
New-Onset Atrial Fibrillation in Acute Myocardial Infarction Is a Different Phenomenon than Other Pre-Existing Types of That Arrhythmia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
- NOAF (group of patients with any newly diagnosed AF that appeared during AMI hospitalization without a prior diagnosis of AF as it was precisely described [9]);
- AF (group of patients with a previously documented diagnosis of AF who additionally had AF during AMI hospitalization);
- Prior-AF (group of patients with a previously documented diagnosis of AF who had not developed AF during AMI hospitalization); and
- Non-AF (group of patients with no evidence of AF during AMI hospitalization and without the prior AF diagnosis).
Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. In-Hospital Characteristics and Outcomes
3.3. In-Hospital Laboratory and Echocardiographic Parameters
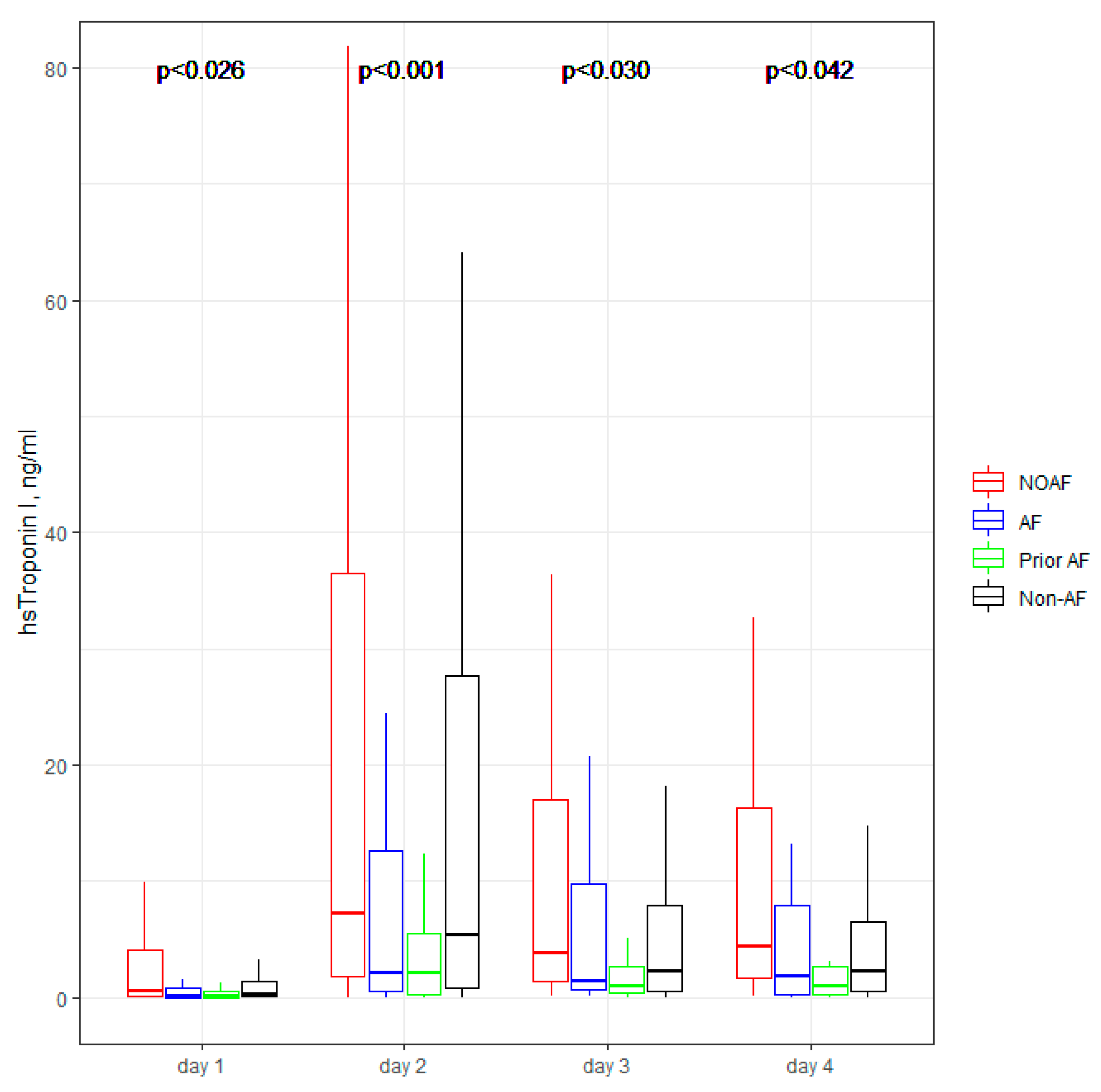
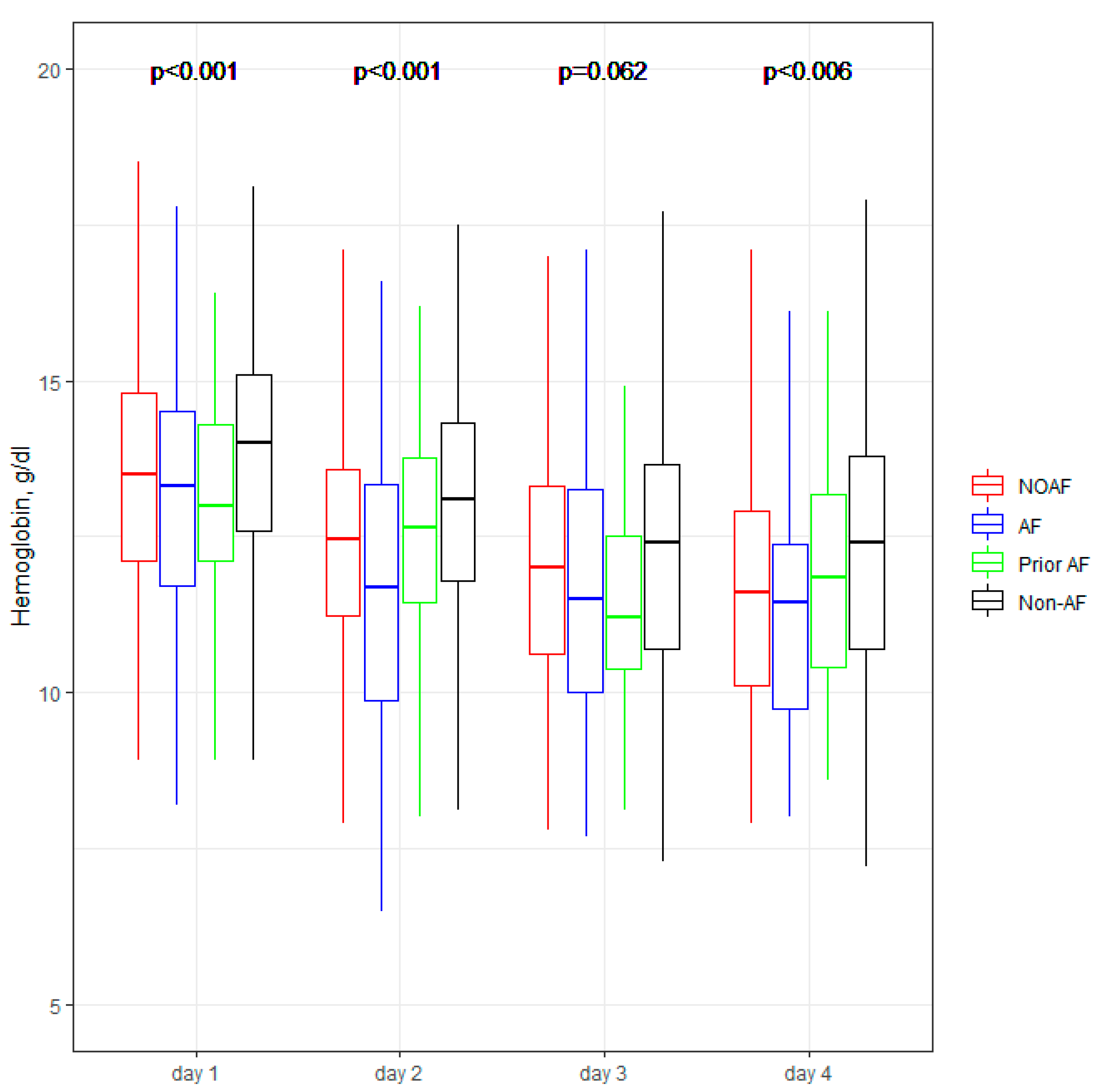
3.4. In-Hospital Laboratory Parameters Dynamic
3.5. Pharmacological Treatment at Discharge
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.J.; Yarzebski, J.; Lessard, D.; Wu, J.; Gore, J.M. Recent trends in the incidence rates of and death rates from atrial fibrillation complicating initial acute myocardial infarction: A community-wide perspective. Am. Heart J. 2002, 143, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Batra, G.; Svennblad, B.; Held, C.; Jernberg, T.; Johanson, P.; Wallentin, L.; Oldgren, J. All types of atrial fibrillation in the setting of myocardial infarction are associated with impaired outcome. Heart 2016, 102, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.J.; Seeley, D.; Becker, R.C.; Brady, P.; Chen, Z.; Osganian, V.; Gore, J.M.; Alpert, J.S.; Dalen, J.E. Impact of atrial fibrillation on the in-hospital and long-term survival of patients with acute myocardial infarction: A community-wide perspective. Am. Heart J. 1990, 119, 996–1001. [Google Scholar] [CrossRef]
- Schmitt, J.; Duray, G.; Gersh, B.J.; Hohnloser, S.H. Atrial fibrillation in acute myocardial infarction: A systematic review of the incidence, clinical features and prognostic implications. Eur. Heart J. 2009, 30, 1038–1045. [Google Scholar] [CrossRef] [Green Version]
