
Gentle Touch Therapy, Pain Relief and Neuroplasticity at Baseline in Fibromyalgia Syndrome: A Randomized, Multicenter Trial with Six-Month Follow-Up

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
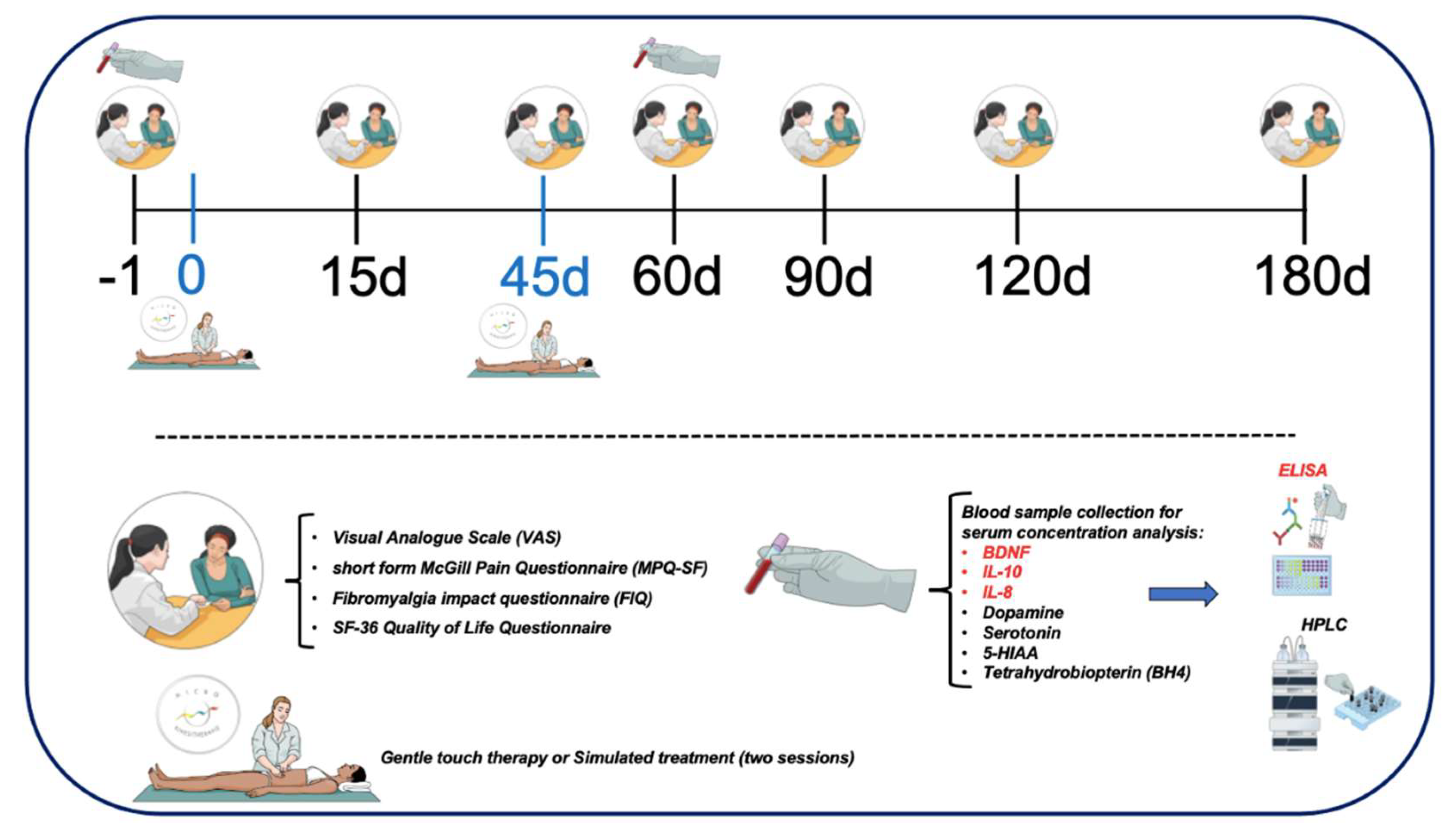
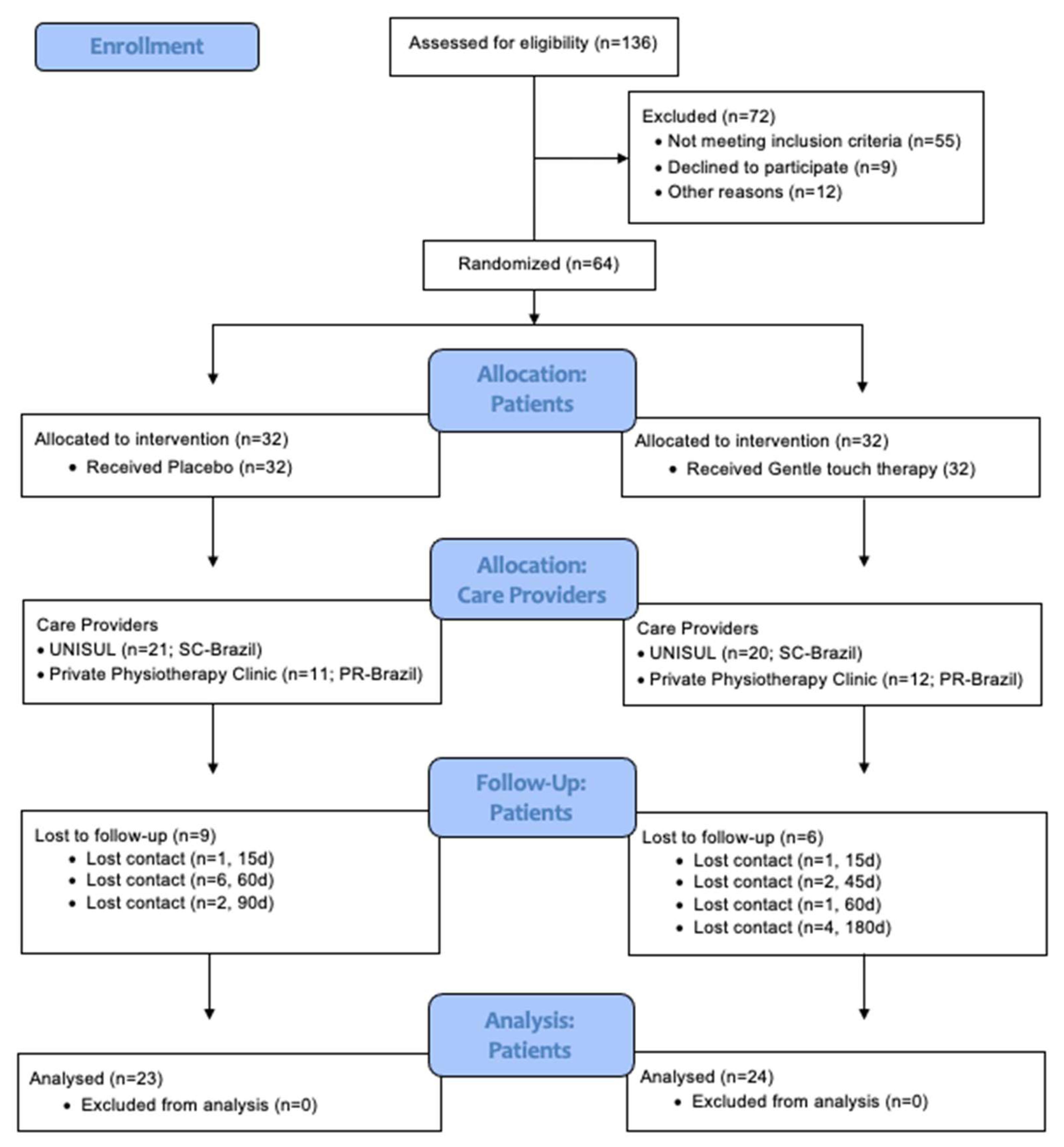
2.1. Study Design and Eligibility
2.2. Inclusion and Exclusion Criteria
2.3. Sample Size Justification
2.4. Randomization
2.5. Blinding
2.6. Intervention
2.7. Instruments and Assessments
2.7.1. Primary Outcome Measures
VAS for Pain
2.8. Secondary Outcome Measures
2.8.1. Short-Form McGill Pain Questionnaire (MPQ-SF)
2.8.2. FIQ
2.8.3. SF-36 Quality of Life Questionnaire
2.9. Blood Samples
2.10. Serum Immune-Inflammatory Biomarkers Level
2.11. Measurements of Neurotransmitters Levels
2.12. Measurements of BH4 Levels
2.13. Statistical Analysis
3. Results
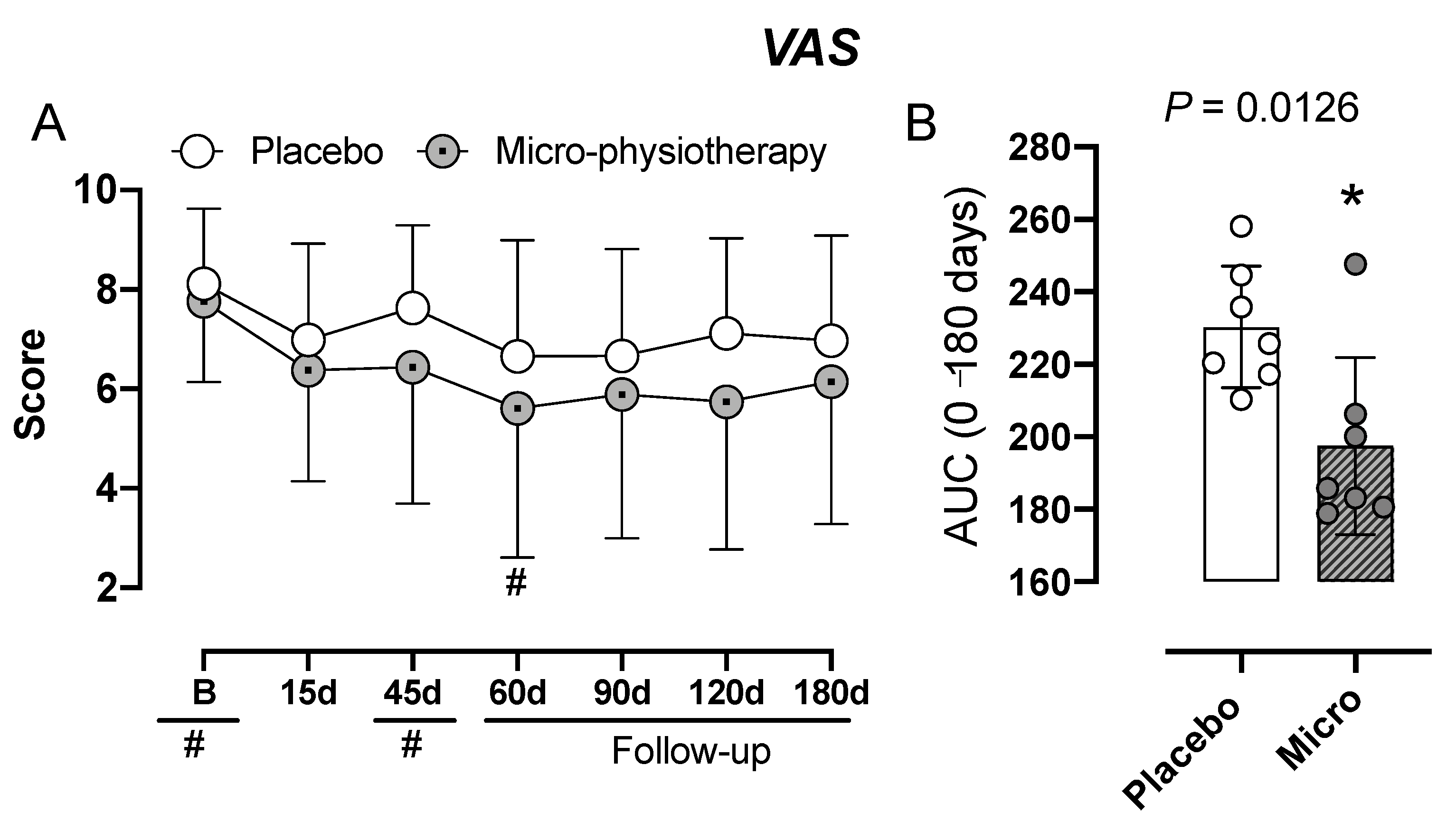
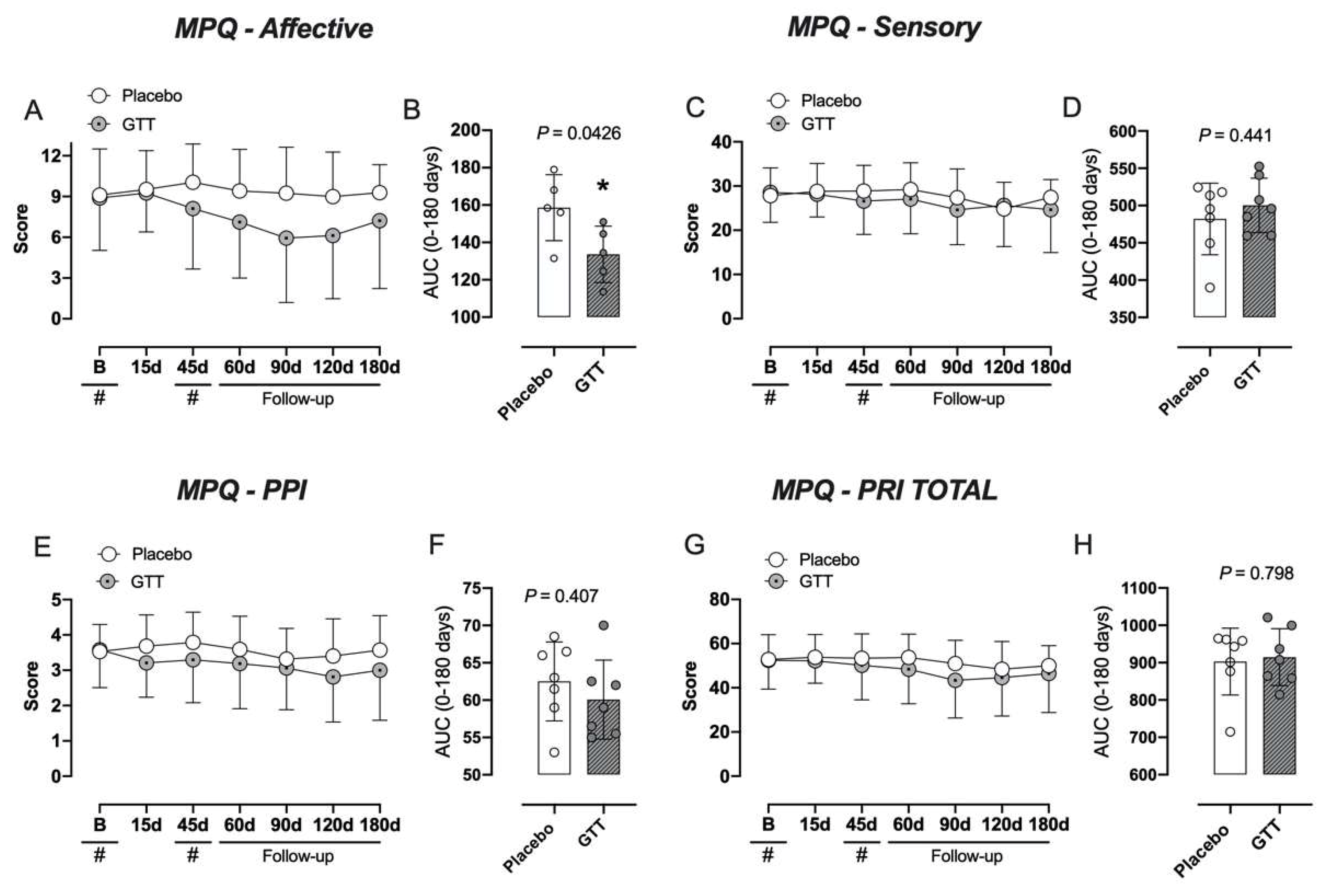
3.1. Assessment of Pain: VAS and McGill-SF Questionnaire
3.2. Assessment of Quality of Life: FIQ and SF-36 Questionnaires
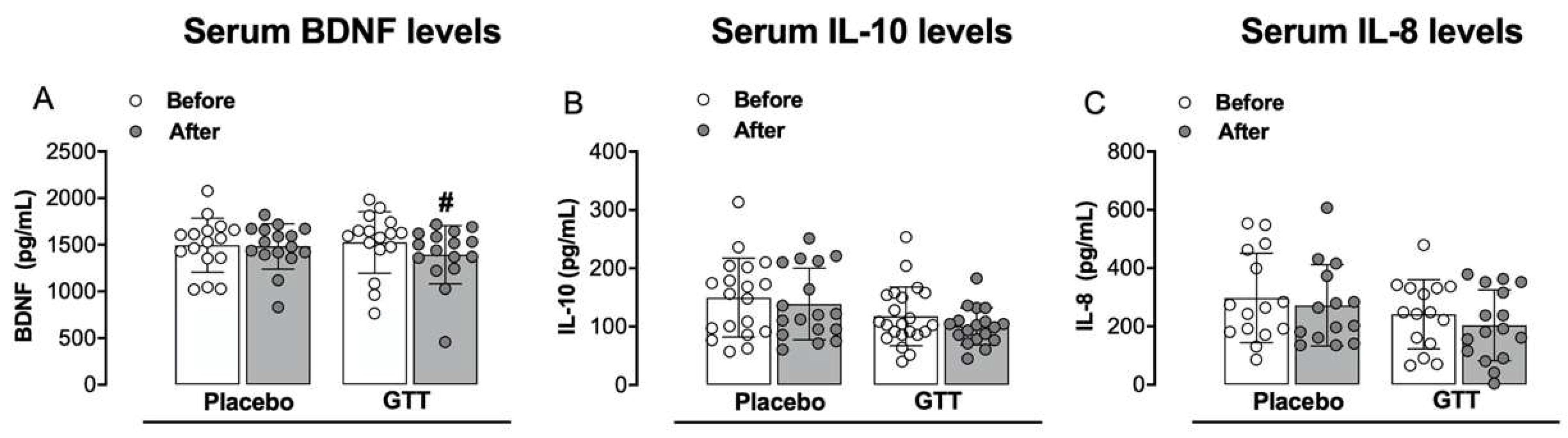
3.3. Assessment of Inflammatory Mediators: Serum Neurotrophic Factor and Cytokines Levels
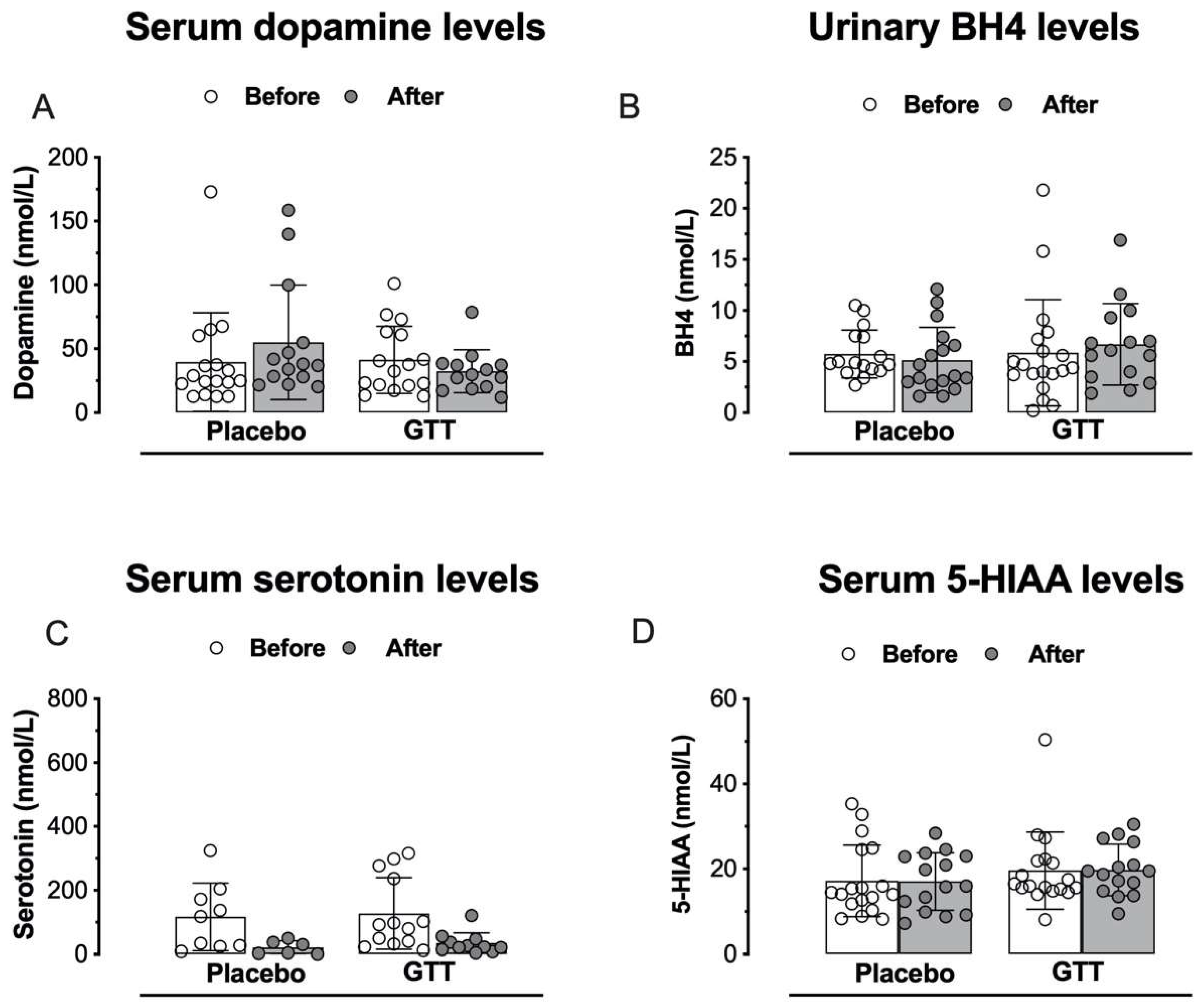
3.4. Assessment of Neurotransmitters or Neuromodulators: Serum Catecholamines, Monoamines and BH4 Levels
3.5. GTT, Pain Relief and Neuroplasticity at Baseline in FM Syndrome: Exploratory Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feliu-Soler, A.; Montesinos, F.; Gutiérrez-Martínez, O.; Scott, W.; McCracken, L.M.; Luciano, J.V. Current status of acceptance and commitment therapy for chronic pain: A narrative review. J. Pain Res. 2018, 11, 2145–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.B.; Maixner, D.W.; Fillingim, R.B.; Slade, G.; Gracely, R.H.; Ambrose, K.; Zaykin, D.V.; Hyde, C.; John, S.; Tan, K.; et al. Large candidate gene association study reveals genetic risk factors and therapeutic targets for fibromyalgia. Arthritis Rheum. 2011, 64, 584–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borchers, A.T.; Gershwin, M.E. Fibromyalgia: A Critical and Comprehensive Review. Clin. Rev. Allergy Immunol. 2015, 49, 100–151. [Google Scholar] [CrossRef] [PubMed]
- Illescas-Montes, R.; Costela-Ruiz, V.J.; Melguizo-Rodríguez, L.; De Luna-Bertos, E.; Ruiz, C.; Ramos-Torrecillas, J. Application of Salivary Biomarkers in the Diagnosis of Fibromyalgia. Diagnostics 2021, 11, 63. [Google Scholar] [CrossRef]
- Becker, S.; Schweinhardt, P. Dysfunctional Neurotransmitter Systems in Fibromyalgia, Their Role in Central Stress Circuitry and Pharmacological Actions on These Systems. Pain Res. Treat. 2011, 2012, 741746. [Google Scholar] [CrossRef]
- Martins, D.F.; Viseux, F.J.; Salm, D.C.; Ribeiro, A.C.A.; da Silva, H.K.L.; Seim, L.A.; Bittencourt, E.B.; Bianco, G.; Moré, A.O.O.; Reed, W.R.; et al. The role of the vagus nerve in fibromyalgia syndrome. Neurosci. Biobehav. Rev. 2021, 131, 1136–1149. [Google Scholar] [CrossRef]
- Ángel García, D.; Martínez Nicolás, I.; Saturno Hernández, P.J. Clinical approach to fibromyalgia: Synthesis of Evidence-based recommendations, a systematic review. Reumatol. Clin. 2016, 12, 65–71. [Google Scholar] [CrossRef]
- Matsushita, K.; Masuda, A.; Tei, C. Efficacy of Waon Therapy for Fibromyalgia. Intern. Med. 2008, 47, 1473–1476. [Google Scholar] [CrossRef] [Green Version]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.-A.; Rice, A.S.C.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef]
