
Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
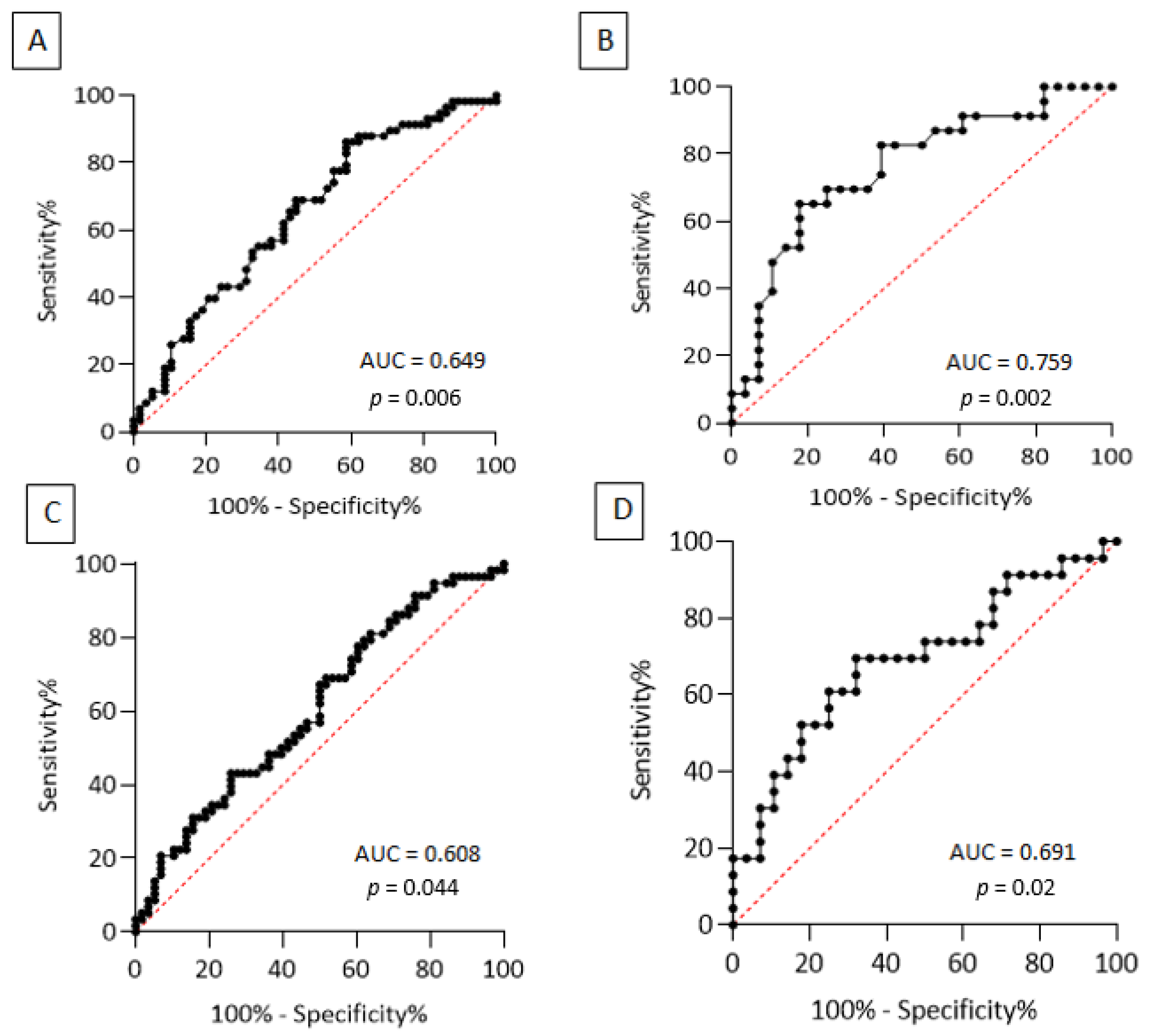
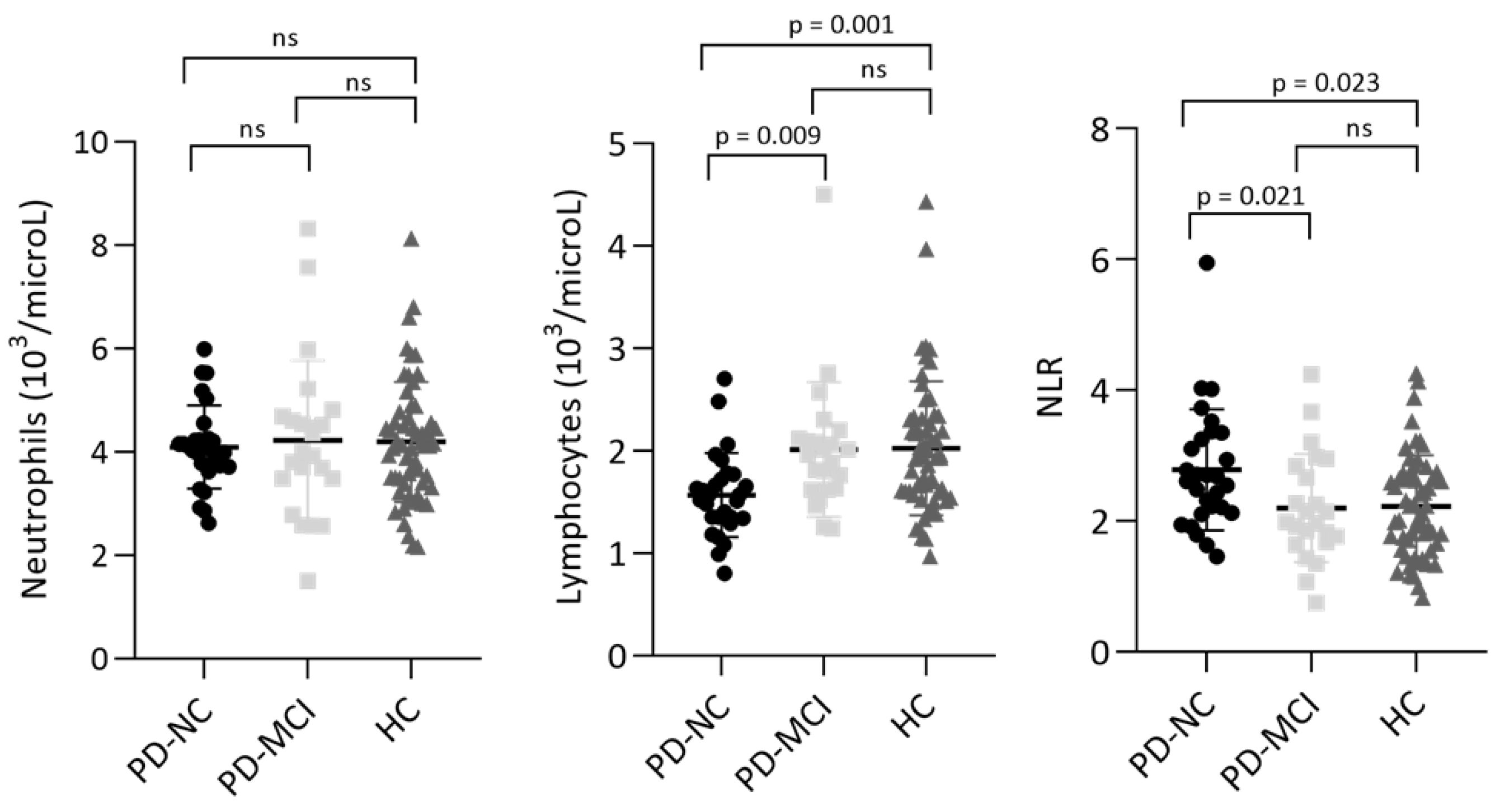
3.1. Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio in Parkinson’s Disease vs. Healthy Subjects
3.2. Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio in Parkinson’s Disease-Related Mild Cognitive Impairment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jankovic, J. Parkinson’s Disease: Clinical Features and Diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef]
- Dickson, D.W. Neuropathology of Parkinson Disease. Parkinsonism Relat. Disord. 2018, 46 (Suppl. S1), S30–S33. [Google Scholar] [CrossRef]
- Jensen, M.P.; Jacobs, B.M.; Dobson, R.; Bandres-Ciga, S.; Blauwendraat, C.; Schrag, A.; Noyce, A.J. The International Parkinson’s Disease Genomics Consortium (IPDGC) Lower Lymphocyte Count Is Associated With Increased Risk of Parkinson’s Disease. Ann. Neurol. 2021, 89, 803–812. [Google Scholar] [CrossRef]
- Tsukita, K.; Sakamaki-Tsukita, H.; Takahashi, R. Lower Circulating Lymphocyte Count Predicts ApoE ε 4-Related Cognitive Decline in Parkinson’s Disease. Mov. Disord. 2021, 36, 2969–2971. [Google Scholar] [CrossRef]
- Brochard, V.; Combadière, B.; Prigent, A.; Laouar, Y.; Perrin, A.; Beray-Berthat, V.; Bonduelle, O.; Alvarez-Fischer, D.; Callebert, J.; Launay, J.-M.; et al. Infiltration of CD4+ Lymphocytes into the Brain Contributes to Neurodegeneration in a Mouse Model of Parkinson Disease. J. Clin. Investig. 2008, 119, 182–192. [Google Scholar] [CrossRef]
- Kustrimovic, N.; Comi, C.; Magistrelli, L.; Rasini, E.; Legnaro, M.; Bombelli, R.; Aleksic, I.; Blandini, F.; Minafra, B.; Riboldazzi, G.; et al. Parkinson’s Disease Patients Have a Complex Phenotypic and Functional Th1 Bias: Cross-Sectional Studies of CD4+ Th1/Th2/T17 and Treg in Drug-Naïve and Drug-Treated Patients. J. Neuroinflamm. 2018, 15, 205. [Google Scholar] [CrossRef]
- Afari, M.E.; Bhat, T. Neutrophil to Lymphocyte Ratio (NLR) and Cardiovascular Diseases: An Update. Expert Rev. Cardiovasc. Ther. 2016, 14, 573–577. [Google Scholar] [CrossRef]
- Ethier, J.-L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Breast Cancer: A Systematic Review and Meta-Analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef]
