
Lateral or Medial Parapatellar Surgical Approach to the Valgus Osteoarthritic Knee? A Retrospective Single-Center Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
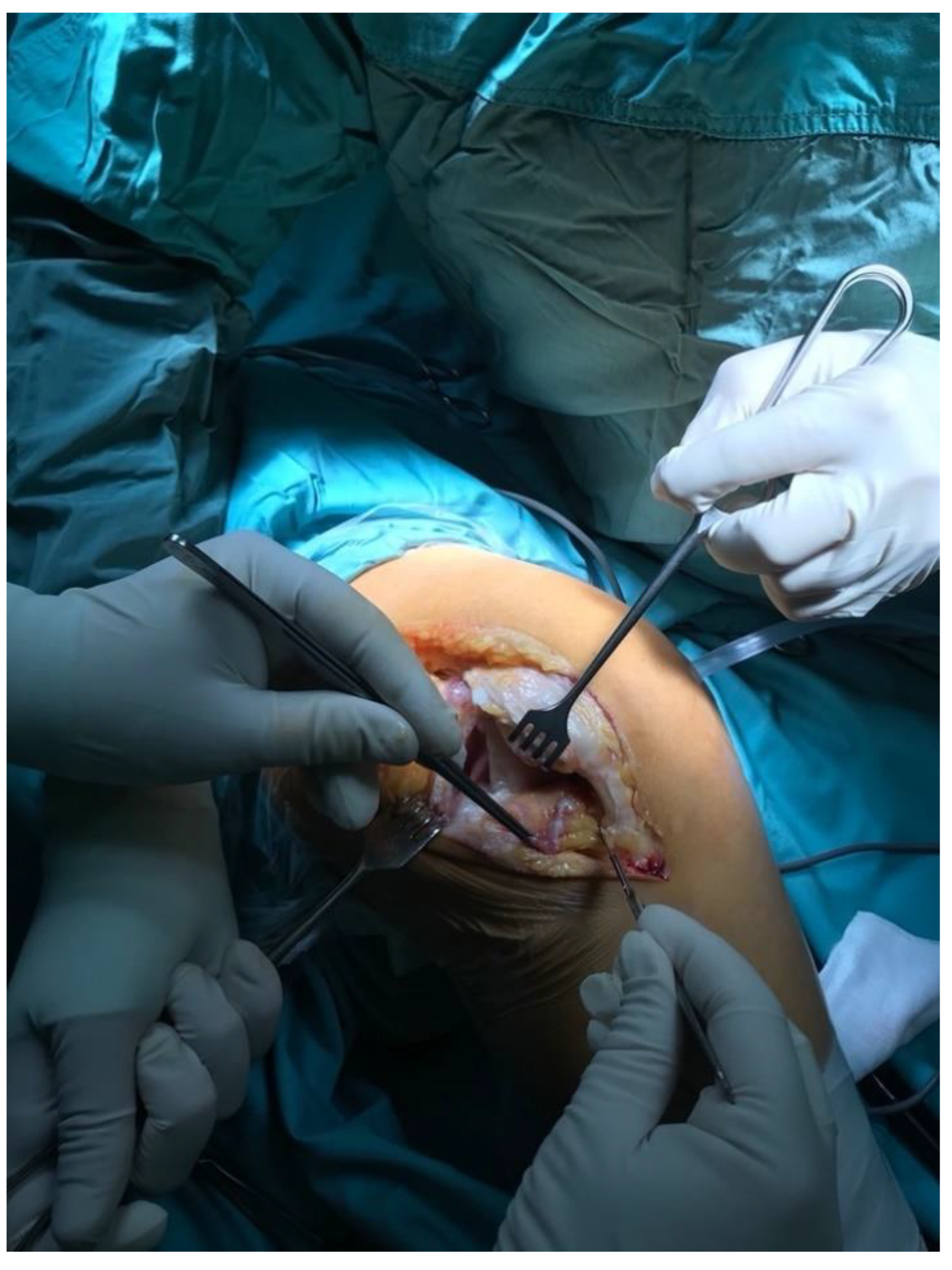
2.2. Surgical Approach
2.3. Postoperative Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apostolopoulos, A.; Nikolopoulos, D.; Polyzois, I.; Nakos, A.; Liarokapis, S.; Stefanakis, G.; Michos, I. Total knee arthroplasty in severe valgus deformity: Interest of combining a lateral approach with a tibial tubercle osteotomy. Orthop. Traumatol. Surg. Res. 2010, 96, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranawat, A.S.; Ranawat, C.S.; Elkus, M.; Rasquinha, V.J.; Rossi, R.; Babhulkar, S. Total Knee Arthroplasty for Severe Valgus Deformity. J. Bone Jt. Surg. 2005, 87 (Suppl. 1), 271–284. [Google Scholar] [CrossRef]
- Gunst, S.; Villa, V.; Magnussen, R.; Servien, E.; Lustig, S.; Neyret, P. Equivalent results of medial and lateral parapatellar approach for total knee arthroplasty in mild valgus deformities. Int. Orthop. 2016, 40, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Rosso, F.; Cottino, U.; Dettoni, F.; Bonasia, D.E.; Bruzzone, M. Total knee arthroplasty in the valgus knee. Int. Orthop. 2013, 38, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Keblish, P. The lateral approach to the valgus knee. Surgical technique and analysis of 53 cases with over two-year follow-up evaluation. Clin. Orthop. Relat. Res. 1991, 271, 52–62. [Google Scholar] [CrossRef]
- Xu, G.; Fu, X.; Tian, P.; Bahat, D.; Huang, Y.; Li, Z. The lateral and medial approach in total arthroplasty for valgus knee: A meta-analysis of current literature. J. Comp. Eff. Res. 2020, 9, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Norman, W. Rationale, of The Knee Society Clinical Rating System. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar] [CrossRef]
- Sekiya, H.; Takatoku, K.; Takada, H.; Sugimoto, N.; Hoshino, Y. Lateral approach is advantageous in total knee arthroplasty for valgus deformed knee. Eur. J. Orthop. Surg. Traumatol. 2012, 24, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawal, J.; Devany, A.J.; A Jeffery, J. Arthroplasty in the Valgus Knee: Comparison and Discussion of Lateral vs Medial Parapatellar Approaches and Implant Selection. Open Orthop. J. 2015, 9, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalidis, B.E.; Ye, K.; Sachinis, N.P.; Hawdon, G.; McMahon, S. Lateral parapatellar approach with tibial tubercle osteotomy for the treatment of non-correctable valgus knee osteoarthritis: A retrospective clinical study. Knee 2014, 21, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Piedade, S.R.; Pinaroli, A.; Servien, E.; Neyret, P. Tibial tubercle osteotomy in primary total knee arthroplasty: A safe procedure or not? Knee 2008, 15, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Hirschmann, M.T.; Hoffmann, M.; Krause, R.; Jenabzadeh, R.-A.; Arnold, M.P.; Friederich, N.F. Anterolateral approach with tibial tubercle osteotomy versus standard medial approach for primary total knee arthroplasty: Does it matter? BMC Musculoskelet. Disord. 2010, 11, 167. [Google Scholar] [CrossRef] [Green Version]
