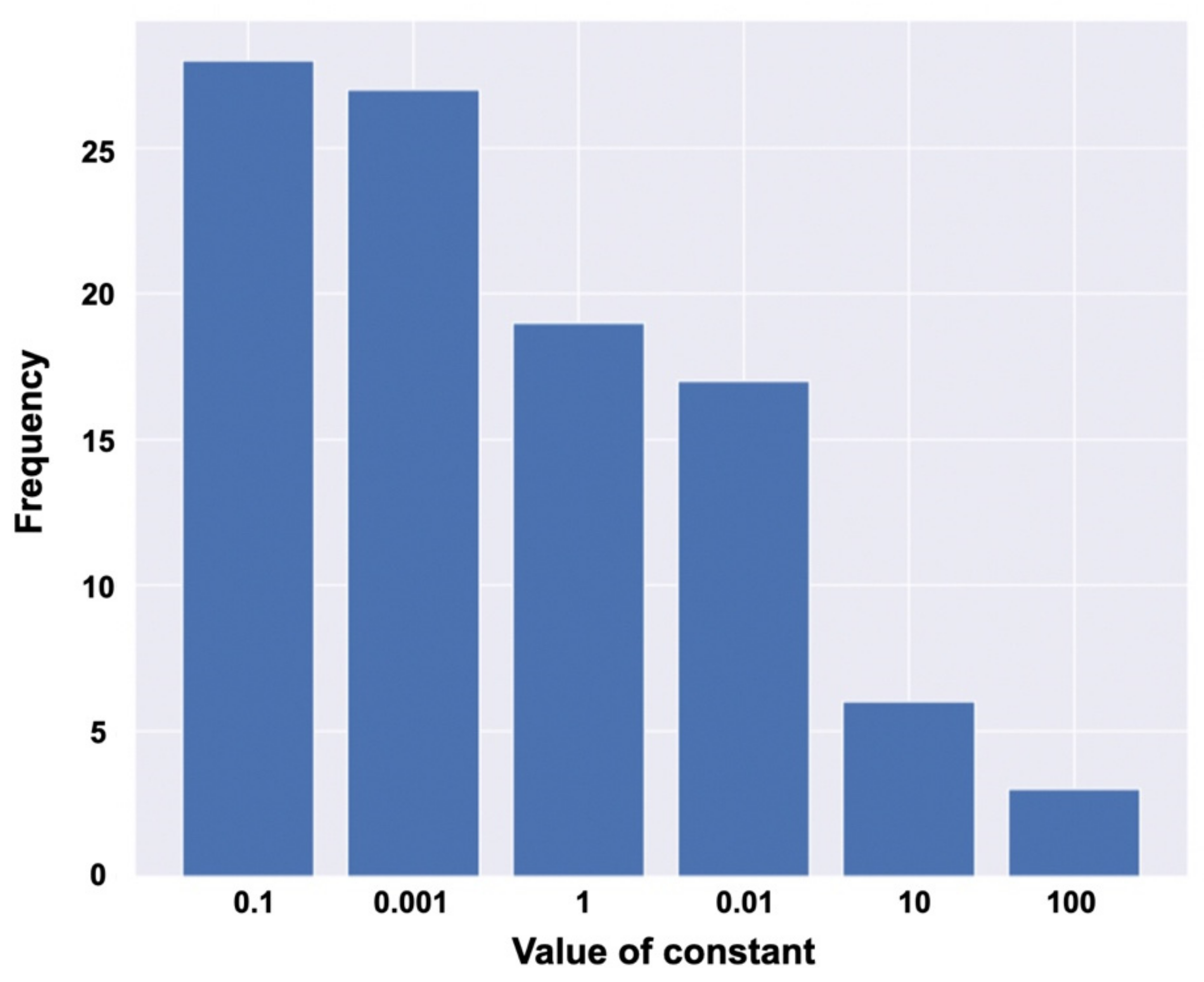
3.3. Hyperparameters of Logistic Regression
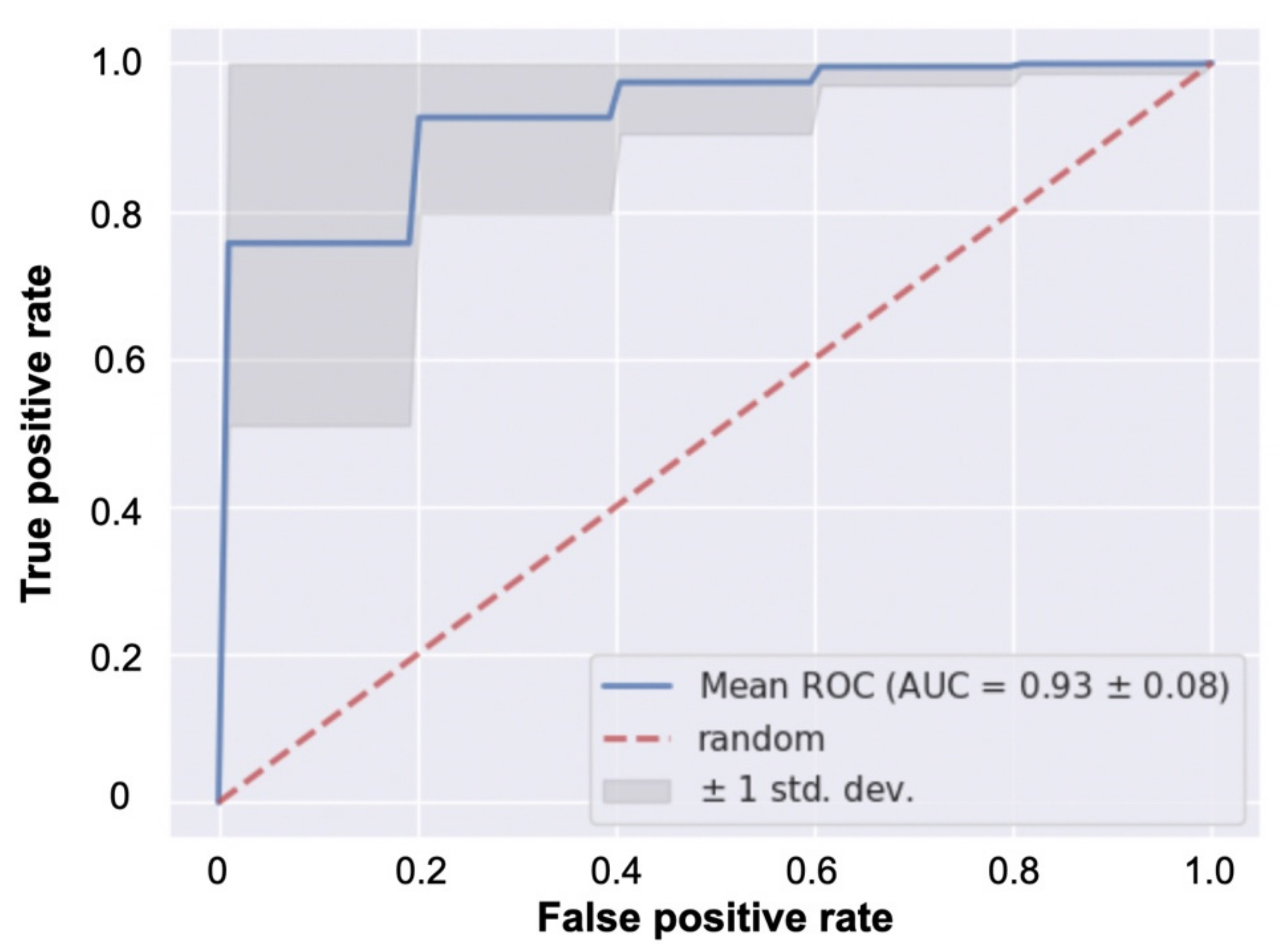
3.4. Classification Performance
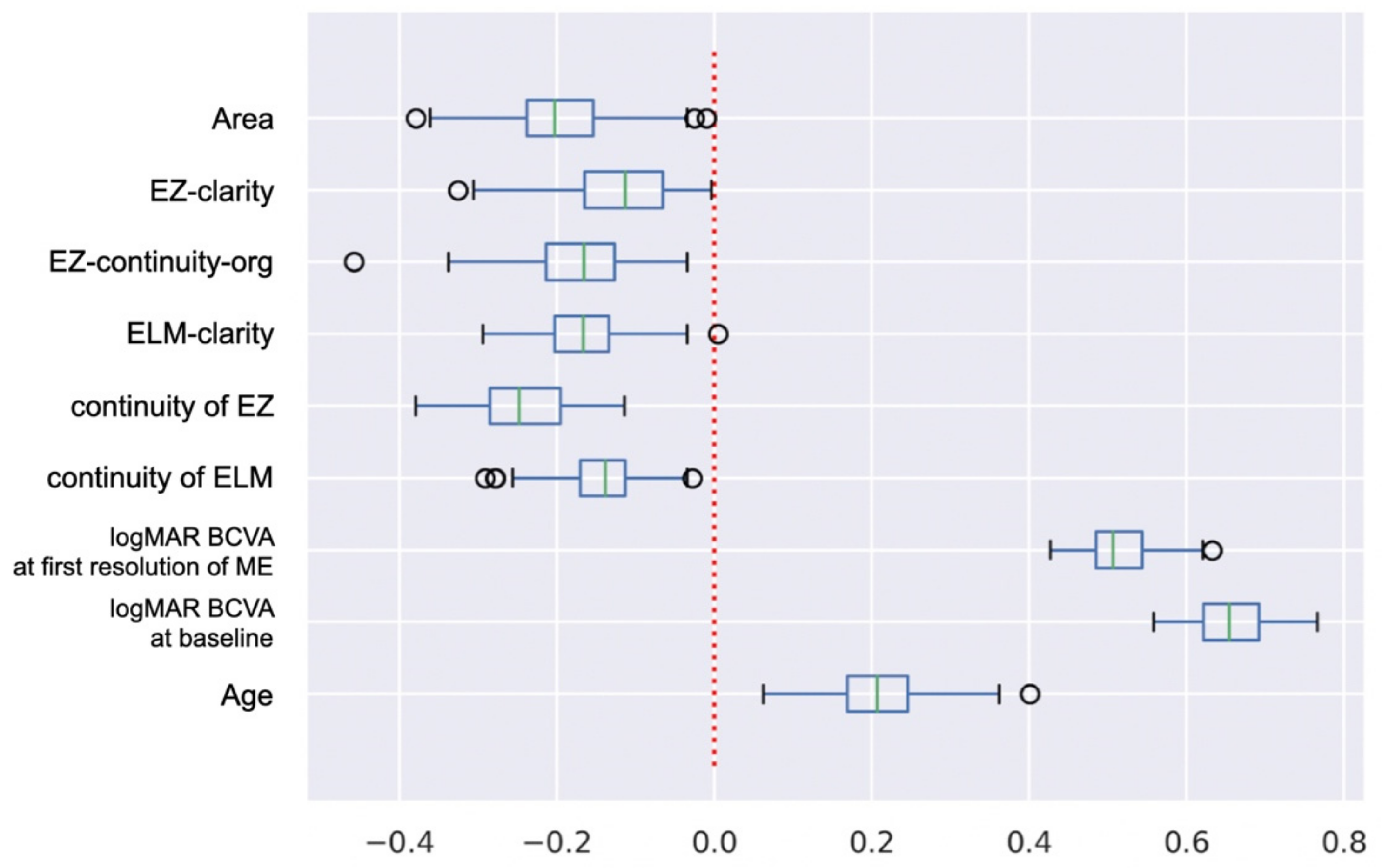
3.5. Specific Contribution of Explanatory Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Branch Vein Occlusion Study Group. Argon laser scatter photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. A randomized clinical trial. Brunch Vein Occlusion Study Group. Arch. Ophthalmol. 1986, 104, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Sruthi, A.; Angela, B.; Peter, K.K. Branch vein occlusion. In Ryan’s Retina E-Book, 7th ed.; Sadda, S.R., Schachat, A.P., Wilikinson, C.P., Hinton, D.R., Wiedemann, P., Freund, K.B., Sarraf, D., Eds.; Elsevier Health Science: Amsterdam, The Netherlands, 2022; Volume 2, pp. 1176–1187. [Google Scholar]
- Shilling, J.S.; Jones, C.A. Retinal branch vein occlusion: A study of argon laser photocoagulation in the treatment of macular oedema. Br. J. Ophthalmol. 1984, 68, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Campochiaro, P.A.; Bhisitkul, R.B.; Ho, A.C.; Gray, S.; Saroj, N.; Adamis, A.P.; Rubio, R.G.; Murahashi, W.Y. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology 2011, 118, 1594–1602. [Google Scholar] [CrossRef]