- Legangneux, E.; Mora, J.J.; Spreux-Varoquaux, O.; Thorin, I.; Herrou, M.; Alvado, G.; Gomeni, C. Cerebrospinal fluid biogenic amine metabolites, plasma-rich platelet serotonin and [3H]imipramine reuptake in the primary fibromyalgia syndrome. Rheumatology 2001, 40, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Light, K.C.; Bragdon, E.E.; Grewen, K.M.; Brownley, K.A.; Girdler, S.S.; Maixner, W. Adrenergic Dysregulation and Pain with and without Acute Beta-Blockade in Women with Fibromyalgia and Temporomandibular Disorder. J. Pain 2009, 10, 542–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julien, N.; Goffaux, P.; Arsenault, P.; Marchand, S. Widespread pain in fibromyalgia is related to a deficit of endogenous pain inhibition. Pain 2005, 114, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Wood, P.B.; Holman, A.J. An Elephant among Us: The Role of Dopamine in the Pathophysiology of Fibromyalgia. J. Rheumatol. 2009, 36, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Wood, P.B.; Patterson, J.C., II; Sunderland, J.J.; Tainter, K.H.; Glabus, M.F.; Lilien, D.L. Reduced Presynaptic Dopamine Activity in Fibromyalgia Syndrome Demonstrated with Positron Emission Tomography: A Pilot Study. J. Pain 2007, 8, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Maletic, V. Neurobiology of depression, fibromyalgia and neuropathic pain. Front. Biosci. 2009, 14, 5291–5338. [Google Scholar] [CrossRef]
- Kosek, E.; Hansson, P. Modulatory influence on somatosensory perception from vibration and heterotopic noxious conditioning stimulation (HNCS) in fibromyalgia patients and healthy subjects. Pain 1997, 70, 41–51. [Google Scholar] [CrossRef]
- Zanette, S.A.; Dussan-Sarria, J.A.; Souza, A.; Deitos, A.; Torres, I.L.S.; Caumo, W. Higher Serum S100B and BDNF Levels are Correlated with a Lower Pressure-Pain Threshold in Fibromyalgia. Mol. Pain 2014, 10, 46. [Google Scholar] [CrossRef] [Green Version]
- Caumo, W.; Deitos, A.; Carvalho, S.; Leite, J.; Carvalho, F.; Dussan-Sarria, J.; Tarragó, M.D.G.L.; Souza, A.; Torres, I.L.; Fregni, F. Motor Cortex Excitability and BDNF Levels in Chronic Musculoskeletal Pain According to Structural Pathology. Front. Hum. Neurosci. 2016, 10, 357. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Cervero, F.; De Koninck, Y. Role of Cation-Chloride-Cotransporters (CCC) in Pain and Hyperalgesia. Curr. Top. Med. Chem. 2005, 5, 547–555. [Google Scholar] [CrossRef]
- Price, T.J.; Cervero, F.; Gold, M.S.; Hammond, D.L.; Prescott, S.A. Chloride regulation in the pain pathway. Brain Res. Rev. 2009, 60, 149–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coull, J.A.M.; Beggs, S.; Boudreau, D.; Boivin, D.; Tsuda, M.; Inoue, K.; Gravel, C.; Salter, M.W.; De Koninck, Y. BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature 2005, 438, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Scholz, J.; Woolf, C.J. The neuropathic pain triad: Neurons, immune cells and glia. Nat. Neurosci. 2007, 10, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Basbaum, A.I.; Bautista, D.M.; Scherrer, G.; Julius, D. Cellular and Molecular Mechanisms of Pain. Cell 2009, 139, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Chavan, S.S.; Pavlov, V.A.; Tracey, K.J. Mechanisms and Therapeutic Relevance of Neuro-immune Communication. Immunity 2017, 46, 927–942. [Google Scholar] [CrossRef] [Green Version]
- Andrés-Rodríguez, L.; Borràs, X.; Feliu-Soler, A.; Pérez-Aranda, A.; Rozadilla-Sacanell, A.; Montero-Marin, J.; Maes, M.; Luciano, J.V. Immune-inflammatory pathways and clinical changes in fibromyalgia patients treated with Mindfulness-Based Stress Reduction (MBSR): A randomized, controlled clinical trial. Brain Behav. Immun. 2019, 80, 109–119. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef]
- Üçeyler, N.; Sommer, C. Cytokine regulation in animal models of neuropathic pain and in human diseases. Neurosci. Lett. 2008, 437, 194–198. [Google Scholar] [CrossRef]
- Bote, M.E.; Garcia, J.; Hinchado, M.D.; Ortega, E. Fibromyalgia: Anti-Inflammatory and Stress Responses after Acute Moderate Exercise. PLoS ONE 2013, 8, e74524. [Google Scholar] [CrossRef]
