
Depression and Quality of Life in Patients with Gliomas: A Narrative Review


Abstract
:1. Introduction
2. Prevalence of Mental Disorders in Glioma
3. Diagnostic Criteria for Depression in Patients with Gliomas
4. Current Knowledge
- A.
- What are the risk factors for depression in patients with gliomas?
- B.
- Is depression a risk factor for the development of glioma?
- C.
- Is depression a prognostic factor for mortality in glioma?
- D.
- Is glioma a risk factor for depression?
- E.
- Is there a correlation between depression and glioma severity?
- F.
- How does depression affect the QoL of patients with gliomas?
- G.
- What is the relationship between antidepressants and the risk and prognosis of glioma?
5. Depression and Risk Factors in Glioma
5.1. Gender
5.2. Marital Status
5.3. Education
5.4. Tumor
5.5. Treatment
5.6. Psychiatric History
6. Depression as a Risk Factor for Glioma
7. Depression as a Prognostic Factor for Glioma Mortality
8. Glioma as a Risk Factor for Depression
9. Depression and Glioma Severity
10. Depression and QoL in Glioma
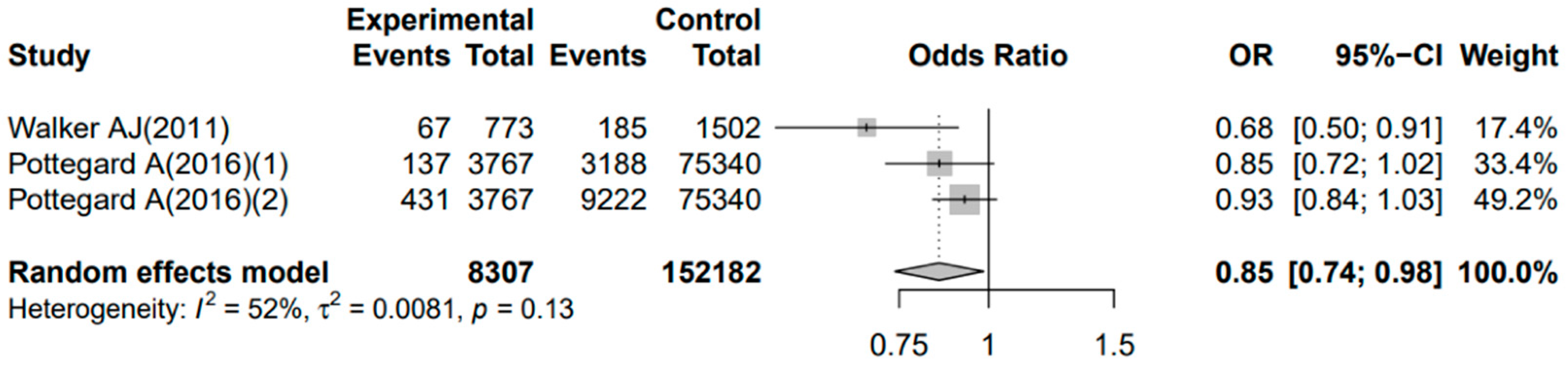
11. Antidepressants and Glioma
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, G.; Chen, G.; Zhou, Q.; Li, N.; Zheng, X. Prevalence of Mental Disorders among Older Chinese People in Tianjin City. Can. J. Psychiatry 2017, 62, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Momen, N.C.; Plana-Ripoll, O.; Agerbo, E.; Benros, M.E.; Børglum, A.D.; Christensen, M.K.; Dalsgaard, S.; Degenhardt, L.; de Jonge, P.; Debost, J.C.; et al. Association between Mental Disorders and Subsequent Medical Conditions. N. Engl. J. Med. 2020, 382, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Pine, D.S.; Holmes, E.A.; Reif, A. Anxiety disorders [published correction appears in Lancet]. Lancet 2021, 397, 914–927. [Google Scholar] [CrossRef]
- Thoma, P.; Friedmann, C.; Suchan, B. Empathy and social problem solving in alcohol dependence, mood disorders and selected personality disorders. Neurosci. Biobehav. Rev. 2013, 37, 448–470. [Google Scholar] [CrossRef]
- Okuyama, T.; Akechi, T.; Mackenzie, L.; Furukawa, T.A. Psychotherapy for depression among advanced, incurable cancer pa-tients: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 56, 16–27. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Satin, J.R.; Linden, W.; Phillips, M.J. Depression as a Predictor of Disease Progression and Mortality in Cancer Patients. Cancer 2009, 115, 5349–5361. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Cote, D.J.; Ascha, M.; Kruchko, C.; Barnholtz-Sloan, J.S. Adult Glioma Incidence and Survival by Race or Ethnicity in the United States From 2000 to 2014. JAMA Oncol. 2018, 4, 1254–1262. [Google Scholar] [CrossRef]
- Xu, S.; Tang, L.; Li, X.; Fan, F.; Liu, Z. Immunotherapy for glioma: Current management and future application. Cancer Lett. 2020, 476, 1–12. [Google Scholar] [CrossRef]
- Gilbert, M.R.; Wang, M.; Aldape, K.D.; Stupp, R.; Hegi, M.E.; Jaeckle, K.A.; Armstrong, T.S.; Wefel, J.S.; Won, M.; Blumenthal, D.T.; et al. Dose-Dense Temozolomide for Newly Diagnosed Glioblastoma: A Randomized Phase III Clinical Trial. J. Clin. Oncol. 2013, 31, 4085. [Google Scholar] [CrossRef]
