

Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Data Collection
2.3. Patient and Public Involvement
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Immunosuppressive Regimens
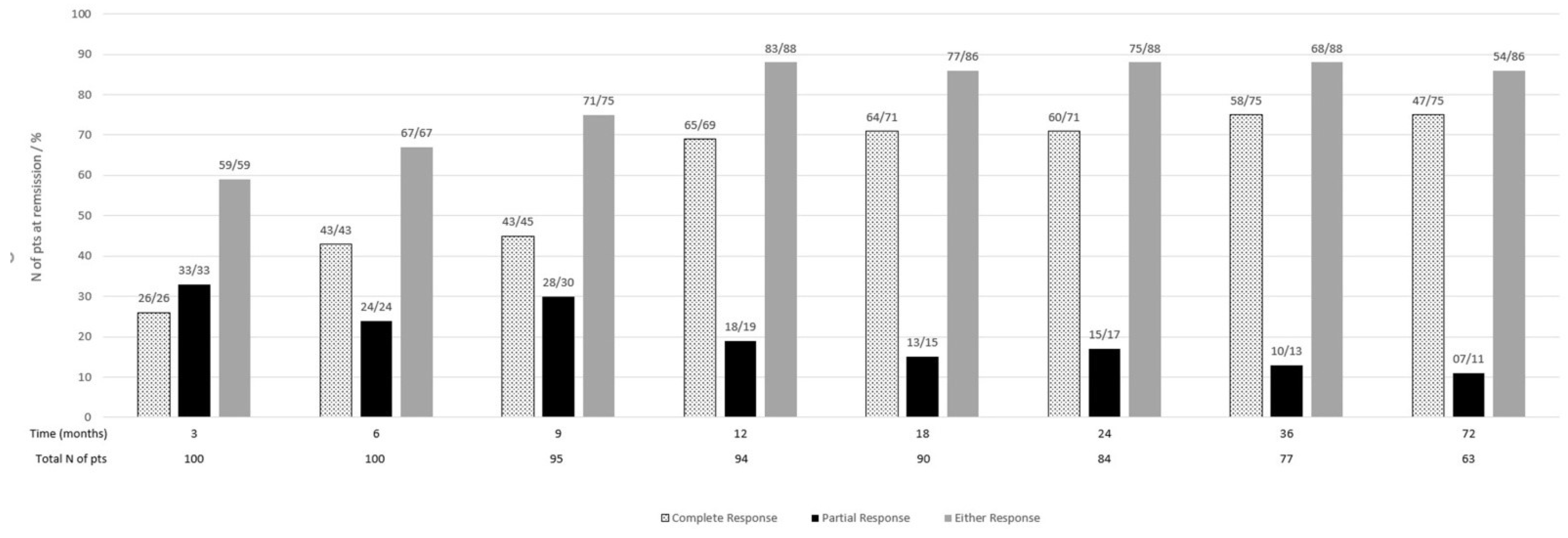
3.3. Renal Response and Determinants of Response
3.4. Renal Flares and Determinants of Flares
3.5. Patient Survival
3.6. Renal Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anders, H.-J.; Saxena, R.; Zhao, M.-H.; Parodis, I.; Salmon, J.E.; Mohan, C. Lupus nephritis. Nat. Rev. Dis. Primers 2020, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Iaccarino, L.; Ghirardello, A.; Zampieri, S.; Arienti, S.; Sarzi-Puttini, P.; Atzeni, F.; Piccoli, A.; Todesco, S. Long-term prognosis and causes of death in systemic lupus erythematosus. Am. J. Med. 2006, 119, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Yap, D.Y.; Tang, C.S.; Ma, M.K.; Lam, M.F.; Chan, T.M. Survival analysis and causes of mortality in patients with lupus nephritis. Nephrol. Dial. Transplant. 2012, 27, 3248–3254. [Google Scholar] [CrossRef] [PubMed]
- Lerang, K.; Gilboe, I.M.; Steinar Thelle, D.; Gran, J.T. Mortality and years of potential life loss in systemic lupus erythematosus: A population-based cohort study. Lupus 2014, 23, 1546–1552. [Google Scholar] [CrossRef] [PubMed]
- Costenbader, K.H.; Desai, A.; Alarcón, G.S.; Hiraki, L.T.; Shaykevich, T.; Brookhart, M.A.; Massarotti, E.; Lu, B.; Solomon, D.H.; Winkelmayer, W.C. Trends in the incidence, demographics, and outcomes of end-stage renal disease due to lupus nephritis in the US from 1995 to 2006. Arthritis Rheum. 2011, 63, 1681–1688. [Google Scholar] [CrossRef]
- Tektonidou, M.; Dasgupta, A.; Ward, M.M. Risk of end-stage renal disease in patients with lupus nephritis, 1971-2015: A systematic review and Bayesian meta-analysis. Arthritis Rheumatol. 2016, 68, 1432–1441. [Google Scholar] [CrossRef]
- Bastian, H.M.; Roseman, J.M.; McGwin, G.; Alarcón, G.S.; Friedman, A.W.; Fessler, B.J.; A Baethge, B.; Reveille, J.D.; LUMINA Study Group. Systemic lupus erythematosus in three ethnic groups. XII. Risk factors for lupus nephritis after diagnosis. Lupus 2002, 11, 152–160. [Google Scholar] [CrossRef]
- Bertsias, G.K.; Tektonidou, M.; Amoura, Z.; Aringer, M.; Bajema, I.; Berden, J.H.; Boletis, J.; Cervera, R.; Dörner, T.; Doria, A.; et al. Joint European League Against Rheumatism and European Renal Association–European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann. Rheum. Dis. 2012, 71, 1771–1782. [Google Scholar] [CrossRef]
- Almalki, A.H.; Alrowaie, F.A.; Alhozali, H.M.; Almalki, N.K.; Alsubei, A.I.; Alturki, M.S.; Sadagah, L.F. Remission and long-term outcomes of proliferative lupus nephritis: Retrospective study of 96 patients from Saudi Arabia. Lupus 2019, 28, 1082–1090. [Google Scholar] [CrossRef]