- Clauw, D.J. Fibromyalgia and Related Conditions. Mayo Clin. Proc. 2015, 90, 680–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendieta, D.; De la Cruz-Aguilera, D.L.; Barrera-Villalpando, M.I.; Becerril-Villanueva, E.; Arreola, R.; Hernández-Ferreira, E.; Pérez-Tapia, S.M.; Pérez-Sánchez, G.; Garcés-Alvarez, M.E.; Aguirre-Cruz, L.; et al. IL-8 and IL-6 primarily mediate the inflammatory response in fibromyalgia patients. J. Neuroimmunol. 2016, 290, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Cunha, F.; Lorenzetti, B.; Poole, S.; Ferreira, S. Interleukin-8 as a mediator of sympathetic pain. J. Cereb. Blood Flow Metab. 1991, 104, 765–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, D.J.; Linker-Israeli, M.; Hallegua, D.; Silverman, S.; Silver, D.; Weisman, M.H. Cytokines play an aetiopathogenetic role in fibromyalgia: A hypothesis and pilot study. Rheumatology 2001, 40, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Üçeyler, N.; Häuser, W.; Sommer, C. Systematic review with meta-analysis: Cytokines in fibromyalgia syndrome. BMC Musculoskelet. Disord. 2011, 12, 245. [Google Scholar] [CrossRef] [Green Version]
- Werner, E.R.; Blau, N.; Thöny, B. Tetrahydrobiopterin: Biochemistry and pathophysiology. Biochem. J. 2011, 438, 397–414. [Google Scholar] [CrossRef] [Green Version]
- Pires, A.C.S.; Tan, V.; Heng, R.B.; Guillemin, G.J.; Latini, A. Kynurenine and Tetrahydrobiopterin Pathways Crosstalk in Pain Hypersensitivity. Front. Neurosci. 2020, 14, 620. [Google Scholar] [CrossRef]
- Latremoliere, A.; Latini, A.; Andrews, N.; Cronin, S.J.; Fujita, M.; Gorska, K.; Hovius, R.; Romero, C.; Chuaiphichai, S.; Painter, M.; et al. Reduction of Neuropathic and Inflammatory Pain through Inhibition of the Tetrahydrobiopterin Pathway. Neuron 2015, 86, 1393–1406. [Google Scholar] [CrossRef] [Green Version]
- Tegeder, I.; Costigan, M.; Griffin, R.S.; Abele, A.; Belfer, I.; Schmidt, H.; Ehnert, C.; Nejim, J.; Marian, C.; Scholz, J.; et al. GTP cyclohydrolase and tetrahydrobiopterin regulate pain sensitivity and persistence. Nat. Med. 2006, 12, 1269–1277. [Google Scholar] [CrossRef]
- Kim, S.-K.; Nah, S.-S.; Lee, J.H.; Hong, S.-J.; Kim, H.-S.; Lee, H.-S.; Kim, H.A.; Joung, C.-I.; Bae, J.; Choe, J.-Y.; et al. Association of Guanosine Triphosphate Cyclohydrolase 1 Gene Polymorphisms with Fibromyalgia Syndrome in a Korean Population. J. Rheumatol. 2013, 40, 316–322. [Google Scholar] [CrossRef]
- Russo, M.A.; Georgius, P.; Pires, A.S.; Heng, B.; Allwright, M.; Guennewig, B.; Santarelli, D.M.; Bailey, D.; Fiore, N.T.; Tan, V.X.; et al. Novel immune biomarkers in complex regional pain syndrome. J. Neuroimmunol. 2020, 347, 577330. [Google Scholar] [CrossRef] [PubMed]
- Staats Pires, A.; Heng, B.; Tan, V.X.; Latini, A.; Russo, M.A.; Santarelli, D.M.; Bailey, D.; Wynne, K.; O’Brien, J.A.; Guillemin, G.J.; et al. Kynurenine, Tetrahydrobiopterin, and Cytokine Inflammatory Biomarkers in Individuals Affected by Diabetic Neuropathic Pain. Front. Neurosci. 2020, 14, 890. [Google Scholar] [CrossRef] [PubMed]
- Kamonseki, D.H.; Christenson, P.; Rezvanifar, S.C.; Calixtre, L.B. Effects of manual therapy on fear avoidance, kinesiophobia and pain catastrophizing in individuals with chronic musculoskeletal pain: Systematic review and meta-analysis. Musculoskelet. Sci. Pract. 2020, 51, 102311. [Google Scholar] [CrossRef] [PubMed]
- Cumplido-Trasmonte, C.; Fernández-González, P.; Alguacil-Diego, I.; Molina-Rueda, F. Manual therapy in adults with tension-type headache: A systematic review. Neurologia 2020, 36, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Martins, D.F.; Mazzardo-Martins, L.; Gadotti, V.M.; Nascimento, F.P.; Lima, D.A.; Speckhann, B.; Favretto, G.A.; Bobinski, F.; Cargnin-Ferreira, E.; Bressan, E.; et al. Ankle joint mobilization reduces axonotmesis-induced neuropathic pain and glial activation in the spinal cord and enhances nerve regeneration in rats. Pain 2011, 152, 2653–2661. [Google Scholar] [CrossRef]
- Martins, D.F.; Bobinski, F.; Martins, L.M.; Cidral-Filho, F.J.; Nascimento, F.P.; Gadotti, V.M.; Santos, A.R.S. Ankle Joint Mobilization Decreases Hypersensitivity by Activation of Peripheral Opioid Receptors in a Mouse Model of Postoperative Pain. Pain Med. 2012, 13, 1049–1058. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.F.; Mazzardo-Martins, L.; Cidral-Filho, F.J.; Stramosk, J.; Santos, A.R. Ankle joint mobilization affects postoperative pain through peripheral and central adenosine A1 receptors. Phys. Ther. 2013, 93, 401–412. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.; Mazzardo-Martins, L.; Cidral-Filho, F.; Gadotti, V.; Santos, A. Peripheral and spinal activation of cannabinoid receptors by joint mobilization alleviates postoperative pain in mice. Neuroscience 2013, 255, 110–121. [Google Scholar] [CrossRef]