- Rooney, A.G.; Carson, A.; Grant, R. Depression in Cerebral Glioma Patients: A Systematic Review of Observational Studies. Jnci-J. Natl. Cancer Inst. 2011, 103, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Bosnyák, E.; Kamson, D.O.; Behen, M.E.; Barger, G.R.; Mittal, S.; Juhász, C. Imaging cerebral tryptophan metabolism in brain tumor-associated depression. Ejnmmi Res. 2015, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rooney, A.G.; McNamara, S.; Mackinnon, M.; Fraser, M.; Rampling, R.; Carson, A.; Grant, R. Frequency, Clinical Associations, and Longitudinal Course of Major Depressive Disorder in Adults With Cerebral Glioma. J. Clin. Oncol. 2011, 29, 4307–4312. [Google Scholar] [CrossRef] [PubMed]
- Pranckeviciene, A.; Deltuva, V.P.; Tamasauskas, A.; Bunevicius, A. Association between psychological distress, subjective cognitive complaints and objective neuropsychological functioning in brain tumor patients. Clin. Neurol. Neurosurg. 2017, 163, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ryden, I.; Thurin, E.; Carstam, L.; Smits, A.; Gulati, S.; Henriksson, R.; Salvesen, Ø.; Store Jakola, A. Psychotropic and anti-epileptic drug use, before and after surgery, among patients with low-grade glioma: A nationwide matched cohort study. BMC Cancer 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Kuhnt, S.; Brahler, E.; Faller, H.; Harter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; Boehncke, A.; Hund, B.; et al. Twelve-Month and Lifetime Prevalence of Mental Disorders in Cancer Patients. Psychother. Psychosom. 2016, 85, 289–296. [Google Scholar] [CrossRef]
- Harter, M.; Reuter, K.; Aschenbrenner, A.; Schretzmann, B.; Marschner, N.; Hasenburg, A.; Weis, J. Psychiatric disorders and associated factors in cancer: Results of an interview study with patients in inpatient, rehabilitation and outpatient treatment. Eur. J. Cancer 2001, 37, 1385–1393. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef]
- Walker, J.; Hansen, C.H.; Martin, P.; Symeonides, S.; Ramessur, R.; Murray, G.; Sharpe, M. Prevalence, associations, and adequacy of treatment of major depression in patients with cancer: A cross-sectional analysis of routinely collected clinical data. Lancet Psychiatry 2014, 1, 343–350. [Google Scholar] [CrossRef]
- Song, L.; Quan, X.Y.; Su, L.; Wang, K.; Wang, H.R.; Wu, L.H.; Chen, C.Y.; Li, S.J.; Xiang, W.; Chen, L.; et al. Inflammation and behavioral symptoms in preoperational glioma patients: Is depression, anxiety, and cognitive impairment related to markers of systemic inflammation? Brain Behav. 2020, 10, e01771. [Google Scholar] [CrossRef]
- Bunevicius, A.; Deltuva, V.P.; Tamasauskas, A. Association of pre-operative depressive and anxiety symptoms with five-year survival of glioma and meningioma patients: A prospective cohort study. Oncotarget 2017, 8, 57543–57551. [Google Scholar] [CrossRef] [PubMed]
- Hao, A.P.; Huang, J.L.; Xu, X. Anxiety and depression in glioma patients: Prevalence, risk factors, and their correlation with survival. Ir. J. Med. Sci. 2021, 190, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, M.; Jiao, J.T.; Wu, Y.L.; Ouyang, T.H.; Huang, J.; Liu, S.S.; Li, C.L. Relationship between concentrations of IGF-1 and IGFBP-3 and preoperative depression risk, and effect of psychological intervention on outcomes of high-grade glioma patients with preoperative depression in a 2-year prospective study. Med. Oncol. 2014, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Piil, K.; Jakobsen, J.; Christensen, K.B.; Juhler, M.; Jarden, M. Health-related quality of life in patients with high-grade gliomas: A quantitative longitudinal study. J. Neuro-Oncol. 2015, 124, 185–195. [Google Scholar] [CrossRef]
