
Case-Fatality and Temporal Trends in Patients with Psoriasis and End-Stage Renal Disease

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Source of Data and Diagnoses Codes
2.2. Study Parameters, Outcomes, and Ethical Statement
2.3. Methods for Statistical Analyses
3. Results
3.1. Patient Collective
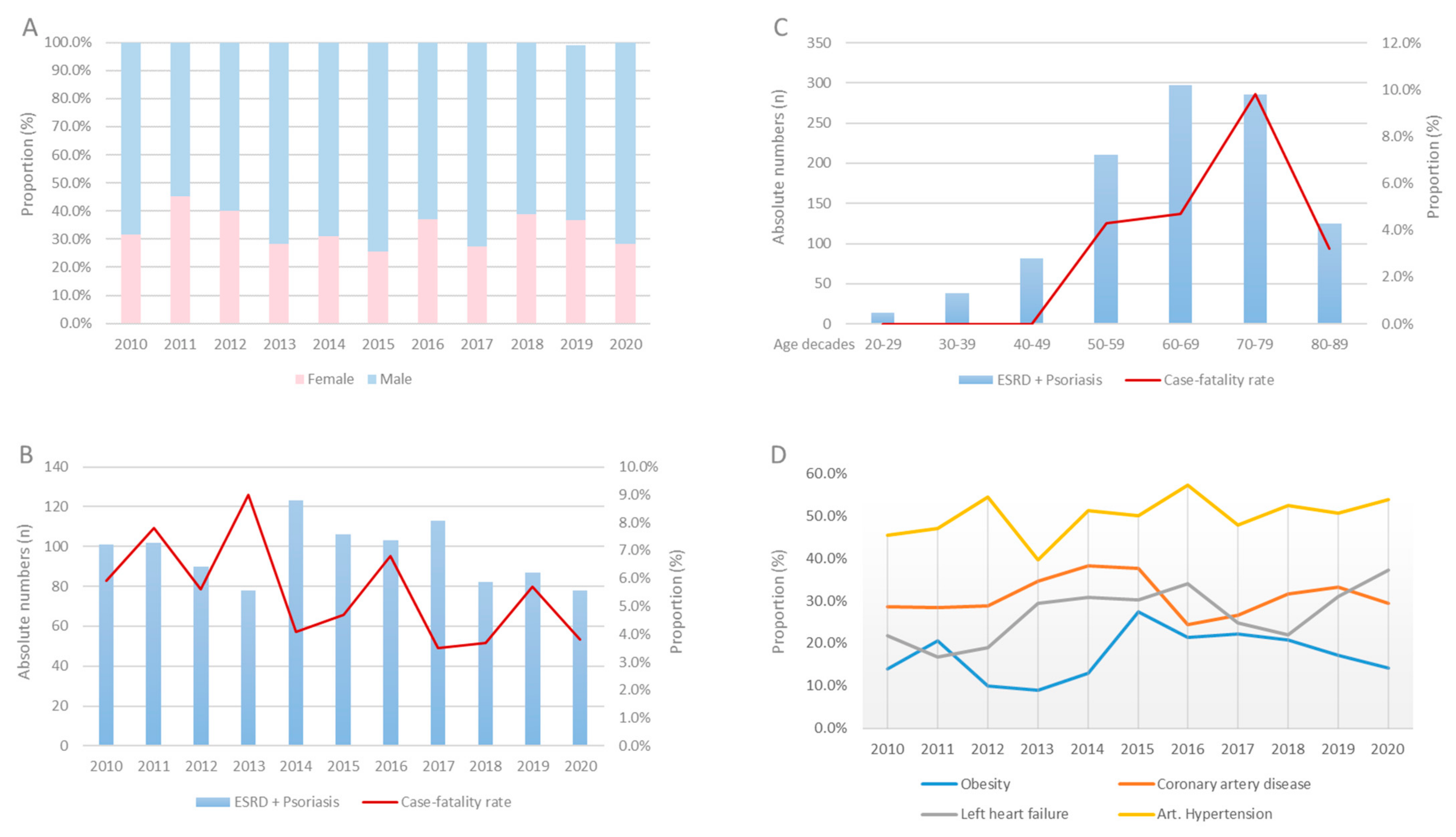
3.2. In-Hospital Trends over Eleven Years
3.3. Patients’ Characteristics of Nonsurvivors Compared with Survivors in Patients with ESRD and Psoriasis
3.4. Impact of Psoriasis on Adverse Events on Patients with ESRD
4. Discussion
- (I)
- Annual numbers of ESRD patients increased, whereas numbers of ERDS with psoriasis remained widely constant from 2010 to 2020.