- Topaz, G.; Flint, N.; Steinvil, A.; Finkelstein, A.; Banai, S.; Keren, G.; Shacham, Y.; Yankelson, L. Long term prognosis of atrial fibrillation in ST-elevation myocardial infarction patients undergoing percutaneous coronary intervention. Int. J. Cardiol. 2017, 240, 228–233. [Google Scholar] [CrossRef]
- Khalfallah, M.; Elsheikh, A. Incidence, predictors, and outcomes of new-onset atrial fibrillation in patients with ST-elevation myocardial infarction. Ann. Noninvasive Electrocardiol. 2020, 25, e12746. [Google Scholar] [CrossRef] [Green Version]
- Shiyovich, A.; Axelrod, M.; Gilutz, H.; Plakht, Y. Early Versus Late New-Onset Atrial Fibrillation in Acute Myocardial Infarction: Differences in Clinical Characteristics and Predictors. Angiology 2019, 70, 921–928. [Google Scholar] [CrossRef]
- Raczkowska-Golanko, M.; Raczak, G.; Gruchała, M.; Daniłowicz-Szymanowicz, L. Comprehensive use of routine clinical parameters to identify patients at risk of new-onset atrial fibrillation in acute myocardial infarction. J. Clin. Med. 2021, 10, 3622. [Google Scholar] [CrossRef]
- Podolecki, T.; Lenarczyk, R.; Kowalczyk, J.; Kurek, T.; Boidol, J.; Chodor, P.; Swiatkowski, A.; Sredniawa, B.; Polonski, L.; Kalarus, Z. Effect of type of atrial fibrillation on prognosis in acute myocardial infarction treated invasively. Am. J. Cardiol. 2012, 109, 1689–1693. [Google Scholar] [CrossRef]
- Mehta, R.H.; Dabbous, O.H.; Granger, C.B.; Kuznetsova, P.; Kline-Rogers, E.M.; Anderson, F.A.; Fox, K.A.A.; Gore, J.M.; Goldberg, R.J.; Eagle, K.A. Comparison of outcomes of patients with acute coronary syndromes with and without atrial fibrillation. Am. J. Cardiol. 2003, 92, 1031–1036. [Google Scholar] [CrossRef]
- Biasco, L.; Radovanovic, D.; Moccetti, M.; Rickli, H.; Roffi, M.; Eberli, F.; Jeger, R.; Moccetti, T.; Erne, P.; Pedrazzini, G. New-onset or Pre-existing Atrial Fibrillation in Acute Coronary Syndromes: Two Distinct Phenomena with a Similar Prognosis. Rev. Esp. Cardiol. 2019, 72, 383–391. [Google Scholar] [CrossRef]
- Maagh, P.; Butz, T.; Wickenbrock, I.; Prull, M.W.; Plehn, G.; Trappe, H.J.; Meissner, A. New-onset versus chronic atrial fibrillation in acute myocardial infarction: Differences in short- and long-term follow-up. Clin. Res. Cardiol. 2011, 100, 167–175. [Google Scholar] [CrossRef]
