
Topical Steroids and Glaucoma Filtration Surgery Outcomes: An In Vivo Confocal Study of the Conjunctiva

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Pre-Operative Treatments and Peri-Operative Considerations
2.3. Examinations
2.4. IVCM of the Bulbar Conjunctiva
2.5. Confocal Parameters
- (i)
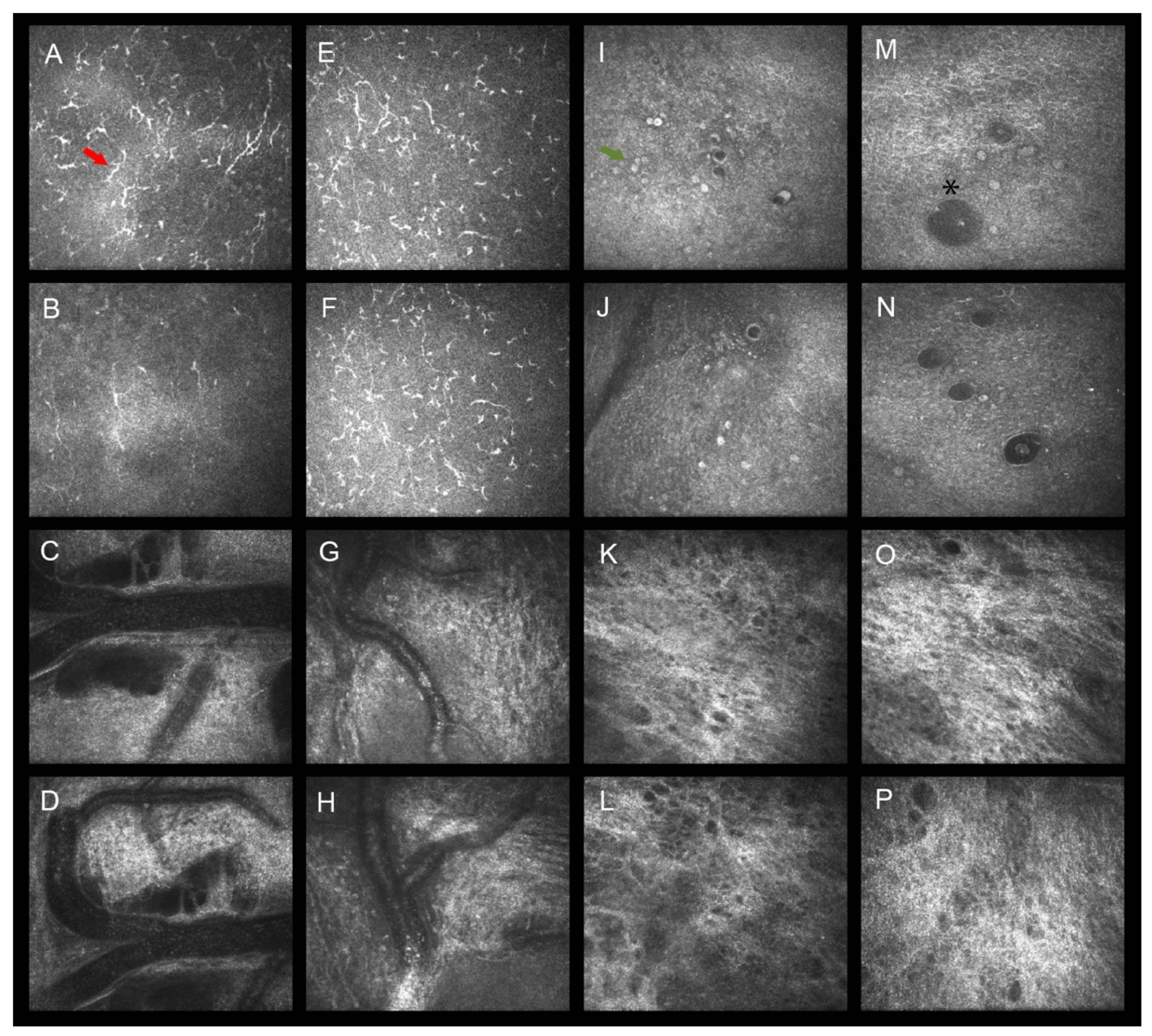
- Goblet cell density (GCD): in accordance with the definition and images provided in previous confocal studies, GCs had to appear as oval-shaped and hyperreflective cells, dispersed within the epithelium (or crowded in groups), larger than the surrounding epithelial cells, and located at a depth of 10–30 µm [7,8,9,11]. As documented, GCs act as carriers of the AH through the bleb-wall epithelium after filtration surgery [8,9,11]. The cell count software (Heidelberg Engineering GmbH) of the confocal microscope was used to determine the GCD (cells/mm2 ± SD) in manual mode.