- (II)
- While overall in-hospital mortality declined through time, patient characteristics shifted toward older age and more severe comorbidity profiles
- (III)
- Hospitalized ESRD patients with psoriasis were in median five years younger than in those without psoriasis.
- (IV)
- Despite younger age, we found a higher prevalence of severe, life-shortening comorbidities such as cancer and coronary heart disease in hospitalized patients with psoriasis than in patients without psoriasis.
- (V)
- The additive diagnosis psoriasis was not associated with the in-hospital case-fatality rate of patients with ESRD.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| CKD | chronic kidney disease |
| CPR | cardiopulmonary resuscitation |
| DRG | diagnosis related groups |
| ESRD | end-stage renal disease |
| GP | general practitioner |
| ICD | International Classification of Disease |
| IQR | interquartile range |
| OPS | surgery and interventional procedure keys (Operationen- und Prozedurenschlüssel) |
| OR | odds ratio |
References
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Rachakonda, T.D.; Schupp, C.W.; Armstrong, A.W. Psoriasis prevalence among adults in the United States. J. Am. Acad. Dermatol. 2014, 70, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boehncke, W.H.; Boehncke, S.; Tobin, A.M.; Kirby, B. The ‘psoriatic march’: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef]
- Reich, K. The concept of psoriasis as a systemic inflammation: Implications for disease management. J. Eur. Acad. Dermatol. Venereol. 2012, 26 (Suppl. S2), 3–11. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Troxel, A.B.; Lewis, J.D.; Kurd, S.K.; Shin, D.B.; Wang, X.; Margolis, D.J.; Strom, B.L. The risk of mortality in patients with psoriasis: Results from a population-based study. Arch. Dermatol. 2007, 143, 1493–1499. [Google Scholar] [CrossRef]
- Garshick, M.S.; Berger, J.S. Psoriasis and Cardiovascular Disease-An Ounce of Prevention Is Worth a Pound of Cure. JAMA Dermatol. 2022, 10, 4723. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B. Risk of myocardial infarction in patients with psoriasis. JAMA 2006, 296, 1735–1741. [Google Scholar] [CrossRef] [Green Version]
- Karbach, S.; Croxford, A.L.; Oelze, M.; Schuler, R.; Minwegen, D.; Wegner, J.; Koukes, L.; Yogev, N.; Nikolaev, A.; Reissig, S.; et al. Interleukin 17 drives vascular inflammation, endothelial dysfunction, and arterial hypertension in psoriasis-like skin disease. Arter. Thromb. Vasc. Biol. 2014, 34, 2658–2668. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.; Han, J.H.; Bang, C.H.; Yoo, S.A.; Han, K.D.; Kim, H.N.; Park, Y.M.; Lee, J.Y.; Lee, J.H. Risk of End-Stage Renal Disease in Psoriatic Patients: Real-World Data from a Nationwide Population-Based Cohort Study. Sci. Rep. 2019, 9, 16581. [Google Scholar] [CrossRef] [Green Version]
- Chi, C.C.; Wang, J.; Chen, Y.F.; Wang, S.H.; Chen, F.L.; Tung, T.H. Risk of incident chronic kidney disease and end-stage renal disease in patients with psoriasis: A nationwide population-based cohort study. J. Dermatol. Sci. 2015, 78, 232–238. [Google Scholar] [CrossRef]
- Wan, J.; Wang, S.; Haynes, K.; Denburg, M.R.; Shin, D.B.; Gelfand, J.M. Risk of moderate to advanced kidney disease in patients with psoriasis: Population based cohort study. BMJ 2013, 347, f5961. [Google Scholar] [CrossRef] [Green Version]
- Jabbar-Lopez, Z.K.; Weatherhead, S.C.; Reynolds, N.J. Kidney disease in moderate-to-severe psoriasis: A critical appraisal. Br. J. Dermatol. 2016, 174, 267–270. [Google Scholar] [CrossRef]