- Foudad, H.; Bouaguel, I.; Trichine, A.; Merghit, R.; Adjabi, T. 0264: Short- and long-term prognosis of previous and new-onset atrial fibrillation in ST-segment elevation acute myocardial infarction in Algeria. Arch. Cardiovasc. Dis. Suppl. 2016, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Podolecki, T.; Lenarczyk, R.; Kowalczyk, J.; Jedrzejczyk-Patej, E.; Swiatkowski, A.; Chodor, P.; Sedkowska, A.; Streb, W.; Mitrega, K.; Kalarus, Z. Significance of Atrial Fibrillation Complicating ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2017, 120, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef]
- Pedersen, O.D.; Bagger, H.; Køber, L.; Torp-Pedersen, C. The occurrence and prognostic significance of atrial fibrillation/-flutter following acute myocardial infarction. TRACE Study group. TRAndolapril Cardiac Evalution. Eur. Heart J. 1999, 20, 748–754. [Google Scholar] [CrossRef] [Green Version]
- Pizzetti, F.; Turazza, F.M.; Franzosi, M.G.; Barlera, S.; Ledda, A.; Maggioni, A.P.; Santoro, L.; Tognoni, G. Incidence and prognostic significance of atrial fibrillation in acute myocardial infarction: The GISSI-3 data. Heart 2001, 86, 527–532. [Google Scholar] [CrossRef]
- González-Pacheco, H.; Eid-Lidt, G.; Altamirano-Castillo, A.; Álvarez-Sangabriel, A.; González-Hermosillo, A.; Meléndez-Ramírez, G.; Briseño-Cruz, J.L.; Galván-Carrasco, M.; Ordaz-Soto, S.; Martínez-Sánchez, C. Prevalence and prognostic implications of different types of atrial fibrillation in patients admitted to a coronary care unit. Int. J. Cardiol. 2014, 172, e379–e381. [Google Scholar] [CrossRef]
- Meyers, H.P.; Bracey, A.; Lee, D.; Lichtenheld, A.; Li, W.J.; Singer, D.D.; Kane, J.A.; Dodd, K.W.; Meyers, K.E.; Thode, H.C.; et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. J. Emerg. Med. 2021, 60, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Gal, P.; Parlak, E.; Schellings, D.A.A.M.; Beukema, R.; ten Berg, J.; Adiyaman, A.; van ’t Hof, A.W.J.; Elvan, A. Association of serial high sensitivity troponin T with onset of atrial fibrillation in ST elevation myocardial infarction patients undergoing primary percutaneous coronary intervention. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Farah, R.; Nassar, M.; Aboraya, B.; Nseir, W. Low serum potassium levels are associated with the risk of atrial fibrillation. Acta Cardiol. 2021, 76, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Murakami, Y.; Okada, T.; Okamoto, M.; Shimizu, T.; Toyama, J.; Yoshida, Y.; Tsuboi, N.; Ito, T.; Muto, M.; et al. Plasma Atrial Natriuretic Peptide and Brain Natriuretic Peptide Levels After Radiofrequency Catheter Ablation of Atrial Fibrillation. Am. J. Cardiol. 2006, 97, 1741–1744. [Google Scholar] [CrossRef]
- Miake, J.; Kato, M.; Ogura, K.; Iitsuka, K.; Okamura, A.; Tomomori, T.; Tsujimoto, D.; Kato, M.; Yamamoto, K. Pre-ablation levels of brain natriuretic peptide are independently associated with the recurrence of atrial fibrillation after radiofrequency catheter ablation in patients with nonvalvular atrial fibrillation. Heart Vessel. 2019, 34, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Lip, G.Y.H.; Apostolakis, S. Inflammation in atrial fibrillation. J. Am. Coll. Cardiol. 2012, 60, 2263–2270. [Google Scholar] [CrossRef] [Green Version]
- Gedikli, O.; Dogan, A.; Altuntas, I.; Altinbas, A.; Ozaydin, M.; Akturk, O.; Acar, G. Inflammatory markers according to types of atrial fibrillation. Int. J. Cardiol. 2007, 120, 193–197. [Google Scholar] [CrossRef]
- Rizos, I.; Rigopoulos, A.G.; Kalogeropoulos, A.S.; Tsiodras, S.; Dragomanovits, S.; Sakadakis, E.A.; Faviou, E.; Kremastinos, D.T. Hypertension and paroxysmal atrial fibrillation: A novel predictive role of high sensitivity C-reactive protein in cardioversion and long-term recurrence. J. Hum. Hypertens. 2010, 24, 447–457. [Google Scholar] [CrossRef]
- Amar, D.; Goenka, A.; Zhang, H.; Park, B.; Thaler, H.T. Leukocytosis and increased risk of atrial fibrillation after general thoracic surgery. Ann. Thorac. Surg. 2006, 82, 1057–1061. [Google Scholar] [CrossRef]
- Lamm, G.; Auer, J.; Weber, T.; Berent, R.; Ng, C.; Eber, B. Postoperative white blood cell count predicts atrial fibrillation after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2006, 20, 51–56. [Google Scholar] [CrossRef]
- Yoshizaki, T.; Umetani, K.; Ino, Y.; Takahashi, S.; Nakamura, M.; Seto, T.; Aizawa, K. Activated inflammation is related to the incidence of atrial fibrillation in patients with acute myocardial infarction. Intern. Med. 2012, 51, 1467–1471. [Google Scholar] [CrossRef] [Green Version]
