


Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review

 ,
,  ,
,  , ,
, ,  , ,
, ,  ,
,
Abstract
:1. Introduction
- Assess the prevalence of the viruses mentioned above (except for HCV) in OLP lesions;
- Evaluate whether any clinical features correlate with the viruses;
- Evaluate if there is any relationship between malignant transformation in OLP and viral infection.
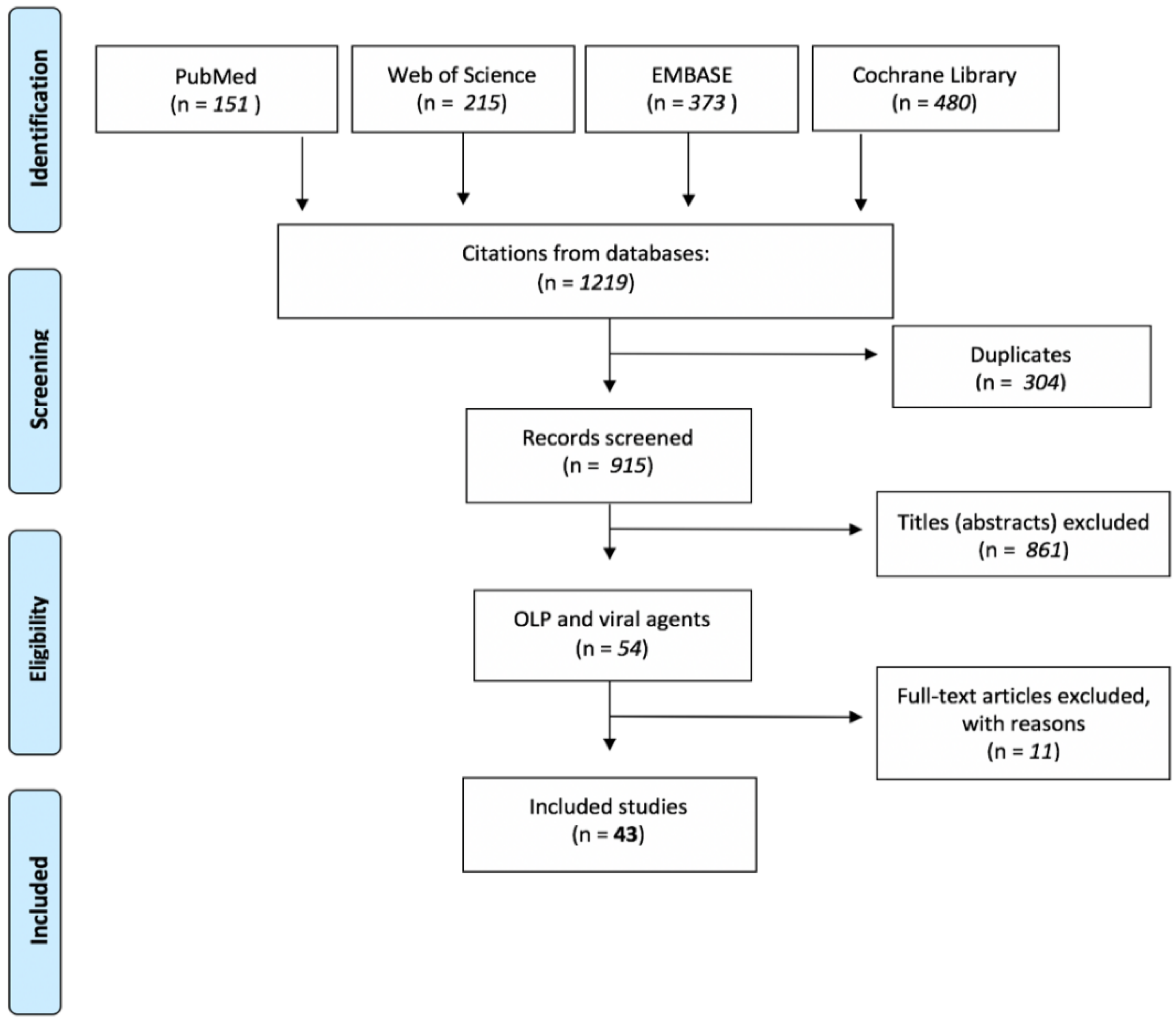
2. Materials and Methods
3. Results
3.1. Risk of Bias in Individual Studies
3.2. HPV
3.3. EBV
3.4. HSV-1
3.5. CMV
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Payeras, M.R.; Cherubini, K.; Figueiredo, M.A.; Salum, F.G. Oral Lichen Planus: Focus on Etiopathogenesis. Arch. Oral Biol. 2013, 58, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.B.; Kumar, S.K.S.; Zain, R.B. Oral Lichen Planus and Lichenoid Reactions: Etiopathogenesis, Diagnosis, Management and Malignant Transformation. J. Oral Sci. 2007, 49, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.-L.; Fan, M.-W.; Wang, S.-Z.; Chen, X.-M.; Li, Y.; Wang, L. A Clinical Study of 674 Patients with Oral Lichen Planus in China. J. Oral Pathol. Med. 2005, 34, 467–472. [Google Scholar] [CrossRef]
- Andreasen, J.O. Oral Lichen Planus. 1. A Clinical Evaluation of 115 Cases. Oral Surg. Oral Med. Oral Pathol. 1968, 25, 31–42. [Google Scholar] [CrossRef]
- Eisen, D. The Clinical Features, Malignant Potential, and Systemic Associations of Oral Lichen Planus: A Study of 723 Patients. J. Am. Acad. Dermtol. 2002, 46, 207–214. [Google Scholar] [CrossRef]
- Gandolfo, S.; Richiardi, L.; Carrozzo, M.; Broccoletti, R.; Carbone, M.; Pagano, M.; Vestita, C.; Rosso, S.; Merletti, F. Risk of Oral Squamous Cell Carcinoma in 402 Patients with Oral Lichen Planus: A Follow-up Study in an Italian Population. Oral Oncol. 2004, 40, 77–83. [Google Scholar] [CrossRef]
- van der Meij, E.H.; Mast, H.; van der Waal, I. The Possible Premalignant Character of Oral Lichen Planus and Oral Lichenoid Lesions: A Prospective Five-Year Follow-up Study of 192 Patients. Oral Oncol. 2007, 43, 742–748. [Google Scholar] [CrossRef]
- van der Waal, I. Potentially Malignant Disorders of the Oral and Oropharyngeal Mucosa; Terminology, Classification and Present Concepts of Management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef]
- Landini, G.; Mylonas, P.; Shah, I.Z.; Hamburger, J. The Reported Rates of Transformation of Oral Lichen Planus. J. Oral Maxillofac Surg. Med. Pathol. 2014, 26, 213–220. [Google Scholar] [CrossRef]
- Lodi, G.; Scully, C.; Carrozzo, M.; Griffiths, M.; Sugerman, P.B.; Thongprasom, K. Current Controversies in Oral Lichen Planus: Report of an International Consensus Meeting. Part 1. Viral Infections and Etiopathogenesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2005, 100, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Dorrego, M.V.; Correnti, M.; Delgado, R.; Tapia, F.J. Oral Lichen Planus: Immunohistology of Mucosal Lesions. J. Oral Pathol. Med. 2002, 31, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, B.; Sengüven, B.; Demir, C. Prevalence of Herpes Simplex, Epstein Barr and Human Papilloma Viruses in Oral Lichen Planus. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e170–e174. [Google Scholar] [CrossRef] [PubMed]