- Salgado, A.S.I.; Stramosk, J.; Ludtke, D.D.; Kuci, A.C.C.; Salm, D.C.; Ceci, L.A.; Petronilho, F.; Florentino, D.; Danielski, L.G.; Gassenferth, A.; et al. Manual Therapy Reduces Pain Behavior and Oxidative Stress in a Murine Model of Complex Regional Pain Syndrome Type I. Brain Sci. 2019, 9, 197. [Google Scholar] [CrossRef] [Green Version]
- Ruffini, N.; D’Alessandro, G.; Mariani, N.; Pollastrelli, A.; Cardinali, L.; Cerritelli, F. Variations of high frequency parameter of heart rate variability following osteopathic manipulative treatment in healthy subjects compared to control group and sham therapy: Randomized controlled trial. Front. Neurosci. 2015, 9, 272. [Google Scholar] [CrossRef] [Green Version]
- Pereira, A.P.; Carvalho, E.M.D.S.; Kerppers, I.I.; Furmann, M.; Pires, J.A.W.; Ribeiro, L.G.; Rolão, M.P.P.; Salgado, A.S.I. Assessment of Heart Rate Variability in Fibromyalgia after Micro-physiotherapy. Man. Ther. Posturol. Rehabil. J. 2014, 12, 189. [Google Scholar] [CrossRef]
- Grosjean, D.; Salgado, A.; Parreira, R.; Ceci, L.A.; Carraro, E.; Hosni, A.P.; Miri, A.L.; Camargo, J.; Gomes; Kerppers, I.I. A New Approach t Manual Therapy for the Immune System: An Experimental Study. IJSRM 2017, 8, 137–148. [Google Scholar]
- Baconnier, P.; Vial, B.; Vaudaux, G.; Vaudaux, G.F.; Maindet-Dominici, C.; Poquin, D.; Juvin, R. Evaluation of the clinical effectiveness of microkinesitherapy in post-traumatic cervi-calgia. A randomized, double-blinded clinical trial. Man. Ther. Posturology Rehabil. J. 2016, 14, 1–6. [Google Scholar] [CrossRef]
- Grosjean, D.; Benini, P.; Carayon, P. Managing irritable bowel syndrome: The impact of micro-physiotherapy. J. Complement. Integr. Med. 2017, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P.; For The CONSORT NPT Group. CONSORT Statement for Randomized Trials of Nonpharmacologic Treatments: A 2017 Update and a CONSORT Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 2013, MR000030. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Silva, F.C.; Deliberato, P.C.P. Analysis of pain scales: Literature review. Rev. Bras. Scien. Health 2009, 19, 86–89. [Google Scholar]
- Pimenta, C.A.M.; Teixeira, M.J. McGill pain questionnaire: Adaptation proposal for the Portuguese language. Rev. Esc. Enferm. USP 1996, 30, 3. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.P.; Santos, A.M.B.; Assumpção, A.; Matsutani, L.A.; Lage, L.V.; Pereira, C.A.B. Validação da versão brasileira do fibromyalgia impact questionnaire (FIQ). Rev. Bras. Reumatol. 2006, 46, 24–31. [Google Scholar] [CrossRef]
- Ciconelli, R.; Ferraz, M.; Santos, W.; Meinao, I.; Quaresma, M. Brazilian-Portuguese version of the SF-36. A reliable and valid quality of life outcome measure. Rev. Bras. Reumatol. 1999, 39, 143–150. [Google Scholar]
- Brüggemann, A.K.; Mello, C.L.; Dal Pont, T.; Kunzler, D.H.; Martins, D.F.; Bobinski, F.; Yamaguti, W.P.; Paulin, E. Effects of Neuromuscular Electrical Stimulation During Hemodialysis on Pe-ripheral Muscle Strength and Exercise Capacity: A Randomized Clinical Trial. Arch. Phys. Med. Rehabil. 2017, 98, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Quialheiro, A.; Bobinski, F.; Haefliger, J.D.G.; Del Antonio, R.; Lins, E.F.; Martins, D.F.; D’Orsi, E.; Xavier, A.J.; Peres, M.A. A comprehensive program of cognitive stimulation with digital inclusion, physical activity and social interaction can modify BDNF levels and improve cognition in adults over 50: A randomized controlled pilot study. Aging Ment. Health 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Scheffer, D.D.L.; Ghisoni, K.; Aguiar, A.S., Jr.; Latini, A. Moderate running exercise prevents excessive immune system activation. Physiol. Behav. 2019, 204, 248–255. [Google Scholar] [CrossRef]