- Sanjay, O.P. Pre-operative serum potassium levels and peri-operative outcomes in patients undergoing cardiac surgery. Indian J. Clin. Biochem. 2004, 19, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Schulman, M.; Narins, R.G. Hypokalemia and cardiovascular disease. Am. J. Cardiol. 1990, 65, E4. [Google Scholar] [CrossRef]
- Krijthe, B.P.; Heeringa, J.; Kors, J.A.; Hofman, A.; Franco, O.H.; Witteman, J.C.M.; Stricker, B.H. Serum potassium levels and the risk of atrial fibrillation: The Rotterdam Study. Int. J. Cardiol. 2013, 168, 5411–5415. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.D.; Bai, Y.; Liu, X.Y.; Liu, Y.; Wang, Z.Z.; Zhong, P. Patients with acute myocardial infarction and atrial fibrillation: Association of anaemia with risk of in-hospital bleeding, stroke and other death causes. Biomarkers 2021, 26, 163–167. [Google Scholar] [CrossRef]
- Vaziri, S.M.; Larson, M.G.; Benjamin, E.J.; Levy, D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation 1994, 89, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Aronson, D.; Mutlak, D.; Bahouth, F.; Bishara, R.; Hammerman, H.; Lessick, J.; Carasso, S.; Dabbah, S.; Reisner, S.; Agmon, Y. Restrictive left ventricular filling pattern and risk of new-onset atrial fibrillation after acute myocardial infarction. Am. J. Cardiol. 2011, 107, 1738–1743. [Google Scholar] [CrossRef]
- Ice, D.S.; Shapiro, T.A.; Gnall, E.M.; Kowey, P.R. Unanswered questions in patients with concurrent atrial fibrillation and acute coronary syndrome. Am. J. Cardiol. 2014, 113, 888–896. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NOAF * n = 106 | AF § n = 95 | Prior-AF ¶ n = 60 | Non-AF n = 693 | p | |
|---|---|---|---|---|---|
| Age (years old) | 73 (66–84) | 74 (67–82) | 72 (69–78) | 65 (59–73), *,¶ | 0.001 |
| Male sex, n (%) | 67 (63%) | 55 (58%) | 42 (70%) | 473 (68%) | 0.172 |
| Prior MI, n (%) | 31 (29%), ¶ | 41 (43%) | 32 (53%), * | 172 (25%), §,¶ | 0.001 |
| Prior revascularization (PCI/CABG), n (%) | 26 (25%), §,¶ | 41 (43%), * | 28 (47%), * | 175 (25%), §,¶ | 0.001 |
| Hypertension, n (%) | 79 (75%), ¶ | 82 (86%) | 55 (92%), * | 502 (73%), §,¶ | 0.001 |