- Sand, L.P.; Jalouli, J.; Larsson, P.-A.; Hirsch, J.-M. Prevalence of Epstein-Barr Virus in Oral Squamous Cell Carcinoma, Oral Lichen Planus, and Normal Oral Mucosa. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2002, 93, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Ghodratnama, F.; Wray, D.; Bagg, J. Detection of Serum Antibodies against Cytomegalovirus, Varicella Zoster Virus and Human Herpesvirus 6 in Patients with Recurrent Aphthous Stomatitis. J. Oral Pathol. Med. 2007, 28, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, S.; Lodi, G.; von Bültzingslöwen, I.; Aliko, A.; Arduino, P.; Campisi, G.; Challacombe, S.; Ficarra, G.; Flaitz, C.; Zhou, H.; et al. Human Papillomaviruses in Oral Carcinoma and Oral Potentially Malignant Disorders: A Systematic Review. Oral Dis. 2011, 17, 58–72. [Google Scholar] [CrossRef]
- Lodi, G.; Pellicano, R.; Carrozzo, M. Hepatitis C Virus Infection and Lichen Planus: A Systematic Review with Meta-Analysis. Oral Dis. 2010, 16, 601–612. [Google Scholar] [CrossRef]
- Petti, S.; Rabiei, M.; de Luca, M.; Scully, C. The Magnitude of the Association between Hepatitis C Virus Infection and Oral Lichen Planus: Meta-Analysis and Case Control Study. Odontology 2011, 99, 168–178. [Google Scholar] [CrossRef]
- di Stasio, D.; Lucchese, A.; Romano, A.; Elio Adinolfi, L.; Serpico, R.; Marrone, A. The Clinical Impact of Direct-Acting Antiviral Treatment on Patients Affected by Hepatitis C Virus-Related Oral Lichen Planus: A Cohort Study. Clin. Oral Investig. 2022, 26, 5409–5417. [Google Scholar] [CrossRef]
- Lucchese, A. A Potential Peptide Pathway from Viruses to Oral Lichen Planus. J. Med. Virol. 2015, 87, 1060–1065. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Romano, A.; di Stasio, D.; Gentile, E.; Petruzzi, M.; Serpico, R.; Lucchese, A. The Potential Role of Photodynamic Therapy in Oral Premalignant and Malignant Lesions: A Systematic Review. J. Oral Pathol. Med. 2021, 50, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, S.M.; Syrjänen, K.J.; Lamberg, M.A. Detection of Human Papillomavirus DNA in Oral Mucosal Lesions Using in Situ DNA-Hybridization Applied on Paraffin Sections. Oral Surg. Oral Med. Oral Pathol. 1986, 62, 660–667. [Google Scholar] [CrossRef]
- Maitland, N.; Cox, M.; Lynas, C.; Prime, S.; Meanwell, C.; Scully, C. Detection of Human Papillomavirus DNA in Biopsies of Human Oral Tissue. Br. J. Cancer 1987, 56, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Jontell, M.; Watts, S.; Wallstrom, M.; Levin, L.; Sloberg, K. Human Papilloma Virus in Erosive Oral Lichen Planus. J. Oral Pathol. Med. 1990, 19, 273–277. [Google Scholar] [CrossRef]
- Kashima, H.K.; Levin, L.S.; Kutcher, M.; de Villiers, E.-M.; Kessis, T.; Shah, K. Human Papillomavirus in Squamous Cell Carcinoma, Leukoplakia, Lichen Planus, and Clinically Normal Epithelium of the Oral Cavity. Ann. Otol. Rhinol. Laryngol. 1990, 99, 55–61. [Google Scholar] [CrossRef]
