
Retinal Vascular Occlusion after COVID-19 Vaccination: More Coincidence than Causal Relationship? Data from a Retrospective Multicentre Study
 , ,
, ,  ,
,  , , , , ,
, , , , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
Statistics
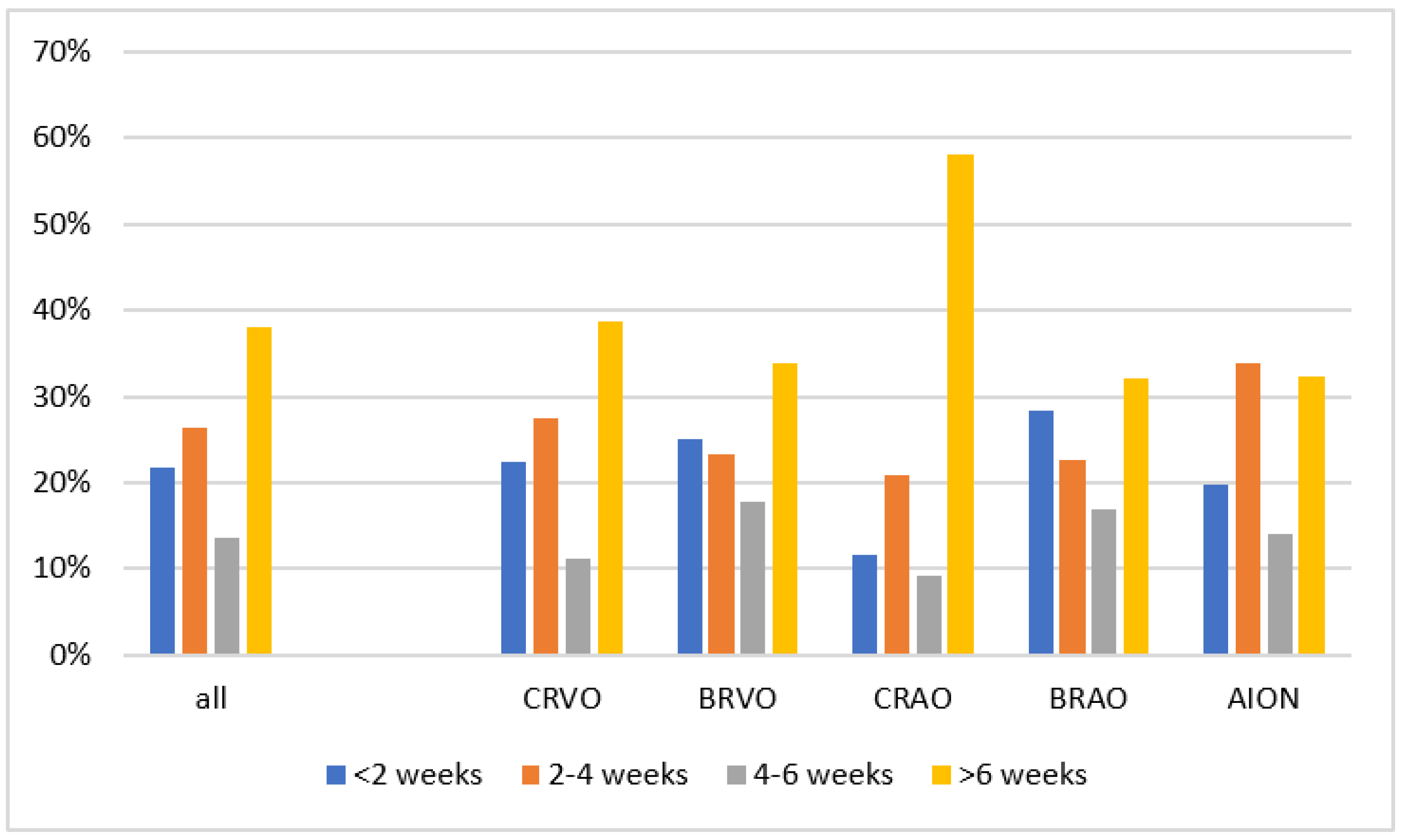
- Case-by-case analysis (descriptive case-only study): Herein, we descriptively investigated the time-dependent accumulation of COVID-19 vaccinations prior to RVOD disease—more specifically, whether there were more patients who received a COVID-19 vaccination shortly before the RVOD disease.