- Hay, G.C.; Kampshoff, J.; Kuster, M.S.; Hassan, A.; Whately, C.; Letts, M. Lateral subvastus approach with osteotomy of the tibial tubercle for total knee replacement: A two-year prospective, randomised, blinded controlled trial. J. Bone Jt. Surgery. Br. Vol. 2010, 92, 862–866. [Google Scholar] [CrossRef]
- Nikolopoulos, D.D.; Polyzois, I.; Apostolopoulos, A.P.; Rossas, C.; Moutsios-Rentzos, A.; Michos, I.V. Total knee arthroplasty in severe valgus knee deformity: Comparison of a standard medial parapatellar approach combined with tibial tubercle osteotomy. Knee Surgery Sports Traumatol. Arthrosc. 2011, 19, 1834–1842. [Google Scholar] [CrossRef] [PubMed]
- Buechel, F.F. A sequential three-step lateral release for correcting fixed valgus knee deformities during total knee arthroplasty. Clin. Orthop. Relat. Res. 1990, 260, 170–175. [Google Scholar] [CrossRef]
- Kayler, D.E.; Lyttle, D. Surgical Interruption of Patellar Blood Supply by Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 1988, 229, 221–227. [Google Scholar] [CrossRef]
- Scott, R.D.; Turoff, N.; Ewald, F.C. Stress fracture of the patella following duopatellar total knee arthroplasty with patellar resur-facing. Clin. Orthop Relat Res. 1982, 170, 147–151. [Google Scholar] [CrossRef]
- Greenberg, A.; Kandel, L.; Liebergall, M.; Mattan, Y.; Rivkin, G. Total Knee Arthroplasty for Valgus Deformity via a Lateral Approach: Clinical Results, Comparison to Medial Approach, and Review of Recent Literature. J. Arthroplast. 2020, 35, 2076–2083. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Xing, D.; Li, J.J.; Zhu, Y.; Dong, S.; Zhao, B. Lateral or medial approach for valgus knee in total knee arthroplasty - which one is better? A systematic review. J. Int. Med Res. 2019, 47, 5400–5413. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | I | II | III |
|---|---|---|---|
| Correction | Full | No | No |
| Grade of deformity | Minimal | Substantial | Severe osseus |
| Medial Collateral Ligament | Functional and intact | Elongated, functional | severely impaired |
| Angle of deformity | <10 | 10–20 | >20 |
| Implant type | Posterior-Stabilized [PS] | PS/Constrained Condylar Knee [CCK] | CCK/Hinged |
| Lateral Approach [LA] (n = 143) | Medial Approach [MA] (n = 50) | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | LL | UL | d Cohen’s | |
| Age at the time of surgery (years) | 68.2 | 11.2 | 67.2 | 9.4 | 0.55 | 0.583 | −2.52 | 4.47 | 0.09 |