- Young, S.K.; Min, K.W. In Situ DNA Hybridization Analysis of Oral Papillomas, Leukoplakias, and Carcinomas for Human Papillomavirus. Oral Surg. Oral Med. Oral Pathol. 1991, 71, 726–729. [Google Scholar] [CrossRef]
- Miller, C.S.; White, D.K.; Royse, D.D. In Situ Hybridization Analysis of Human Papillomavirus in Orofacial Lesions Using a Consensus Biotinylated Probe. Am. J. Derm. 1993, 15, 256–259. [Google Scholar] [CrossRef]
- Cox, M.; Maitlan, N.; Scully, C. Human Herpes Simplex-1 and Papillomavirus Type 16 Homologous DNA Sequences in Normal, Potentially Malignant and Malignant Oral Mucosa. Eur. J. Cancer B Oral Oncol. 1993, 29, 215–219. [Google Scholar] [CrossRef]
- Wen, S.; Tsuji, T.; Li, X.; Mizugaki, Y.; Hayatsu, Y.; Shinozaki, F. Detection and Analysis of Human Papillomavirus 16 and 18 Homologous DNA Sequences in Oral Lesions. Anticancer Res. 1997, 17, 307–311. [Google Scholar]
- González-Moles, M.A.; Rodríguez-Archilla, A.; Ruiz Avila, I.; Esteban, F.; González-Moles, S.; Bravo, M. Presence of HPV 16 Sequences in Oral Lichen Planus Lesions. Bull. Group. Int. Rech. Sci. Stomatol. Odontol. 1998, 40, 92–97. [Google Scholar]
- Sand, L.; Jalouli, J.; Larsson, P.A.; Hirsch, J.M. Human Papilloma Viruses in Oral Lesions. Anticancer Res. 2000, 20, 1183–1188. [Google Scholar] [PubMed]
- Yaltirik, M.; Özveren, A.; Alatli, C.; Büyükakyüz, N. Detection of Human Papilloma Virus in Benign, Malignant and Pre-Cancerous Lesions of Oral Mucosa By in Situ Hybridization. Turk. J. Med. Sci. 2001, 31, 509–515. [Google Scholar]
- Giovannelli, L.; Campisi, G.; Lama, A.; Giambalvo, O.; Osborn, J.; Margiotta, V.; Ammatuna, P. Human Papillomavirus DNA in Oral Mucosal Lesions. J. Infect. Dis. 2002, 185, 833–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostwald, C.; Rutsatz, K.; Schweder, J.; Schmidt, W.; Gundlach, K.; Barten, M. Human Papillomavirus 6/11, 16 and 18 in Oral Carcinomas and Benign Oral Lesions. Med. Microbiol. Immunol. 2003, 192, 145–148. [Google Scholar] [CrossRef] [PubMed]
- ÓFlatharta, C.; Flint, S.R.; Toner, M.; Butler, D.; Mabruk, M.J.E.M.F. Investigation into a Possible Association Between Oral Lichen Planus, the Human Herpesviruses, and the Human Papillomaviruses. Mol. Diagn. 2003, 7, 73–83. [Google Scholar] [CrossRef]
- Campisi, G.; Giovannelli, L.; Aricò, P.; Lama, A.; di Liberto, C.; Ammatuna, P.; D’Angelo, M. HPV DNA in Clinically Different Variants of Oral Leukoplakia and Lichen Planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2004, 98, 705–711. [Google Scholar] [CrossRef]
- Giovannelli, L.; Campisi, G.; Colella, G.; Capra, G.; Liberto, C.D.; Caleca, M.P.; Matranga, D.; D’Angelo, M.; Muzio, L.L.; Ammatuna, P. Brushing of Oral Mucosa for Diagnosis of HPV Infection in Patients with Potentially Malignant and Malignant Oral Lesions. Mol. Diagn. 2006, 10, 49–55. [Google Scholar] [CrossRef]
- Zarei, M.R.; Moradie, A.; Hamkar, R.; Mohammadalizadeh, S.; Chamani, G.; Alizadeh, N.; Kakooei, S.; Eslami, B. Detection of Human Papillomavirus DNA Sequences in Oral Lesions Using Polymerase Chain Reaction. Acta Med. Iran. 2007, 45, 177–182. [Google Scholar]