- (ii)
- Dendritic cell density (DCD): the definition and features of DCs had to be consistent with those reported in literature [9,11,20]. DCs can appear mature and activated (hyper-reflective and elongated body, with membrane processes and frequently crowded in clusters) or immature and silent (large body with rare membrane processes, if any). They are located within the epithelium and the basal membrane of the conjunctiva (10–30 µm to 30–50 µm of depth) and act as peripheral effectors of the immune system, stimulating inflammation and fibrosis in response to toxic stimuli [20,21]. As for GCD, the cell count software was used to determine the DCD (cells/mm2 ± SD) in manual mode.
- (iii)
- Stromal meshwork reflectivity (SMR): as for GCs and DCs, the characteristics of the conjunctival stroma at IVCM had to be consistent with those reported in previous studies [9,22]. This layer (50–150 µm of depth) appears loosely arranged with thin collagen fibers and some blood vessels in the external portion but presents a denser, fibrous network with bundles of collagen fibers—occasionally hosting blood vessels, cystic spaces, and inflammatory cells—in the internal portion [22,23,24]. The tissue reflectivity represents an indirect confocal indicator of the amount of collagen fibers contained within the stroma and, thus, is a surrogate measure of the conjunctival resistivity to fluid movement. SMR was calculated as previously described, i.e., by determining the average gray value of a selected high-quality image, using the Image J software (http://imagej.nih.gov/ij/ accessed on 21 September 2021; provided in the public domain by the National Institutes of Health, Bethesda, MD, USA) [9]. SMR was graded as follows: normal (Grade 0: average gray value <90), mild (Grade 1: gray value between 90.01 and 105), moderate (Grade 2: gray value between 105.01 and 125), and high (Grade 3: >125.01), reflectivity; according to this grading scale, grades 0 to 3 corresponded to a loosely, mildly, densely, and very densely arranged stromal networks, respectively.
- (iv)
- Vessel tortuosity (VT): conjunctival vessels are located in the sub-epithelium or superficial stroma, and less frequently in the deep fibrotic portion of the stroma. They appear as broad black linear or slightly curved structures with parallel sides, frequently showing hyper-reflective and round-shaped cells within the lumen [22,23,24]. VT was assessed according to a previously adopted grading scale with four grades: straight (0), mild (1), moderate (2), and severe (3) [22]. Vessel tortuosity is an indirect indicator of stromal fibrosis and a direct indicator of chronic local inflammation [25].