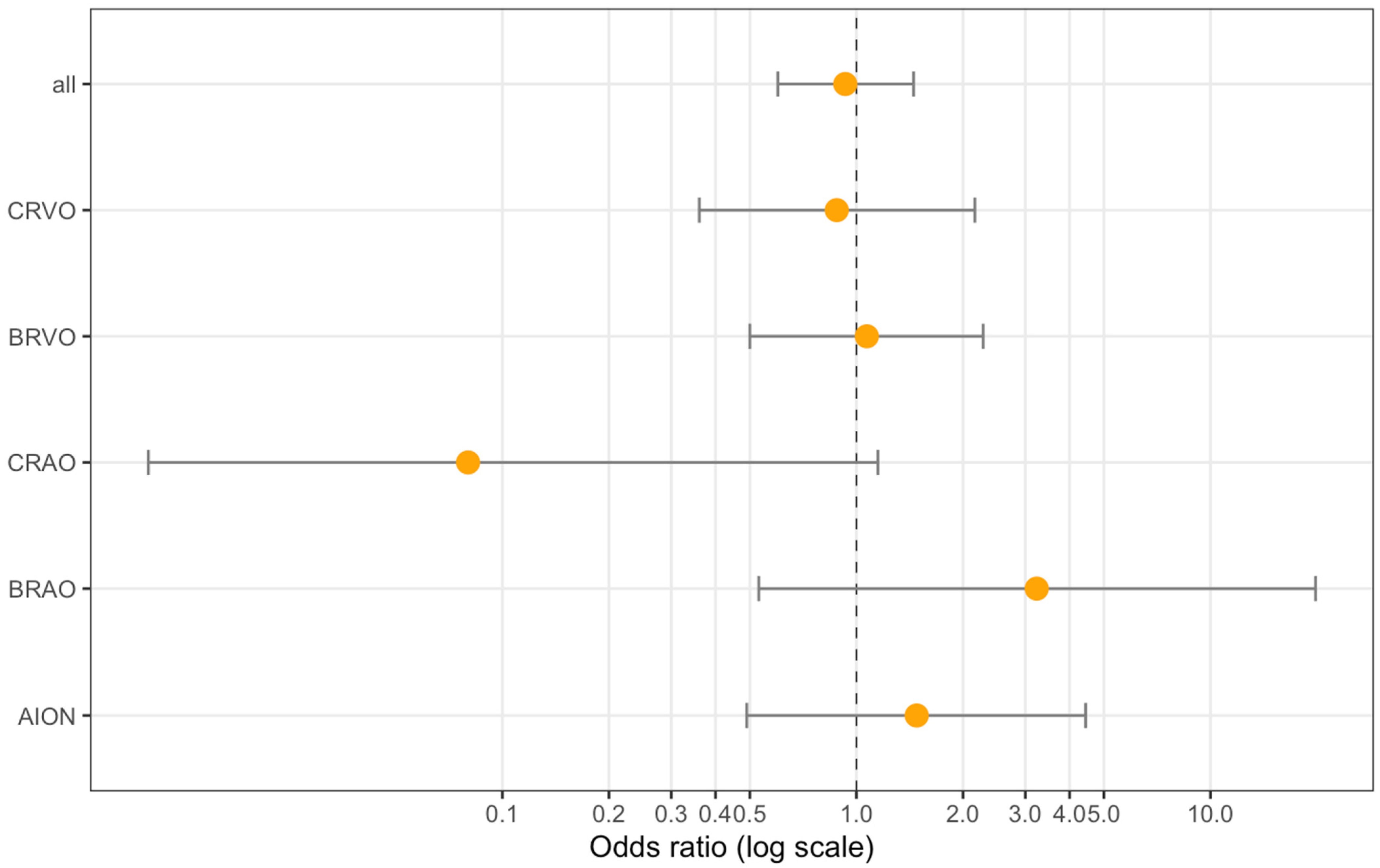
- Case–control study: In this analysis, we compared the odds of being vaccinated in the last four weeks among patients with RVOD (cases) to controls from the general population recruited by the Gutenberg Health Study (GHS) (age ±5 years and sex-matched). The recruitment of the controls took place between August 2021 and November 2021 (N = 939). For each control, the vaccination status within the 4 weeks prior to the date of the RVOD diagnosis of the corresponding case was analysed and believed not to be affected by the shift in recruitment time. A conditional logistic regression analysis was computed in (I) an unadjusted way and (II) adjusted for obesity (BMI ≥ 30), diabetes, arterial hypertension, smoking, and use of anticoagulation. All RVOD cases were analysed, as were the different entities of retinal vascular occlusions separately. A sensitivity analysis with cases presenting <2 weeks after symptoms onset was carried out.