- Kilbride, L.; Smith, G.; Grant, R. The frequency and cause of anxiety and depression amongst patients with malignant brain tumours between surgery and radiotherapy. J. Neuro-Oncol. 2007, 84, 297–304. [Google Scholar] [CrossRef]
- Battle, D.E. Diagnostic and Statistical Manual of Mental Disorders (DSM). CoDAS 2013, 25, 191–192. [Google Scholar]
- Rooney, A.G.; Brown, P.D.; Reijneveld, J.C.; Grant, R. Depression in glioma: A primer for clinicians and researchers. J. Neurol. Neurosurg. Psychiatry 2014, 85, 230–235. [Google Scholar] [CrossRef]
- Block, S.D. Psychological issues in end-of-life care. J. Palliat. Med. 2006, 9, 751–772. [Google Scholar] [CrossRef]
- Shi, C.; Lamba, N.; Zheng, L.J.; Cote, D.; Regestein, Q.R.; Liu, C.M.; Tran, Q.; Routh, S.; Smith, T.R.; Mekary, R.A.; et al. Depression and survival of glioma patients: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2018, 172, 8–19. [Google Scholar] [CrossRef]
- Katz, M.R.; Kopek, N.; Waldron, J.; Devins, G.M.; Tomlinson, G. Screening for depression in head and neck cancer. Psycho-Oncology 2004, 13, 269–280. [Google Scholar] [CrossRef]
- Rooney, A.G.; McNamara, S.; Mackinnon, M.; Fraser, M.; Rampling, R.; Carson, A.; Grant, R. Screening for major depressive disorder in adults with cerebral glioma: An initial validation of 3 self-report instruments. Neuro-Oncol. 2013, 15, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, C.L.; Goldstein, B.; Cohen, B.; Jo, M.Y.; Tallent, E.M. Clinical predictors of depression in patients with low-grade brain tumors: Consideration of a neurologic versus a psychogenic model. J. Clin. Psychol. Med. Settings 2002, 9, 97–107. [Google Scholar] [CrossRef]
- Greenberg, D.B. Barriers to the treatment of depression in cancer patients. J. Natl. Cancer Inst. Monogr. 2004, 2004, 127–135. [Google Scholar] [CrossRef]
- Ford, E.; Catt, S.; Chalmers, A.; Fallowfield, L. Systematic review of supportive care needs in patients with primary malignant brain tumors. Neuro-Oncology 2012, 14, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.D.; Forman, L.M.; Brigidi, B.D.; Carter, K.E.; Schweitzer, H.A.; Quinn, H.E.; Guill, A.B.; Herndon, J.E., 2nd; Raynor, R.H. Evaluation and characterization of generalized anxiety and depression in patients with primary brain tumors. Neuro-Oncology 2008, 10, 171–181. [Google Scholar] [CrossRef]
- Kessler, R.C.; McGonagle, K.A.; Swartz, M.; Blazer, D.G.; Nelson, C.B. Sex and depression in the National Comorbidity Survey. I: Lifetime prevalence, chronicity and recurrence. J. Affect. Disord. 1993, 29, 85–96. [Google Scholar] [CrossRef]
- Moeini, B.; Bashirian, S.; Soltanian, A.R.; Ghaleiha, A.; Taheri, M. Prevalence of depression and its associated sociodemographic factors among Iranian female adolescents in secondary schools. BMC Psychol. 2019, 7, 25. [Google Scholar] [CrossRef]
- Cutter, W.J.; Norbury, R.; Murphy, D.G. Oestrogen, brain function, and neuropsychiatric disorders. J. Neurol. Neu-Rosurgery Psychiatry 2003, 74, 837–840. [Google Scholar] [CrossRef]
- Jansson, M.; Gatz, M.; Berg, S.; Johansson, B.; Malmberg, B.; McClearn, G.E.; Schalling, M.; Pedersen, N.L. Gender differences in heritability of depressive symptoms in the elderly. Psychol. Med. 2004, 34, 471–479. [Google Scholar] [CrossRef]