- Parikh, S.V.; Nagaraja, H.N.; Hebert, L.; Rovin, B.H. Renal flare as a predictor of incident and progressive CKD in patients with lupus nephritis. Clin. J. Am. Soc. Nephrol. 2014, 9, 279–284. [Google Scholar] [CrossRef]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic Lupus Erythematosus Disease Activity Index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group. KDIGO Clinical Practice Guideline for Glomerulonephritis. Kidney Int. Suppl. 2012, 2, 139–274. [Google Scholar]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Ichinose, K.; Kitamura, M.; Sato, S.; Eguchi, M.; Okamoto, M.; Endo, Y.; Tsuji, S.; Takatani, A.; Shimizu, T.; Umeda, M.; et al. Complete renal response at 12 months after induction therapy is associated with renal relapse-free rate in lupus nephritis: Asinglecenter, retrospective cohort study. Lupus 2019, 28, 501–509. [Google Scholar] [CrossRef]
- Dall’Era, M.; Cisternas, M.G.; Smilek, D.E.; Straub, L.; Houssiau, F.A.; Cervera, R.; Rovin, B.H.; Mackay, M. Predictors of long-term renal outcome in lupus nephritis trials: Lessons learned from the Euro-Lupus nephritis cohort. Arthritis Rheumatol. 2015, 67, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Tamirou, F.; Lauwerys, B.R.; Dall’Era, M.; Mackay, M.; Rovin, B.; Cervera, R.; AHoussiau, F. A proteinuria cut-off level of 0.7 g/day after 12 months of treatment best predicts long-term renal outcome in lupus nephritis: Data from the MAINTAIN Nephritis Trial. Lupus Sci. Med. 2015, 2, e000123. [Google Scholar] [CrossRef]
- Ugolini-Lopes, M.R.; Seguro, L.P.C.; Castro, M.X.F.; Daffre, D.; Lopes, A.C.; Borba, E.F.; Bonfá, E. Early proteinuria response: A valid real-life situation predictor of long-term lupus renal outcome in an ethnically diverse group with severe biopsy-proven nephritis? Lupus Sci. Med. 2017, 4, e000213. [Google Scholar] [CrossRef]
- Moroni, G.; Gatto, M.; Tamborini, F.; Quaglini, S.; Radice, F.; Saccon, F.; Frontini, G.; Alberici, F.; Sacchi, L.; Binda, V.; et al. Lack of EULAR/ERA-EDTA response at 1 year predicts poor long-term renal outcome in patients with lupus nephritis. Ann. Rheum. Dis. 2020, 79, 1077–1083. [Google Scholar] [CrossRef]
- Chen, Y.E.; Korbet, S.M.; Katz, R.S.; Schwartz, M.M.; Lewis, E.J. Value of a complete or partial remission in severe lupus nephritis. Clin. J. Am. Soc. Nephrol. 2008, 3, 46–53. [Google Scholar] [CrossRef]
- Ginzler, E.M.; Wofsy, D.; Isenberg, D.; Gordon, C.; Lisk, L.; Dooley, M.A. Mycophenolate mofetil or intravenous cyclophosphamide for induction treatment for lupus nephritis. N. Engl. J. Med. 2005, 353, 2219–2228. [Google Scholar] [CrossRef]
