
Advanced Glycation End Product (AGE) and Soluble Receptor of AGE (sRAGE) Levels in Relation to Periodontitis Severity and as Putative 3-Year Outcome Predictors in Patients Undergoing Coronary Artery Bypass Grafting (CABG)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
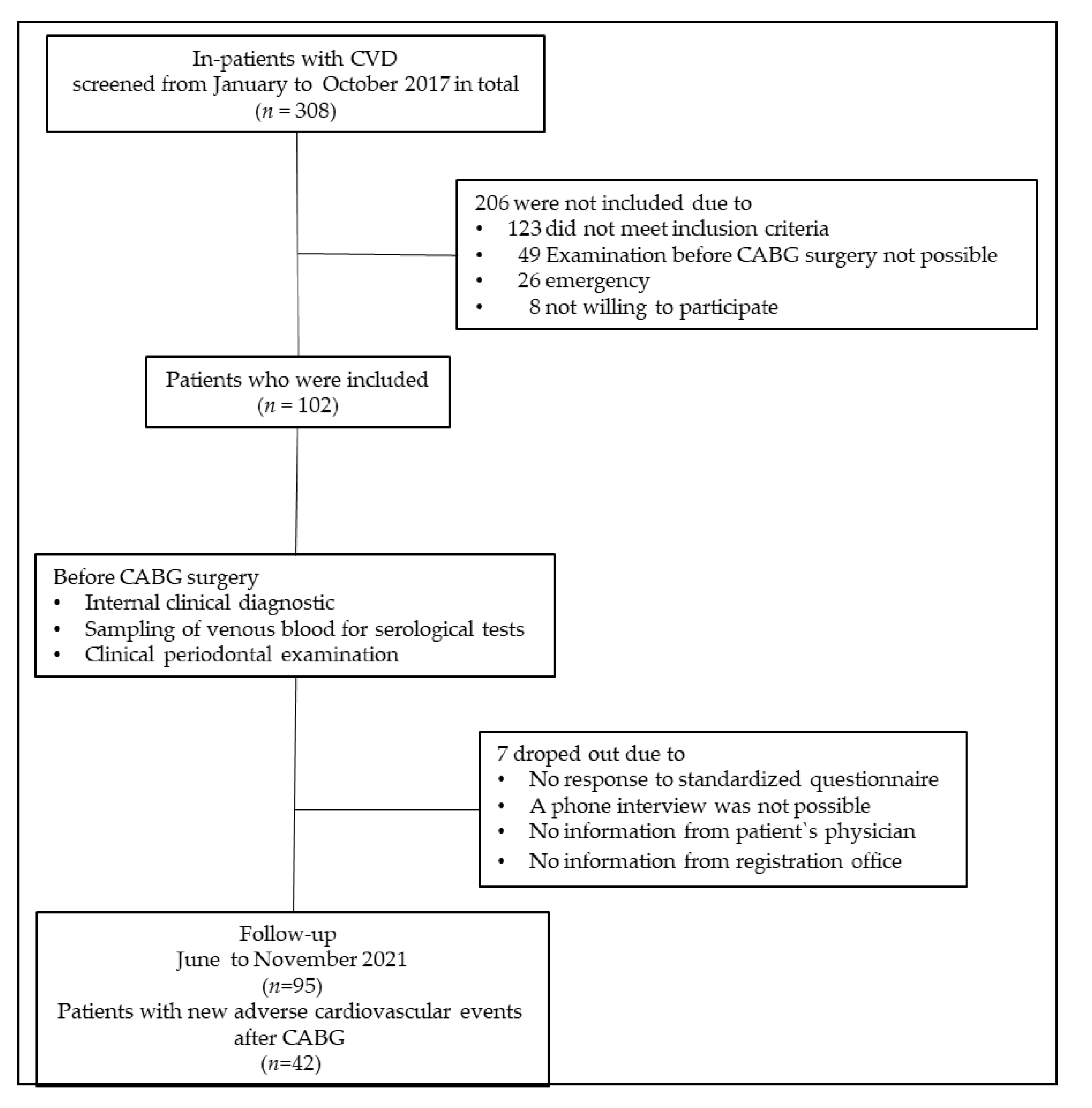
2.1. Patient Enrollment
2.2. Demographic Parameters and Clinical and Cardiological Diagnostics
2.3. Dental Anamnesis and Examinations
2.4. Skin Autofluorescence (sAF)
2.5. Determination of Peripheral Soluble Receptor of AGE (sRAGE) Concentration
2.6. Follow-Up
2.7. Statistics
2.7.1. Power Analysis
2.7.2. Statistical Procedures
3. Results
3.1. Baseline Characteristics of Study Participants
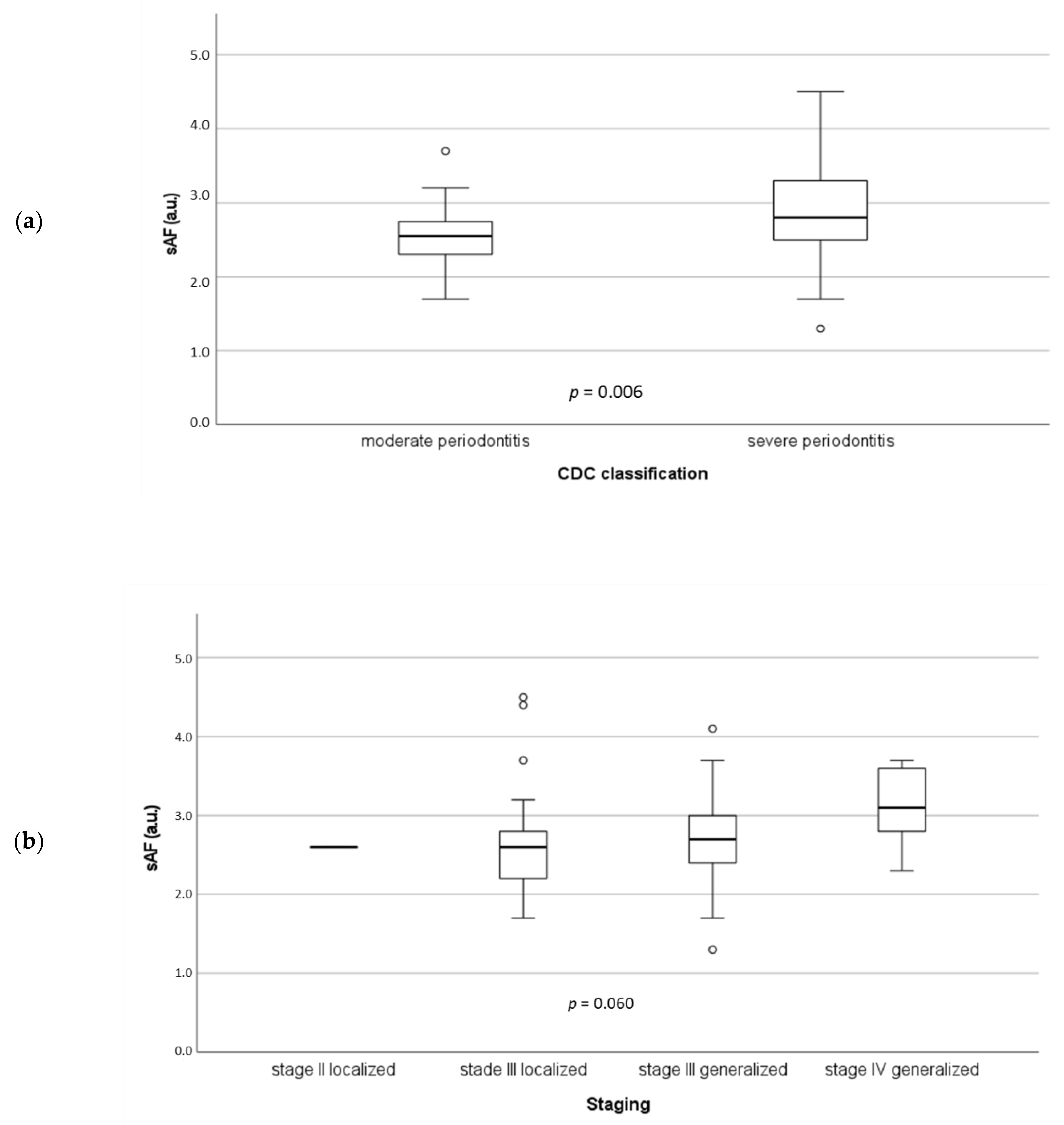
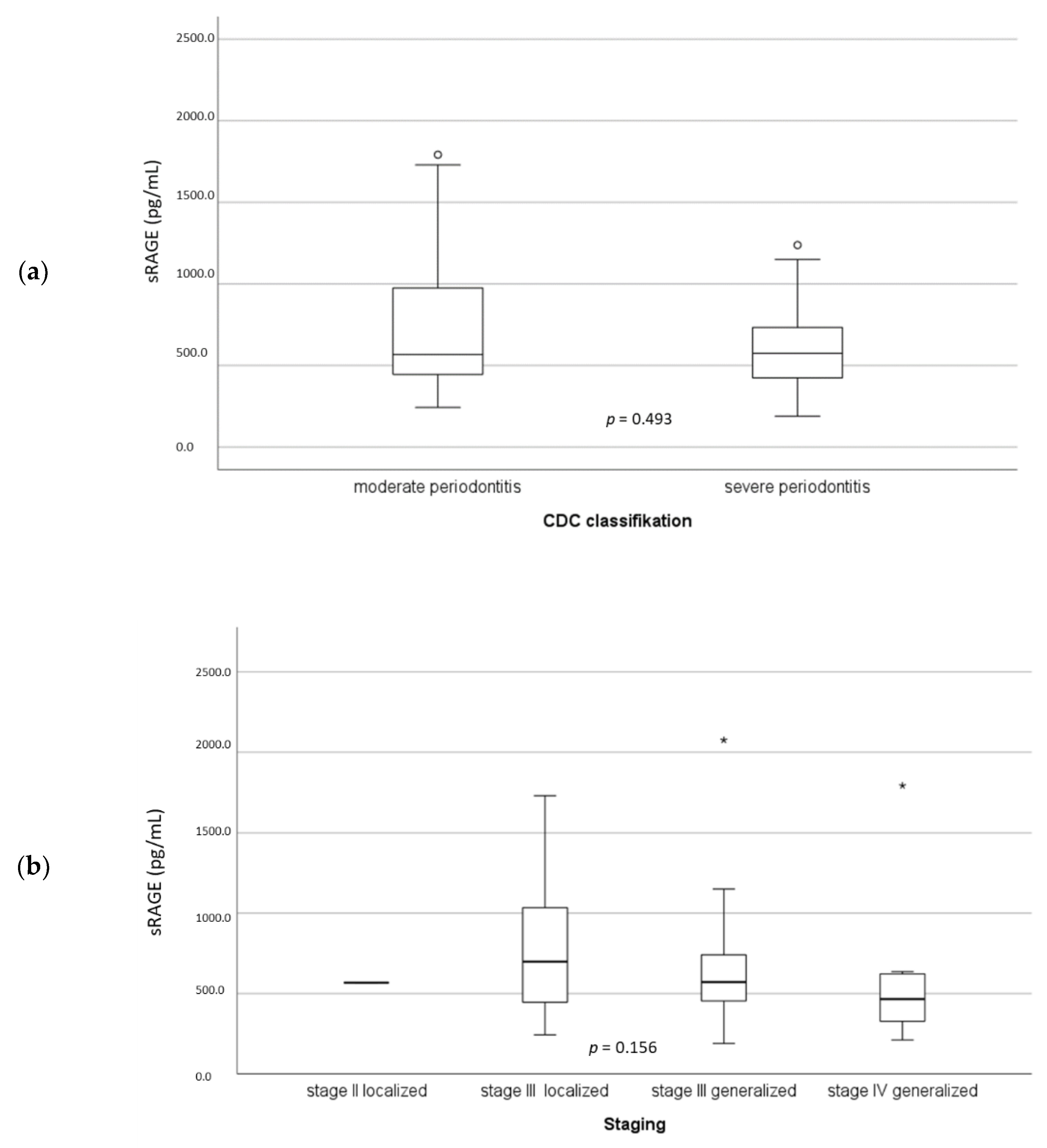
3.2. RAGE and sRAGE in Association to Severity of Periodontitis
3.3. RAGE and sRAGE Associated with BOP
3.4. Multivariate Analysis
3.5. RAGE, sRAGE, and Severe Periodontitis Associated with New Adverse Cardiovascular Events after CAGB
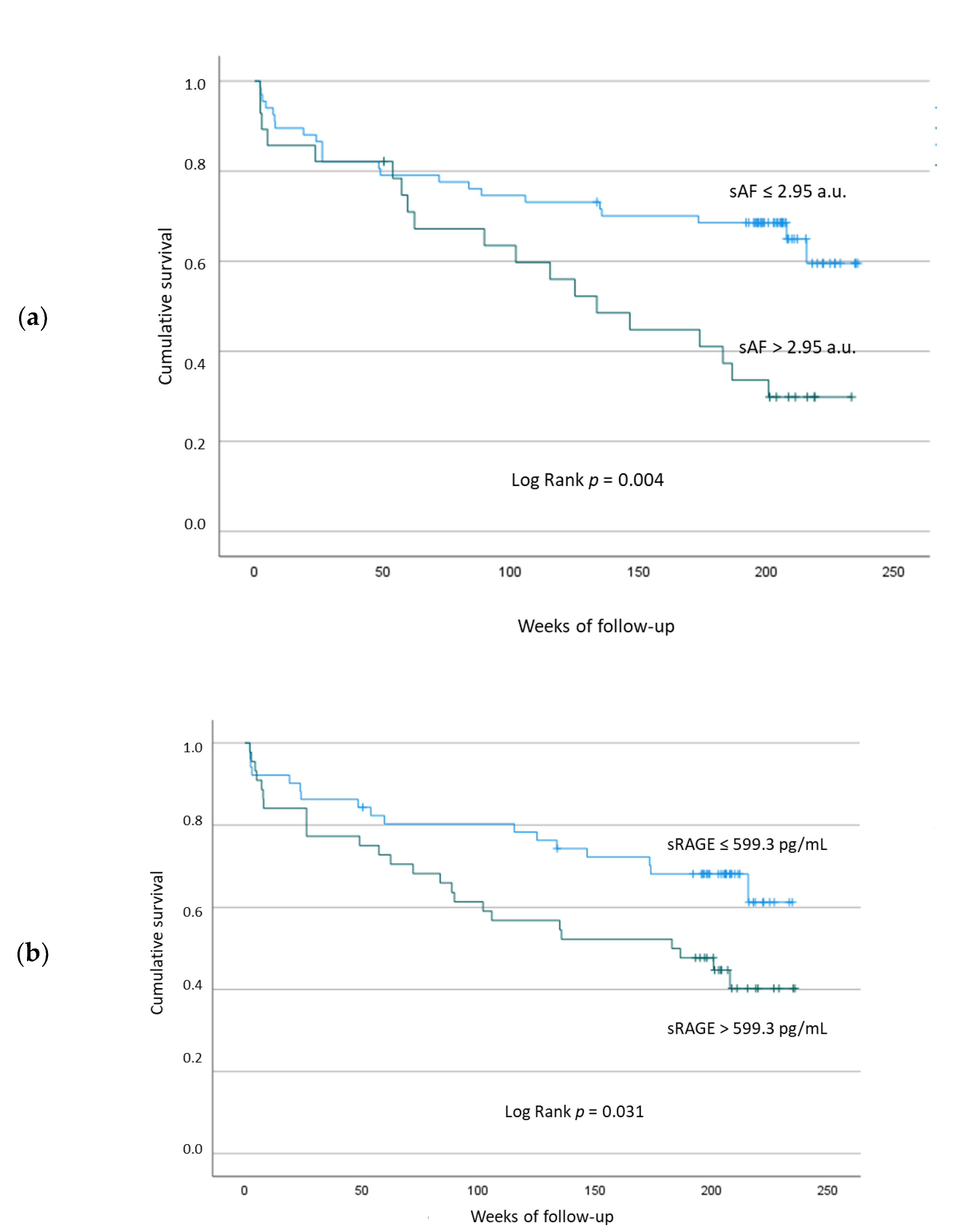
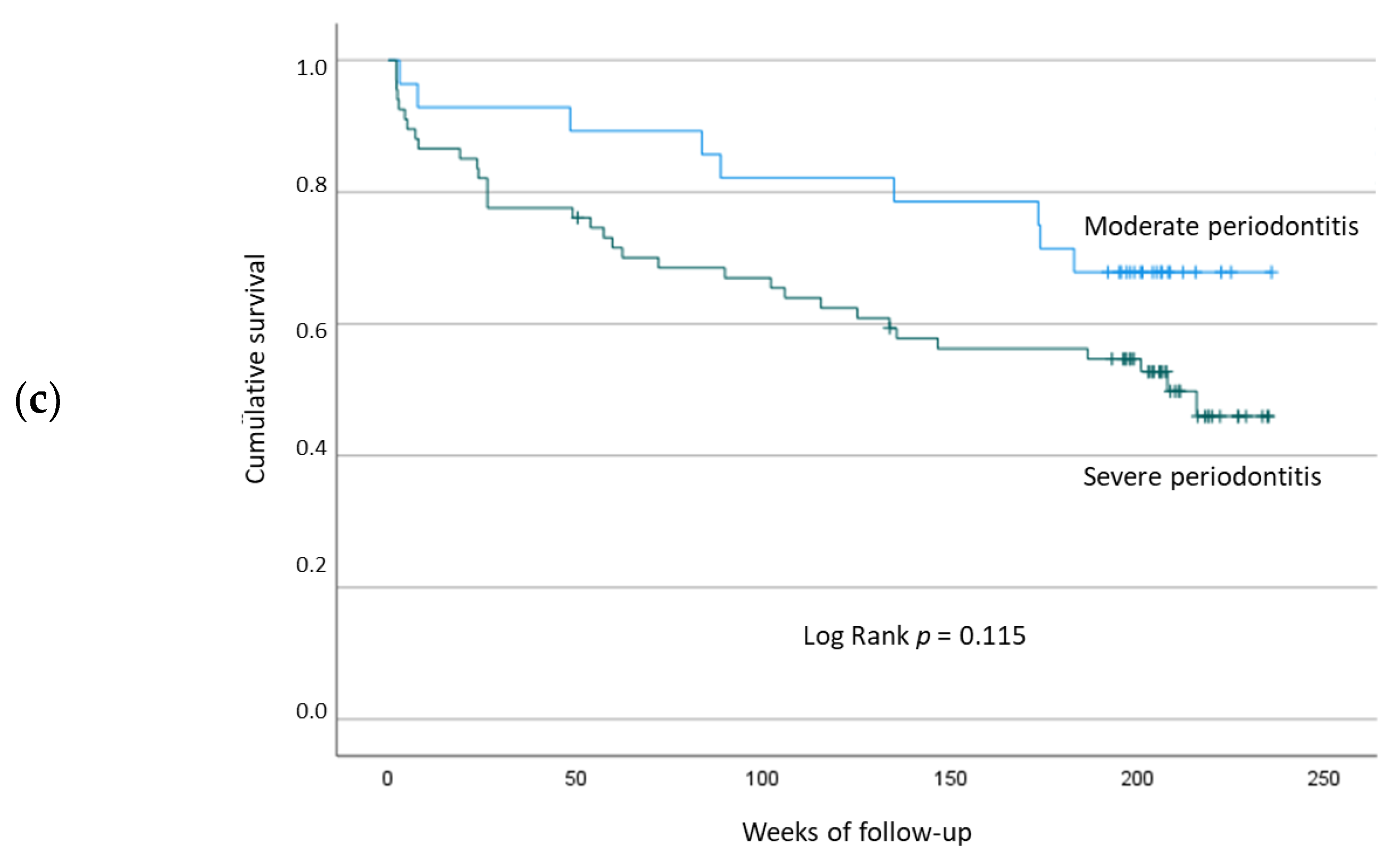
3.5.1. Univariate Kaplan–Meier Analyses
3.5.2. Multivariate Analysis with Cox Regression
4. Discussion
4.1. Limitations of the Study
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Graham, M.M.; Ghali, W.A.; Faris, P.D.; Galbraith, P.D.; Norris, C.M.; Knudtson, M.L. Survival after coronary revascularization in the elderly. Circulation 2002, 105, 2378–2384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toumpoulis, I.K.; Anagnostopoulos, C.E.; Balaram, S.K.; Rokkas, C.K.; Swistel, D.G.; Ashton, R.C.; DeRose, J.J. Assessment of independent predictors for long-term mortality between women and men after coronary artery bypass grafting: Are women different from men? J. Thorac. Cardiovasc. Surg. 2006, 131, 343–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axelsson, T.A.; Adalsteinsson, J.A.; Arnadottir, L.O.; Helgason, D.; Johannesdottir, H.; Helgadottir, S.; Orrason, A.W.; Andersen, K.; Gudbjartsson, T. Long-term outcomes after coronary artery bypass surgery in patients with diabetes. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 685–690. [Google Scholar] [CrossRef] [Green Version]