| Diabetes mellitus, n (%) | 31 (29%), §,¶ | 45 (47%), * | 28 (47%), * | 210 (30%), §,¶ | 0.001 |
| Previous stroke, n (%) | 10 (9.4%) | 19 (20%) | 5 (8%) | 36 (5%), § | 0.001 |
| On-Admission Treatment | |||||
| Aspirin, n (%) | 43 (41%) | 32 (34%) | 22 (37%) | 259 (38%) | 0.826 |
| ACE inhibitors/sartans, n (%) | 53 (50%), §,¶ | 67 (71%), * | 44 (73%), * | 346 (50%), §,¶ | 0.001 |
| Statins, n (%) | 41 (39%), ¶ | 48 (51%) | 37 (62%), * | 249 (36%), §,¶ | 0.001 |
| NOAF * n = 106 | AF § n = 95 | Prior-AF ¶ n = 60 | Non-AF n = 693 | p | |
|---|---|---|---|---|---|
| Types of Myocardial Infarction | |||||
| ST-elevation MI, n (%) | 42 (40%), §,¶ | 16 (17%), * | 9 (15%), * | 260 (36%), §,¶ | 0.001 |
| Non-ST-elevation MI, n (%) | 64 (60%), §,¶ | 79 (83%), * | 51 (85%), * | 423 (62%), §,¶ | 0.001 |
| In-hospital coronary angiography, n (%) | 99 (93%) | 90 (95%) | 58 (97%) | 674 (97%) | 0.121 |
| In-hospital PCI, n (%) | 81 (76%) | 69 (73%) | 49 (82%) | 580 (83%) | 0.413 |
| In-Hospital Prognosis | |||||
| Length of hospitalization (days) | 10 (7–17), ¶ | 9 (6–14), ¶ | 7 (5–10), *, § | 6 (5–8), *,§ | 0.001 |
| VT during hospitalization, n (%) | 6 (6%) | 3 (3%) | 2 (3%) | 15 (2%) | 0.166 |
| VF during hospitalization, n (%) | 14 (13%) | 4 (4%) | 1 (2%) | 46 (7%) | 0.023 |
| AVB III during hospitalization, n (%) | 6 (6%) | 1 (1%) | 1 (2%) | 7 (1%), * | 0.013 |
| Stroke during hospitalization, n (%) | 3 (3%) | 2 (2%) | 1 (2%) | 3 (0.43%) | 0.023 |
| In-hospital mortality, n (%) | 19 (18%), ¶ | 9 (9%) | 2 (3%), * | 28 (4%), * | 0.001 |
| Sinus rhythm at discharge, n (%) | 74 (85%), §,¶ | 31 (36%), *,¶ | 52 (89%), *,§ | 661 (99%), *,§ | 0.001 |
| NOAF * n = 106 | AF § n = 95 | Prior-AF ¶ n = 60 | Non-AF n = 693 | p | |
|---|---|---|---|---|---|
| BNP, pg/mL | 491 (193–1087), ¶ | 270 (158–895) | 248 (78–622), * | 114 (43–362), *, § | 0.001 |
| hsTnI, ng/mL | 0.64 (0.06–4.84), §,¶ | 0.148 (0.04–0.78), * | 0.127 (0.03–0.55), * | 0.215 (0.05–1.40) | 0.026 |
| hsTnI max, ng/mL | 10.59 (2.98–36.62), §,¶ | 3.11 (0.91–13.48), * | 2.37 (0.78–6.64), * | 6.51 (1.35–28.11), *,§,¶ | 0.001 |
| CK-MB, ng/mL | 4.75 (2.2–14) | 4 (2.0–7.5) | 3.35 (1.5–6.2) | 4.05 (2.1–11.2) | 0.136 |