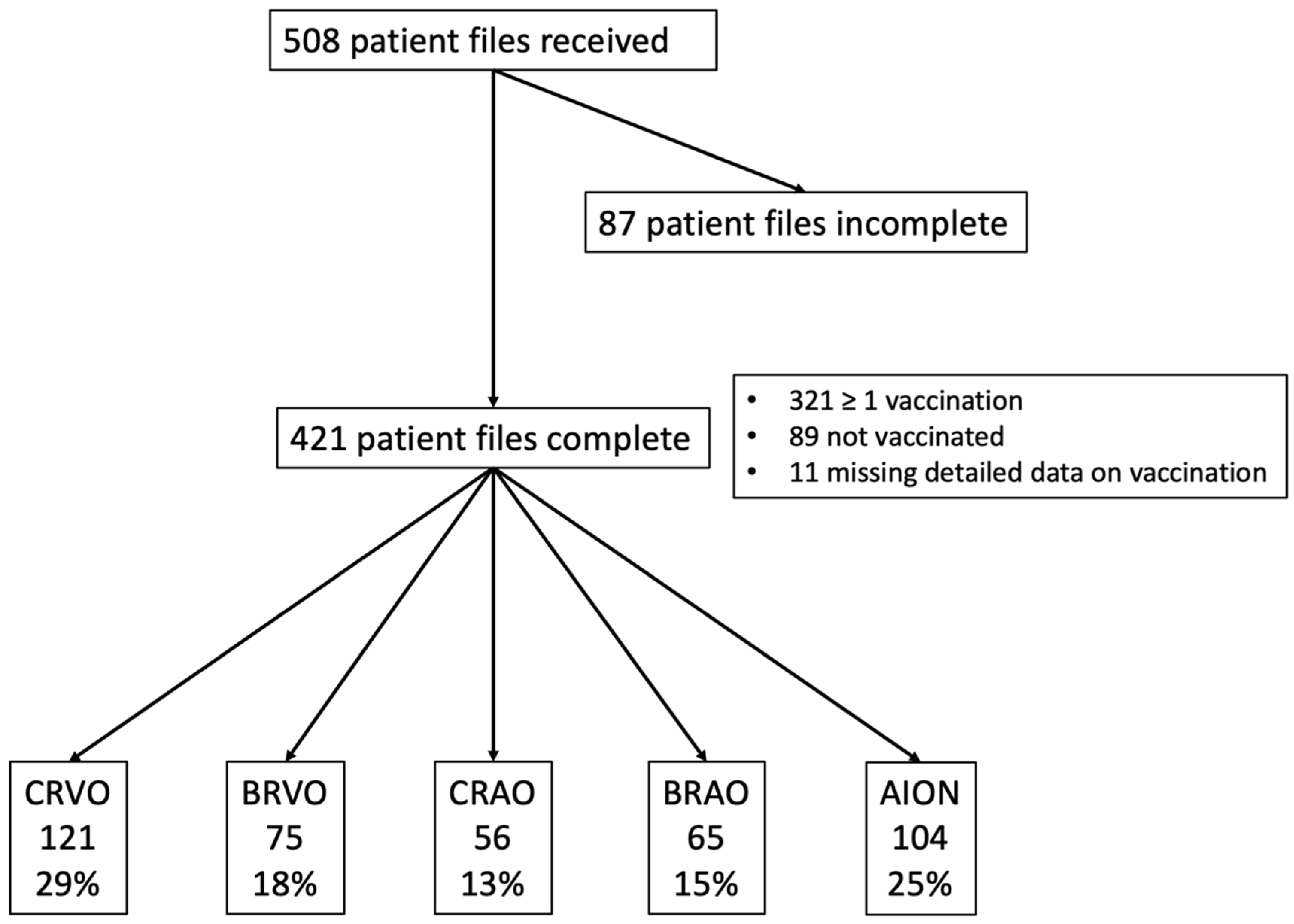
3. Results
3.1. Case-by-Case Analysis
3.2. Case–Control Analysis with Data from the Gutenberg Health Study
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schulz, J.B.; Berlit, P.; Diener, H.; Gerloff, C.; Greinacher, A.; Klein, C.; Petzold, G.C.; Piccininni, M.; Poli, S.; Röhrig, R.; et al. COVID-19 Vaccine-Associated Cerebral Venous Thrombosis in Germany. Ann. Neurol. 2021, 90, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Ng, X.L.; Betzler, B.K.; Testi, I.; Ho, S.L.; Tien, M.; Ngo, W.K.; Zierhut, M.; Chee, S.P.; Gupta, V.; Pavesio, C.E.; et al. Ocular Adverse Events After COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 1216–1224. [Google Scholar] [CrossRef] [PubMed]
- Sen, M.; Honavar, S.G. After the Storm: Ophthalmic Manifestations of COVID-19 Vaccines. Indian J. Ophthalmol. 2021, 69, 3398–3420. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Seo, M.-H.; Choi, K.-E.; Lee, S.; Choi, B.; Yun, C.; Kim, S.-W.; Kim, Y.Y. Vision-Threatening Ocular Adverse Events after Vaccination against Coronavirus Disease 2019. J. Clin. Med. 2022, 11, 3318. [Google Scholar] [CrossRef]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Marietta, M.; Coluccio, V.; Luppi, M. COVID-19, coagulopathy and venous thromboembolism: More questions than answers. Intern. Emerg. Med. 2020, 15, 1375–1387. [Google Scholar] [CrossRef]
- Gross, O.; Moerer, O.; Weber, M.; Huber, T.B.; Scheithauer, S. COVID-19-associated nephritis: Early warning for disease severity and complications? Lancet Lond. Engl. 2020, 395, e87–e88. [Google Scholar] [CrossRef]
- Becker, R.C. COVID-19 update: Covid-19-associated coagulopathy. J. Thromb. Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef]
- Marchetti, M. COVID-19-driven endothelial damage: Complement, HIF-1, and ABL2 are potential pathways of damage and targets for cure. Ann. Hematol. 2020, 99, 1701–1707. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet Lond. Engl. 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Hazell, L.; Shakir, S.A.W. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Ferner, R.E.; Stevens, R.J.; Anton, C.; Aronson, J.K. Spontaneous Reporting to Regulatory Authorities of Suspected Adverse Drug Reactions to COVID-19 Vaccines Over Time: The Effect of Publicity. Drug Saf. 2022, 45, 137–144. [Google Scholar] [CrossRef]
- Robert-Koch-Institute Table with Reported Vaccinations in Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquoten-Tab.html (accessed on 17 February 2022).
