
Renal Tubular Acidosis in Pregnant Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Cohort

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
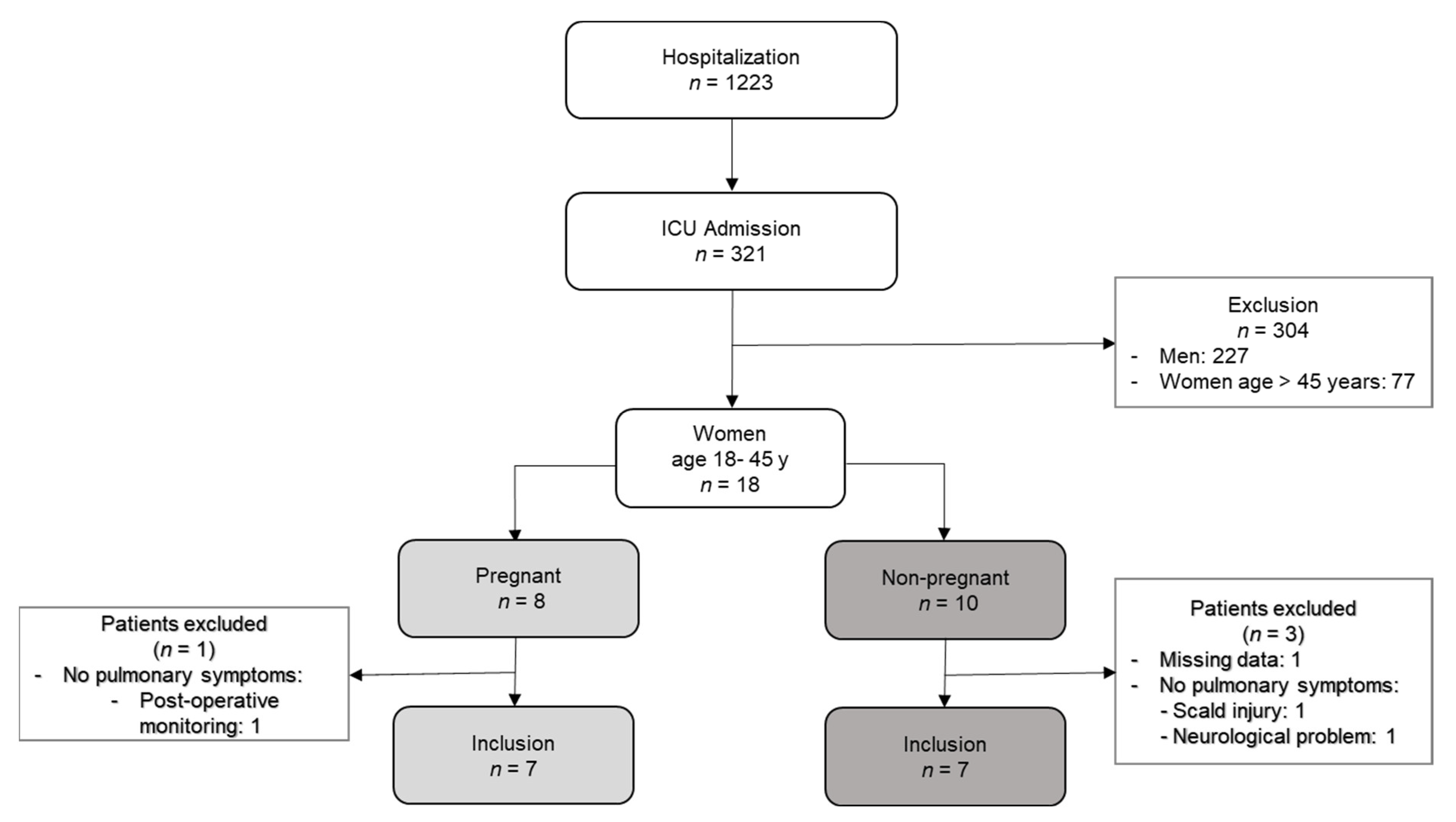
2.1. Patient Population
2.2. Study Design, Data Collection
2.3. Statistical Analysis
3. Results
3.1. Cohort Description/Demographics
3.2. Laboratory Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mir, T.; Almas, T.; Kaur, J.; Faisaluddin, M.; Song, D.; Ullah, W.; Mamtani, S.; Rauf, H.; Yadav, S.; Latchana, S.; et al. Coronavirus disease 2019 (COVID-19): Multisystem review of pathophysiology. Ann. Med. Surg. 2021, 69, 102745. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural evidence for direct renal infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020, 31, 1683–1687. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Udy, A.A.; Nichol, A.; Bellomo, R.; Deane, A.M.; El-Khawas, K.; Thummaporn, N.; Serpa Neto, A.; Bergin, H.; Short-Burchell, R.; et al. Incidence and management of metabolic acidosis with sodium bicarbonate in the ICU: An international observational study. Crit. Care 2021, 25, 45. [Google Scholar] [CrossRef] [PubMed]
- Gunnerson, K.J. Clinical review: The meaning of acid-base abnormalities in the intensive care unit part I—Epidemiology. Crit. Care 2005, 9, 508–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, R.C., Jr. Renal tubular acidosis. Mechanisms, classification and implications. N. Engl. J. Med. 1969, 281, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Vallés, P.G.; Batlle, D. Hypokalemic distal renal tubular acidosis. Adv. Chronic Kidney Dis. 2018, 25, 303–320. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Kelepouris, E.; Clegg, D.J. Renal tubular acidosis and management strategies: A narrative review. Adv. Ther. 2021, 38, 949–968. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Davison, J. Chronic kidney disease in pregnancy. BMJ 2008, 336, 211–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harel, Z.; McArthur, E.; Hladunewich, M.; Dirk, J.S.; Wald, R.; Garg, A.X.; Ray, J.G. Serum creatinine levels before, during, and after pregnancy. JAMA 2019, 321, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Seeger, H. Säure-Basen-Störungen in der Schwangerschaft. Der. Nephrol. 2018, 13, 19–29. [Google Scholar] [CrossRef]