2.6. Confocal Microscopy Procedure
2.7. Outcomes of the Study
2.8. Statistical Analysis
3. Results
3.1. Clinical Results
3.2. IVCM Results
3.3. Canonical Discriminant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parc, C.E.; Johnson, D.H.; Oliver, J.E.; Hattenhauer, M.G.; Hodge, D.O. The long-term outcome of glaucoma filtration surgery. Am. J. Ophthalmol. 2001, 132, 27–35. [Google Scholar] [CrossRef]
- Molteno, A.C.; Bosma, N.J.; Kittelson, J.M. Otago glaucoma surgery outcome study: Long-term results of trabeculectomy-1976 to 1995. Ophthalmology 1999, 106, 1742–1750. [Google Scholar] [CrossRef]
- Galin, M.A.; Baras, I.; McLean, J.M. The mechanism of external filtration. Am. J. Ophthalmol. 1966, 61, 3–68. [Google Scholar] [CrossRef]
- Yu, D.Y.; Morgan, W.H.; Sun, X.; Su, E.N.; Cringle, S.J.; Yu, P.K.; House, P.; Guo, W.; Yu, X. The critical role of the conjunctiva in glaucoma filtration surgery. Prog. Retin. Eye Res. 2009, 28, 303–328. [Google Scholar] [CrossRef]
- Johnson, D.H.; Yoshikawa, K.; Brubaker, R.F.; Hodge, D.O. The effect of long-term medical therapy on the outcome of filtration surgery. Am. J. Ophthalmol 1994, 117, 139–148. [Google Scholar] [CrossRef]
- Baudouin, C. Ocular surface and external filtration surgery: Mutual relationships. Dev. Ophthalmol. 2012, 50, 64–78. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Agnifili, L.; Mastropasqua, R.; Fasanella, V. Conjunctival modifications induced by medical and surgical therapies in patients with glaucoma. Curr. Opin. Pharmacol. 2013, 13, 56–64. [Google Scholar] [CrossRef]
- Agnifili, L.; Fasanella, V.; Mastropasqua, R.; Frezzotti, P.; Curcio, C.; Brescia, L.; Marchini, G. In vivo goblet cell density as a potential indicator of glaucoma filtration surgery outcome. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2928–2935. [Google Scholar] [CrossRef] [Green Version]
- Mastropasqua, R.; Fasanella, V.; Brescia, L.; Oddone, F.; Mariotti, C.; Di Staso, S.; Agnifili, L. In vivo confocal imaging of the conjunctiva as a predictive tool for the glaucoma filtration surgery outcome. Investig. Ophthalmol. Vis. Sci. 2017, 58, BIO114–BIO120. [Google Scholar] [CrossRef]
- Kronfeld, P.C. The chemical demonstration of trans-conjunctival passage of aqueous after antiglaucomatous operations. Am. J. Ophthalmol. 1952, 35, 38–45. [Google Scholar] [CrossRef]