- Wang, L.; Wang, C.; Jia, X.; Yang, M.; Yu, J. Relationship between Neutrophil-to-Lymphocyte Ratio and Systemic Lupus Erythematosus: A Meta-Analysis. Clinics 2020, 75, e1450. [Google Scholar] [CrossRef]
- Muñoz-Delgado, L.; Macías-García, D.; Jesús, S.; Martín-Rodríguez, J.F.; Labrador-Espinosa, M.Á.; Jiménez-Jaraba, M.V.; Adarmes-Gómez, A.; Carrillo, F.; Mir, P. Peripheral Immune Profile and Neutrophil-to-Lymphocyte Ratio in Parkinson’s Disease. Mov. Disord. 2021, 36, 2426–2430. [Google Scholar] [CrossRef]
- Haghshomar, M.; Rahmani, F.; Hadi Aarabi, M.; Shahjouei, S.; Sobhani, S.; Rahmani, M. White Matter Changes Correlates of Peripheral Neuroinflammation in Patients with Parkinson’s Disease. Neuroscience 2019, 403, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.M.; Ehgoetz Martens, K.A.; Walton, C.C.; O’Callaghan, C.; Keller, P.E.; Lewis, S.J.G.; Moustafa, A.A. Diffusion Alterations Associated with Parkinson’s Disease Symptomatology: A Review of the Literature. Parkinsonism Relat. Disord. 2016, 33, 12–26. [Google Scholar] [CrossRef]
- Kustrimovic, N.; Rasini, E.; Legnaro, M.; Bombelli, R.; Aleksic, I.; Blandini, F.; Comi, C.; Mauri, M.; Minafra, B.; Riboldazzi, G.; et al. Dopaminergic Receptors on CD4+ T Naive and Memory Lymphocytes Correlate with Motor Impairment in Patients with Parkinson’s Disease. Sci. Rep. 2016, 6, 33738. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Álvarez-Luquín, D.D.; Guevara-Salinas, A.; Arce-Sillas, A.; Espinosa-Cárdenas, R.; Leyva-Hernández, J.; Montes-Moratilla, E.U.; Adalid-Peralta, L. Increased Tc17 Cell Levels and Imbalance of Naïve/Effector Immune Response in Parkinson’s Disease Patients in a Two-Year Follow-up: A Case Control Study. J. Transl. Med. 2021, 19, 378. [Google Scholar] [CrossRef]
- Liu, Z.; Zhai, X.-R.; Du, Z.-S.; Xu, F.-F.; Huang, Y.; Wang, X.-Q.; Qiu, Y.-H.; Peng, Y.-P. Dopamine Receptor D2 on CD4+ T Cells Is Protective against Neuroinflammation and Neurodegeneration in a Mouse Model of Parkinson’s Disease. Brain Behav. Immun. 2021, 98, 110–121. [Google Scholar] [CrossRef]
- Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C.; Stebbins, G.T.; Counsell, C.; Giladi, N.; Holloway, R.G.; Moore, C.G.; Wenning, G.K.; et al. Movement Disorder Society Task Force Report on the Hoehn and Yahr Staging Scale: Status and Recommendations. Mov. Disord. 2004, 19, 1020–1028. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Reyes, M.A.; Lloret, S.P.; Gerscovich, E.R.; Martin, M.E.; Leiguarda, R.; Merello, M. Addenbrooke’s Cognitive Examination Validation in Parkinson’s Disease. Eur. J. Neurol. 2009, 16, 142–147. [Google Scholar] [CrossRef]
- McColgan, P.; Evans, J.R.; Breen, D.P.; Mason, S.L.; Barker, R.A.; Williams-Gray, C.H. Addenbrooke’s Cognitive Examination-Revised for Mild Cognitive Impairment in Parkinson’s Disease. Mov. Disord. 2012, 27, 1173–1177. [Google Scholar] [CrossRef]
- Siciliano, M.; Raimo, S.; Tufano, D.; Basile, G.; Grossi, D.; Santangelo, F.; Trojano, L.; Santangelo, G. The Addenbrooke’s Cognitive Examination Revised (ACE-R) and Its Sub-Scores: Normative Values in an Italian Population Sample. Neurol. Sci. 2016, 37, 385–392. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Fuzzati-Armentero, M.T.; Cerri, S.; Blandini, F. Peripheral-Central Neuroimmune Crosstalk in Parkinson’s Disease: What Do Patients and Animal Models Tell Us? Front. Neurol. 2019, 10, 232. [Google Scholar] [CrossRef]
- Akıl, E.; Bulut, A.; Kaplan, İ.; Özdemir, H.H.; Arslan, D.; Aluçlu, M.U. The Increase of Carcinoembryonic Antigen (CEA), High-Sensitivity C-Reactive Protein, and Neutrophil/Lymphocyte Ratio in Parkinson’s Disease. Neurol. Sci. 2015, 36, 423–428. [Google Scholar] [CrossRef]
- Solmaz, V.; Pekdaş Genç, E.; Aksoy, D.; Çevik, B.; Kurt, S.G.; Benli, İ. Parkinson Hastalarında Nötrofil/Lenfosit Oranları, C Reaktif Protein ve Sedimantasyon Hızlarının Değerlendirilmesi. Cukurova Med. J. 2018, 43, 305–311. [Google Scholar] [CrossRef]
- Ataç Uçar, C.; Gökçe Çokal, B.; Ünal Artık, H.A.; İnan, L.E.; Yoldaş, T.K. Comparison of Neutrophil-Lymphocyte Ratio (NLR) in Parkinson’s Disease Subtypes. Neurol. Sci. 2017, 38, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Büyükkoyuncu Pekel, N. Parkinson s Disease: Is It Actually an Inflammatory Disorder. Turk. J. Geriatr.-Turk Geriatr. Derg. 2018, 21, 483–489. [Google Scholar] [CrossRef]
- An, P.; Zhou, X.; Du, Y.; Zhao, J.; Song, A.; Liu, H.; Ma, F.; Huang, G. Association of Neutrophil-Lymphocyte Ratio with Mild Cognitive Impairment in Elderly Chinese Adults: A Case-Control Study. Curr. Alzheimer Res. 2019, 16, 1309–1315. [Google Scholar] [CrossRef]