- Sakanishi, Y.; Lee, A.; Usui-Ouchi, A.; Ito, R.; Ebihara, N. Twelve-month outcomes in patients with retinal vein occlusion treated with low-frequency intravitreal ranibizumab. Clin. Ophthalmol. 2016, 10, 1161. [Google Scholar] [CrossRef] [Green Version]
- Miwa, Y.; Muraoka, Y.; Osaka, R.; Ooto, S.; Murakami, T.; Suzuma, K. Ranibizumab for macular edema after branch retinal vein occlusion: One initial injection versus three monthly injections. Retina 2017, 37, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Ang, J.L.; Ah-Moye, S.; Kim, L.N.; Nguyen, V.; Hunt, A.; Barthelmes, D.; Mehta, H.A. Systematic review of real-world evidence of the management of macular oedema secondary to branch retinal vein occlusion. Eye 2020, 34, 1770–1796. [Google Scholar] [CrossRef]
- Gallardo, M.; Munk, M.R.; Kurmann, T.; De Zanet, S.; Mosinska, A.; Karagoz, I.K.; Wolf, S. Machine learning can predict anti-VEGF treatment demand in a Treat-and-Extend regimen for patients with nAMD, DME and RVO associated ME. Ophthalmol. Retin. 2021, 5, 604–624. [Google Scholar] [CrossRef] [PubMed]
- Tomiyasu, T.; Hirano, Y.; Yoshida, M.; Suzuki, N.; Nishiyama, T.; Uemura, A.; Ogura, Y. Microaneurysms cause refractory macular edema in branch retinal vein occlusion. Sci. Rep. 2016, 6, 29445. [Google Scholar] [CrossRef]