- Debanth, S.; Singh, P.A.; Mehrotra, R.; Singh, M.; Gupta, S.C.; Pandya, S.; Chowdhury, A.; Singh, M. Human Papillomavirus Infection and Premalignant Lesions of the Oral Cavity: A Cross-Sectional Study in Allahabad, North India. Asia Pac. J. Clin. Oncol 2009, 5, 111–118. [Google Scholar] [CrossRef]
- Razavi, S.M.; Ghalayani, P.; Salehi, M.R.; Attarzadeh, H.; Shahmoradi, M. Human Papilloma Virus as a Possible Factor in the Pathogenesis of Oral Lichen Planus. Dent. Res. J. 2009, 6, 82–86. [Google Scholar]
- Mattila, R.; Rautava, J.; Syrjänen, S. Human Papillomavirus in Oral Atrophic Lichen Planus Lesions. Oral Oncol. 2012, 48, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Arirachakaran, P.; Chansaengroj, J.; Lurchachaiwong, W.; Kanjanabud, P.; Thongprasom, K.; Poovorawan, Y. Oral Lichen Planus in Thai Patients Has a Low Prevalence of Human Papillomavirus. ISRN Dent. 2013, 2013, 362750. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Kawai, R.; Isomura, M.; Sato, N.; Yoshida, W.; Kamiya, K.; Nagaya, Y.; Hattori, T.; Sato, E.; Sugita, Y.; et al. Human Papillomavirus in Oral Lichen Planus of Japanese Patients. J. Hard Tissue Biol. 2015, 24, 181–188. [Google Scholar] [CrossRef]
- Pol, C.A.; Ghige, S.K.; Gosavi, S.R. Role of Human Papilloma Virus-16 in the Pathogenesis of Oral Lichen Planus—An Immunohistochemical Study. Int. Dent. J. 2015, 65, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Sahebjamiee, M.; Sand, L.; Karimi, S.; Biettolahi, J.M.; Jabalameli, F.; Jalouli, J. Prevalence of Human Papillomavirus in Oral Lichen Planus in an Iranian Cohort. J. Oral Maxillofac. Pathol. 2015, 19, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Viguier, M.; Bachelez, H.; Poirier, B.; Kagan, J.; Battistella, M.; Aubin, F.; Touzé, A.; Carmagnat, M.; Francès, C.; Gougeon, M.-L.; et al. Peripheral and Local Human Papillomavirus 16–Specific CD8 + T-Cell Expansions Characterize Erosive Oral Lichen Planus. J. Investig. Dermatol. 2015, 135, 418–424. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, H.; Yang, X.; Li, X.; Shi, Y.; Niu, W.; Liu, T. Study on Expression of P16 and Human Papillomavirus 16 and 18 (E6) in OLP and Its Malignant Transformation. Pathol. Res. Pract. 2018, 214, 296–302. [Google Scholar] [CrossRef]
- Zendeli-Bedjeti, L. Human Papillomavirus as a Potential Risk Factor for Oral Premalignant Lesions. Acta Clin. Croat. 2017, 56, 369–374. [Google Scholar] [CrossRef]
- Gomez-Armayones, S.; Chimenos-Küstner, E.; Marí, A.; Tous, S.; Penin, R.; Clavero, O.; Quirós, B.; Pavon, M.A.; Taberna, M.; Alemany, L.; et al. Human Papillomavirus in Premalignant Oral Lesions: No Evidence of Association in a Spanish Cohort. PLoS ONE 2019, 14, e0210070. [Google Scholar] [CrossRef]
- Sameera, A.; Kotikalpudi, R.; Patel, R.K.; Reddy, K.K.; Prasanna, M.; Erugula, S.R. Molecular Detection of Human Papillomavirus DNA in Oral Lichen Planus Patients. J. Clin. Diagn. Res. 2019, 13, 20–24. [Google Scholar] [CrossRef]
