

Optical Coherence Tomography as a Biomarker for Differential Diagnostics in Nystagmus: Ganglion Cell Layer Thickness Ratio

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Measurements
2.2.1. Visual Evoked Potentials
2.2.2. Optical Coherence Tomography (OCT)
2.3. Statistics
3. Results
3.1. Overview of Ophthalmological Characteristics
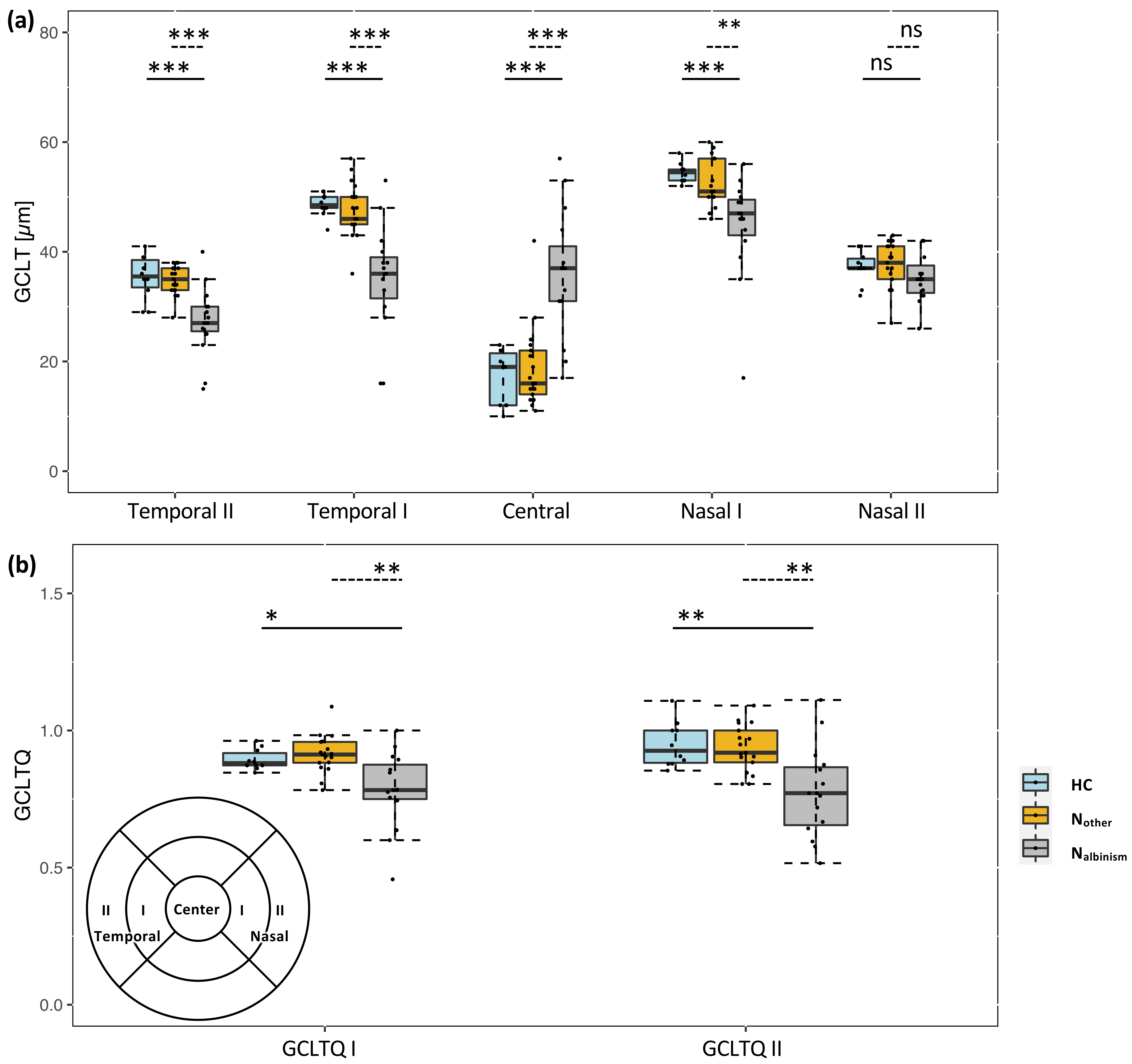
3.2. OCT Analysis: GCLTQ
3.3. GCLTQ Diagnostic Performance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brücher, V.C.; Heiduschka, P.; Grenzebach, U.; Eter, N.; Biermann, J. Distribution of macular ganglion cell layer thickness in foveal hypoplasia: A new diagnostic criterion for ocular albinism. PLoS ONE 2019, 14, e0224410. [Google Scholar] [CrossRef] [PubMed]
- Bakker, R.; Wagstaff, P.E.; Kruijt, C.C.; Emri, E.; van Karnebeek, C.D.M.; Hoffmann, M.B.; Brooks, B.P.; Boon, C.J.F.; Montoliu, L.; van Genderen, M.M.; et al. The retinal pigmentation pathway in human albinism: Not so black and white. Prog. Retin. Eye Res. 2022, 101091, in press. [Google Scholar] [CrossRef] [PubMed]
- Kruijt, C.C.; de Wit, G.C.; Bergen, A.A.; Florijn, R.J.; Schalij-Delfos, N.E.; van Genderen, M.M. The Phenotypic Spectrum of Albinism. Ophthalmology 2018, 125, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Cronin, T.H.; Hertle, R.W.; Ishikawa, H.; Schuman, J.S. Spectral domain optical coherence tomography for detection of foveal morphology in patients with nystagmus. J. AAPOS 2009, 13, 563–566. [Google Scholar] [CrossRef]
- Kuht, H.J.; Maconachie, G.D.E.; Han, J.; Kessel, L.; van Genderen, M.M.; McLean, R.J.; Hisaund, M.; Tu, Z.; Hertle, R.W.; Gronskov, K.; et al. Genotypic and Phenotypic Spectrum of Foveal Hypoplasia: A Multicenter Study. Ophthalmology 2022, 129, 708–718. [Google Scholar] [CrossRef]