| CRP, mg/L | 11.2 (3.55–34.5), ¶ | 6.5 (2.8–16.6), * | 3.56 (1.8–12.4), * | 3.4 (1.4–9.9 ), *,§ | 0.001 |
| Sodium, mmol/L | 138 (135–140) | 138 (135–140) | 138 (136–140) | 138 (136–140) | 0.167 |
| Potassium, mmol/L | 4.1 (3.8–4.5), § | 4.4 (4.1–4.8), * | 4.3 (3.9–4.7) | 4.3 (4.0–4.6), * | 0.007 |
| Hemoglobin, g/dL | 13.5 (12.1–14.8) | 13.3 (11.7–14.5) | 13.0 (12.1–14.3) | 14 (12.6–15.1), §,¶ | 0.001 |
| Leucocytes, × 109/L | 10.87 (8.18–13.91) | 10.23 (7.84–13.3) | 9.08 (7.13–12.69) | 9.77 (7.86–12.12), * | 0.065 |
| Neutrophil to lymphocyte ratio | 3.81 (2.2–6.8) | 3.82 (2.5–8.0) | 3.8 (2.5–6.5) | 3.08 (2.0–5.1), § | 0.002 |
| Total cholesterol, mg/dL | 169 (129–191) | 148 (128–189) | 159 (136–196) | 181 (148–218), *,§,¶ | 0.001 |
| LDL-C, mg/dL | 98 (64–124) | 87 (72–107) | 94 (78–130) | 109 (80–145), *,§ | 0.001 |
| Creatinine, ml/dL | 0.96 (0.78–1.24), § | 1.14 (0.94–1.48), * | 0.95 (0.8–1.33) | 0.92 (0.78–1.13), § | 0.004 |
| TSH, uU/L | 1.16 (0.66–1.85) | 1.13 (0.60–2.22) | 1.24 (0.82–2.59) | 1.06 (0.48–1.67) | 0.147 |
| FT3, pmol/L | 2.97 (2.75–3.30) | 3.41 (2.54–3.78) | 2.94 (2.54–3.42) | 3.12 (2.67–3.7) | 0.696 |
| FT4, pmol/L | 14.74 (13.40–16.10) | 14.07 (12.36–15.27) | 13.44 (12.49–14.54) | 12.71 (11.31–14.51), * | 0.009 |
| Glucose, mg/dL | 155 (120–219), §,¶ | 132 (101–186), * | 118 (106–163), * | 126 (103–172), * | 0.001 |
| Echocardiographic Parameters | |||||
| LVEF, % | 40 (33–50) | 44 (32–55) | 49 (40–55) | 50 (41–58), *,§ | 0.001 |
| LA size, mm | 42 (38–46), § | 45 (41–50), *,¶ | 42 (38–45), § | 39 (35–42), *,§,¶ | 0.001 |
| LVIDd, mm | 50 (44–55) | 50 (46–56) | 49 (45–56) | 49 (45–53) | 0.204 |
| RVID, mm | 42 (34–44) | 42 (35–49) | 36 (32–43) | 35 (32–39), *,§ | 0.001 |
| TAPSE, mm | 19 (15–22) | 17 (15–20) | 19 (17–22) | 21 (18–24), *,§ | 0.001 |
| RVSP, mmHg | 43 (35–47) | 45 (35–46) | 40 (31–47) | 40 (30–46) | 0.410 |
| NOAF n= 86 | AF n = 85 | Prior-AF n = 58 | Non-AF n = 662 | p | |
|---|---|---|---|---|---|
| Beta-blockers, n (%) | 76 (88%) | 76 (89%) | 48 (83%) | 575 (87%) | 0.677 |
| ACE inhibitors/sartans, n (%) | 73 (85%) | 73 (86%) | 47 (81%) | 608 (92%) | 0.006 |
| Statins, n (%) | 81 (94%) | 74 (87%) | 53 (91%) | 633 (96%) | 0.011 |
| Antithrombotic Therapy | |||||