- Cronin, S.J.F.; Seehus, C.; Weidinger, A.; Talbot, S.; Reissig, S.; Seifert, M.; Pierson, Y.; McNeill, E.; Longhi, M.S.; Turnes, B.L.; et al. The metabolite BH4 controls T cell proliferation in autoimmunity and cancer. Nature 2018, 563, 7732. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Perrot, S.; Fitzcharles, M.-A. Management of fibromyalgia: Practical guides from recent evidence-based guidelines. Pol. Arch. Intern. Med. 2017, 127, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, D.A.; Holmes, D. Discipline, desire, and transgression in physiotherapy practice. Physiother. Theory Pract. 2012, 28, 454–465. [Google Scholar] [CrossRef]
- Rutberg, S.; Kostenius, C.; Öhrling, K. Professional tools and a personal touch–experiences of physical therapy of persons with migraine. Disabil. Rehabil. 2013, 35, 1614–1621. [Google Scholar] [CrossRef] [Green Version]
- Zusman, M. There’s something about passive movement. Med. Hypotheses 2010, 75, 106–110. [Google Scholar] [CrossRef]
- Geri, T.; Viceconti, A.; Minacci, M.; Testa, M.; Rossettini, G. Manual therapy: Exploiting the role of human touch. Musculoskelet. Sci. Pract. 2019, 44, 102044. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Beneciuk, J.M.; Bishop, M.D.; Coronado, R.A.; Penza, C.W.; Simon, C.B.; George, S.Z. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J. Orthop. Sports Phys. Ther. 2018, 48, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Rossettini, G.; Carlino, E.; Testa, M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet. Disord. 2018, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Dur, Ş.; Çağlar, S.; Yıldız, N.U.; Doğan, P.; Varal, I.G. The effect of Yakson and Gentle Human Touch methods on pain and physiological parameters in preterm infants during heel lancing. Intensiv. Crit. Care Nurs. 2020, 61, 102886. [Google Scholar] [CrossRef] [PubMed]
- Weze, C.; Leathard, H.L.; Grange, J.; Tiplady, P.; Stevens, G. Evaluation of healing by gentle touch in 35 clients with cancer. Eur. J. Oncol. Nurs. 2004, 8, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Olausson, H.; Wessberg, J.; Morrison, I.; McGlone, F.; Vallbo, Å. The neurophysiology of unmyelinated tactile afferents. Neurosci. Biobehav. Rev. 2010, 34, 185–191. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel–now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Čeko, M.; Seminowicz, D.; Bushnell, M.C.; Olausson, H.W. Anatomical and Functional Enhancements of the Insula after Loss of Large Primary Somatosensory Fibers. Cereb. Cortex 2012, 23, 2017–2024. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef]
- Craig, A.D. A new view of pain as a homeostatic emotion. Trends Neurosci. 2003, 26, 303–307. [Google Scholar] [CrossRef]
- Brietzke, A.P.; Zortea, M.; Carvalho, F.; Sanches, P.R.; Silva, D.P.J.; Torres, I.L.D.S.; Fregni, F.; Caumo, W. Large Treatment Effect with Extended Home-Based Transcranial Direct Current Stimulation over Dorsolateral Prefrontal Cortex in Fibromyalgia: A Proof of Concept Sham-Randomized Clinical Study. J. Pain 2020, 21, 212–224. [Google Scholar] [CrossRef]
- Villamar, M.F.; Wivatvongvana, P.; Patumanond, J.; Bikson, M.; Truong, D.Q.; Datta, A.; Fregni, F. Focal Modulation of the Primary Motor Cortex in Fibromyalgia Using 4×1-Ring High-Definition Transcranial Direct Current Stimulation (HD-tDCS): Immediate and Delayed Analgesic Effects of Cathodal and Anodal Stimulation. J. Pain 2013, 14, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Deitos, A.; Dussán-Sarria, J.A.; de Souza, A.; Medeiros, L.; Tarragô, M.D.G.; Sehn, F.; Chassot, M.; Zanette, S.; Schwertner, A.; Fregni, F.; et al. Clinical Value of Serum Neuroplasticity Mediators in Identifying the Central Sensitivity Syndrome in Patients with Chronic Pain with and without Structural Pathology. Clin. J. Pain 2015, 31, 959–967. [Google Scholar] [CrossRef]