- Farhadi, S.; Sadri, D.; Bandehpour, M.; Akbari, M.; Jafarzadeh, E.; Hashemi, M. Detection of Human Papillomavirus 33 in Erosive Oral Lichen Planus. Int. J. Cancer Manag. 2020, 13, e101488. [Google Scholar] [CrossRef]
- Kaewmaneenuan, N.; Lekawanvijit, S.; Pongsiriwet, S.; Chatupos, V.; Iamaroon, A. High Prevalence of Human Papillomavirus Type 18 in Oral Potentially Malignant Disorders in Thailand. Asian Pac. J. Cancer Prev. 2021, 22, 1875–1881. [Google Scholar] [CrossRef]
- della Vella, F.; Lauritano, D.; Pannone, G.; del Prete, R.; di Stasio, D.; Contaldo, M.; Petruzzi, M. Prevalence of HPV in Patients Affected by Oral Lichen Planus: A Prospective Study Using Two Different Chair-side Sampling Methods. J. Oral Pathol. Med. 2021, 50, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A. Abnormal EBV Immune Status in Oral Lichen Planus. Oral Dis. 1996, 2, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Cruz, I.; van den Brule, A.J.C.; Steenbergen, R.D.M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Walboomers, J.M.M.; Snow, G.B.; van der Waal, I. Prevalence of Epstein—Barr Virus in Oral Squamous Cell Carcinomas, Premalignant Lesions and Normal Mucosa—A Study Using the Polymerase Chain Reaction. Oral Oncol. 1997, 33, 182–188. [Google Scholar] [CrossRef]
- Sahebjamee, M.; Eslami, M.; Jahanzad, I.; Babaee, M.; Kharanzani Tafreshi, N. Presence of Epstein-Barr Virus in Oral Lichen Planus and Normal Oral Mucosa. Iran. J. Public Health 2007, 36, 92–98. [Google Scholar]
- Kis, A.; Fehér, E.; Gáll, T.; Tar, I.; Boda, R.; Tóth, E.D.; Méhes, G.; Gergely, L.; Szarka, K. Epstein-Barr Virus Prevalence in Oral Squamous Cell Cancer and in Potentially Malignant Oral Disorders in an Eastern Hungarian Population. Eur. J. Oral Sci. 2009, 117, 536–540. [Google Scholar] [CrossRef]
- Adtani, P.; Malathi, N. Epstein–Barr Virus and Its Association with Rheumatoid Arthritis and Oral Lichen Planus. J. Oral Maxillofac. Pathol. 2015, 19, 282. [Google Scholar] [CrossRef]
- da Rocha Vieira, R.; Ferreira, L.L.; Biasoli, É.R.; Bernabé, D.G.; Nunes, C.M.; Miyahara, G.I. Detection of Epstein–Barr Virus in Different Sources of Materials from Patients with Oral Lichen Planus: A Case–Control Study. J. Clin. Pathol. 2016, 69, 358–363. [Google Scholar] [CrossRef]
- Danielsson, K.; Nylander, E.; Sjostrom, M.; Ebrahimi, M. Epstein-Barr Virus Is Not Detected in Mucosal Lichen Planus. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e560–e563. [Google Scholar] [CrossRef]
- Raybaud, H.; Olivieri, C.V.; Lupi-Pegurier, L.; Pagnotta, S.; Marsault, R.; Cardot-Leccia, N.; Doglio, A. Epstein-Barr Virus–Infected Plasma Cells Infiltrate Erosive Oral Lichen Planus. J. Dent. Res. 2018, 97, 1494–1500. [Google Scholar] [CrossRef]
- Shariati, M.; Mokhtari, M.; Masoudifar, A. Association between Oral Lichen Planus and Epstein–Barr Virus in Iranian Patients. J. Res. Med. Sci. 2018, 23, 24. [Google Scholar] [CrossRef] [PubMed]
- Kanduc, D.; Lucchese, A.; Mittelman, A. Individuation of Monoclonal Anti-HPV16 E7 Antibody Linear Peptide Epitope by Computational Biology. Peptides 2001, 22, 1981–1985. [Google Scholar] [CrossRef]