- Seeger, H.; Salfeld, P.; Eisel, R.; Wagner, C.A.; Mohebbi, N. Complicated pregnancies in inherited distal renal tubular acidosis: Importance of acid-base balance. J. Nephrol. 2017, 30, 455–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firmin, C.J.; Kruger, T.F.; Davids, R. Proximal renal tubular acidosis in pregnancy. A case report and literature review. Gynecol. Obstet. Investig. 2007, 63, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Narcisse, D.; Agarwal, M.; Kumar, A. A rare case of transient proximal renal tubular acidosis in pregnancy. Case Rep. Nephrol. 2017, 2017, 1342135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaxley, J.; Pirrone, C. Review of the diagnostic evaluation of renal tubular acidosis. Ochsner J. 2016, 16, 525–530. [Google Scholar] [PubMed]
- Jonigk, D.; Märkl, B.; Helms, J. COVID-19: What the clinician should know about post-mortem findings. Intensive Care Med. 2021, 47, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pregnant (n = 7) | Nonpregnant (n = 7) | |
|---|---|---|
| HFOT (n, %) | 5 (71) | 3 (43) |
| Invasive MV (n, %) | 3 (43) | 5 (71) |
| ECMO (n, %) | 0 | 3 (43) |
| Steroids (n, %) | 6 (86) | 6 (86) |
| Remdesivir (n, %) | 0 | 3 (43) |
| Tocilizumab (n, %) | 0 | 2 (29) |
| Convalescent plasma (n, %) | 0 | 1 (14) |
| Pregnant (n = 7) | Nonpregnant (n = 7) | p-Value | |
|---|---|---|---|
| Age (years) | 31 (26–35) | 29 (25–43) | 1.0 |
| BMI (kg/m2) | 35 (26–43) | 29 (22–33) | 0.259 |
| SOFA score admission | 3 (3–6) | 2 (2–6) | 0.535 |
| SOFA score maximal | 6 (3–8) | 8 (6–10) | 0.209 |
| SAPS (24 h) | 19 (6–23) | 22 (21–42) | 0.053 |
| LDH (U/L) | 320 (284–553) | 403 (313–453) | 0.836 |
| Ferritin (µg/L) | 14 (40–285) | 518 (443–766) | 0.024 |
| CRP (mg/L) | 81 (56–131) | 166 (42–317) | 0.318 |
| PCT(µg/L) | 0.22 (0.13–0.26) | 0.22 (0.09–8.8) | 0.841 |
| Lymphocytes (G/L) | 0.76 (0.59–1.1) | 0.81 (0.56–1.41) | 0.62 |
| D-dimers (µg/L) | 2030 (720–2650) | 980 (410–1560) | 0.25 |
| Creatinine (µmol/L) | 42 (28–51) | 48 (44–75) | 0.073 |
| eGFR (mL/min) | 135 (123–158) | 117 (100–131) | 0.138 |
| BUN (mmol/L) | 1.1 (0.8–1.2) | 3.1 (2.6–6.2) | 0.002 |