- Dong, X.; Nao, J.; Shi, J.; Zheng, D. Predictive Value of Routine Peripheral Blood Biomarkers in Alzheimer’s Disease. Front. Aging Neurosci. 2019, 11, 332. [Google Scholar] [CrossRef]
- King, E.; O’Brien, J.T.; Donaghy, P.; Morris, C.; Barnett, N.; Olsen, K.; Martin-Ruiz, C.; Taylor, J.-P.; Thomas, A.J. Peripheral Inflammation in Prodromal Alzheimer’s and Lewy Body Dementias. J. Neurol. Neurosurg. Psychiatry 2018, 89, 339–345. [Google Scholar] [CrossRef]
- Kalelioglu, T.; Yuruyen, M.; Gultekin, G.; Yavuzer, H.; Özturk, Y.; Kurt, M.; Topcu, Y.; Doventas, A.; Emul, M. Neutrophil and Platelet to Lymphocyte Ratios in People with Subjective, Mild Cognitive Impairment and Early Alzheimer’s Disease: Inflammation in Cognitive Impairment. Psychogeriatrics 2017, 17, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Halazun, H.J.; Mergeche, J.L.; Mallon, K.A.; Connolly, E.S.; Heyer, E.J. Neutrophil-Lymphocyte Ratio as a Predictor of Cognitive Dysfunction in Carotid Endarterectomy Patients. J. Vasc. Surg. 2014, 59, 768–773. [Google Scholar] [CrossRef]
- Lee, M.; Lim, J.-S.; Kim, C.-H.; Lee, S.-H.; Kim, Y.; Hun Lee, J.; Jang, M.U.; Sun Oh, M.; Lee, B.-C.; Yu, K.-H. High Neutrophil-Lymphocyte Ratio Predicts Post-Stroke Cognitive Impairment in Acute Ischemic Stroke Patients. Front. Neurol. 2021, 12, 693318. [Google Scholar] [CrossRef]
- Hu, Z.X.; Song, W.N.; Lu, X.D.; Zhou, M.L.; Shao, J.H. Peripheral T Lymphocyte Immunity and L-Dopamine in Patients with Parkinson’s Disease. J. Biol. Regul. Homeost. Agents 2018, 32, 687–691. [Google Scholar] [PubMed]
- Magistrelli, L.; Storelli, E.; Rasini, E.; Contaldi, E.; Comi, C.; Cosentino, M.; Marino, F. Relationship between Circulating CD4+ T Lymphocytes and Cognitive Impairment in Patients with Parkinson’s Disease. Brain Behav. Immun. 2020, 89, 668–674. [Google Scholar] [CrossRef]
- Berankova, D.; Janousova, E.; Mrackova, M.; Eliasova, I.; Kostalova, M.; Skutilova, S.; Rektorova, I. Addenbrooke’s Cognitive Examination and Individual Domain Cut-Off Scores for Discriminating between Different Cognitive Subtypes of Parkinson’s Disease. Parkinson’s Dis. 2015, 2015, 579417. [Google Scholar] [CrossRef]