- Haas, L.; Portela, L.V.C.; Böhmer, A.E.; Oses, J.P.; Lara, D.R. Increased Plasma Levels of Brain Derived Neurotrophic Factor (BDNF) in Patients with Fibromyalgia. Neurochem. Res. 2010, 35, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Ranzolin, A.; Duarte, A.L.B.P.; Bredemeier, M.; Neto, C.A.D.C.; Ascoli, B.M.; Wollenhaupt-Aguiar, B.; Kapczinski, F.; Xavier, R.M. Evaluation of cytokines, oxidative stress markers and brain-derived neurotrophic factor in patients with fibromyalgia—A controlled cross-sectional study. Cytokine 2016, 84, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Montero-Marin, J.; Andrés-Rodríguez, L.; Tops, M.; Luciano, J.V.; Navarro-Gil, M.; Feliu-Soler, A.; López-Del-Hoyo, Y.; Garcia-Campayo, J. Effects of attachment-based compassion therapy (ABCT) on brain-derived neurotrophic factor and low-grade inflammation among fibromyalgia patients: A randomized controlled trial. Sci. Rep. 2019, 9, 15639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannion, R.J.; Costigan, M.; Decosterd, I.; Amaya, F.; Ma, Q.-P.; Holstege, J.C.; Ji, R.-R.; Acheson, A.; Lindsay, R.M.; Wilkinson, G.A.; et al. Neurotrophins: Peripherally and centrally acting modulators of tactile stimulus-induced inflammatory pain hypersensitivity. Proc. Natl. Acad. Sci. USA 1999, 96, 9385–9390. [Google Scholar] [CrossRef] [Green Version]
- Habig, K.; Schaenzer, A.; Schirner, W.; Lautenschlaeger, G.; Dassinger, B.; Olausson, H.; Birklein, F.; Gizewski, E.R.; Kraemer, H.H. Low threshold unmyelinated mechanoafferents can modulate pain. BMC Neurol. 2017, 17, 184. [Google Scholar] [CrossRef] [Green Version]
- Case, L.K.; Čeko, M.; Gracely, J.L.; Richards, E.A.; Olausson, H.; Bushnell, M.C. Touch Perception Altered by Chronic Pain and by Opioid Blockade. eNeuro 2016, 3, ENEURO.0138-15.2016. [Google Scholar] [CrossRef]
- Apfel, S.C.; Wright, U.E.; Wiideman, A.M.; Dormia, C.; Snider, W.D.; Kessler, J.A. Nerve Growth Factor Regulates the Expression of Brain-Derived Neurotrophic Factor mRNA in the Peripheral Nervous System. Mol. Cell. Neurosci. 1996, 7, 134–142. [Google Scholar] [CrossRef]
- Yan, Q.; Rosenfeld, R.; Matheson, C.; Hawkins, N.; Lopez, O.; Bennett, L.; Welcher, A. Expression of brain-derived neurotrophic factor protein in the adult rat central nervous system. Neuroscience 1997, 78, 431–448. [Google Scholar] [CrossRef]
- Zhou, X.-F.; Rush, R. Endogenous brain-derived neurotrophic factor is anterogradely transported in primary sensory neurons. Neuroscience 1996, 74, 945–951. [Google Scholar] [CrossRef]
- Michael, G.J.; Averill, S.; Nitkunan, A.; Rattray, M.; Bennett, D.; Yan, Q.; Priestley, J.V. Nerve Growth Factor Treatment Increases Brain-Derived Neurotrophic Factor Selectively in TrkA-Expressing Dorsal Root Ganglion Cells and in Their Central Terminations within the Spinal Cord. J. Neurosci. 1997, 17, 8476–8490. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Evidence for a central component of post-injury pain hypersensitivity. Nature 1983, 306, 686–688. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.; Nash, T.; Iannetti, G.D.; Haggard, P. Pain relief by touch: A quantitative approach. Pain 2014, 155, 635–642. [Google Scholar] [CrossRef] [Green Version]
- Krahé, C.; Drabek, M.M.; Paloyelis, Y.; Fotopoulou, A. Affective touch and attachment style modulate pain: A laser-evoked potentials study. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20160009. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Pintó, I.; Agmon-Levin, N.; Howard, A.; Shoenfeld, Y. Fibromyalgia and cytokines. Immunol. Lett. 2014, 161, 200–203. [Google Scholar] [CrossRef]
- Theoharides, T.C.; Tsilioni, I.; Arbetman, L.; Panagiotidou, S.; Stewart, J.M.; Gleason, R.M.; Russell, I.J. Fibromyalgia Syndrome in Need of Effective Treatments. J. Pharmacol. Exp. Ther. 2015, 355, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Littlejohn, G.O. Neurogenic neuroinflammation in fibromyalgia and complex regional pain syndrome. Nat. Rev. Rheumatol. 2015, 11, 639–648. [Google Scholar] [CrossRef]