- Kuht, H.J.; Thomas, M.G.; McLean, R.J.; Sheth, V.; Proudlock, F.A.; Gottlob, I. Abnormal foveal morphology in carriers of oculocutaneous albinism. Br. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Noval, S.; Freedman, S.F.; Asrani, S.; El-Dairi, M.A. Incidence of fovea plana in normal children. J. Am. Assoc. Pediatric Ophthalmol. Strabismus 2014, 18, 471–475. [Google Scholar] [CrossRef]
- Thomas, M.G.; Kumar, A.; Mohammad, S.; Proudlock, F.A.; Engle, E.C.; Andrews, C.; Chan, W.-M.; Thomas, S.; Gottlob, I. Structural Grading of Foveal Hypoplasia Using Spectral-Domain Optical Coherence Tomography: A Predictor of Visual Acuity? Ophthalmology 2011, 118, 1653–1660. [Google Scholar] [CrossRef]
- Schmitz, B.; Schaefer, T.; Krick, C.M.; Reith, W.; Backens, M.; Käsmann-Kellner, B. Configuration of the Optic Chiasm in Humans with Albinism as Revealed by Magnetic Resonance Imaging. Investig. Ophthalmol. Vis. Sci. 2003, 44, 16–21. [Google Scholar] [CrossRef]
- American Electroencephalographic Society. Guideline thirteen: Guidelines for standard electrode position nomenclature. J. Clin. Neurophysiol. 1994, 11, 111–113. [Google Scholar] [CrossRef]
- Odom, J.V.; Bach, M.; Brigell, M.; Holder, G.E.; McCulloch, D.L.; Mizota, A.; Tormene, A.P. ISCEV standard for clinical visual evoked potentials: (2016 update). Doc. Ophthalmol. 2016, 133, 1–9. [Google Scholar] [CrossRef]
- Hoffmann, M.B.; Wolynski, B.; Bach, M.; Meltendorf, S.; Behrens-Baumann, W.; Golla, F. Optic Nerve Projections in Patients with Primary Ciliary Dyskinesia. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4617–4625. [Google Scholar] [CrossRef]
- Hoffmann, M.B.; Lorenz, B.; Morland, A.B.; Schmidtborn, L.C. Misrouting of the Optic Nerves in Albinism: Estimation of the Extent with Visual Evoked Potentials. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3892–3898. [Google Scholar] [CrossRef]
- R Core Team. R: The R Project for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: https://www.r-project.org/ (accessed on 1 January 2020).