- Appel, G.B.; Contreras, G.; Dooley, M.A.; Ginzler, E.M.; Isenberg, D.; Jayne, D.; Li, L.-S.; Mysler, E.; Sánchez-Guerrero, J.; Solomons, N.; et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J. Am. Soc. Nephrol. 2009, 20, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Korbet, S.M.; Lewis, E.J.; Collaborative Study Group. Complete remission in severe lupus nephritis: Assessing the rate of loss in proteinuria. Nephrol. Dial. Transplant. 2012, 27, 2813–2819. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Wang, H.; Le, J.; Lan, L.; Xu, Y.; Yang, Y.; Chen, J.; Han, F. Early-stage predictors for treatment responses in patients with active lupus nephritis. Lupus 2019, 28, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Luís, M.S.; Bultink, I.E.; da Silva, J.A.; Voskuyl, A.E.; Inês, L.S. Early predictors of renal outcome in patients with proliferative lupus nephritis:a 36-month cohort study. Rheumatology 2021, 60, 5134–5141. [Google Scholar] [CrossRef] [PubMed]
- Fernandes das Neves, M.; Irlapati RV, P.; Isenberg, D. Assessment of long-term remission in lupus nephritis patients: A retrospective analysis over 30 years. Rheumatology 2015, 54, 1403–1407. [Google Scholar] [CrossRef]
- Pakchotanon, R.; Gladman, D.D.; Su, J.; Urowitz, M.B. Sustained complete renal remission is a predictor of reduced mortality, chronic kidney disease and endstage renal disease in lupus nephritis. Lupus 2018, 27, 468–474. [Google Scholar] [CrossRef]
- Koo, H.S.; Kim, S.; Chin, H.J. Remission of proteinuria indicates good prognosis in patients with diffuse proliferative lupus nephritis. Lupus 2016, 25, 3–11. [Google Scholar] [CrossRef]
- Pirson, V.; Enfrein, A.; Houssiau, F.A.; Tamirou, F. Absence of renal remission portends poor long-term kidney outcome in lupus nephritis. Lupus Sci. Med. 2021, 8, e000533. [Google Scholar] [CrossRef]
- Moroni, G.; Quaglini, S.; Radice, A.; Trezzi, B.; Raffiotta, F.; Messa, P.; Sinico, R.A. The value of a panel of autoantibodies for predicting the activity of lupus nephritis at time of renal biopsy. J. Immunol. Res. 2015, 2015, 106904. [Google Scholar] [CrossRef]
- Ichinose, K.; Kitamura, M.; Sato, S.; Fujikawa, K.; Horai, Y.; Matsuoka, N.; Tsuboi, M.; Nonaka, F.; Shimizu, T.; Fukui, S.; et al. Factors predictive of long-term mortality in lupus nephritis: A multicenter retrospective study of a Japanese cohort. Lupus 2019, 28, 295–303. [Google Scholar] [CrossRef]
- McDonald, S.; Yiu, S.; Su, L.; Gordon, C.; Truman, M.; Lisk, L.; Solomons, N.; Bruce, I.N. Predictors of treatment response in a lupus nephritis population: Lessons from the Aspreva Lupus Management Study (ALMS) trial. Lupus Sci. Med. 2022, 9, e000584. [Google Scholar] [CrossRef] [PubMed]
- Touma, Z.; Urowitz, M.B.; Ibañez, M.; Gladman, D.D. Time to recovery from proteinuria in patients with lupus nephritis receiving standard treatment. J. Rheumatol. 2014, 41, 688–697. [Google Scholar] [CrossRef] [Green Version]
- Mosca, M.; Bencivelli, W.; Neri, R.; Pasquariello, A.; Batini, V.; Puccini, R.; Tavoni, A.; Bombardieri, S. Renal flares in 91 SLE patients with diffuse proliferative glomerulonephritis. Kidney Int. 2002, 61, 1502–1509. [Google Scholar] [CrossRef] [PubMed]