- Singh, N.P.; Prakash, A.; Kubba, S.; Ganguli, A.; Singh, A.K.; Sikdar, S.; Agarwal, S.K.; Dinda, A.K.; Grover, C. Psoriatic nephropathy—Does an entity exist? Ren. Fail. 2005, 27, 123–127. [Google Scholar]
- Bae, E.H.; Kim, B.; Song, S.H.; Oh, T.R.; Suh, S.H.; Choi, H.S.; Kim, C.S.; Ma, S.K.; Han, K.D.; Kim, S.W. Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 2356. [Google Scholar] [CrossRef]
- Wen, C.P.; Matsushita, K.; Coresh, J.; Iseki, K.; Islam, M.; Katz, R.; McClellan, W.; Peralta, C.A.; Wang, H.; de Zeeuw, D.; et al. Relative risks of chronic kidney disease for mortality and end-stage renal disease across races are similar. Kidney Int. 2014, 86, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Hobohm, L.; Ebner, M.; Kresoja, K.P.; Munzel, T.; Konstantinides, S.V.; Lankeit, M. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur. Heart J. 2019, 41, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Hobohm, L.; von Bardeleben, R.S.; Ostad, M.A.; Wenzel, P.; Munzel, T.; Gori, T.; Keller, K. 5-Year Experience of In-Hospital Outcomes After Percutaneous Left Atrial Appendage Closure in Germany. JACC Cardiovasc. Int. 2019, 12, 1044–1052. [Google Scholar] [CrossRef]
- Shaheen, F.A.M.; Al-Attar, B.; Ahmad, M.K.; Follero, P.M. Burden of disease: Prevalence and incidence of endstage renal disease in Middle Eastern countries. Clin. Nephrol. 2020, 93, 120–123. [Google Scholar] [CrossRef]
- Springate, D.A.; Parisi, R.; Kontopantelis, E.; Reeves, D.; Griffiths, C.E.; Ashcroft, D.M. Incidence, prevalence and mortality of patients with psoriasis: A U.K. population-based cohort study. Br. J. Dermatol. 2017, 176, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Tokuyama, M.; Mabuchi, T. New Treatment Addressing the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, K.; Olsen, A.O.; Wilsgaard, T.; Furberg, A.S. Is the prevalence of psoriasis increasing? A 30-year follow-up of a population-based cohort. Br. J. Dermatol. 2013, 168, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Hobohm, L.; Ostad, M.A.; Karbach, S.; Espinola-Klein, C.; Munzel, T.; Gelfand, J.M.; Konstantinides, S.V.; Steinbrink, K.; Gori, T. Psoriasis and its impact on the clinical outcome of patients with pulmonary embolism. Int. J. Cardiol. 2021, 343, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Karbach, S.; Hobohm, L.; Wild, J.; Munzel, T.; Gori, T.; Wegner, J.; Steinbrink, K.; Wenzel, P.; Keller, K. Impact of Psoriasis on Mortality Rate and Outcome in Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e016956. [Google Scholar] [CrossRef]
- Wild, J.; Hobohm, L.; Munzel, T.; Wenzel, P.; Steinbrink, K.; Karbach, S.; Keller, K. Psoriasis and Its Impact on In-Hospital Outcome in Patients Hospitalized with Acute Kidney Injury. J. Clin. Med. 2020, 9, 3004. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Patients with severe psoriasis are at increased risk of cardiovascular mortality: Cohort study using the General Practice Research Database. Eur. Heart J. 2010, 31, 1000–1006. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, E.J.; Harskamp, C.T.; Armstrong, A.W. Psoriasis and major adverse cardiovascular events: A systematic review and meta-analysis of observational studies. J. Am. Heart Assoc. 2013, 2, e000062. [Google Scholar] [CrossRef] [Green Version]
- Ahlehoff, O.; Gislason, G.H.; Lindhardsen, J.; Olesen, J.B.; Charlot, M.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Prognosis following first-time myocardial infarction in patients with psoriasis: A Danish nationwide cohort study. J. Intern. Med. 2011, 270, 237–244. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | ESRD with Psoriasis (n = 1063; 0.3%) | ESRD without Psoriasis (n = 359,917; 99.7%) | p-Value |