- Bonacchi, M.; Parise, O.; Matteucci, F.; Tetta, C.; Moula, A.I.; Micali, L.R.; Dokollari, A.; de Martino, M.; Sani, G.; Grasso, A.; et al. Is Peripheral Artery Disease an Independent Predictor of Isolated Coronary Artery Bypass Outcome? Heart Lung Circ. 2020, 29, 1502–1510. [Google Scholar] [CrossRef]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Suzuki, H.; Matsuo, K.; Okamoto, M.; Nakata, H.; Sakamoto, H.; Fujita, M. Preoperative periodontal treatment and its effects on postoperative infection in cardiac valve surgery. Clin. Exp. Dent. Res. 2019, 5, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Reichert, S.; Schulz, S.; Friebe, L.; Kohnert, M.; Grollmitz, J.; Schaller, H.-G.; Hofmann, B. Is Periodontitis a Predictor for an Adverse Outcome in Patients Undergoing Coronary Artery Bypass Grafting? A Pilot Study. J. Clin. Med. 2021, 10, 818. [Google Scholar] [CrossRef]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced glycation end products: Sparking the development of diabetic vascular injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Gill, V.; Kumar, V.; Singh, K.; Kumar, A.; Kim, J.-J. Advanced Glycation End Products (AGEs) May Be a Striking Link Between Modern Diet and Health. Biomolecules 2019, 9, 888. [Google Scholar] [CrossRef] [Green Version]
- Nicholl, I.D.; Bucala, R. Advanced glycation endproducts and cigarette smoking. Cell. Mol. Biol. 1998, 44, 1025–1033. [Google Scholar]
- Del Turco, S.; Basta, G. An update on advanced glycation endproducts and atherosclerosis. Biofactors 2012, 38, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Alqahtani, F.; Alqahtani, M.; Al-Kheraif, A.A.; Javed, F. Levels of advanced glycation end products in gingival crevicular fluid of chronic periodontitis patients with and without type-2 diabetes mellitus. J. Periodontol. 2020, 91, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Ding, Z.; Yang, Y. The impact of diabetes on periodontal diseases. Periodontol. 2000 2020, 82, 214–224. [Google Scholar] [CrossRef]
- Hofmann, B.; Gerull, K.A.; Bloch, K.; Riemer, M.; Erbs, C.; Fröhlich, A.; Richter, S.; Ehrhardt, M.; Zitterbart, C.; Bartel, F.F.; et al. It’s all in our skin—Skin autofluorescence—A promising outcome predictor in cardiac surgery: A single centre cohort study. PLoS ONE 2020, 15, e0234847. [Google Scholar] [CrossRef]