- Wild, P.S.; Zeller, T.; Beutel, M.; Blettner, M.; Dugi, K.A.; Lackner, K.J.; Pfeiffer, N.; Münzel, T.; Blankenberg, S. The Gutenberg Health Study. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 824–829. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Guemes-Villahoz, N.; Burgos-Blasco, B.; Vidal-Villegas, B.; Donate-López, J.; de la Muela, M.H.; López-Guajardo, L.; Martín-Sánchez, F.J.; García-Feijoó, J. Reduced macular vessel density in COVID-19 patients with and without associated thrombotic events using optical coherence tomography angiography. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Graefes Arch. Klin. Exp. Ophthalmol. 2021, 259, 2243–2249. [Google Scholar] [CrossRef]
- Hohberger, B.; Ganslmayer, M.; Lucio, M.; Kruse, F.; Hoffmanns, J.; Moritz, M.; Rogge, L.; Heltmann, F.; Szewczykowski, C.; Fürst, J.; et al. Retinal Microcirculation as a Correlate of a Systemic Capillary Impairment After Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Front. Med. 2021, 8, 676554. [Google Scholar] [CrossRef]
- Abrishami, M.; Emamverdian, Z.; Shoeibi, N.; Omidtabrizi, A.; Daneshvar, R.; Saeidi Rezvani, T.; Saeedian, N.; Eslami, S.; Mazloumi, M.; Sadda, S.; et al. Optical coherence tomography angiography analysis of the retina in patients recovered from COVID-19: A case-control study. Can. J. Ophthalmol. J. Can. Ophtalmol. 2021, 56, 24–30. [Google Scholar] [CrossRef]
- Girbardt, C.; Busch, C.; Al-Sheikh, M.; Gunzinger, J.M.; Invernizzi, A.; Xhepa, A.; Unterlauft, J.D.; Rehak, M. Retinal Vascular Events after mRNA and Adenoviral-Vectored COVID-19 Vaccines-A Case Series. Vaccines 2021, 9, 1349. [Google Scholar] [CrossRef]
- Da Silva, L.S.C.; Finamor, L.P.S.; Andrade, G.C.; Lima, L.H.; Zett, C.; Muccioli, C.; Sarraf, E.P.; Marinho, P.M.; Peruchi, J.; Oliveira, R.D.d.L.; et al. Vascular retinal findings after COVID-19 vaccination in 11 cases: A coincidence or consequence? Arq. Bras. Oftalmol. 2022, 85, 158–165. [Google Scholar] [CrossRef]
- Lee, S.; Sankhala, K.K.; Bose, S.; Gallemore, R.P. Combined Central Retinal Artery and Vein Occlusion with Ischemic Optic Neuropathy After COVID-19 Vaccination. Int. Med. Case Rep. J. 2022, 15, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Xu, Y.; Zha, M.; Zhang, Y.; Rudan, I. Global epidemiology of retinal vein occlusion: A systematic review and meta-analysis of prevalence, incidence, and risk factors. J. Glob. Health 2019, 9, 010427. [Google Scholar] [CrossRef] [PubMed]
- Pick, J.; Nickels, S.; Saalmann, F.; Finger, R.P.; Schuster, A.K. Incidence of retinal artery occlusion in Germany. Acta Ophthalmol. (Copenh.) 2020, 98, e656–e657. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.; Lin, W.V.; Sadaka, A.; Lee, A.G. Nonarteritic anterior ischemic optic neuropathy: Cause, effect, and management. Eye Brain 2017, 9, 23–28. [Google Scholar] [CrossRef]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G.-S. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology 2020, 127, P259–P287. [Google Scholar] [CrossRef]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G.-S. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology 2020, 127, P288–P320. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Garcia-Arumi, J.; Gerendas, B.S.; Midena, E.; Sivaprasad, S.; Tadayoni, R.; Wolf, S.; Loewenstein, A. Guidelines for the Management of Retinal Vein Occlusion by the European Society of Retina Specialists (EURETINA). Ophthalmol. J. Int. Ophtalmol. Int. J. Ophthalmol. Z. Augenheilkd. 2019, 242, 123–162. [Google Scholar] [CrossRef]