|---|---|---|---|
| Age (years) | 66 [56–75] | 71 [59–79] | <0.001 |
| Sex (female) | 356 (33.5%) | 144,561 (40.2%) | <0.001 |
| Obesity | 186 (17.5%) | 29,610 (8.2%) | <0.001 |
| In-hospital stay | 8 (3–16) | 5 (2–13) | <0.001 |
| Comorbidities | |||
| Coronary artery disease | 331 (31.1%) | 100,843 (28.0%) | 0.026 |
| Malignancy | 52 (4.9%) | 11,778 (3.3%) | <0.001 |
| Left heart failure | 286 (26.9%) | 81,221 (22.6%) | 0.001 |
| Right heart failure | 111 (10.4%) | 32,042 (8.9%) | 0.082 |
| COPD | 172 (16.2%) | 48,906 (13.6%) | 0.014 |
| Diabetes mellitus | 454 (42.7%) | 138,502 (38.5%) | 0.005 |
| Arterial hypertension | 532 (50.0%) | 172,778 (48.0%) | 0.186 |
| Hypertensive Nephropathy | 101 (9.5%) | 26,325 (7.3%) | 0.007 |
| Atrial fibrillation/flutter | 239 (22.5%) | 83,677 (23.2%) | 0.584 |
| Deep vein thrombosis or thrombophlebitis | 9 (0.8%) | 2906 (0.8%) | 0.863 |
| Dialysis modalities | |||
| Dialysis general | 467 (43.9%) | 153,121 (42.5%) | 0.368 |
| Haemofiltration | 26 (2.4%) | 6662 (1.9%) | 0.166 |
| Haemodialysis | 459 (43.2%) | 150,567 (41.8%) | 0.383 |
| Haemodiafiltration | 108 (10.2%) | 27,720 (7.7%) | 0.003 |
| Adverse events during hospitalization | |||
| Gastrointestinal bleeding | 6 (0.2%) | 3746 (1.0%) | 0.169 |
| Intracranial bleeding | 0 (0%) | 361 (0.1%) | 0.632 |
| Myocardial infarction | 12 (1.1%) | 4402 (1.2%) | 0.889 |
| Ischemic Stroke | 11 (1.0%) | 2248 (0.6%) | 0.113 |
| Pulmonary embolism | 6 (0.6%) | 888 (0.2%) | 0.051 |
| Cardiopulmonary reanimation | 14 (1.3%) | 5432 (1.5%) | 0.693 |
| Transfusion of erythrocytes | 209 (19.7%) | 62,038 (17.2%) | 0.037 |
| MACCE | 73 (6.9%) | 26,096 (7.3%) | 0.673 |
| In-hospital mortality | 58 (5.5%) | 21,362 (5.9%) | 0.554 |
| Univariate Regression Model | Multivariate Regression Model * | |||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| In-hospital mortality | 0.92 (0.70–1.19) | 0.509 | 1.015 (0.78–1.33) | 0.915 |
| Acute myocardial infarction | 0.92 (0.52–1.63) | 0.780 | 0.84 (0.48–1.49) | 0.563 |
| Ischemic Stroke | 1.66 (0.92–3.02) | 0.094 | 1.64 (0.90–2.97) | 0.105 |
| Deep venous thrombosis or thrombophlebitis | 1.05 (0.54–2.02) | 0.886 | 1.02 (0.53–1.97) | 0.955 |
| Pulmonary embolism | 2.30 (1.03–5.13) | 0.043 | 2.16 (0.96–4.83) | 0.062 |
| Gastrointestinal bleeding | 0.54 (0.23–1.21) | 0.132 | 0.54 (0.24–1.21) | 0.137 |
| Transfusion of blood constituents | 1.18 (1.01–1.37) | 0.037 | 1.18 (1.02–1.38) | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wild, J.; Keller, K.; Karbach, S.; Weinmann-Menke, J.; Münzel, T.; Hobohm, L. Case-Fatality and Temporal Trends in Patients with Psoriasis and End-Stage Renal Disease. J. Clin. Med. 2022, 11, 4328. https://doi.org/10.3390/jcm11154328
Wild J, Keller K, Karbach S, Weinmann-Menke J, Münzel T, Hobohm L. Case-Fatality and Temporal Trends in Patients with Psoriasis and End-Stage Renal Disease. Journal of Clinical Medicine. 2022; 11(15):4328. https://doi.org/10.3390/jcm11154328
Chicago/Turabian StyleWild, Johannes, Karsten Keller, Susanne Karbach, Julia Weinmann-Menke, Thomas Münzel, and Lukas Hobohm. 2022. "Case-Fatality and Temporal Trends in Patients with Psoriasis and End-Stage Renal Disease" Journal of Clinical Medicine 11, no. 15: 4328. https://doi.org/10.3390/jcm11154328
APA StyleWild, J., Keller, K., Karbach, S., Weinmann-Menke, J., Münzel, T., & Hobohm, L. (2022). Case-Fatality and Temporal Trends in Patients with Psoriasis and End-Stage Renal Disease. Journal of Clinical Medicine, 11(15), 4328. https://doi.org/10.3390/jcm11154328