- Sprangers, B.; Monahan, M.; Appel, G.B. Diagnosis and treatment of lupus nephritis flares—an update. Nat. Rev. Nephrol. 2012, 8, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Illei, G.G.; Takada, K.; Parkin, D.; Austin, H.A.; Crane, M.; Yarboro, C.H.; Vaughan, E.M.; Kuroiwa, T.; Danning, C.L.; Pando, J.; et al. Renal flares are common in patients with severe proliferative lupus nephritis treated with pulse immunosuppressive therapy: Long-term followup of a cohort of 145 patients participating in randomized controlled studies. Arthritis Rheum. 2002, 46, 995–1002. [Google Scholar] [CrossRef]
- Yap, D.Y.; Tang, C.; Ma, M.K.; Mok, M.M.; Chan, G.C.; Kwan, L.P.; Chan, T.M. Longterm data on disease flares in patients with proliferative lupus nephritis in recent years. J. Rheumatol. 2017, 44, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- So, M.W.; Koo, B.S.; Kim, Y.G.; Lee, C.-K.; Yoo, B. Predictive value of remission status after 6 months induction therapy in patients with proliferative lupus nephritis: A retrospective analysis. Clin. Rheumatol. 2011, 30, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Parodis, I.; Adamichou, C.; Aydin, S.; Gomez, A.; Demoulin, N.; Weinmann-Menke, J.; A Houssiau, F.; Tamirou, F. Per-protocol repeat kidney biopsy portends relapse and long-term outcome in incident cases of proliferative lupus nephritis. Rheumatology 2020, 59, 3424–3434. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, M.; Azzato, F.; Toblli, J.E.; De Rosa, G.; Fuentes, F.; Nagaraja, H.N.; Nash, R.; Rovin, B.H. A prospective observational cohort study highlights kidney biopsy findings of lupus nephritis patients in remission who flare following withdrawal of maintenance therapy. Kidney Int. 2018, 94, 788–794. [Google Scholar] [CrossRef]
- Farinha, F.; Pepper, R.J.; Oliveira, D.G.; McDonnell, T.; Isenberg, D.A.; Rahman, A. Outcomes of membranous and proliferative lupus nephritis–analysis of a single-centre cohort with more than 30 years of follow-up. Rheumatology 2020, 59, 3314–3323. [Google Scholar] [CrossRef]
- Mahajan, A.; Amelio, J.; Gairy, K.; Kaur, G.; A Levy, R.; Roth, D.; Bass, D. Systemic lupus erythematosus, lupus nephritis and end-stage renal disease: A pragmatic review mapping disease severity and progression. Lupus 2020, 29, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Hanly, J.G.; O’Keeffe, A.G.; Su, L.; Urowitz, M.B.; Romero-Diaz, J.; Gordon, C.; Bae, S.-C.; Bernatsky, S.; Clarke, A.E.; Wallace, D.J.; et al. The frequency and outcome of lupus nephritis: Results from an international inception cohort study. Rheumatology 2016, 55, 252–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moroni, G.; Vercelloni, P.G.; Quaglini, S.; Gatto, M.; Gianfreda, D.; Sacchi, L.; Raffiotta, F.; Zen, M.; Costantini, G.; Urban, M.L.; et al. Changing patterns in clinical–histological presentation and renal outcome over the last five decades in a cohort of 499 patients with lupusnephritis. Ann. Rheum. Dis. 2018, 77, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liang, D.; Zhang, H.; Liu, Z.; Le, W.; Zhou, M.; Hu, W.; Zeng, C. Long-term renal outcomes in a cohort of 1814 Chinese patients with biopsy-proven lupus nephritis. Lupus 2015, 24, 1468–1478. [Google Scholar] [CrossRef]