- Smith, C.; Malek, N.; Grosset, K.; Cullen, B.; Gentleman, S.; Grosset, D.G. Neuropathology of Dementia in Patients with Parkinson’s Disease: A Systematic Review of Autopsy Studies. J. Neurol. Neurosurg. Psychiatry 2019, 90, 1234–1243. [Google Scholar] [CrossRef]
- Bawa, K.K.; Krance, S.H.; Herrmann, N.; Cogo-Moreira, H.; Ouk, M.; Yu, D.; Wu, C.-Y.; Black, S.E.; Lanctôt, K.L.; Swardfager, W.; et al. A Peripheral Neutrophil-Related Inflammatory Factor Predicts a Decline in Executive Function in Mild Alzheimer’s Disease. J. Neuroinflamm. 2020, 17, 84. [Google Scholar] [CrossRef] [PubMed]
- Pietronigro, E.C.; Della Bianca, V.; Zenaro, E.; Constantin, G. NETosis in Alzheimer’s Disease. Front. Immunol. 2017, 8, 211. [Google Scholar] [CrossRef]
- Vida, C.; Martinez de Toda, I.; Garrido, A.; Carro, E.; Molina, J.A.; De la Fuente, M. Impairment of Several Immune Functions and Redox State in Blood Cells of Alzheimer’s Disease Patients. Relevant Role of Neutrophils in Oxidative Stress. Front. Immunol. 2018, 8, 1974. [Google Scholar] [CrossRef] [Green Version]
- Petrone, A.B.; Eisenman, R.D.; Steele, K.N.; Mosmiller, L.T.; Urhie, O.; Zdilla, M.J. Temporal Dynamics of Peripheral Neutrophil and Lymphocytes Following Acute Ischemic Stroke. Neurol. Sci. 2019, 40, 1877–1885. [Google Scholar] [CrossRef] [PubMed]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic Criteria for Mild Cognitive Impairment in Parkinson’s Disease: Movement Disorder Society Task Force Guidelines: PD-MCI Diagnostic Criteria. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | PD (n = 58) | HC (n = 58) | p-Value |
|---|---|---|---|
| Age, years | 69.28 (8.13) | 69.31 (8.18) | 0.969 |
| Sex, M/F | 42/16 | 42/16 | 1.0 |
| History of cardiovascular diseases | 34 (58.6) | 31 (53.4) | 0.575 |
| Disease duration, years | 1.38 (0.91) | - | - |
| UPDRS-III “OFF”, score | 13.62 (6.79) | - | - |
| H&Y stage -Stage 1 -Stage 2 | 41 (70.7) 17 (29.3) | - | - |
| Tremor dominant phenotype | 39 (67.2) | - | - |
| ACE-R total score (baseline) | 93.20 (2.92) | - | - |
| ACE-R attention and orientation (baseline) | 18 (2.24) | - | - |
| ACE-R memory (baseline) | 25.86 (4.87) | - | - |
| ACE-R fluency (baseline) | 11.71 (2.80) | - | - |
| ACE-R language (baseline) | 27.37 (2.86) | - | - |