- Amar, N.; Labbè, A.; Hamard, P.; Dupas, B.; Baudouin, C. Filtering blebs and aqueous pathway: An immunocytological and in vivo confocal microscopy study. Ophthalmology 2008, 115, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Boimer, C.; Birt, C.M. Preservative exposure and surgical outcomes in glaucoma patients: The PESO study. J. Glaucoma 2013, 22, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Tailor, R.; Batra, R.; Mohamed, S. A National Survey of Glaucoma Specialists on the Preoperative (Trabeculectomy) Management of the Ocular Surface. Semin. Ophthalmol. 2016, 31, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Agnifili, L.; Sacchi, M.; Figus, M.; Posarelli, C.; Lizzio, R.A.U.; Nucci, P.; Mastropasqua, L. Preparing the ocular surface for glaucoma filtration surgery: An unmet clinical need. Acta Ophthalmol. 2022, 15098. [Google Scholar] [CrossRef]
- Breusegem, C.; Spielberg, L.; Van Ginderdeuren, R.; Vandewalle, E.; Renier, C.; Van de Veire, S.; Fieuws, S.; Zeyen, T.; Stalmans, I. Preoperative nonsteroidal anti-inflammatory drug or steroid and outcomes after trabeculectomy: A randomized controlled trial. Ophthalmology 2010, 117, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, K.; Wasielica-Poslednik, J.; Bell, K.; Renieri, G.; Keicher, A.; Ruckes, C.; Pfeiffer, N.; Thieme, H. Efficacy and safety of preoperative IOP reduction using a preservative-free fixed combination of dorzolamide/timolol eye drops versus oral acetazolamide and dexamethasone eye drops and assessment of the clinical outcome of trabeculectomy in glaucoma. PLoS ONE 2017, 12, e0171636. [Google Scholar] [CrossRef]
- Law, S.K.; Shih, K.; Tran, D.H.; Coleman, A.L.; Caprioli, J. Long-term outcomes of repeat vs initial trabeculectomy in open-angle glaucoma. Am. J. Ophthalmol. 2009, 148, 685–695.e1. [Google Scholar] [CrossRef]
- Hoffmann, E.M.; Herzog, D.; Wasielica-Poslednik, J.; Butsch, C.; Schuster, A.K. Bleb grading by photographs versus bleb grading by slit-lamp examination. Acta Ophthalmol. 2019, 98, e607–e610. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, B.K.; Giannouladis, K.; Leighton, P.; King, A.J. Seeking a practical definition of stable glaucoma: A Delphi consensus survey of UK glaucoma consultants. Eye 2020, 34, 335–343. [Google Scholar] [CrossRef]
- Mastropasqua, R.; Agnifili, L.; Fasanella, V.; Lappa, A.; Brescia, L.; Lanzini, M.; Oddone, F.; Perri, P.; Mastropasqua, L. In vivo distribution of corneal epithelial dendritic cells in patients with glaucoma. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5996–6002. [Google Scholar] [CrossRef]