- Park, L.; Raman, K.G.; Lee, K.J.; Lu, Y.; Ferran, L.J.; Chow, W.S.; Stern, D.; Schmidt, A.M. Suppression of accelerated diabetic atherosclerosis by the soluble receptor for advanced glycation endproducts. Nat. Med. 1998, 4, 1025–1031. [Google Scholar] [CrossRef]
- Reichert, S.; Triebert, U.; Santos, A.N.; Hofmann, B.; Schaller, H.-G.; Schlitt, A.; Schulz, S. Soluble form of receptor for advanced glycation end products and incidence of new cardiovascular events among patients with cardiovascular disease. Atherosclerosis 2017, 266, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Simm, A.; Philipp, C.; Friedrich, I.; Scheubel, R.J.; Hofmann, H.-S.; Meibodi, K.H.; Sablotzki, A.; Silber, R.-E.; Börgermann, J. Intraoperative sRAGE kinetics. A new age-related outcome predictor of cardiac surgery. Z. Gerontol. Geriatr. 2014, 47, 666–672. [Google Scholar] [CrossRef]
- Scheiber-Camoretti, R.; Mehrotra, A.; Yan, L.; Raman, J.; Beshai, J.F.; Hofmann Bowman, M.A. Elevated S100A12 and sRAGE are associated with increased length of hospitalization after non-urgent coronary artery bypass grafting surgery. Am. J. Cardiovasc. Dis. 2013, 3, 85–90. [Google Scholar]
- Detzen, L.; Cheng, B.; Chen, C.-Y.; Papapanou, P.N.; Lalla, E. Soluble Forms of the Receptor for Advanced Glycation Endproducts (RAGE) in Periodontitis. Sci. Rep. 2019, 9, 8170. [Google Scholar] [CrossRef]
- Singhal, S.; Pradeep, A.R.; Kanoriya, D.; Garg, V. Human soluble receptor for advanced glycation end products and tumor necrosis factor-α as gingival crevicular fluid and serum markers of inflammation in chronic periodontitis and type 2 diabetes. J. Oral Sci. 2016, 58, 547–553. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-S.; Lee, Y.J.; Ahn, S.; Chang, Y.-S.; Choi, Y.; Lee, H.-J. Association between soluble forms of the receptor for advanced glycation end products and periodontal disease: A retrospective study. J. Korean Assoc. Oral Maxillofac. Surg. 2021, 47, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef] [PubMed]
- Loe, H.; Silness, J. Periodontal disease in pregnancy. i. prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Grouven, U.; Bender, R.; Ziegler, A.; Lange, S. Vergleich von Messmethoden. Dtsch. Med. Wochenschr. 2007, 132 (Suppl. 1), e69–e73. [Google Scholar] [CrossRef] [Green Version]