- Woertz, E.N.; Omoba, B.S.; Dunn, T.M.; Chiu, S.J.; Farsiu, S.; Strul, S.; Summers, C.G.; Drack, A.V.; Carroll, J. Assessing Ganglion Cell Layer Topography in Human Albinism Using Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2020, 61, 36. [Google Scholar] [CrossRef]
- Oki, R.; Yamada, K.; Nakano, S.; Kimoto, K.; Yamamoto, K.; Kondo, H.; Kubota, T. A Japanese Family with Autosomal Dominant Oculocutaneous Albinism Type 4. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1008–1016. [Google Scholar] [CrossRef]
- Bridge, H.; von dem Hagen, E.A.H.; Davies, G.; Chambers, C.; Gouws, A.; Hoffmann, M.; Morland, A.B. Changes in brain morphology in albinism reflect reduced visual acuity. Cortex 2014, 56, 64–72. [Google Scholar] [CrossRef]
- Hoffmann, M.B.; Dumoulin, S.O. Congenital visual pathway abnormalities: A window onto cortical stability and plasticity. Trends Neurosci. 2015, 38, 55–65. [Google Scholar] [CrossRef]
- Puzniak, R.J.; Prabhakaran, G.T.; Hoffmann, M.B. Deep Learning-Based Detection of Malformed Optic Chiasms From MRI Images. Front. Neurosci. 2021, 15, 755785. [Google Scholar] [CrossRef]
- Puzniak, R.J.; Ahmadi, K.; Kaufmann, J.; Gouws, A.; Morland, A.B.; Pestilli, F.; Hoffmann, M.B. Quantifying nerve decussation abnormalities in the optic chiasm. NeuroImage Clin. 2019, 24, 102055. [Google Scholar] [CrossRef]
- Hoffmann, M.B.; Tolhurst, D.J.; Moore, A.T.; Morland, A.B. Organization of the Visual Cortex in Human Albinism. J. Neurosci. 2003, 23, 8921–8930. [Google Scholar] [CrossRef]
- Von Dem Hagen, E.A.H.; Houston, G.C.; Hoffmann, M.B.; Morland, A.B. Pigmentation predicts the shift in the line of decussation in humans with albinism. Eur. J. Neurosci. 2007, 25, 503–511. [Google Scholar] [CrossRef]
- Puzniak, R.J.; McPherson, B.; Ahmadi, K.; Herbik, A.; Kaufmann, J.; Liebe, T.; Gouws, A.; Morland, A.B.; Gottlob, I.; Hoffmann, M.B.; et al. CHIASM, the human brain albinism and achiasma MRI dataset. Sci. Data 2021, 8, 308. [Google Scholar] [CrossRef]


{kind=link}
| Center-ID | Eye | Group | Nystagmus Type | BCVA OD/OS | Fundus Hypopigmentation OD/OS | Misrouting VEP | Foveal Hypoplasia OD/OS |
|---|---|---|---|---|---|---|---|
| MD-BWZ133 | Both | HC | None | −0.1/−0.2 | 0/0 | − | 0/0 |
| MD-KZJ780 | Both | HC | None | −0.1/−0.1 | 0/0 | − | 0/0 |
| MD-LHP483 | Both | HC | None | 0/0 | 0/0 | − | 0/0 |
| MD-RKM968 | Both | HC | None | −0.2/−0.2 | 0/0 | − | 0/0 |
| MD-YHW227 | Both | HC | None | −0.2/−0.2 | 0/0 | − | 0/0 |
| MD-BJA815 | OS | INS | J/H | 0.2/0.2 | 0/0 | − | n.a./0 |
| MD-ENH995 | Both | INS | J/H | 0.6/0.49 | 0/0 | − | 0/0 |
| MD-JDG458 | Both | INS | P/H | 0.3/0.3 | 0/0 | − | 0/0 |
| MD-MFY773 | OD | INS | J/H | 0.1/0.3 | 0/0 | − | 0/n.a. |
| MD-PEP763 | Both | INS | J/H | 0/0.4 | 0/0 | − | 0/0 |
| MD-SUQ660 | Both | INS | J/H | −0.1/−0.1 | 0/0 | − | 0/0 |
| MD-WQE170 | OD | INS | P/H | 0.2/0.2 | 0/0 | − | 1/n.a. |
| MS-MS01 | OS | INS | J/H | 0.1/0.3 | 0/0 | n.a. | n.a./0 |
| MS-MS02 | OD | INS | J/H | 0.4/0.4 | 0/0 | n.a. | 4/n.a. |
| MD-TGY248 | Both | AN | J/V | 0/0 | 0/0 | − | 0/0 |
| MD-TIO945 | Both | AN | J/H | 0/−0.1 | 0/0 | − | 0/0 |
| MD-HAA059 | Both | Albinism ⁎ | n.a. ‡ | 0.6/0.7 | 3/3 | + | 3/4 |