- Dale, S.B.; Saban, D.R. Linking immune responses with fibrosis in allergic eye disease. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efron, N.; Al-Dossari, M.; Pritchard, N. In vivo confocal microscopy of the bulbar conjunctiva. Clin. Exp. Ophthalmol. 2009, 37, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M.; Zapp, D.M.; Mackert, M.J.; Thiel, M.; Kampik, A. In vivo confocal microscopy of filtering blebs after trabeculectomy. Arch. Ophthalmol. 2006, 124, 1095–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messmer, E.M.; Mackert, M.J.; Zapp, D.M.; Kampik, A. In vivo confocal microscopy of normal conjunctiva and conjunctivitis. Cornea 2006, 25, 781–788. [Google Scholar] [CrossRef]
- Seo, J.H.; Kim, Y.A.; Park, K.H.; Lee, Y. Evaluation of Functional Filtering Bleb Using Optical Coherence Tomography Angiography. Transl. Vis. Sci. Technol. 2019, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Baudouin, C. Ocular Surface and External Filtration Surgery: Mutual Relationships. Dev. Ophthalmol. 2017, 59, 67–79. [Google Scholar] [CrossRef]
- Baudouin, C.; Nordmann, J.P.; Denis, P.; Creuzot-Garcher, C.; Allaire, C.; Trinquand, C. Efficacy of indomethacin 0.1% and fluorometholone 0.1% on conjunctival inflammation following chronic application of antiglaucomatous drugs. Graefes Arch. Clin. Exp. Ophthalmol. 2002, 240, 929–935. [Google Scholar] [CrossRef]
- Nguyen, K.D.; Lee, D.A. Effect of steroids and nonsteroidal antiinflammatory agents on human ocular fibroblast. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2693–2701. [Google Scholar]
- Broadway, D.C.; Grierson, I.; Sturmer, J.; Hitchings, R.A. Reversal of topical antiglaucoma medication effects on the conjunctiva. Arch. Ophthalmol. 1966, 114, 262–267. [Google Scholar] [CrossRef]
- Agnifili, L.; Brescia, L.; Oddone, F.; Sacchi, M.; D’Ugo, E.; Di Marzio, G.; Perna, F.; Costagliola, C.; Mastropasqua, R. The ocular surface after successful glaucoma filtration surgery: A clinical, in vivo confocal microscopy, and immune-cytology study. Sci. Rep. 2019, 9, 11299. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Gender (M/F) | Age (Years ± SD) | Time on Therapy (Months ± SD) | Baseline IOP (mmHg ± SD) | Pre-OP IOP (mmHg ± SD) | 12 Months IOP (mmHg ± SD) | Post-OP Procedures (n ± SD) | Post-OP IOP Lowering Medications (n ± SD) | |
|---|---|---|---|---|---|---|---|---|
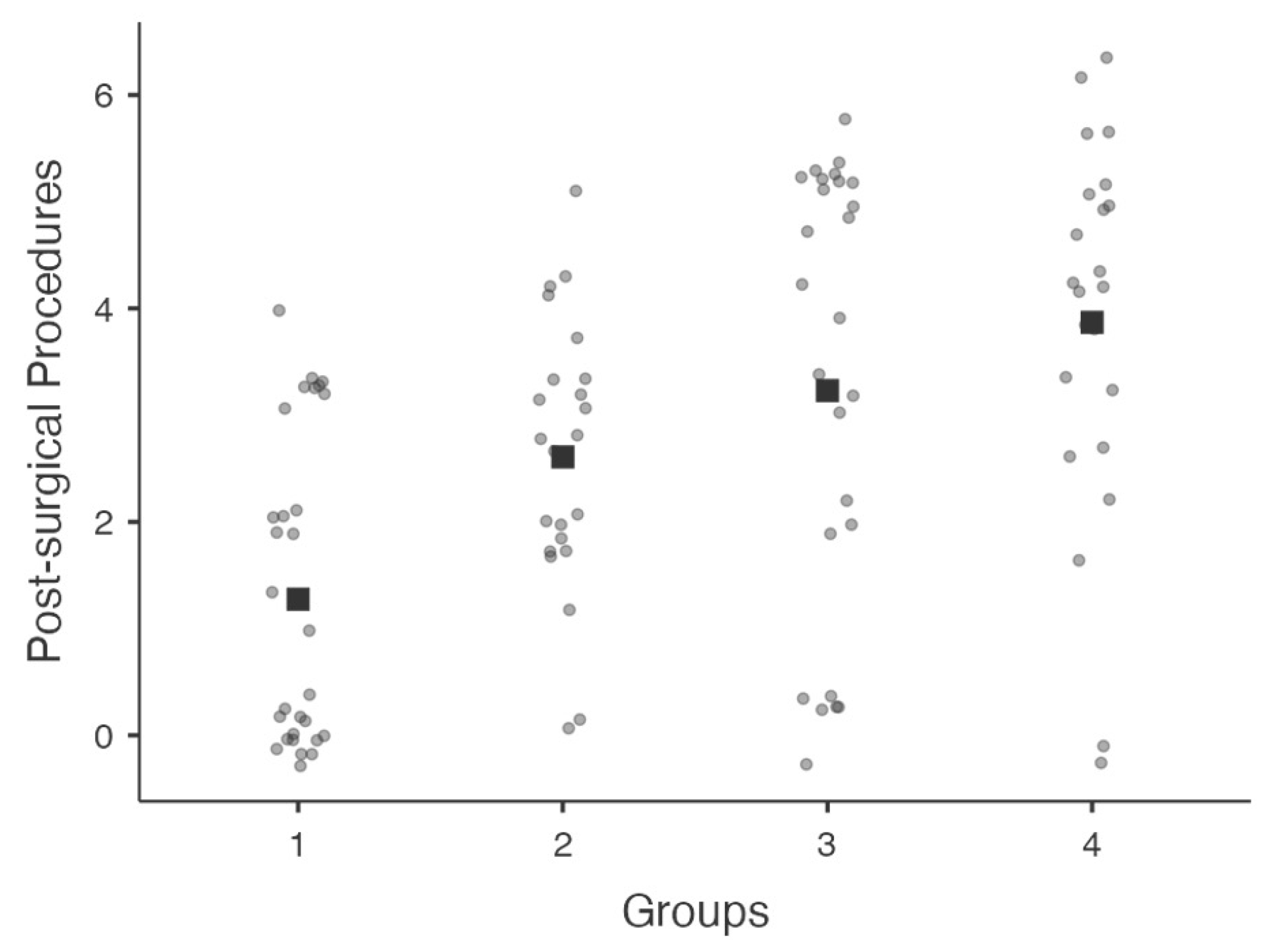
| Group 1 | 13/16 | 68.34 ± 7.97 | 72.5 ± 3.2 | 29.55 ± 5.32 | 28.24 ± 4.57 | 15.51 ± 2.28 †‡ | 1.28 ± 1.01 *# | 0.93 ± 0.88 * |