- Page, R.C.; Eke, P.I. Case definitions for use in population-based surveillance of periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef] [Green Version]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Meerwaldt, R.; Links, T.; Graaff, R.; Thorpe, S.R.; Baynes, J.W.; Hartog, J.; Gans, R.; Smit, A. Simple noninvasive measurement of skin autofluorescence. Ann. N. Y. Acad. Sci. 2005, 1043, 290–298. [Google Scholar] [CrossRef]
- Møller, C.H.; Perko, M.J.; Lund, J.T.; Andersen, L.W.; Kelbæk, H.; Madsen, J.K.; Winkel, P.; Gluud, C.; Steinbrüchel, D.A. Three-year follow-up in a subset of high-risk patients randomly assigned to off-pump versus on-pump coronary artery bypass surgery: The Best Bypass Surgery trial. Heart 2011, 97, 907–913. [Google Scholar] [CrossRef]
- Janket, S.-J.; Baird, A.E.; Chuang, S.-K.; Jones, J.A. Meta-analysis of periodontal disease and risk of coronary heart disease and stroke. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 559–569. [Google Scholar] [CrossRef]
- Bahekar, A.A.; Singh, S.; Saha, S.; Molnar, J.; Arora, R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: A meta-analysis. Am. Heart J. 2007, 154, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal disease and coronary heart disease incidence: A systematic review and meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, T.; Sharma, P.; Walter, C.; Weston, P.; Beck, J. The epidemiological evidence behind the association between periodontitis and incident atherosclerotic cardiovascular disease. J. Clin. Periodontol. 2013, 40 (Suppl. 14), S70–S84. [Google Scholar] [CrossRef]
- Rydén, L.; Buhlin, K.; Ekstrand, E.; de Faire, U.; Gustafsson, A.; Holmer, J.; Kjellström, B.; Lindahl, B.; Norhammar, A.; Nygren, Å.; et al. Periodontitis Increases the Risk of a First Myocardial Infarction: A Report From the PAROKRANK Study. Circulation 2016, 133, 576–583. [Google Scholar] [CrossRef]
- Valiyaveetil Karattil, L.; Joseph, R.S.; Ambooken, M.; Mathew, J.J. Evaluation of serum concentrations of hs-CRP and Hb in varying severities of chronic periodontitis. Biomarkers 2022, 27, 258–263. [Google Scholar] [CrossRef]