- Hong, J.-H.; Sohn, S.-I.; Kwak, J.; Yoo, J.; Ahn, S.J.; Woo, S.J.; Jung, C.; Yum, K.S.; Bae, H.-J.; Chang, J.Y.; et al. Retinal artery occlusion and associated recurrent vascular risk with underlying etiologies. PLoS ONE 2017, 12, e0177663. [Google Scholar] [CrossRef]
- Callizo, J.; Feltgen, N.; Ammermann, A.; Ganser, J.; Bemme, S.; Bertelmann, T.; Pfeiffer, S.; Duvinage, A.; Gröschel, K.; Hoerauf, H.; et al. Atrial fibrillation in retinal vascular occlusion disease and non-arteritic anterior ischemic optic neuropathy. PLoS ONE 2017, 12, e0181766. [Google Scholar] [CrossRef]
- Callizo, J.; Feltgen, N.; Pantenburg, S.; Wolf, A.; Neubauer, A.S.; Jurklies, B.; Wachter, R.; Schmoor, C.; Schumacher, M.; Junker, B.; et al. Cardiovascular Risk Factors in Central Retinal Artery Occlusion: Results of a Prospective and Standardized Medical Examination. Ophthalmology 2015, 122, 1881–1888. [Google Scholar] [CrossRef]
- Umeya, R.; Yoshida, Y.; Ono, K. Impact of retinal vein occlusion on cardiovascular events in elderly Japanese patients. Medicine 2021, 100, e28424. [Google Scholar] [CrossRef]
- Christiansen, C.B.; Torp-Pedersen, C.; Olesen, J.B.; Gislason, G.; Lamberts, M.; Carlson, N.; Buron, M.; Juul, N.; Lip, G.Y.H. Risk of incident atrial fibrillation in patients presenting with retinal artery or vein occlusion: A nationwide cohort study. BMC Cardiovasc. Disord. 2018, 18, 91. [Google Scholar] [CrossRef]
- Bertelsen, M.; Linneberg, A.; Rosenberg, T.; Christoffersen, N.; Vorum, H.; Gade, E.; Larsen, M. Comorbidity in patients with branch retinal vein occlusion: Case-control study. BMJ 2012, 345, e7885. [Google Scholar] [CrossRef]
- Neuhauser, H.; Diederichs, C.; Boeing, H.; Felix, S.B.; Jünger, C.; Lorbeer, R.; Meisinger, C.; Peters, A.; Völzke, H.; Weikert, C.; et al. Hypertension in Germany. Dtsch. Arztebl. Int. 2016, 113, 809–815. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Johannsen, S.S.; Wild, P.S.; Blankenberg, S. Prevalence and risk factors of atrial fibrillation in Germany: Data from the Gutenberg Health Study. Herz 2015, 40, 8–15. [Google Scholar] [CrossRef]
- Schmitt, V.H.; Leuschner, A.; Jünger, C.; Pinto, A.; Hahad, O.; Schulz, A.; Arnold, N.; Tröbs, S.-O.; Panova-Noeva, M.; Keller, K.; et al. Cardiovascular profiling in the diabetic continuum: Results from the population-based Gutenberg Health Study. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2021, 111, 272–283. [Google Scholar] [CrossRef]
- Zeiher, J.; Finger, J.D.; Kuntz, B.; Hoebel, J.; Lampert, T.; Starker, A. Trends in smoking among adults in Germany. Evidence from seven population-based health surveys from 1991–2015. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 1365–1376. [Google Scholar] [CrossRef]
- Radtke, R. Rauchen—Statistiken und Zahlen. 2022. Available online: https://de.statista.com/themen/150/rauchen/#topicHeader__wrapper (accessed on 20 February 2022).