- Üçeyler, N.; Valenza, R.; Stock, M.; Schedel, R.; Sprotte, G.; Sommer, C. Reduced levels of antiinflammatory cytokines in patients with chronic widespread pain. Arthritis Rheum. 2006, 54, 2656–2664. [Google Scholar] [CrossRef]
- Shao, Q.; Li, Y.; Wang, Q.; Zhao, J. IL-10 and IL-1β Mediate Neuropathic-Pain Like Behavior in the Ventrolateral Orbital Cortex. Neurochem. Res. 2015, 40, 733–739. [Google Scholar] [CrossRef]
- Andrés-Rodríguez, L.; Borràs, X.; Feliu-Soler, A.; Pérez-Aranda, A.; Angarita-Osorio, N.; Moreno-Peral, P.; Montero-Marin, J.; García-Campayo, J.; Carvalho, A.F.; Maes, M.; et al. Peripheral immune aberrations in fibromyalgia: A systematic review, meta-analysis and meta-regression. Brain Behav. Immun. 2019, 87, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Puma, C.; Danik, M.; Quirion, R.; Ramon, F.; Williams, S. The chemokine interleukin-8 acutely reduces Ca2+ currents in identified cholinergic septal neurons expressing CXCR1 and CXCR2 receptor mRNAs. J. Neurochem. 2001, 78, 960–971. [Google Scholar] [CrossRef] [PubMed]
- Kutlu, F.C.; Özdolap, Ş.; Sarikaya, S. Pro-inflammatory Cytokines and Oxidized Low-Density-Lipoprotein in Patients with Fibromyalgia. Arch. Rheumatol. 2019, 34, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Clauw, D.J.; Arnold, L.M.; McCarberg, B.H.; FibroCollaborative. The Science of Fibromyalgia. Mayo Clin. Proc. 2011, 86, 907–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rus, A.; Molina, F.; Del Moral, M.L.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Catecholamine and Indolamine Pathway: A Case–Control Study in Fibromyalgia. Biol. Res. Nurs. 2018, 20, 577–586. [Google Scholar] [CrossRef]
- Russell, I.J.; Vaeroy, H.; Javors, M.; Nyberg, F. Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthritis Rheum. 1992, 35, 550–556. [Google Scholar] [CrossRef]
- Williams, D.A.; Clauw, D.J. Understanding Fibromyalgia: Lessons from the Broader Pain Research Community. J. Pain 2009, 10, 777–791. [Google Scholar] [CrossRef] [Green Version]
- Bote, M.E.; García, J.J.; Hinchado, M.D.; Ortega, E. Inflammatory/Stress Feedback Dysregulation in Women with Fibromyalgia. Neuroimmunomodulation 2012, 19, 343–351. [Google Scholar] [CrossRef]
- Paul-Savoie, E.; Potvin, S.; Daigle, K.; Normand, E.; Corbin, J.-F.; Gagnon, R.; Marchand, S. A Deficit in Peripheral Serotonin Levels in Major Depressive Disorder but Not in Chronic Widespread Pain. Clin. J. Pain 2011, 27, 529–534. [Google Scholar] [CrossRef]
- Welsch, P.; Üçeyler, N.; Klose, P.; Walitt, B.; Häuser, W. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia. Cochrane Database Syst. Rev. 2018, 2020, CD010292. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Carvalho, A.F. The Compensatory Immune-Regulatory Reflex System (CIRS) in Depression and Bipolar Disorder. Mol. Neurobiol. 2018, 55, 8885–8903. [Google Scholar] [CrossRef] [PubMed]
- Salgado, A.S.I. Fisioterapia Integrativa: Como ter Saúde em um Mundo Doente; Midiograf: Londrina, Brasil, 2019; p. 304. [Google Scholar]
- Grosjean, D. Investigação da Etiologia em Microfisioterapia; Andreoli: São Paulo, Brasil, 2016; p. 160. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Gentle Touch Therapy (n = 32) | Placebo (n = 32) | p-Value |
|---|---|---|---|
| Age (years) | 53.7 (9.6) | 53.2 (8.16 | 0.837 |
| Body mass index (Kg/m2) | 29.0 (5.1) | 28.9 (5.9) | 0.984 |
| Time of fibromyalgia diagnosis (years) | 7.3 (5.2) | 6.9 (4.9) | 0.638 |
| Physical activity (yes/no) | 15/17 | 16/19 | - |
| Smoking (yes/no) | 4/28 | 6/26 | - |
| Analgesic medication in use (yes/no) | 15/16 | 15/17 | - |
| History of anxiety (yes/no) | 4/28 | 6/26 | - |
| History of depression disorders (yes/no) | 10/22 | 14/18 | - |
| Drug active on the nervous system in use (yes/no) ** | 14/18 | 13/19 | - |
| Selective Serotonin Reuptake Inhibitor in use (yes/no) | 12/20 | 12/20 | - |
| History of chronic disease (yes/no) | 14/18 | 22/10 | - |
| Hypertension (yes/no) | 10/21 | 13/19 | - |
| Type 2 Diabetes Mellitus (yes/no) | 3/28 | 4/28 | - |
| Pain on the VAS (range 0–10) | 7.7 (1.6) | 8.1 (1.5) | 0.368 |