- Lucchese, A.; Mittelman, A.; Lin, M.S.; Kanduc, D.; Sinha, A.A. Epitope Definition by Proteomic Similarity Analysis: Identification of the Linear Determinant of the Anti-Dsg3 MAb 5H10. J. Transl. Med. 2004, 2, 43. [Google Scholar] [CrossRef] [PubMed]
- Kanduc, D.; Serpico, R.; Lucchese, A.; Shoenfeld, Y. Correlating Low-Similarity Peptide Sequences and HIV B-Cell Epitopes. Autoimmun. Rev. 2008, 7, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Serpico, R.; Crincoli, V.; Shoenfeld, Y.; Kanduc, D. Sequence Uniqueness as a Molecular Signature of HIV-1-Derived B-Cell Epitopes. Int. J. Immunopathol. Pharmacol. 2009, 22, 639–646. [Google Scholar] [CrossRef]
- Lodi, G.; Scully, C.; Carrozzo, M.; Griffiths, M.; Sugerman, P.B.; Thongprasom, K. Current Controversies in Oral Lichen Planus: Report of an International Consensus Meeting. Part 2. Clinical Management and Malignant Transformation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2005, 100, 164–178. [Google Scholar] [CrossRef]
- Kanduc, D.; Lucchese, A.; Mittelman, A. Non-Redundant Peptidomes from DAPs: Towards “the Vaccine”? Autoimmun. Rev. 2007, 6, 290–294. [Google Scholar] [CrossRef]
- Pathmanathan, R.; Prasad, U.; Sadler, R.; Flynn, K.; Raab-Traub, N. Clonal Proliferations of Cells Infected with Epstein–Barr Virus in Preinvasive Lesions Related to Nasopharyngeal Carcinoma. N. Engl. J. Med. 1995, 333, 693–698. [Google Scholar] [CrossRef]


{kind=link}
| Search Topic | |||
|---|---|---|---|
| 1 | OR 2 | OR 3 | AND 4 |
| AND 5 | |||
| AND 6 | |||
| AND 7 | |||
| AND 8 | |||
| AND 9 | |||
| AND 10 |
| Reference (First Author + Year) | Detection of HPV-DNA in Specimens of Oral Lichen Planus (%) | Technique | HPV Probe Used | Specimens Positive for Each Genotype * (n°) | Clinical Features | Malignant Transformation |
|---|---|---|---|---|---|---|
| Syrjänen 1986 [22] | 2/2 (100) | ISH | 6, 11, 16 | 11 (1); 16 (1) | ||
| Maitland 1987 [23] | 7/8 (87.5) | SBH | 1, 2, 4, 6, 11, 13, 16, 18 | 16 (6); 1 more specimen was positive for HPV but not for the tested specific primers | Reticular keratosic form | |
| Jontell 1990 [24] | 6/20 (30) | SBH | 6, 11, 16, 18 | 11 (6) | Atrophic form with no or mild dysplasia | |
| Jontell 1990 [24] | 13/20 (65) | PCR | 6, 11, 16, 18 | 6 (5); 11 (8); 16 (3) | Atrophic form with no or mild dysplasia | |
| Kashima 1990 [25] | 0/22 (0) | ISH | 6, 11, 16, 18, 31 | NA | HPV positive OLPs were not classified as erosive form (NS) | |
| Kashima 1990 [25] | 4/22 (18.1) | PAP | 6, 11, 16, 18, 31 | NA | HPV positive OLPs were not classified as erosive form (NS) | |
| Young 1991 [26] | 0/6 (0) | ISH | 6, 11, 16, 18, 31, 33, 35 | NA | ||
| Miller 1993 [27] | 0/10 (0) | ISH | 6, 11, 16, 18, 31, 33, 35, 42, 43, 44, 45, 51, 52, 56 | NA | ||
| Cox 1993 [28] | 3/4 (75) | SBH | 16 | 16 (3) | ||
| Wen 1997 [29] | 2/9 (22.2) | PCR, SBH | 16, 18 | 16 (1); 18 (1) | ||
| González-Moles 1998 [30] | 2/17 (11.8) | PCR | 16 | 16 (2) | 2 HPV16+ specimens were erosive OLP type | |
| Sand 2000 [31] | 6/22 (27.3) | PCR, SBH | 6, 11, 16, 18 | 18 (5); 1 more specimen was positive for HPV but not for the tested primers | No correlation between the type of OLP and HPV positivity was found | |