- Vajgel, G.; Oliveira, C.B.L.; Costa, D.M.N.; Cavalcante, M.A.G.M.; Valente, L.M.; Sesso, R.; Crovella, S.; Kirsztajn, G.M.; Sandrin-Garcia, P. Initial renal histology and early response predict outcomes of Brazilian lupus nephritis patients. Lupus 2020, 29, 83–91. [Google Scholar] [CrossRef]
- Gatto, M.; Radice, F.; Saccon, F.; Calatroni, M.; Frontini, G.; Trezzi, B.; Zen, M.; Ghirardello, A.; Tamborini, F.; Binda, V.; et al. Clinical and histological findings at second but not at first kidney biopsy predict end-stage kidney disease in a large multicentric cohort of patients with active lupus nephritis. Lupus Sci. Med. 2022, 9, 000689. [Google Scholar] [CrossRef]
- Wilson, P.C.; Kashgarian, M.; Moeckel, G. Interstitial inflammation and interstitial fibrosis and tubular atrophy predict renal survival in lupus nephritis. Clin. Kidney J. 2018, 11, 207–218. [Google Scholar] [CrossRef]
- Tamirou, F.; D’Cruz, D.; Sangle, S.; Remy, P.; Vasconcelos, C.; Fiehn, C.; Guttierez, M.D.M.A.; Gilboe, I.-M.; Tektonidou, M.; Blockmans, D.; et al. Long-term follow-up of the MAINTAIN Nephritis Trial, comparing azathioprine and mycophenolate mofetil as maintenance therapy of lupus nephritis. Ann. Rheum. Dis. 2016, 75, 526–531. [Google Scholar] [CrossRef]
- Hanaoka, H.; Yamada, H.; Kiyokawa, T.; Iida, H.; Suzuki, T.; Yamasaki, Y.; Ooka, S.; Nagafuchi, H.; Okazaki, T.; Ichikawa, D.; et al. Lack of partial renal response by 12 weeks after induction therapy predicts poor renal response and systemic damage accrual in lupus nephritis class III or IV. Arthritis Res. Ther. 2017, 19, 4. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics | Mean ± SD, Median(IQR), N/% |
|---|---|
| Age (yr) mean ± SD | 31 ± 13 |
| Sex (M-F) N/% | 20/20–80/80 |
| Race (Caucasian-Other) N/% | 96/96–4/4 |
| Time from SLE diagnosis to LN (years)median(IQR) | () |
| LN as first presentation of SLE N/% | 51/51 |
| SLEDAI score median(IQR) | 12(4) |
| Low C3 N/% 1 | 65/77.5 |
| Low C4 N/% 1 | 55/65.5 |
| Positive anti-dsDNA antibodies N/% 2 | 63/78.5 |
| Proteinuria (g/24 h) median (IQR) | 2.6(4) |
| 48/48 |
| 31/31 |
| 21/21 |
| Active urine sediment N/% | 92/92 |
| Hypertension N/% | 28/28 |
| Serum albumin (g/dL) mean ± SD | 3.1 ± 0.8 |
| Serum Cr (mg/dL) median(IQR) | 0.8(0.5) |
| eGFR (mL/min/1.73 m2) median(IQR) | 94.5(50) |
| 75/75 |
| 14/14 |
| 11/11 |
| LN class | |
| 28/28 |
| 47/47 |
| 9/9 |
| 16/16 |
| Number of crescents median(IQR) | 2(4) |
| Activity Index median(IQR) | 10(6) |