| MD-JTE807 | Both | Albinism | J/H | 0.4/0.8 | 0/0 | + | 4/4 |
| MD-NLE254 | Both | Albinism ⁎ | n.a. ‡ | 0.4/0.4 | 2/2 | + | 3/3 |
| MD-PYV946 | OS | Albinism | J/H | 0.4/0.4 | 2/2 | + | n.a./1 |
| MD-TCU787 | Both | Albinism ⁎ | n.a. ‡ | 0.8/0.6 | 2/2 | + | 3/3 |
| MS-MS03 | Both | Albinism | J/H | 0.5/0.4 | 2/2 | n.a. | 3/3 |
| MS-MS04 | Both | Albinism | P/H | 0.4/0.4 | 3/3 | + | 3/3 |
| MS-MS05 | Both | Albinism ⁎ | J/H | 0.5/0.4 | 3/3 | n.a. | 3/4 |
| HC | Nother | Nalbinism | |||||
|---|---|---|---|---|---|---|---|
| p | HC vs. Nother | HC vs. Nalbinism | Nother vs. Nalbinism | ||||
| n (f) | 5 (3) | 11 (6) | 8 (5) | ||||
| Age [y] | 37 (21–56) | 27 (8–56) | 19 (5–52) | 0.12 | |||
| Eyes (OD) | 10 (5) | 17 (9) | 15 (7) | 1.0§ | |||
| SE [Diopters] ‡ | [−0.25 (−2–+3.4)] | [−1.0 (−7–+3.5)] | [1.5 (−4.4–+6.3)] | 0.005 ‡ | 0.16 | 0.07 | 0.001 |
| BCVA [LogMAR] ‡ | [−0.15 (0–−0.20)] | [0.20 (+1–−0.1)] | [0.4 (+0.8–+0.4)] | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| (n of Eyes) Ophthalmological examination | 10 | 17 | 15 | ||||
| Strabismus | 0 | 2 | 4 | 0.16 § | |||
| Iris translucency | 0 | 0 | 8 | <0.001 § | |||
| Fundus hypopigmentation | <0.001 § | ||||||
| 0 | 10 | 17 | 2 | ||||
| 1 | 0 | 0 | 0 | ||||
| 2 | 0 | 0 | 7 | ||||
| 3 | 0 | 0 | 6 | ||||
| OCT | |||||||
| FH | <0.001 § | ||||||
| 0 | 10 | 15 | 0 | ||||
| 1 | 0 | 1 | 1 | ||||
| 2 | 0 | 0 | 0 | ||||
| 3 | 0 | 0 | 10 | ||||
| 4 | 0 | 1 | 4 | ||||
| Retinal GCLT [µm] | |||||||
| Nasal II | 37 ± 3 | 37 ± 4 | 35 ± 5 | 0.31 | |||
| Nasal I ‡ | [55 (52–58)] | [51 (46–60)] | [47 (17–56)] | <0.001 ‡ | >0.05 | <0.001 | 0.004 |
| Central ‡ | [19 (10–23)] | [16 (11–42)] | [37 (17–57)] | <0.001 ‡ | >0.05 | <0.001 | <0.001 |
| Temporal I | 49 ± 2 | 48 ± 5 | 35 ± 10 | <0.001 | >0.05 | <0.001 | <0.001 |
| Temporal II | 35 ± 4 | 35 ± 3 | 27 ± 6 | <0.001 | >0.05 | <0.001 | <0.001 |
| GCLTQ I [ratio] | 0.89 ± 0.04 | 0.91 ± 0.07 | 0.78 ± 0.14 | 0.001 | 0.60 | 0.025 | 0.002 |
| GCLTQ II [ratio] | 0.95 ± 0.08 | 0.93 ± 0.09 | 0.77 ± 0.17 | <0.001 | 0.99 | 0.003 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Nosairy, K.O.; Quanz, E.V.; Biermann, J.; Hoffmann, M.B. Optical Coherence Tomography as a Biomarker for Differential Diagnostics in Nystagmus: Ganglion Cell Layer Thickness Ratio. J. Clin. Med. 2022, 11, 4941. https://doi.org/10.3390/jcm11174941
Al-Nosairy KO, Quanz EV, Biermann J, Hoffmann MB. Optical Coherence Tomography as a Biomarker for Differential Diagnostics in Nystagmus: Ganglion Cell Layer Thickness Ratio. Journal of Clinical Medicine. 2022; 11(17):4941. https://doi.org/10.3390/jcm11174941
Chicago/Turabian StyleAl-Nosairy, Khaldoon O., Elisabeth V. Quanz, Julia Biermann, and Michael B. Hoffmann. 2022. "Optical Coherence Tomography as a Biomarker for Differential Diagnostics in Nystagmus: Ganglion Cell Layer Thickness Ratio" Journal of Clinical Medicine 11, no. 17: 4941. https://doi.org/10.3390/jcm11174941
APA StyleAl-Nosairy, K. O., Quanz, E. V., Biermann, J., & Hoffmann, M. B. (2022). Optical Coherence Tomography as a Biomarker for Differential Diagnostics in Nystagmus: Ganglion Cell Layer Thickness Ratio. Journal of Clinical Medicine, 11(17), 4941. https://doi.org/10.3390/jcm11174941