- Machado, V.; Botelho, J.; Lopes, J.; Patrão, M.; Alves, R.; Chambrone, L.; Alcoforado, G.; Mendes, J.J. Periodontitis Impact in Interleukin-6 Serum Levels in Solid Organ Transplanted Patients: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 184. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.; Lüdike, H.; Lierath, M.; Schlitt, A.; Werdan, K.; Hofmann, B.; Gläser, C.; Schaller, H.-G.; Reichert, S. C-reactive protein levels and genetic variants of CRP as prognostic markers for combined cardiovascular endpoint (cardiovascular death, death from stroke, myocardial infarction, and stroke/TIA). Cytokine 2016, 88, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Li, X.-L.; Zhao, C.-R.; Pan, C.-L.; Zhang, Z. Interleukin-6 as a Predictor of the Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Epidemiological Studies. Immunol. Investig. 2018, 47, 689–699. [Google Scholar] [CrossRef]
- Duda-Sobczak, A.; Lipski, J.; Tarnowski, M.; Surdacka, A.; Zozulińska-Ziółkiewicz, D.; Wyganowska-Świątkowska, M. Association of skin autofluorescence with periodontal inflammation in adults with type 1 diabetes. Pol. Arch. Intern. Med. 2017, 127, 708–711. [Google Scholar] [CrossRef]
- Kunimoto, M.; Shimada, K.; Yokoyama, M.; Matsubara, T.; Aikawa, T.; Ouchi, S.; Shimizu, M.; Fukao, K.; Miyazaki, T.; Kadoguchi, T.; et al. Association between the tissue accumulation of advanced glycation end products and exercise capacity in cardiac rehabilitation patients. BMC Cardiovasc. Disord. 2020, 20, 195. [Google Scholar] [CrossRef] [Green Version]
- Kunimoto, M.; Yokoyama, M.; Shimada, K.; Matsubara, T.; Aikawa, T.; Ouchi, S.; Fukao, K.; Miyazaki, T.; Fujiwara, K.; Abulimiti, A.; et al. Relationship between skin autofluorescence levels and clinical events in patients with heart failure undergoing cardiac rehabilitation. Cardiovasc. Diabetol. 2021, 20, 208. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Yamagishi, S.-i.; Adachi, H.; Matsui, T.; Kurita-Nakamura, Y.; Takeuchi, M.; Inoue, H.; Imaizumi, T. Serum levels of soluble form of receptor for advanced glycation end products (sRAGE) are positively associated with circulating AGEs and soluble form of VCAM-1 in patients with type 2 diabetes. Microvasc. Res. 2008, 76, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, S.