| Yaltirik 2001 [32] | 0/2 (0) | ISH | 6, 11, 16, 18, 31, 33, 51 | NA | ||
| Giovannelli 2002 [33] | 9/34 (26.4) | PCR | 6, 16, 18, 31, 33 | NA | ||
| Ostwald 2003 [34] | 10/65 (15.4) | PCR, SBH | 6, 11, 16, 18 | 6 (6); 11 (6); 16 (2); 18 (5) | ||
| ÓFlatharta 2003 [35] | 20/38 (52.6) | PCR, SBH | 4, 8, 14, 16, 20, 23, 37, 38 | 4 (1); 8 (2); 14 (1); 16 (11); 20 (1); 23 (1); 37 (1); 38 (7) | ||
| Campisi 2004 [36] | 14/71 (19.7) | PCR | 6, 16, 18, 31 | 6 (1); 16 (2); 18 (10); 31 (1) | 9 out of 14 HPV positive OLPs were clinically identified as atrophic/erosive variant, and 5 as non-atrophic/erosive variant | |
| Giovannelli 2006 [37] | 13/49 (26.5) | PCR | 6, 16, 18, 33, 53 | NA | No association was found between type of lesion and site keratinization | |
| Zarei 2007 [38] | 2/15 (13.3) | PCR | 6, 11, 16, 18 | 6 (2) | ||
| Debanth 2009 [39] | NA | NAH | 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68 | NA | ||
| Razavi 2009 [40] | 9/29 (31) | PCR | 18 | 18 (9) | ||
| Yildirim 2011 [12] | 14/65 (21.5) | ABC | 16 | 16 (14) | 2 erosive, 5 plaque, and 7 reticular types of OLP | |
| Mattila 2012 [41] | 13/82 (15.9) | PCR | 6, 11, 16, 18, 26, 31, 33, 35, 39, 42, 43, 44, 45, 51, 52, 53, 56, 58, 59, 66, 68, 70, 73, 82 | 6 (1); 11 (3); 16 (7); 31 (1); 33 (1); 58 (1); 66 (1) | Five patients with atrophic OLP developed invasive OSCC during the follow-up; LR-HPV was detected in two samples: one had HPV6 and the other HPV11 | |
| Arirachakaran 2013 [42] | 1/37 (2.7) | PCR | 6, 11, 16, 18, 30, 31, 32, 33, 34, 35, 39, 40, 42, 44, 51, 52, 53, 55, 56, 58, 59, 66, 68, 70, 71, 73, 74, 81, 82, 85, 90, 91 | 16 (1) | The only HPV-DNA positive sample came from an atrophic-type OLP lesion | |
| Kato 2015 [43] | 83/200 (41.5) | PCR, ISH, IHC | 1, 6, 11, 16, 18, 30, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 54, 56, 58, 61, 66, 81 | 6 (11); 11 (13); 16 (51); 18 (47); 33 (7) | HPV16 positive rates according to OLP clinical type were 28.3% (13/46), 18.6% (8/43), 25.9% (7/27), and 0.0% (0/6) for erosive, reticular, plaque-type, and atrophic | |
| Pol 2015 [44] | 21/30 (70) | IHC | 16 | 16 (21) | All cases of OLP were of the reticular form | |
| Sahebjamiee 2015 [45] | 11/40 (27.5) | PCR | 16, 18 | 16 (5); 18 (3); 3 more specimens were positive for HPV but not for the tested-specific primers | ||
| Viguier 2015 [46] | 3/6 (50) | PCR | 16 | 16 (2); 1 more specimen was positive for HPV but not for the tested-specific primers | All cases of OLP were of the severe erosive form | |
| Liu 2018 [47] | 33/46 (71.7) | IHC, OD | 16, 18 | NA | MT-OLP showed significantly higher infection by HPV16/18(E6) than OLP (p < 0.05). HPV infection rates in normal mucosa, OLP, and MT-OLP were 62.50%, 67.50%, and 100.00%, respectively | |
| Zendeli-Bedjeti 2017 [48] | 7/31 (22.6) | PCR | 16, 18, 31, 56 | 56 (4); 16 (3) | ||
| Gomez-Armayones 2018 [49] | 1/41 (2.4) | IHC, PCR, OD | 16, 18 | 16 (1) | ||
| Sameera 2019 [50] | 13/15 (86.6) | PCR | 18 | 18 (13) | Non-atrophic (8/13) and atrophic (5/13) HPV18+ OLP type | |