- Chen, C.Y.; Wang, H.R.; Zhang, L.Y.; Wang, K.; Jiang, L.; Li, S.J.; Xiang, W.; Song, L.; Hu, S.S.; Yang, C.M.; et al. Clinical study of preoperative psychological distress and its related factors in the primary caregivers of patients with glioma. Clin. Neurol. Neurosurg. 2021, 200, 106364. [Google Scholar] [CrossRef]
- Rooney, A.G.; van Nieuwenhuizen, D.; Reijneveld, J.C.; Grant, R. Female gender is not a proven risk factor for depression in glioma. J. Neurooncol. 2009, 95, 449. [Google Scholar] [CrossRef] [PubMed]
- de Graeff, A.; de Leeuw, J.R.; Ros, W.J.; Hordijk, G.J.; Blijham, G.H.; Winnubst, J.A. Sociodemographic factors and quality of life as prognostic indicators in head and neck cancer. Eur. J. Cancer 2001, 37, 332–339. [Google Scholar] [CrossRef]
- Naseri, N.; Taleghani, F. Social Support and Depression in Iranian Cancer Patients: The Role of Demographic Variables. J. Caring Sci. 2018, 7, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Cubo, E.; Rojo, A.; Ramos, S.; Quintana, S.; Gonzalez, M.; Kompoliti, K.; Aguilar, M. The importance of educational and psychological factors in Parkinson’s disease quality of life. Eur. J. Neurol. 2002, 9, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Litofsky, N.S.; Farace, E.; Anderson, F.; Meyers, C.A., Jr.; Huang, W.; Laws, E.R., Jr.; Glioma Outcomes Project Investigators. Depression in patients with high-grade glioma: Results of the Glioma Outcomes Project. Neurosurgery 2004, 54, 358–366; discussion 66–67. [Google Scholar] [PubMed]
- Rijnen, S.J.M.; Kaya, G.; Gehring, K.; Verheul, J.B.; Wallis, O.C.; Sitskoorn, M.M.; Rutten, G.M. Cognitive functioning in patients with low-grade glioma: Effects of hemispheric tumor location and surgical procedure. J. Neurosurg. 2019, 133, 1671–1682. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Qi, F.; Song, X.P.; Di, J.; Zhang, L.C.; Zhou, Y.; Lu, X.; Chang, J.; Yu, Y.H. A prospective longitudinal evaluation of cognition and depression in postoper-ative patients with high-grade glioma following radiotherapy and chemotherapy. J. Cancer Res. Ther. 2018, 14, S1048–S1051. [Google Scholar]
- Wen, P.Y.; Kesari, S. Malignant gliomas in adults. New Engl. J. Med. 2008, 359, 492–507. [Google Scholar] [CrossRef]
- Løppenthin, K.; Johansen, C.; Larsen, M.B.; Forchhammer, B.H.; Brennum, J.; Piil, K.; Aaronson, N.; Rasmussen, B.K.; Bidstrup, P. Depressive Symptoms in Danish Patients With Glioma and a Cancer-Free Comparison Group. J. Natl. Compr. Cancer Netw. JNCCN 2020, 18, 1222–1229. [Google Scholar] [CrossRef]
- Palma, C. Tachykinins and their receptors in human malignancies. Curr. Drug Targets 2006, 7, 1043–1052. [Google Scholar] [CrossRef]
- McKenna, M.C.; Zevon, M.A.; Corn, B.; Rounds, J. Psychosocial factors and the development of breast cancer: A meta-analysis. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 1999, 18, 520–531. [Google Scholar] [CrossRef]
- Galasko, D.; Kwo-On-Yuen, P.F.; Thal, L. Intracranial mass lesions associated with late-onset psychosis and depression. Psychiatr. Clin. N. Am. 1988, 11, 151–166. [Google Scholar] [CrossRef]
- Edvardsson, T.; Påhlson, A.; Ahlstrom, G. Experiences of onset and diagnosis of low-grade glioma from the patient’s perspective. Cancer Nurs. 2006, 29, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Dawande, P.; Shukla, S.; Acharya, S. Effect of lifestyle and dietary factors in the development of brain tumors. J. Fam. Med. Prim. Care 2020, 9, 5200–5204. [Google Scholar] [CrossRef]