- Eckstein, H.H.; Kühnl, A.; Berkefeld, J.; Dörfler, A.; Kopp, I.; Langhoff, R.; LAwall, H.; Ringleb, P.; Sander, D.; Storck, M.; et al. S3-Leitlinie zur Diagnostik, Therapie und Nachsorge der Extracraniellen Carotisstenose, 2nd ed.; Association of the Scientific Medical Societies in Germany: Frankfurt, Germany, 2020; AWMF register number: 004-028. [Google Scholar]
- Hattenbach, L.-O.; Heinz, P.; Feltgen, N.; Hoerauf, H.; Kohnen, T.; Priglinger, S.; Bachmann, W.; Rieks, J.; Eter, N.; Reinhard, T. Impact of the SARS-CoV-2 pandemic on ophthalmic care in Germany. Ophthalmol. Z. Dtsch. Ophthalmol. Ges. 2021, 118, 166–175. [Google Scholar] [CrossRef]
- Al-Moujahed, A.; Boucher, N.; Fernando, R.; Saroj, N.; Vail, D.; Rosenblatt, T.R.; Moshfeghi, D.M. Incidence of Retinal Artery and Vein Occlusions During the COVID-19 Pandemic. Ophthalmic Surg. Lasers Imaging Retin. 2022, 53, 22–30. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Robert-Koch-Institut Übergewicht und Adipositas. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Themen/Uebergewicht_Adipositas/Uebergewicht_Adipositas_node.html (accessed on 17 June 2022).




{kind=link}
{kind=link}
{kind=link}
| All | CRVO | BRVO | CRAO | BRAO | AION | |
|---|---|---|---|---|---|---|
| n | 421 | 121 | 75 | 56 | 65 | 104 |
| Age (years) | 67.6 ± 14.6 | 65.6 ± 16.0 | 65.4 ± 13.5 | 74.5 ± 9.9 | 67.3 ± 17.0 | 68.0 ± 13.2 |
| Sex (female) (%) | 51.8 | 49.6 | 41.3 | 58.9 | 55.4 | 55.8 |
| Eye (OS) (%) | 49.0 | 51.2 | 49.3 | 39.3 | 60.0 | 44.7 |
| Time point of presentation at eye clinics after onset of symptoms (% of patients) | ||||||
| <2 weeks | 76.7 | 74.8 | 62.9 | 96.4 | 88.5 | 70.4 |
| 2–4 weeks | 11.0 | 11.3 | 14.3 | - | 4.9 | 18.4 |
| 4–6 weeks | 2.5 | 1.7 | 7.1 | 3.6 | 1.6 | 2.0 |
| >6 weeks | 9.8 | 12.2 | 15.7 | - | 4.9 | 9.2 |
| Ophthalmological data | ||||||
| Visual acuity diseased eye (LogMAR; median and interquartile range) | 0.40 (0.10–1.30) | 0.50 (0.20–1.00) | 0.35 (0.10–0.70) | 2.27 (1.15–2.27) | 0.20 (0.10–0.80) | 0.35 (0.10–1.23) |
| Visual acuity fellow eye (LogMAR) | 0.10 (0.00–0.30) | 0.10 (0.00–0.40) | 0.10 (0.00–0.20) | 0.10 (0.00–0.20) | 0.10 (0.00–0.20) | 0.20 (0.00–0.38) |
| Glaucoma (yes) (%) | 10.7 | 15.0 | 12.5 | 7.4 | 7.8 | 7.9 |
| Systemic risk factors | ||||||
| Arterial hypertension (yes) (%) | 64.5 | 58.3 | 60.0 | 85.5 | 54.7 | 69.9 |
| Diabetes (yes) (%) | 18.0 | 10.8 | 13.7 | 20.4 | 15.6 | 30.0 |
| Obesity (yes) (%) | 14.3 | 8.5 | 9.6 | 18.5 | 11.1 | 24.2 |
| Smoking (yes) (%) | 12.3 | 9.4 | 12.2 | 23.2 | 17.5 | 6.8 |
| Carotid artery stenosis (yes) (%) | 18.4 | 10.1 | 6.9 | 29.6 | 20.9 | 27.0 |
| Atrial fibrillation (yes) (%) | 11.7 | 14.2 | 8.2 | 14.8 | 12.7 | 9.1 |
| Anticoagulation (yes) (%) | ||||||
| All | 39.7 | 32.2 | 23.5 | 61.1 | 50.0 | 41.8 |