| Farhadi 2020 [51] | 8/32 (25) | PCR | 7, 18 | 7 (7); 18 (1) | The 8/32 OLP samples that were HPV positive presented erosive features | |
| Kaewmaneenuan 2021 [52] | 11/59 (18.6) | PCR | 16, 18 | 16 (1); 18 (10) | 11/59 OLP samples that tested positive for HPV were atrophic/ulcerative type | |
| Della Vella 2021 [53] | 9/52 (17.3) | PCR | 6, 8, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 66, 68, 69, 70, 73 | 6 (5); 11(3); 16(1); 42 (2); 53 (1) | 8 out of 43 hyperkeratotic OLP type were HPV+; 1 out of 9 erosive OLP type was HPV+ (9 out of 52) |
| Reference (First Author + Year) | Detection of EBV in Specimens of Oral Lichen Planus (%) | Detection of HSV1 in Specimens of Oral Lichen Planus (%) | Detection of HHV7 in Specimens of Oral Lichen Planus (%) | Technique | Clinical Features | Malignant Transformation |
|---|---|---|---|---|---|---|
| Cox 1993 [28] | 2/4 (50) | SBH | ||||
| Pedersen 1996 [54] | NA (serum analysis) | OD | ||||
| Cruz 1997 [55] | 1/2 (50) | PCR, SBH | ||||
| Sand 2002 [13] | 6/23 (26) | nPCR | 2 atrophic, 3 reticular, 1 unspecified OLP type (6/23 EBV+) | |||
| ÓFlatharta 2003 [35] | 2/26 (7.69) | 0/26 (0) | 3/26 (11.5) | PCR, SBH | ||
| Sahebjamee 2007 [56] | 0/22 (0) | PCR | ||||
| Kis 2009 [57] | 54/116 (46.5) | nPCR, IHC | 26/57 non- atrophic/erosive OLP EBV+ (57/116); 28/59 atrophic/erosive -OLP EBV+ (59/116) | |||
| Yildirim 2011 [12] | 23/65 (35.3) | 6/65 (9.2) | ABC | |||
| Adtani 2015 [58] | NA (serum analysis) | EI | ||||
| Vieira Rda 2016 [59] | 15/24 (62.5) | nPCR | 9/11 were atrophic/erosive lesions EBV+ (11/24); 6/13 were non-atrophic/erosive lesions EBV+ (13/24) | |||
| Danielsson 2018 [60] | 0/25 (0) | ISH, IHC | ||||
| Raybaud 2018 [61] | 73/99 (74) | ISH, PCR | 19/33 were reticular white lesions EBV+ (33/99); 55/66 erosive/ulcerative lesions with or without reticular lesions were EBV+ (66/99) | |||
| Shariati 2018 [62] | 6/38 (15.8) | PCR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucchese, A.; Di Stasio, D.; Romano, A.; Fiori, F.; De Felice, G.P.; Lajolo, C.; Serpico, R.; Cecchetti, F.; Petruzzi, M. Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review. J. Clin. Med. 2022, 11, 5487. https://doi.org/10.3390/jcm11185487
Lucchese A, Di Stasio D, Romano A, Fiori F, De Felice GP, Lajolo C, Serpico R, Cecchetti F, Petruzzi M. Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review. Journal of Clinical Medicine. 2022; 11(18):5487. https://doi.org/10.3390/jcm11185487
Chicago/Turabian StyleLucchese, Alberta, Dario Di Stasio, Antonio Romano, Fausto Fiori, Guido Paolo De Felice, Carlo Lajolo, Rosario Serpico, Francesco Cecchetti, and Massimo Petruzzi. 2022. "Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review" Journal of Clinical Medicine 11, no. 18: 5487. https://doi.org/10.3390/jcm11185487
APA StyleLucchese, A., Di Stasio, D., Romano, A., Fiori, F., De Felice, G. P., Lajolo, C., Serpico, R., Cecchetti, F., & Petruzzi, M. (2022). Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review. Journal of Clinical Medicine, 11(18), 5487. https://doi.org/10.3390/jcm11185487