- Peeters, M.C.; Dirven, L.; Koekkoek, J.A.; Numans, M.E.; Taphoorn, M.J. Prediagnostic presentations of glioma in primary care: A case-control study. CNS Oncol. 2019, 8, Cns44. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M., Jr.; Schatzberg, A.F. HPA axis in major depression: Cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef]
- Giannogonas, P.; Apostolou, A.; Manousopoulou, A.; Theocharis, S.; Macari, S.A.; Psarras, S.; Garbis, S.D.; Pothoulakis, C.; Karalis, K.P. Identification of a novel interaction between corticotropin releasing hormone (Crh) and macroautophagy. Sci. Rep. 2016, 6, 23342. [Google Scholar] [CrossRef]
- Pozzoli, G.; De Simone, M.L.; Cantalupo, E.; Cenciarelli, C.; Lisi, L.; Boninsegna, A.; Dello Russo, C.; Sgambato, A.; Navarra, P. The activation of type 1 corticotropin releasing factor receptor (CRF-R1) inhibits proliferation and promotes differentiation of neuroblastoma cells in vitro via p27(Kip1) protein up-regulation and c-Myc mRNA down-regulation. Mol. Cell. Endocrinol. 2015, 412, 205–215. [Google Scholar] [CrossRef]
- Coppola, G.; Rurak, G.M.; Simard, S.; Salmaso, N. A Further Analysis and Commentary on: Profiling Changes in Cortical Astroglial Cells Following Chronic Stress. J. Exp. Neurosci. 2019, 13, 1179069519870182. [Google Scholar] [CrossRef]
- Zhang, S.; Chen, Y.; Wang, Y.; Zhang, P.; Chen, G.; Zhou, Y. Insights Into Translatomics in the Nervous System. Front. Genet. 2020, 11, 599548. [Google Scholar] [CrossRef]
- Klimaschewski, L.; Claus, P. Fibroblast Growth Factor Signalling in the Diseased Nervous System. Mol. Neurobiol. 2021, 58, 3884–3902. [Google Scholar] [CrossRef] [PubMed]
- Sacher, M.; Meixensberger, J.; Krupp, W. Interaction of quality of life, mood and depression of patients and their informal caregivers after surgical treatment of high-grade glioma: A prospective study. J. Neurooncol. 2018, 140, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Gathinji, M.; McGirt, M.J.; Attenello, F.J.; Chaichana, K.L.; Than, K.; Olivi, A.; Weingart, J.D.; Brem, H.; Quinones-Hinojosa, A. Association of preoperative depression and survival after resection of malignant brain astrocytoma. Surg. Neurol. 2009, 71, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Mainio, A.; Hakko, H.; Timonen, M.; Niemelä, A.; Koivukangas, J.; Räsänen, P. Depression in relation to survival among neurosurgical patients with a primary brain tumor: A 5-year follow-up study. Neurosurgery 2005, 56, 1234–1241; discussion 41–42. [Google Scholar] [CrossRef]
- Litofsky, N.S.; Resnick, A.G. The relationships between depression and brain tumors. J. Neurooncol. 2009, 94, 153–161. [Google Scholar] [CrossRef]
- Fox, S.W.; Lyon, D.; Farace, E. Symptom clusters in patients with high-grade glioma. J. Nurs. Scholarsh. Off. Publ. Sigma Tau Int. Honor. Soc. Nurs. 2007, 39, 61–67. [Google Scholar] [CrossRef]
- Krebber, A.M.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; de Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; van Straten, A.; Cuijpers, P.; et al. Prevalence of depression in cancer patients: A meta-analysis of diagnostic interviews and self-report instruments. Psycho-Oncology 2014, 23, 121–130. [Google Scholar] [CrossRef]
- Cheng, J.X.; Zhang, X.; Liu, B.L. Health-related quality of life in patients with high-grade glioma. Neuro-Oncol. 2009, 11, 41–50. [Google Scholar] [CrossRef]