| Chronicity Index median(IQR) | 2(2) |
| Interstitial fibrosis/tubular atrophy *,3 | |
| 85/87 |
| 13/13 |
| Induction Treatment | |
| 27/27 |
| 69/69 |
| 3/3 |
| 1/1 |
| Maintenance Treatment | |
| 77/77 |
| 8/8 |
| 5/5 |
| 10/10 |
| Duration of total treatment (months)median(IQR) | 39(38) |
| Variables | Univariate Models | Multivariate Model | ||
|---|---|---|---|---|
| HR | 95% Cis (p-Value) | HR | 95% Cis (p-Value) | |
| Age (years) | 1.01 | 0.98, 1.02 (0.53) | ||
| Sex | ||||
| Reference Group | |||
| 1.29 | 0.73, 2.29 (0.36) | ||
| Time from SLE diagnosis to LN (years) | 0.98 | 0.94, 1.03 (0.6) | ||
| Hypertension | ||||
| Reference Group | |||
| 0.7 | 0.43, 1.16 (0.18) | ||
| Low C3 | ||||
| Reference Group | |||
| 0.73 | 0.40, 1.33 (0.31) | ||
| Low C4 | ||||
| Reference Group | |||
| 0.68 | 0.4, 1.15 (0.15) | ||
| Anti-dsDNA antibodies | ||||
| Reference Group | |||
| 1.26 | 0.7, 2.32 (0.44) | ||
| eGFR at diagnosis(mL/min/1.73 m2) | ||||
| Reference Group | |||
| 0.66 | 0.39, 1.13 (0.13) | ||
| Proteinuria at diagnosis (g/day) | ||||
| Reference Group | |||
| 1.77 | 1.10, 2.84 (0.01) | ||
| LN class | ||||
| Reference Group | |||
| 0.87 | 0.5, 1.47 (0.62) | ||
| 0.69 | 0.37, 1.31 (0.26) | ||
| Number of Crescents | 0.97 | 0.93, 1.01 (0.24) | ||
| Activity Index | 1 | 0.96, 1.05 (0.75) | ||
| Chronicity Index | 0.92 | 0.82, 1.04 (0.19) | ||
| Interstitial fibrosis/Tubular atrophy | ||||
| Reference Group | |||
| 0.82 | 0.39, 1.72 (0.61) | ||
| Induction treatment ** | ||||
| Reference Group | |||
| 0.92 | 0.55, 1.56 (0.78) | ||
| Variables | Univariate Models | Multivariate Model | ||
|---|---|---|---|---|
| OR | 95% CIs (p-Value) | OR | 95% CIs (p-Value) | |
| Age (years) | 0.95 | 0.92, 0.98 (0.02) | 0.98 | 0.94, 1.03 (0.58) |
| Sex | ||||
| Reference Group | |||
| 0.5 | 0.19, 1.42 (0.2) | ||
| Time from SLE diagnosis to LN (years) | 0.93 | 0.84, 1.04 (0.23) | ||
| Hypertension | ||||
| Reference Group | |||
| 0.96 | 0.37, 2.47 (0.94) | ||
| Low C3 | ||||
| Reference Group | |||
| 0.9 | 0.29, 2.96 (0.9) | ||
| Low C4 | ||||
| Reference Group | |||
| 0.3 | 0.09, 0.99 (0.05) | ||
| Anti-dsDNA antibodies | ||||
| Reference Group | |||
| 0.96 | 0.29, 3.1 (0.94) | ||
| eGFR at diagnosis (mL/min/1.73 m2) | ||||
| Reference Group | |||
| 0.7 | 0.27, 1.98 (0.5) | ||
| Proteinuria at diagnosis (g/day) | ||||
| Reference Group | |||
| 3 | 1.14, 7.89 (0.02) | ||
| LN class | ||||
| Reference Group | |||
| 0.59 | 0.22, 1.55 (0.28) | 0.38 | 0.09, 1.6 (0.19) |
| 0.21 | 0.05, 0.8 (0.02) | 0.13 | 0.01, 0.8 (0.02) |
| Number of Crescents | 0.96 | 0.88, 1.05 (0.44) | ||
| Activity Index | 1.01 | 0.91, 1.11 (0.8) | ||
| Chronicity Index | 0.77 | 0.59, 1.01 (0.06) | ||
| Interstitial fibrosis/Tubular atrophy | ||||
| Reference Group | |||
| 0.6 | 0.15, 2.4 (0.48) | ||
| Induction treatment ** | ||||
| Reference Group | |||
| 0.25 | 0.08, 0.8 (0.02) | 0.14 | 0.03, 0.7 (0.01) |