| ACE-R visuospatial (baseline) | 16.08 (2.49) | - | - |
| WBC (103/microL) | 6.47 (1.34) | 6.71 (1.54) | 0.600 |
| RBC (106/microL) | 4.69 (0.50) | 4.91 (0.78) | 0.251 |
| Hemoglobin (g/dL) | 14.12 (1.40) | 14.24 (1.13) | 0.519 |
| Hematocrit (%) | 42.39 (4.02) | 42.90 (3.38) | 0.467 |
| MCV (fL) | 90.62 (3.30) | 91.47 (4.93) | 0.588 |
| MCH (pg) | 30.15 (1.10) | 30.47 (1.73) | 0.118 |
| MCHC (g/dL) | 33.87 (4.44) | 33.52 (2.28) | 0.601 |
| Platelets (103/microL) | 218.75 (51.48) | 222.63 (52.80) | 0.612 |
| Monocytes (103/microL) | 0.55 (0.17) | 0.56 (0.15) | 0.712 |
| Eosinophils (103/microL) | 0.15 (0.09) | 0.22 (0.21) | 0.108 |
| Basophils (103/microL) | 0.04 (0.03) | 0.04 (0.02) | 0.601 |
| Neutrophils (103/microL) | 4.20 (1.22) | 4.19 (1.16) | 0.943 |
| Lymphocytes (103/microL) | 1.73 (0.56) | 2.02 (0.65) | 0.006 |
| NLR | 2.63 (1.15) | 2.23 (0.78) | 0.044 |
| ESR (mm/h) | 12.14 (10.98) | - | - |
| CRP (mg/dL) | 0.37 (0.97) | - | - |
| Lymphocyte Count Cut-off Values | Sensitivity (95% CI) | Specificity (95% CI) | LR+ | LR− | PPV | NPV |
|---|---|---|---|---|---|---|
| PD vs. HC | ||||||
| ≤1.915 (103/microL) | 69% (56.20–79.38%) | 55.2% (42.45–67.25%) | 1.54 | 0.56 | 60.6% | 64% |
| PD-MCI vs. PD-NC | ||||||
| ≥1.790 (103/microL) | 65.2% (44.89–81.19%) | 82.1% (64.41–92.12%) | 3.64 | 0.42 | 75% | 74.2% |
| NLR Cut-off Values | Sensitivity (95% CI) | Specificity (95% CI) | LR+ | LR− | PPV | NPV |
| PD vs. HC | ||||||
| ≥2.065 | 69% (56.20–79.38%) | 48.3% (35.93–60.84%) | 1.33 | 0.64 | 57.1% | 60.9% |
| PD-MCI vs. PD-NC | ||||||
| ≤2.295 | 69.6% (49.13–84.4%) | 67.8% (49.34–82.07%) | 2.16 | 0.45 | 64% | 73.1% |
| Variables | PD-NC (n = 28) | PD-MCI (n = 23) | p-Value |
|---|---|---|---|
| Age at baseline, years | 67.39 (9.09) | 68.80 (8.48) | 0.185 |
| Sex, M/F | 18/10 | 18/5 | 0.360 |
| Scholarity, years | 10.86 (4.02) | 9.17 (4.72) | 0.116 |
| History of cardiovascular diseases | 17 (60.71) | 13 (56.52) | 0.783 |
| Disease duration, years | 2.86 (1.48) | 3.48 (1.65) | 0.162 |
| UPDRS-III “ON”, score | 13 (5.48) | 13.65 (7.15) | 0.753 |
| LEDD, mg/day | 360.84 (179.36) | 409.65 (258.24) | 0.463 |
| H&Y stage -Stage 1 -Stage 2 | 20 (71.43) 8 (28.57) | 18 (78.26) 5 (21.73) | 0.749 |