- Iida-Miwa, Y.; Muraoka, Y.; Iida, Y.; Ooto, S.; Murakami, T.; Suzuma, K.; Tsujikawa, A. Branch retinal vein occlusion: Treatment outcomes according to the retinal nonperfusion area, clinical subtype, and crossing pattern. Sci. Rep. 2019, 9, 6569. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ueda, T.; Okamoto, M.; Ogata, N. Presence of foveal bulge in optical coherence tomographic images in eyes with macular edema associated with branch retinal vein occlusion. Am. J. Ophthalmol. 2014, 157, 390–396. [Google Scholar] [CrossRef]
- Shiono, A.; Kogo, J.; Sasaki, H.; Yomoda, R.; Jujo, T.; Tokuda, N.; Takagi, H. Optical coherence tomography findings as a predictor of clinical course in patients with branch retinal vein occlusion treated with ranibizumab. PLoS ONE 2018, 13, e0199552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, H.M.; Chung, E.J.; Kim, Y.M.; Koh, H.J. Spectral-domain optical coherence tomography (SD-OCT) patterns and response to intravitreal bevacizumab therapy in macular edema associated with branch retinal vein occlusion. Graefes. Arch. Clin. Exp. Ophthalmol. 2013, 251, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Masuda, N.; Ogata, N. Highly reflective line in optical coherence tomography images of eyes with macular edema associated with branch retinal vein occlusion. Am. J. Ophthalmol. 