| Direct oral anticoagulants (DOAC) | 11.4 | 9.3 | 5.9 | 16.7 | 15.6 | 12.2 |
| Vitamin-K-dependent drugs | 2.2 | 3.4 | 1.5 | 3.7 | 0 | 2.0 |
| Acetylsalicylic acid (ASA) | 22.6 | 18.6 | 13.2 | 35.2 | 28.1 | 23.5 |
| combination | 3.5 | 0.8 | 2.9 | 5.6 | 6.2 | 4.1 |
| Prior COVID-19 infection (%) | 1.9 | 0.9 | 0 | 2.1 | 3.2 | 3.3 |
| RVOD Cases | Controls | ||
|---|---|---|---|
| Vaccination within the last 4 weeks | No | 191 | 202 |
| YES | 136 | 125 | |
| overall | 327 | 327 |
| Crude | Adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| n | OR | 95% CI | p-Value | n | OR | 95% CI | p-Value | |
| all | 654 | 1.15 | 0.84–1.58 | 0.38 | 506 | 0.93 | 0.60–1.45 | 0.75 |
| CRVO | 186 | 1.53 | 0.86–2.72 | 0.15 | 141 | 0.88 | 0.36–2.16 | 0.78 |
| BRVO | 126 | 1.06 | 0.55–2.05 | 0.87 | 106 | 1.07 | 0.50–2.28 | 0.98 |
| CRAO | 78 | 0.21 | 0.06–0.75 | 0.02 | 65 | 0.08 | 0.01–1.15 | 0.06 |
| BRAO | 94 | 1.86 | 0.74–4.66 | 0.19 | 72 | 3.23 | 0.53–19.8 | 0.21 |
| AION | 170 | 1.31 | 0.68–2.52 | 0.41 | 127 | 1.48 | 0.49–4.44 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feltgen, N.; Ach, T.; Ziemssen, F.; Quante, C.S.; Gross, O.; Abdin, A.D.; Aisenbrey, S.; Bartram, M.C.; Blum, M.; Brockmann, C.; et al. Retinal Vascular Occlusion after COVID-19 Vaccination: More Coincidence than Causal Relationship? Data from a Retrospective Multicentre Study. J. Clin. Med. 2022, 11, 5101. https://doi.org/10.3390/jcm11175101
Feltgen N, Ach T, Ziemssen F, Quante CS, Gross O, Abdin AD, Aisenbrey S, Bartram MC, Blum M, Brockmann C, et al. Retinal Vascular Occlusion after COVID-19 Vaccination: More Coincidence than Causal Relationship? Data from a Retrospective Multicentre Study. Journal of Clinical Medicine. 2022; 11(17):5101. https://doi.org/10.3390/jcm11175101
Chicago/Turabian StyleFeltgen, Nicolas, Thomas Ach, Focke Ziemssen, Carolin Sophie Quante, Oliver Gross, Alaa Din Abdin, Sabine Aisenbrey, Martin C. Bartram, Marcus Blum, Claudia Brockmann, and et al. 2022. "Retinal Vascular Occlusion after COVID-19 Vaccination: More Coincidence than Causal Relationship? Data from a Retrospective Multicentre Study" Journal of Clinical Medicine 11, no. 17: 5101. https://doi.org/10.3390/jcm11175101
APA StyleFeltgen, N., Ach, T., Ziemssen, F., Quante, C. S., Gross, O., Abdin, A. D., Aisenbrey, S., Bartram, M. C., Blum, M., Brockmann, C., Dithmar, S., Friedrichs, W., Guthoff, R., Hattenbach, L. -O., Herrlinger, K. R., Kaskel-Paul, S., Khoramnia, R., Klaas, J. E., Krohne, T. U., ... Schuster, A. K. (2022). Retinal Vascular Occlusion after COVID-19 Vaccination: More Coincidence than Causal Relationship? Data from a Retrospective Multicentre Study. Journal of Clinical Medicine, 11(17), 5101. https://doi.org/10.3390/jcm11175101