| Time to PR (months) | 1.14 | 1.02, 1.26 (0.01) | ||
| Time to CR (months) | 1.05 | 1.01, 1.1 (0.01) | ||
| Time to CR/PR (months) | 1.11 | 1.02, 1.21 (0.01) | ||
| Proteinuria at 12 m (g/day) | ||||
| Reference Group | |||
| 3.38 | 1.14, 10 (0.02) | 4.12 | 1.15, 14 (0.02) |
| Variables | Univariate Models | Multivariate Model | ||
|---|---|---|---|---|
| OR | 95% CIs (p-Value) | OR | 95% CIs (p-Value) | |
| Age (years) | 1 | 0.96, 1.03 (0.9) | ||
| Sex | ||||
| Reference Group | |||
| 0.8 | 0.2, 2.5 (0.7) | ||
| Time from SLE diagnosis to LN (years) | 1 | 0.9, 1.1 (0.9) | ||
| Hypertension | ||||
| Reference Group | |||
| 2.28 | 0.83, 6.2 (0.1) | ||
| Low C3 | ||||
| Reference Group | |||
| 0.75 | 0.2, 3 (0.68) | ||
| Low C4 | ||||
| Reference Group | |||
| 1.6 | 0.53, 4.9 (0.4) | ||
| Anti-dsDNA antibodies | ||||
| Reference Group | |||
| 0.45 | 0.1, 1.5 (0.2) | ||
| eGFR at diagnosis (mL/min/1.73 m2) | ||||
| Reference Group | |||
| 6 | 2, 16 (0.001) | ||
| Proteinuria at diagnosis (g/day) | ||||
| Reference Group | |||
| 1.7 | 0.56, 5.12 (0.34) | ||
| LN class | ||||
| Reference Group | |||
| 0.59 | 0.19, 1.77 (0.34) | ||
| 0.62 | 0.17, 2.24 (0.47) | ||
| Number of Crescents | 1 | 0.93, 1.07 (0.91) | ||
| Activity Index | 1.03 | 0.92, 1.16 (0.5) | ||
| Chronicity Index | 1.13 | 0.87, 1.47 (0.34) | ||
| Interstitial fibrosis/Tubular atrophy | ||||
| Reference Group | |||
| 5.44 | 1.59, 18 (0.007) | 7.7 | 1.48, 40 (0.01) |
| Induction treatment ** | ||||
| Reference Group | |||
| 1.02 | 0.35, 3 (0.95) | ||
| Time to PR (months) | 1.14 | 1.04, 1.26 (0.006) | ||
| Time to CR (months) | 1.04 | 0.99, 1.1 (0.1) | ||
| Time to CR/PR (months) | 1.1 | 1.02, 1.2 (0.01) | ||
| Proteinuria at 12 m (g/day) | ||||
| Reference Group | |||
| 9.5 | 1.84, 20 (0.003) | 10.8 | 2.7, 42 (0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapsia, E.; Marinaki, S.; Michelakis, I.; Liapis, G.; Sfikakis, P.P.; Boletis, J.; Tektonidou, M.G. Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort. J. Clin. Med. 2022, 11, 5017. https://doi.org/10.3390/jcm11175017
Kapsia E, Marinaki S, Michelakis I, Liapis G, Sfikakis PP, Boletis J, Tektonidou MG. Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort. Journal of Clinical Medicine. 2022; 11(17):5017. https://doi.org/10.3390/jcm11175017
Chicago/Turabian StyleKapsia, Eleni, Smaragdi Marinaki, Ioannis Michelakis, George Liapis, Petros P. Sfikakis, John Boletis, and Maria G. Tektonidou. 2022. "Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort" Journal of Clinical Medicine 11, no. 17: 5017. https://doi.org/10.3390/jcm11175017
APA StyleKapsia, E., Marinaki, S., Michelakis, I., Liapis, G., Sfikakis, P. P., Boletis, J., & Tektonidou, M. G. (2022). Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort. Journal of Clinical Medicine, 11(17), 5017. https://doi.org/10.3390/jcm11175017