2015, 159, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Thomas, A.S.; Berry, D.; Yoon, S.; Fekrat, S.; Grewal, D.S. Association of retinal inner layer disorganization with ultra-widefield fluorescein angiographic features and visual acuity in branch retinal vein occlusion. Ophthalmic Surg. Lasers Imaging Retin. 2019, 50, 354–364. [Google Scholar] [CrossRef]
- Matsui, Y.; Imamura, K.; Ooka, M.; Chujo, S.; Mase, Y.; Matsubara, H.; Kawanaka, H.; Mineo, K. Classification of good visual acuity over time in patients with branch retinal vein occlusion with macular edema using support vector machine. Graefes. Arch. Clin. Exp. Ophthalmol. 2022, 260, 1501–1508. [Google Scholar] [CrossRef]
- The official Website of the GNU Image Manipulation Program. Available online: https://www.gimp.org (accessed on 1 April 2022).
- Matsui, Y.; Kondo, M.; Uchiyama, E.; Miyata, R.; Matsubara, H. New clinical ultrahigh-resolution SD-OCT using A-scan matching algorithm. Graefes. Arch. Clin. Exp. Ophthalmol. 2019, 25, 255–263. [Google Scholar] [CrossRef]
- Menard, S. Applied Logistic Regression Analysis, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2002; Volume 106. [Google Scholar]
- The official Website of Scikit-Learn. Available online: https://scikit-learn.org/stable/ (accessed on 1 April 2022).