- Yavas, C.; Zorlu, F.; Ozyigit, G.; Gurkaynak, M.; Yavas, G.; Yuce, D.; Cengiz, M.; Yildiz, F.; Akyol, F. Health-related quality of life in high-grade glioma patients: A prospective single-center study. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2012, 20, 2315–2325. [Google Scholar] [CrossRef]
- Rumalla, K.; Lin, M.; Orloff, E.; Ding, L.; Zada, G.; Mack, W.; Attenello, F. Effect of Comorbid Depression on Surgical Outcomes After Craniotomy for Malignant Brain Tumors: A Nationwide Readmission Database Analysis. World Neurosurg. 2020, 142, e458–e473. [Google Scholar] [CrossRef]
- Weitzner, M.A. Psychosocial and neuropsychiatric aspects of patients with primary brain tumors. Cancer Investig. 1999, 17, 285–291; discussion 96–97. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.; DeAngelis, L.M. Glioblastoma and Other Malignant Gliomas A Clinical Review. Jama-J. Am. Med. Assoc. 2013, 310, 1842–1850. [Google Scholar] [CrossRef] [PubMed]
- Boele, F.W.; Klein, M.; Reijneveld, J.C.; Verdonck-de Leeuw, I.M.; Heimans, J.J. Symptom management and quality of life in glioma patients. CNS Oncol. 2014, 3, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Taphoorn, M.J.; Sizoo, E.M.; Bottomley, A. Review on quality of life issues in patients with primary brain tumors. Oncologist 2010, 15, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Dufner, V.; Kessler, A.F.; Just, L.; Hau, P.; Bumes, E.; Pels, H.J.; Grauer, O.M.; Wiese, B.; Löhr, M.; Jordan, K.; et al. The Emesis Trial: Depressive Glioma Patients Are More Affected by Chemotherapy-Induced Nausea and Vomiting. Front. Neurol. 2022, 13, 773265. [Google Scholar] [CrossRef]
- Lucchiari, C.; Botturi, A.; Silvani, A.; Lamperti, E.; Gaviani, P.; Innocenti, A.; Finocchiaro, C.Y.; Masiero, M.; Pravettoni, G. Cognitive strategies and quality of life of patients with high-grade glioma. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2015, 23, 3427–3435. [Google Scholar] [CrossRef]
- Affronti, M.L.; Randazzo, D.; Lipp, E.S.; Peters, K.B.; Herndon, S.C.; Woodring, S.; Healy, P.; Cone, C.K.; Herndon, J.E., 2nd; Schneider, S.M. Pilot Study to Describe the Trajectory of Symptoms and Adaptive Strategies of Adults Living with Low-grade Glioma. Semin. Oncol. Nurs. 2018, 34, 472–485. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Wang, C.; Sun, L. The moderating role of depression on the association between posttraumatic growth and health-related quality of life in low-grade glioma patients in China. Psychol. Health Med. 2019, 24, 643–653. [Google Scholar] [CrossRef]
- Noll, K.R.; Sullaway, C.M.; Wefel, J.S. Depressive symptoms and executive function in relation to survival in patients with glioblastoma. J. Neurooncol. 2019, 142, 183–191. [Google Scholar] [CrossRef]
- Noll, K.R.; Bradshaw, M.E.; Weinberg, J.S.; Wefel, J.S. Relationships between neurocognitive functioning, mood, and quality of life in patients with temporal lobe glioma. Psycho-Oncology 2017, 26, 617–624. [Google Scholar] [CrossRef]
- Leonetti, A.; Puglisi, G.; Rossi, M.; Viganò, L.; Conti Nibali, M.; Gay, L.; Sciortino, T.; Howells, H.; Fornia, L.; Riva, M.; et al. Factors Influencing Mood Disorders and Health Related Quality of Life in Adults With Glioma: A Longitudinal Study. Front. Oncol. 2021, 11, 662039. [Google Scholar] [CrossRef] [PubMed]