| Tremor dominant phenotype | 19 (67.85) | 15 (65.22) | 1.0 |
| ACE-R total score | 92.67 (3.40) | 80.15 (7.84) | <0.0001 |
| ACE-R attention and orientation | 18.13 (0.54) | 20.06 (15.04) | 0.001 |
| ACE-R memory | 26.40 (2.08) | 21.57 (3.25) | <0.0001 |
| ACE-R fluency | 11.63 (2.22) | 9.34 (2.42) | <0.0001 |
| ACE-R language | 27.35 (1.26) | 26.04 (3.05) | 0.117 |
| ACE-R visuospatial | 16.04 (1.24) | 14.17 (1.91) | <0.0001 |
| WBC (103/microL) | 5.95 (1.01) | 7.07 (1.47) | 0.011 |
| RBC (106/microL) | 4.68 (0.44) | 4.67 (0.59) | 0.541 |
| Hemoglobin (g/dL) | 14.12 (1.30) | 13.98 (1.58) | 0.40 |
| Hematocrit (%) | 42.34 (3.54) | 42.27 (4.76) | 0.483 |
| MCV (fL) | 90.77 (2.84) | 90.66 (3.73) | 0.960 |
| MCH (pg) | 30.26 (1.02) | 29.97 (1.23) | 0.416 |
| MCHC (g/dL) | 34.48 (6.17) | 33.09 (1.02) | 0.405 |
| Platelets (103/microL) | 214.15 (41.74) | 223.35 (62.82) | 0.841 |
| Monocytes (103/microL) | 0.54 (0.18) | 0.57 (0.16) | 0.351 |
| Eosinophils (103/microL) | 0.16 (0.09) | 0.15 (0.09) | 0.673 |
| Basophils (103/microL) | 0.04 (0.02) | 0.05 (0.03) | 0.150 |
| Neutrophils (103/microL) | 4.09 (0.80) | 4.22 (1.55) | 1.0 |
| Lymphocytes (103/microL) | 1.57 (0.41) | 2.01 (0.66) | 0.002 |
| NLR | 2.78 (0.93) | 2.20 (0.83) | 0.020 |
| ESR (mm/h) | 10.50 (7.53) | 10.65 (7.22) | 0.857 |
| CRP (mg/dL) | 0.19 (0.22) | 0.47 (1.28) | 0.595 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contaldi, E.; Magistrelli, L.; Cosentino, M.; Marino, F.; Comi, C. Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study. J. Clin. Med. 2022, 11, 5543. https://doi.org/10.3390/jcm11195543
Contaldi E, Magistrelli L, Cosentino M, Marino F, Comi C. Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study. Journal of Clinical Medicine. 2022; 11(19):5543. https://doi.org/10.3390/jcm11195543
Chicago/Turabian StyleContaldi, Elena, Luca Magistrelli, Marco Cosentino, Franca Marino, and Cristoforo Comi. 2022. "Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study" Journal of Clinical Medicine 11, no. 19: 5543. https://doi.org/10.3390/jcm11195543
APA StyleContaldi, E., Magistrelli, L., Cosentino, M., Marino, F., & Comi, C. (2022). Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study. Journal of Clinical Medicine, 11(19), 5543. https://doi.org/10.3390/jcm11195543