| Short-form McGill Pain Questionnaire | 52.4 (13.0) | 52.7 (11.2) | 0.926 |
| Fibromyalgia Impact Questionnaire (FIQ) | 61.6 (10.9) | 65.3 (7.4) | 0.995 |
| SF-36 Quality of Life Questionnaire | |||
| Physical functioning | 30.1 (16.5) | 35.7 (20.7) | 0.237 |
| General health | 44.5 (17.3) | 45.2 (22.5) | 0.901 |
| Physical Role | 11.9 (22.8) | 13.2 (25.3) | 0.820 |
| Bodily pain | 25.4 (16.4) | 24.3 (13.8) | 0.767 |
| Social functioning | 42.1 (22.5) | 44.7 (25.1) | 0.738 |
| Vitality | 29.0 (16.1) | 28.1 (17.1) | 0.875 |
| Emotional Role | 19.8 (30.2) | 28.1 (38.8) | 0.343 |
| Mental health | 41.0 (20.4) | 38.75 (22.4) | 0.668 |
| Serum BDNF (pg/mL) | 1526 (329.8) | 1496 (290.2) | 0.788 |
| Serum IL-8 (pg/mL) | 4.8 (2.3) | 5.9 (3.0) | 0.270 |
| Serum IL-10 (pg/mL) | 2.3 (1.0) | 2.9 (1.3) | 0.090 |
| Serum Serotonin (nmol/L) | 127.6 (112.6) | 117.0 (105.6) | 0.825 |
| Serum 5-HIAA (nmol/L) | 19.6 (9.0) | 17.2 (8.3) | 0.409 |
| Serum Dopamine (nmol/L) | 41.2 (26.3) | 39.6 (38.6) | 0.887 |
| Serum BH4 (nmol/L) | 5.8 (5.1) | 5.7 (2.3) | 0.932 |
| Dependent Variable: Percentage of Change on Pain Scores by Visual Analogue Scale from Baseline | ||||||
|---|---|---|---|---|---|---|
| Beta | Std. Error | df | t | Sig. | CI 95% | |
| Intercept | −58.4104 | 18.096799 | 147.489 | −3.228 | 0.002 | (−94.17 to −22.64) |
| Gentle touch therapy | −16.5963 | 4.374591 | 156.229 | −3.794 | 0.000 | (−25.23 to −7.95) |
| Placebo intervention | Reference 0 | |||||
| Brain-derived neurotrophic factor (BDNF) | 0.020730 | 0.009095 | 154.889 | 2.279 | 0.024 | (0.004 to 0.04) |
| Dopamine | −0.152667 | 0.065176 | 155.827 | −2.342 | 0.020 | (−0.28 to −0.03) |
| Serotonin | −0.024950 | 0.024901 | 154.004 | −1.002 | 0.318 | (−0.07 to 0.02) |
| 5-hydroxyindolacetic acid (5-HIAA) | 0.880112 | 0.273803 | 156.154 | 3.214 | 0.002 | (0.34 to 1.42) |
| Urinary tetrahydrobiopterin (BH4) | −0.272308 | 0.302144 | 126.154 | −0.901 | 0.369 | (−0.87 to 0.33) |
| History of depression diagnosis | 0.176808 | 5.146371 | 156.334 | 0.034 | 0.973 | (−9.98 to 10.34) |
| History of anxiety diagnosis | 18.5303 | 7.145711 | 156.215 | 2.593 | 0.010 | (4.42 to 32.64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salgado, A.S.I.; Takemoto, M.H.; de Souza, C.F.T.C.; Salm, D.C.; da Rosa, D.; Cardoso, G.C.; Ludtke, D.D.; Soares, S.F.C.; Ferreira, J.K.; Dutra, A.R.; et al. Gentle Touch Therapy, Pain Relief and Neuroplasticity at Baseline in Fibromyalgia Syndrome: A Randomized, Multicenter Trial with Six-Month Follow-Up. J. Clin. Med. 2022, 11, 4898. https://doi.org/10.3390/jcm11164898
Salgado ASI, Takemoto MH, de Souza CFTC, Salm DC, da Rosa D, Cardoso GC, Ludtke DD, Soares SFC, Ferreira JK, Dutra AR, et al. Gentle Touch Therapy, Pain Relief and Neuroplasticity at Baseline in Fibromyalgia Syndrome: A Randomized, Multicenter Trial with Six-Month Follow-Up. Journal of Clinical Medicine. 2022; 11(16):4898. https://doi.org/10.3390/jcm11164898
Chicago/Turabian StyleSalgado, Afonso Shiguemi Inoue, Miriam Hatsue Takemoto, Carla Fernanda Tallarico Carvalho de Souza, Daiana Cristina Salm, Danielli da Rosa, Gabriela Correa Cardoso, Daniela Dero Ludtke, Silvia Fiorillo Cabrera Soares, Júlia Koerich Ferreira, Aline Raulino Dutra, and et al. 2022. "Gentle Touch Therapy, Pain Relief and Neuroplasticity at Baseline in Fibromyalgia Syndrome: A Randomized, Multicenter Trial with Six-Month Follow-Up" Journal of Clinical Medicine 11, no. 16: 4898. https://doi.org/10.3390/jcm11164898
APA StyleSalgado, A. S. I., Takemoto, M. H., de Souza, C. F. T. C., Salm, D. C., da Rosa, D., Cardoso, G. C., Ludtke, D. D., Soares, S. F. C., Ferreira, J. K., Dutra, A. R., Szeremeta, Y. C., Mazzardo, G., Mayra, J., Sheffer, D. d. L., Caumo, W., Bittencourt, E. B., Schleip, R., Latini, A., Bobinski, F., & Martins, D. F. (2022). Gentle Touch Therapy, Pain Relief and Neuroplasticity at Baseline in Fibromyalgia Syndrome: A Randomized, Multicenter Trial with Six-Month Follow-Up. Journal of Clinical Medicine, 11(16), 4898. https://doi.org/10.3390/jcm11164898