- Boele, F.W.; Klein, M.; Verdonck-de Leeuw, I.M.; Cuijpers, P.; Heimans, J.J.; Snijders, T.J.; Vos, M.; Bosma, I.; Tijssen, C.C.; Reijneveld, J.C.; et al. Internet-based guided self-help for glioma patients with depressive symptoms: A randomized controlled trial. J. Neurooncol. 2018, 137, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.A.; Abrahamowicz, M.; Srasuebkul, P.; Buckley, N.A. Antidepressant therapy in cancer patients: Initiation and factors associated with treatment. Pharmacoepidemiol. Drug Saf. 2015, 24, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Gøtzsche, P.C. Our prescription drugs kill us in large numbers. Pol. Arch. Med. Wewn. 2014, 124, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.J.; Card, T.; Bates, T.E.; Muir, K. Tricyclic antidepressants and the incidence of certain cancers: A study using the GPRD. Br. J. Cancer 2011, 104, 193–197. [Google Scholar] [CrossRef]
- Pottegård, A.; García Rodríguez, L.A.; Rasmussen, L.; Damkier, P.; Friis, S.; Gaist, D. Use of tricyclic antidepressants and risk of glioma: A nationwide case-control study. Br. J. Cancer 2016, 114, 1265–1268. [Google Scholar] [CrossRef]
- Caudill, J.S.; Brown, P.D.; Cerhan, J.H.; Rummans, T.A. Selective serotonin reuptake inhibitors, glioblastoma multiforme, and impact on toxicities and overall survival: The mayo clinic experience. Am. J. Clin. Oncol. 2011, 34, 385–387. [Google Scholar] [CrossRef]
- Walker, A.J.; Grainge, M.; Bates, T.E.; Card, T.R. Survival of glioma and colorectal cancer patients using tricyclic antidepressants post-diagnosis. Cancer Causes Control 2012, 23, 1959–1964. [Google Scholar] [CrossRef]
- Otto-Meyer, S.; DeFaccio, R.; Dussold, C.; Ladomersky, E.; Zhai, L.; Lauing, K.L.; Bollu, L.R.; Amidei, C.; Lukas, R.V.; Scholtens, D.M.; et al. A retrospective survival analysis of Glioblastoma patients treated with selective serotonin reuptake inhibitors. Brain Behav. Immun. Health 2020, 2, 100025. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Potash, J.B. Carving chaos: Genetics and the classification of mood and psychotic syndromes. Harv. Rev. Psychiatry 2006, 14, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Lim, D.Y.; Chee, K.T. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020, 22, 638–639. [Google Scholar] [CrossRef] [PubMed]
- Levkovitz, Y.; Gil-Ad, I.; Zeldich, E.; Dayag, M.; Weizman, A. Differential induction of apoptosis by antidepressants in glioma and neuroblastoma cell lines: Evidence for p-c-Jun, cytochrome c, and caspase-3 involvement. J. Mol. Neurosci. 2005, 27, 29–42. [Google Scholar] [CrossRef]
- Shchors, K.; Massaras, A.; Hanahan, D. Dual Targeting of the Autophagic Regulatory Circuitry in Gliomas with Repurposed Drugs Elicits Cell-Lethal Autophagy and Therapeutic Benefit. Cancer Cell 2015, 28, 456–471. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Li, H.; Tian, Z.L.; Xu, C.J.; Liu, J.F.; Guo, Y. Disruption of NF-κB signaling by fluoxetine attenuates MGMT expression in glioma cells. OncoTargets Ther. 2015, 8, 2199–2208. [Google Scholar]
- Mugge, L.; Mansour, T.R.; Crippen, M.; Alam, Y.; Schroeder, J. Depression and glioblastoma, complicated concomitant diseases: A systemic review of published literature. Neurosurg. Rev. 2020, 43, 497–511. [Google Scholar] [CrossRef] [PubMed]
- He, J.J.; Zhang, W.H.; Liu, S.L.; Chen, Y.F.; Liao, C.X.; Shen, Q.Q.; Hu, P. Activation of β-adrenergic receptor promotes cellular proliferation in human glioblastoma. Oncol. Lett. 2017, 14, 3846–3852. [Google Scholar] [CrossRef]