- Campochiaro, P.A.; Hafiz, G.; Channa, R.; Shah, S.M.; Nguyen, Q.D.; Ying, H.; Syed, B. Antagonism of vascular endothelial growth factor for macular edema caused by retinal vein occlu- sions: Two-year outcomes. Ophthalmology 2010, 117, 2387–2394. [Google Scholar] [CrossRef]
- Sakanishi, Y.; Yasuda, K.; Morita, S.; Mashimo, K.; Tamaki, K.; Sakuma, T.; Ebihara, N. Twenty-four-month results of intravitreal aflibercept for macular edema due to branch retinal vein occlusion. Jpn. J. Ophthalmol. 2021, 65, 63–68. [Google Scholar] [CrossRef]
- Minami, Y.; Nagaoka, T.; Ishibazawa, A.; Yoshida, A. Correlation between short-and long-term effects of intravitreal ranibizumab therapy on macular edema after branch retinal vein occlusion: A prospective observational study. BMC Ophthalmol. 2017, 17, 90. [Google Scholar] [CrossRef] [Green Version]
- Ota, M.; Tsujikawa, A.; Murakami, T.; Yamaike, N.; Sakamoto, A.; Kotera, Y.; Miyamoto, K.; Kita, M.; Yoshimura, N. Foveal photoreceptor layer in eyes with persistent cystoid macular edema associated with branch retinal vein occlusion. Am. J. Ophthalmol. 2008, 145, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Curcio, C.A.; Sloan, K.R.; Kalina, R.E.; Hendrickson, A.E. Human photoreceptor topography. J. Comp. Neurol. 1990, 292, 497–523. [Google Scholar] [CrossRef] [PubMed]
- Legras, R.; Gaudric, A.; Woog, K. Distribution of cone density, spacing and arrangement in adult healthy retinas with adaptive optics flood illumination. PLoS ONE 2018, 13, e0191141. [Google Scholar] [CrossRef] [PubMed]
- Woog, K.; Legras, R. Visual resolution and cone spacing in the nasal and inferior retina. Ophthalmic Physiol. Opt. 2018, 38, 66–75. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 66) | Group A (n = 23) | Group B (n = 43) | p Value |
|---|---|---|---|---|
| Men, n (%) | 36 (54.5) | 17 (73.9) | 19 (44.2) | 0.368 |
| Age (y), mean ± SD | 67.2 ± 9.4 | 63.6 ± 12.1 | 69.2 ± 6.9 | 0.024 * |
| Duration from onset to treatment (weeks), mean ± SD | 6.86 ± 7.05 | 4.96 ± 3.34 | 7.90 ± 8.28 | 0.147 |
| Type, Major/macula (%) | 44(66.7)/22(33.3) | 15(22.7)/8(12.1) | 29(44.0)/14(21.2) | 1 |
| Affected eye, right/left (%) | 35(53.0)/31(47.0) | 10(15.2)/13(19.7) | 25(37.9)/18(27.3) | 0.299 |
| Location of affected semifield, superior/inferior (%) | 48(72.7)/18(27.3) | 17(25.8)/6(9.1) | 31(47.0)/12(18.2) | 1 |
| logMAR BCVA at baseline, mean ± SD | 0.41 ± 0.30 | 0.15 ± 0.15 | 0.54 ± 0.28 | <0.001 * |
| logMAR BCVA at first resolution of ME, mean ± SD | 0.22 ± 0.24 | 0.04 ± 0.09 | 0.32 ± 0.24 | <0.001 * |
| Period from initial treatment to the first resolution of ME (weeks), mean ± SD | 4.5 ± 1.6 | 4.5 ± 1.4 | 4.5 ± 1.7 | 0.147 |
| logMAR BCVA at 12 months, mean ± SD | 0.01 ± 0.16 | −0.01 ± 0.06 | 0.16 ± 0.17 | <0.001 ** |
| Number of anti-VEGF therapy at 12 months | 3.2 ± 1.9 | 2.6 ± 2.0 | 3.5 ± 1.9 | 0.26 |
| Variables | All (n = 66) | Group A (n = 23) | Group B (n = 43) | p Value |
|---|---|---|---|---|
| Continuity of ELM, defect/discontinuous/continuous (%) | 6(9.1)/12(18.2)/48(72.7) | 0/1(1.5)/22(33.3) | 6(9.1)/11(16.7)/26(39.4) | 0.007 * |