| Group 2 | 10/13 | 72.65 ± 7.23 | 75.2 ± 4.1 | 31.55 ± 7.62 | 30.22 ± 5.69 | 26.11 ± 1.76 | 2.61 ± 1.23 | 1.36 ± 1.01 § |
| Group 3 | 15/11 | 65.54 ± 6.24 | 68.7 ± 3.1 | 28.93 ± 5.07 | 27.08 ± 4.51 | 14.10 ± 2.49 †‡ | 3.23 ± 2.10 | 1.92 ± 0.81 |
| Group 4 | 12/14 | 74.76 ± 8.47 | 70.7 ± 2.9 | 30.22 ± 6.48 | 28.89 ± 5.11 | 25.67 ± 3.16 | 3.87 ± 1.71 | 2.15 ± 1.15 |
| Baseline DCD | Baseline GCD | Baseline SMR | Baseline VT | Pre-OP IOP | Pre-OP DCD | Pre-OP GCD | Pre-OP SMR | Pre-OP VT | |
|---|---|---|---|---|---|---|---|---|---|
| Group 1 | 57.57 ± 8.69 | 28.09 ± 2.82 | 104.68 ± 8.28 | 1.72 ± 0.92 | 28.24 ± 4.57 | 35.04 ± 7.40 * | 30.63 ± 2.78 | 94.99 ± 11.85 # | 1.38 ± 0.82 # |
| Group 2 | 59.26 ± 5.04 | 29.36 ± 4.22 | 100.68 ± 8.70 | 1.55 ± 0.73 | 30.22 ± 5.69 | 41.98 ± 4.42 ^ | 28.61 ± 4.07 | 104.29 ± 9.68 ¥ | 1.33 ± 1.12 |
| Group 3 | 59.35 ± 9.44 | 29.52 ± 4.12 | 103.21 ± 10.65 | 1.54 ± 0.93 | 27.08 ± 4.51 | 55.78 ± 10.65 § | 29.15 ± 4.41 | 96.59 ± 10.57 # | 1.15 ± 0.88 # |
| Group 4 | 58.27 ± 4.78 | 28.39 ± 4.79 | 100.72 ± 9.31 | 1.55 ± 0.88 | 28.89 ± 5.11 | 66.67 ± 4.48 § | 24.93 ± 4.43 ° | 109.11 ± 5.18 ¥ | 1.67 ± 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastropasqua, L.; Brescia, L.; D’Arcangelo, F.; Nubile, M.; D’Onofrio, G.; Totta, M.; Perna, F.; Aloia, R.; Agnifili, L. Topical Steroids and Glaucoma Filtration Surgery Outcomes: An In Vivo Confocal Study of the Conjunctiva. J. Clin. Med. 2022, 11, 3959. https://doi.org/10.3390/jcm11143959
Mastropasqua L, Brescia L, D’Arcangelo F, Nubile M, D’Onofrio G, Totta M, Perna F, Aloia R, Agnifili L. Topical Steroids and Glaucoma Filtration Surgery Outcomes: An In Vivo Confocal Study of the Conjunctiva. Journal of Clinical Medicine. 2022; 11(14):3959. https://doi.org/10.3390/jcm11143959
Chicago/Turabian StyleMastropasqua, Leonardo, Lorenza Brescia, Francesca D’Arcangelo, Mario Nubile, Giada D’Onofrio, Michele Totta, Fabiana Perna, Raffaella Aloia, and Luca Agnifili. 2022. "Topical Steroids and Glaucoma Filtration Surgery Outcomes: An In Vivo Confocal Study of the Conjunctiva" Journal of Clinical Medicine 11, no. 14: 3959. https://doi.org/10.3390/jcm11143959
APA StyleMastropasqua, L., Brescia, L., D’Arcangelo, F., Nubile, M., D’Onofrio, G., Totta, M., Perna, F., Aloia, R., & Agnifili, L. (2022). Topical Steroids and Glaucoma Filtration Surgery Outcomes: An In Vivo Confocal Study of the Conjunctiva. Journal of Clinical Medicine, 11(14), 3959. https://doi.org/10.3390/jcm11143959