- Yang, B.; Qin, J.; Nie, Y.; Li, Y.; Chen, Q. Brain-derived neurotrophic factor propeptide inhibits proliferation and induces apoptosis in C6 glioma cells. Neuroreport 2017, 28, 726–730. [Google Scholar] [CrossRef]


{kind=link}
| Author | No. of Cases (Glioma) | Mental Disorders a (%) | Depression Assessment Method | Major Depression b (%) | Minor Depression (%) | Relationship between Depression and Prognosis in Patients with Gliomas |
|---|---|---|---|---|---|---|
| Song et al. [20] | 71 | 53.5%/70.4%/32.4% (depression/anxiety/cognitive impairment) | HAMD | 53.3% | Not mentioned | Not mentioned |
| Bunevicius et al. [21] | 63 | 28%/36% (depression/anxiety) | HADS | 14% (high-grade glioma (n = 43))/11% (low-grade glioma (n = 20)) | 19% (high-grade glioma (n = 43))/ 26% (low-grade glioma (n = 20)) | No correlation between depression and the overall survival (OS) of low-grade or high-grade glioma patients (p = 0.12 and p = 0.55, respectively) |
| Hao et al. [22] | 190 | 28.4%-32.6%/36.3% (depression/anxiety) | HADS and SDS | 6.3–15.2% | 17.4–22.1% | Depression diagnosed by SDS was associated with a shorter OS (p = 0.016), while depression diagnosed by HADS was not associated with a shorter OS (p = 0.086) |
| Wang et al. [23] | 249 | 46% (depression) | HADS | Not mentioned | Not mentioned | Depression may correlate with QoL and outcomes of patients c |
| Piil et al. [24] | 30 | 26.7% (depression) | HADS | Not mentioned | Not mentioned | Not mentioned |
| Rooney et al. [13] | 155 | 20.6% ± 6.4% (major depressive disorder) | HAD-D | 20.6% ± 6.4% | Not mentioned | Not mentioned |
| Kilbride et al. [25] | 51 | 13–22% | HADS | 6% | Not mentioned | Not mentioned |
| Author | Year | Country | Antidepressants | OR (95% CI) (Adjusted)/HR (95% CI) (Adjusted) a | Name of Drugs or Source of Drugs |
|---|---|---|---|---|---|
| Walker AJ [85] | 2011 | UK | TCAs | 0.59 (0.42–0.81) | Section 4.3.3 of the British National Formulary (BNF) |
| Pottegård A [86] | 2016 | Denmark | TCAs/SSRI | TCAs: 0.89 (0.75–1.06) SSRI: 0.95 (0.86–1.06) | No specific description |
| Caudill JS [87] | 2011 | America | SSRI | 0.65 (0.41–0.99) | Escitalopram, Fluoxetine, Fluvoxamine, Paroxetine, or Sertraline |
| Walker AJ [88] | 2012 | UK | TCAs | 0.83 (0.53–1.30) | Section 4.3.3 of the British National Formulary (BNF) |
| Otto-Meyer S [89] | 2019 | America | SSRI | 1.27 (0.98–1.64) | Escitalopram, Fluoxetine, Fluvoxamine, Paroxetine, or Sertraline |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Deng, F.; Zhang, L.; Hu, K.; Liu, S.; Zhong, S.; Yang, J.; Zeng, X.; Peng, X. Depression and Quality of Life in Patients with Gliomas: A Narrative Review. J. Clin. Med. 2022, 11, 4811. https://doi.org/10.3390/jcm11164811
Hu Y, Deng F, Zhang L, Hu K, Liu S, Zhong S, Yang J, Zeng X, Peng X. Depression and Quality of Life in Patients with Gliomas: A Narrative Review. Journal of Clinical Medicine. 2022; 11(16):4811. https://doi.org/10.3390/jcm11164811
Chicago/Turabian StyleHu, Yue, Fang Deng, Lupeng Zhang, Keyue Hu, Shiqi Liu, Suye Zhong, Jun Yang, Xiaomin Zeng, and Xiaoning Peng. 2022. "Depression and Quality of Life in Patients with Gliomas: A Narrative Review" Journal of Clinical Medicine 11, no. 16: 4811. https://doi.org/10.3390/jcm11164811
APA StyleHu, Y., Deng, F., Zhang, L., Hu, K., Liu, S., Zhong, S., Yang, J., Zeng, X., & Peng, X. (2022). Depression and Quality of Life in Patients with Gliomas: A Narrative Review. Journal of Clinical Medicine, 11(16), 4811. https://doi.org/10.3390/jcm11164811