| Continuity of EZ, defect/discontinuous/continuous (%) | 8(12.1)/26(39.4)/32(48.5) | 0/5(7.6)/18(27.3) | 8(12.1)/21(31.8)/14(21.2) | <0.001 * |
| ELM-continuity-org | 5021 ± 1271 | 5019 ± 1358 | 5021 ± 1271 | 0.295 |
| ELM-clarity | 1.14 ± 0.12 | 1.20 ± 0.10 | 1.10 ± 0.12 | 0.001 * |
| EZ-continuity-org | 6911 ± 2352 | 8140 ± 1827 | 6239 ± 2353 | 0.006 * |
| EZ-clarity | 1.14 ± 0.12 | 1.21 ± 0.11 | 1.11 ± 0.12 | <0.001 * |
| Area | 615 ± 203 | 689 ± 124 | 576 ± 228 | 0.006 * |
| Variables | R2 Score | Judge |
|---|---|---|
| Age | 0.115 | False |
| logMAR BCVA at baseline | 0.382 | False |
| logMAR BCVA at first resolution of ME | 0.613 | False |
| Continuity of ELM | 0.623 | False |
| Continuity of EZ | 0.638 | False |
| ELM-clarity | 0.655 | False |
| EZ-continuity-org | 0.416 | False |
| EZ-clarity | 0.595 | False |
| Area | 0.362 | False |
| Variables | Mean | SD | 95% Confidence Interval of the Mean | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| logMAR BCVA at baseline | 0.656 | 0.049 | 0.646 | 0.666 |
| logMAR BCVA at first resolution of ME | 0.513 | 0.039 | 0.505 | 0.521 |
| Age | 0.210 | 0.070 | 0.196 | 0.224 |
| EZ-clarity | −0.119 | 0.069 | −0.133 | −0.105 |
| Continuity of ELM | −0.144 | 0.050 | −0.154 | −0.134 |
| ELM-clarity | −0.170 | 0.062 | −0.182 | −0.158 |
| EZ-continuity-org | −0.173 | 0.075 | −0.188 | −0.158 |
| Area | −0.198 | 0.076 | −0.213 | −0.183 |
| Continuity of EZ | −0.244 | 0.059 | −0.255 | −0.232 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsui, Y.; Imamura, K.; Chujo, S.; Mase, Y.; Matsubara, H.; Sugimoto, M.; Kawanaka, H.; Kondo, M. Which Explanatory Variables Contribute to the Classification of Good Visual Acuity over Time in Patients with Branch Retinal Vein Occlusion with Macular Edema Using Machine Learning? J. Clin. Med. 2022, 11, 3903. https://doi.org/10.3390/jcm11133903
Matsui Y, Imamura K, Chujo S, Mase Y, Matsubara H, Sugimoto M, Kawanaka H, Kondo M. Which Explanatory Variables Contribute to the Classification of Good Visual Acuity over Time in Patients with Branch Retinal Vein Occlusion with Macular Edema Using Machine Learning? Journal of Clinical Medicine. 2022; 11(13):3903. https://doi.org/10.3390/jcm11133903
Chicago/Turabian StyleMatsui, Yoshitsugu, Kazuya Imamura, Shinichiro Chujo, Yoko Mase, Hisashi Matsubara, Masahiko Sugimoto, Hiroharu Kawanaka, and Mineo Kondo. 2022. "Which Explanatory Variables Contribute to the Classification of Good Visual Acuity over Time in Patients with Branch Retinal Vein Occlusion with Macular Edema Using Machine Learning?" Journal of Clinical Medicine 11, no. 13: 3903. https://doi.org/10.3390/jcm11133903
APA StyleMatsui, Y., Imamura, K., Chujo, S., Mase, Y., Matsubara, H., Sugimoto, M., Kawanaka, H., & Kondo, M. (2022). Which Explanatory Variables Contribute to the Classification of Good Visual Acuity over Time in Patients with Branch Retinal Vein Occlusion with Macular Edema Using Machine Learning? Journal of Clinical Medicine, 11(13), 3903. https://doi.org/10.3390/jcm11133903