-I.; Adachi, H.; Nakamura, K.; Matsui, T.; Jinnouchi, Y.; Takenaka, K.; Takeuchi, M.; Enomoto, M.; Furuki, K.; Hino, A.; et al. Positive association between serum levels of advanced glycation end products and the soluble form of receptor for advanced glycation end products in nondiabetic subjects. Metabolism 2006, 55, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, K.; Katakami, N.; Kaneto, H.; Naka, T.; Takahara, M.; Sakamoto, F.; Irie, Y.; Miyashita, K.; Kubo, F.; Yasuda, T.; et al. Circulating soluble RAGE as a predictive biomarker of cardiovascular event risk in patients with type 2 diabetes. Atherosclerosis 2013, 227, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Sumner, R.; Hardin, J.; Barros, S.; Moss, K.; Beck, J.; Offenbacher, S. Periodontal Disease and Recurrent Vascular Events in Stroke/Transient Ischemic Attack Patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 1420–1427. [Google Scholar] [CrossRef] [Green Version]
- Dorn, J.M.; Genco, R.J.; Grossi, S.G.; Falkner, K.L.; Hovey, K.M.; Iacoviello, L.; Trevisan, M. Periodontal disease and recurrent cardiovascular events in survivors of myocardial infarction (MI): The Western New York Acute MI Study. J. Periodontol. 2010, 81, 502–511. [Google Scholar] [CrossRef]
- Renvert, S.; Ohlsson, O.; Pettersson, T.; Persson, G.R. Periodontitis: A future risk of acute coronary syndrome? A follow-up study over 3 years. J. Periodontol. 2010, 81, 992–1000. [Google Scholar] [CrossRef]
- Reichert, S.; Schulz, S.; Benten, A.-C.; Lutze, A.; Seifert, T.; Schlitt, M.; Werdan, K.; Hofmann, B.; Wienke, A.; Schaller, H.-G.; et al. Periodontal conditions and incidence of new cardiovascular events among patients with coronary vascular disease. J. Clin. Periodontol. 2016, 43, 918–925. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Entire Study Cohort, n = 95 Median (25th/75th Percentile) or n (%) |
|---|---|
| Age (years) | 69.0 (60.8/75.0) |
| Males | 83 (88.3) |
| BMI (kg/m2) | 28.7 (25.6/31.0) |
| Smoking | |
| Current | 19 (20.2) |
| Past | 40 (42.6) |
| Never | 35 (37.2) |
| Affected coronaries | |
| One-vessel disease | 5 (5.3) |
| Two-vessel disease | 20 (21.3) |
| Three-vessel disease | 68 (72.3) |
| More than three vessels affected | 1 (1.1) |
| LVEF (%) | 60 (45/60) |
| History of | |
| Diabetes mellitus | 38 (40.4) |