| Potassium (mmol/L) | 3.1 (2.8–3.7) | 3.9 (3.4–4.2) | 0.053 |
| Hospital stay (days) | 12 (10–20) | 28 (12–40) | 0.209 |
| ICU stay (days) | 5 (5–8) | 15 (10–36) | 0.073 |
| Pregnant (n = 7) | Nonpregnant (n = 7) | p-Value | |
|---|---|---|---|
| pH admission | 7.38 (7.32–7.44) | 7.45 (7.4–7.49) | 0.16 |
| pH min | 7.3 (7.18–7.31) | 7.31 (7.28–7.34) | 0.535 |
| HCO3− admission (mmol/L) | 16.8 (16.2–22.2) | 24 (22.8–25) | 0.07 |
| HCO3− min (mmol/L) | 14.8 (12.8–18.6) | 22.7 (14.3–24.9) | 0.097 |
| paCO2 admission (kPa) | 3.4 (3.1–3.7) | 4.5 (3.9–5.9) | 0.007 |
| paCO2 at minimal HCO3− (kPa) | 3.4 (3.3–4.5) | 5.2 (4.2–5.9) | 0.097 |
| Cl− (mmol/L) | 112 (112–117) | 112 (111–114) | 0.383 |
| AG | 12 (8.2–16.1) | 7.5 (4–9.3) | 0.097 |
| Parameter | Pregnant (n = 7) | Nonpregnant (n = 7) | p-Value |
|---|---|---|---|
| Urine pH | 5.5 (5–6.5) | 6 (5.6–6.0) | 0.73 |
| Urine pH ≤ 5.3 (n) | 2 | 0 | |
| UAG | 33 (26.8–43.5) | 39 * | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humbel, S.; Wendel-Garcia, P.D.; Unseld, S.; Noll, F.; Schuepbach, R.A.; Ganter, C.C.; Seeger, H.; David, S.; Andermatt, R. Renal Tubular Acidosis in Pregnant Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Cohort. J. Clin. Med. 2022, 11, 4273. https://doi.org/10.3390/jcm11154273
Humbel S, Wendel-Garcia PD, Unseld S, Noll F, Schuepbach RA, Ganter CC, Seeger H, David S, Andermatt R. Renal Tubular Acidosis in Pregnant Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Cohort. Journal of Clinical Medicine. 2022; 11(15):4273. https://doi.org/10.3390/jcm11154273
Chicago/Turabian StyleHumbel, Simona, Pedro David Wendel-Garcia, Simone Unseld, Fabienne Noll, Reto Andreas Schuepbach, Christoph Camille Ganter, Harald Seeger, Sascha David, and Rea Andermatt. 2022. "Renal Tubular Acidosis in Pregnant Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Cohort" Journal of Clinical Medicine 11, no. 15: 4273. https://doi.org/10.3390/jcm11154273
APA StyleHumbel, S., Wendel-Garcia, P. D., Unseld, S., Noll, F., Schuepbach, R. A., Ganter, C. C., Seeger, H., David, S., & Andermatt, R. (2022). Renal Tubular Acidosis in Pregnant Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Cohort. Journal of Clinical Medicine, 11(15), 4273. https://doi.org/10.3390/jcm11154273