| Aspirin, n (%) | 76 (88%) | 74 (87%) | 53 (91%) | 639 (97%) | 0.001 |
| Clopidogrel, n (%) | 72 (84%) | 72 (85%) | 51 (88%) | 495 (75%) | 0.012 |
| Ticagrelor, n (%) | 3 (3%) | 0 (0%) | 0 (0%) | 145 (22%) | 0.001 |
| Vitamin K antagonists, n (%) | 8 (9%) | 24 (28%) | 10 (17%) | 13 (2%) | 0.001 |
| NOACs, n (%) | 54 (63%) | 51 (60%) | 23 (40%) | 12 (2%) | 0.001 |
| Low-molecular-weight heparins, n (%) | 7 (8%) | 8 (10%) | 9 (16%) | 18 (3%) | 0.001 |
| Triple Antithrombotic Therapy | |||||
| Aspirin + Clopidogrel + Vitamin K antagonists | 8 (9%) | 19 (22%) | 10 (17%) | 9 (1%) | 0.001 |
| Aspirin + Clopidogrel + NOACs | 40 (47%) | 40 (47%) | 16 (28%) | 12 (2%) | 0.001 |
| Aspirin + Clopidogrel + LMWH | 1 (1%) | 1 (1%) | 0 (0%) | 1 (1%) | 0.001 |
| Double Antithrombotic Therapy | |||||
| Aspirin + Clopidogrel | 14 (16%) | 3 (4%) | 16 (28%) | 457 (69%) | 0.001 |
| Aspirin + Ticagrelor | 2 (2%) | 0 (0%) | 0 (0%) | 137 (21%) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raczkowska-Golanko, M.; Młodziński, K.; Raczak, G.; Gruchała, M.; Daniłowicz-Szymanowicz, L. New-Onset Atrial Fibrillation in Acute Myocardial Infarction Is a Different Phenomenon than Other Pre-Existing Types of That Arrhythmia. J. Clin. Med. 2022, 11, 4410. https://doi.org/10.3390/jcm11154410
Raczkowska-Golanko M, Młodziński K, Raczak G, Gruchała M, Daniłowicz-Szymanowicz L. New-Onset Atrial Fibrillation in Acute Myocardial Infarction Is a Different Phenomenon than Other Pre-Existing Types of That Arrhythmia. Journal of Clinical Medicine. 2022; 11(15):4410. https://doi.org/10.3390/jcm11154410
Chicago/Turabian StyleRaczkowska-Golanko, Monika, Krzysztof Młodziński, Grzegorz Raczak, Marcin Gruchała, and Ludmiła Daniłowicz-Szymanowicz. 2022. "New-Onset Atrial Fibrillation in Acute Myocardial Infarction Is a Different Phenomenon than Other Pre-Existing Types of That Arrhythmia" Journal of Clinical Medicine 11, no. 15: 4410. https://doi.org/10.3390/jcm11154410
APA StyleRaczkowska-Golanko, M., Młodziński, K., Raczak, G., Gruchała, M., & Daniłowicz-Szymanowicz, L. (2022). New-Onset Atrial Fibrillation in Acute Myocardial Infarction Is a Different Phenomenon than Other Pre-Existing Types of That Arrhythmia. Journal of Clinical Medicine, 11(15), 4410. https://doi.org/10.3390/jcm11154410