| Hypertension | 83 (88.3) |
| Dyslipoproteinemia | 77 (81.9) |
| Peripheral arterial dis. | 15 (16.0) |
| CVD | 34 (36.2) |
| Myocardial infarction | 26 (27.7) |
| Stroke/TIA | 8 (8.5) |
| Angina pectoris | 70 (74.5) |
| PTCA/stent | 11 (11.7) |
| Atrial fibrillation | 14 (14.9) |
| Periodontal conditions | |
| Plaque index (%) | 1.3 (0.9/1.7) |
| Bleeding index (%) | 18.2 (9.9/33.3) |
| Pocket depth (mm) | 3.0 (2.6/3.5) |
| Attachment loss (mm) | 3.9 (3.2/4.9) |
| Missing teeth | 6 (3/13.5) |
| CDC classification (2007) | |
| No or mild | 0 (0.0) |
| Moderate | 29 (28.7) |
| Severe | 72 (71.3) |
| New classification (2017) | |
| Staging | |
| I | 0 |
| II (localized) | 1 (1.1) |
| III (localized) | 24 (25.5) |
| III (generalized) | 56 (59.6) |
| IV (generalized) | 13 (13.8) |
| Blood values | |
| Creatinine (µmol/L) | 85 (74.8/100) |
| Urea (mmol/L) | 5.7 (4.5/7.1) |
| HbA1C (mmol/mol) | 37.6 (31.2/44.4) |
| CRP (mg/L) | 2.7 (1.2/6.8) |
| Leukocytes (Gpt/L) | 7.5 (6.5/9.0) |
| Platelet (Gpt/L) | 238.5 (192.5/268.8) |
| Triglycerides (mmol/L) | 1.1 (0/1.55) |
| Glucose (mmol/L) | 6.5 (5.3/9.19) |
| sRAGE (pg/mL) | 567.9 (436/770) |
| AGE tissue concentration (sAF) (a.u.) | 2.7 (2.4/3.1) |
| Drugs | |
| Lipid lowering drugs | 83 (88.3) |
| Oral anticoagulants | 11 (11.7) |
| Antiarrhythmics | 2 (2.1) |
| Variables | BOP | sAF | sRAGE | |
|---|---|---|---|---|
| BOP | r | 1.000 | 0.106 | −0.189 |
| p | 0.154 | 0.034 | ||
| n | 95 | 95 | 94 | |
| sAF | r | 0.106 | 1.000 | 0.086 |
| p | 0.154 | 0.205 | ||
| n | 95 | 95 | 94 | |
| sRAGE | r | −0.189 | 0.086 | 1.000 |
| p | 0.034 | 0.205 | ||
| n | 94 | 94 | 95 |
| Confounding Variables | Odds Ratio | 95% Lower | CI Upper | p-Values |
|---|---|---|---|---|
| Age | 1.034 | 0.974 | 1.097 | 0.278 |
| Gender (male) | 1.467 | 0.328 | 6.558 | 0.616 |
| Current smoking | 1.483 | 0.492 | 4.776 | 0.484 |
| Plaque index | 1.566 | 0.664 | 3.696 | 0.306 |
| Diabetes mellitus | 1.119 | 0.398 | 3.146 | 0.831 |
| sRAGE | 0.999 | 0.997 | 1.000 | 0.049 |
| sAF | 2.891 | 1.119 | 7.466 | 0.028 |
| Confounding Variables | Hazard Ratio | 95% Lower | CI Upper | p-Values |
|---|---|---|---|---|
| Age | 1.016 | 0.974 | 1.060 | 0.454 |
| Gender (male) | 0.678 | 0.224 | 2.051 | 0.492 |
| Current smoking | 0.899 | 0.391 | 2.065 | 0.801 |
| Severe periodontitis (CDC) | 1.701 | 0.737 | 3.930 | 0.214 |
| Bleeding on probing (BOP) | 0.993 | 0.978 | 1.008 | 0.345 |
| Atrial fibrillation | 2.411 | 0.931 | 6.245 | 0.075 |
| PAD | 2.724 | 1.330 | 5.578 | 0.006 |
| Previous MI | 2.797 | 1.281 | 6.107 | 0.010 |
| Urea | 1.084 | 0.918 | 1.280 | 0.342 |
| Creatinine | 1.005 | 0.987 | 1.023 | 0.593 |
| sRAGE | 1.000 | 0.999 | 1.001 | 0.920 |
| AGE tissue concentration (sAF) | 1.401 | 0.782 | 2.513 | 0.257 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reichert, S.; Hofmann, B.; Kohnert, M.; Santos, A.N.; Friebe, L.; Grollmitz, J.; Schaller, H.-G.; Schulz, S. Advanced Glycation End Product (AGE) and Soluble Receptor of AGE (sRAGE) Levels in Relation to Periodontitis Severity and as Putative 3-Year Outcome Predictors in Patients Undergoing Coronary Artery Bypass Grafting (CABG). J. Clin. Med. 2022, 11, 4105. https://doi.org/10.3390/jcm11144105
Reichert S, Hofmann B, Kohnert M, Santos AN, Friebe L, Grollmitz J, Schaller H-G, Schulz S. Advanced Glycation End Product (AGE) and Soluble Receptor of AGE (sRAGE) Levels in Relation to Periodontitis Severity and as Putative 3-Year Outcome Predictors in Patients Undergoing Coronary Artery Bypass Grafting (CABG). Journal of Clinical Medicine. 2022; 11(14):4105. https://doi.org/10.3390/jcm11144105
Chicago/Turabian StyleReichert, Stefan, Britt Hofmann, Michael Kohnert, Alexander Navarrete Santos, Lisa Friebe, Julia Grollmitz, Hans-Günter Schaller, and Susanne Schulz. 2022. "Advanced Glycation End Product (AGE) and Soluble Receptor of AGE (sRAGE) Levels in Relation to Periodontitis Severity and as Putative 3-Year Outcome Predictors in Patients Undergoing Coronary Artery Bypass Grafting (CABG)" Journal of Clinical Medicine 11, no. 14: 4105. https://doi.org/10.3390/jcm11144105
APA StyleReichert, S., Hofmann, B., Kohnert, M., Santos, A. N., Friebe, L., Grollmitz, J., Schaller, H. -G., & Schulz, S. (2022). Advanced Glycation End Product (AGE) and Soluble Receptor of AGE (sRAGE) Levels in Relation to Periodontitis Severity and as Putative 3-Year Outcome Predictors in Patients Undergoing Coronary Artery Bypass Grafting (CABG). Journal of Clinical Medicine, 11(14), 4105. https://doi.org/10.3390/jcm11144105