| Woman (%) | 0.9 | 0.3 | 0.8 | 0.4 | 0.94 | 0.348 | −0.06 | 0.17 | 0.17 |
| Pre-op Range of Motion [ROM] (°) | 101.3 | 20.9 | 102.9 | 25.2 | −0.41 | 0.680 | −9.54 | 6.25 | 0.07 |
| Body Mass Index [BMI] (kg/m2) | 28.5 | 5.1 | 28.0 | 4.2 | 0.68 | 0.497 | −1.03 | 2.12 | 0.11 |
| Pre-op Knee Society Score [KSS] Knee | 27.8 | 15.7 | 37.9 | 17.3 | −3.82 | <0.001 | −15.35 | −4.90 | 0.63 |
| Pre-op KSS Function | 29.6 | 20.3 | 41.8 | 16.7 | −4.18 | <0.001 | −17.91 | −6.38 | 0.62 |
| Pre-op KSS Total | 57.4 | 32.9 | 79.7 | 29.4 | −4.24 | <0.001 | −32.64 | −11.90 | 0.70 |
| Pre-op subluxated patella (%) | 0.3 | 0.5 | 0.4 | 0.5 | −0.91 | 0.364 | −0.23 | 0.08 | 0.15 |
| Pre-op valgus (°) | 21.6 | 7.2 | 16.6 | 6.3 | 4.31 | <0.001 | 2.69 | 7.24 | 0.71 |
| LA (n = 143) | MA (n = 50) | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | LL | UL | d Cohen’s | |
| Post-op ROM (°) | 117 | 13.6 | 115.6 | 13.3 | 0.66 | 0.51 | −2.91 | 5.84 | 0.11 |
| Post-op KSS Knee | 85.3 | 9.7 | 77.4 | 14.4 | 3.61 | <0.001 | 3.53 | 12.25 | 0.71 |
| Post-op KSS Function | 69.9 | 15.0 | 71.8 | 14.7 | −0.79 | 0.431 | −6.79 | 2.91 | 0.13 |
| Post-op KSS Total | 155.2 | 19.5 | 149.2 | 25.0 | 1.72 | 0.087 | −0.88 | 12.77 | 0.28 |
| PS designs | 0.7 | 0.5 | 0.9 | 0.3 | −3.00 | 0.003 | −0.30 | −0.06 | 0.42 |
| CCK designs | 0.3 | 0.5 | 0.1 | 0.3 | 3.37 | 0.001 | 0.08 | 0.31 | 0.46 |
| Surgery time (min.) | 81.0 | 11.8 | 91.4 | 21.2 | −3.26 | 0.002 | −16.65 | −4.00 | 0.70 |
| Post-op valgus (°) | 6.0 | 2.9 | 5.2 | 2.3 | 1.71 | 0.089 | −0.12 | 1.68 | 0.28 |
| Angle of correction (°) | 15.6 | 7.5 | 11.4 | 6.8 | 3.52 | 0.001 | 1.87 | 6.63 | 0.58 |
| Non-RA (n = 107) | RA (n = 36) | ||||||
|---|---|---|---|---|---|---|---|
| M | Me | M | Me | Z | p | η2 | |
| Age at the time of surgery (years) | 70.6 | 71.0 | 60.9 | 64.0 | −4.30 | <0.001 | 0.13 |
| Woman (%) | 0.9 | 1.0 | 0.9 | 1.0 | −0.49 | 0.627 | 0.00 |
| Pre-op ROM (°) | 102.1 | 105.0 | 98.8 | 105.0 | −0.64 | 0.521 | 0.00 |
| Post-op ROM (°) | 116.4 | 120.0 | 119.0 | 120.0 | −0.69 | 0.491 | 0.00 |
| BMI (kg/m2) | 29.2 | 28.7 | 26.7 | 24.9 | −2.67 | 0.008 | 0.05 |
| Pre-op KSS Knee | 27.9 | 29.0 | 27.6 | 27.5 | −0.05 | 0.957 | 0.00 |
| Pre-op KSS Function | 29.4 | 30.0 | 30.1 | 37.5 | −0.35 | 0.729 | 0.00 |
| Pre-op KSS Total | 57.3 | 65.0 | 57.7 | 66.0 | −0.15 | 0.882 | 0.00 |
| Post-op KSS Knee | 85.3 | 88.0 | 85.3 | 88.0 | −0.60 | 0.551 | 0.00 |
| Post-op KSS Function | 70.5 | 70.0 | 68.1 | 70.0 | −0.93 | 0.355 | 0.01 |
| Post-op KSS Total | 155.8 | 157.0 | 153.4 | 157.5 | −0.45 | 0.652 | 0.00 |
| PS designs | 0.7 | 1.0 | 0.8 | 1.0 | −1.60 | 0.109 | 0.02 |
| CCK designs | 0.3 | 0.0 | 0.2 | 0.0 | −1.51 | 0.132 | 0.02 |
| Pre-op subluxated patella (%) | 0.4 | 0.0 | 0.3 | 0.0 | −1.16 | 0.247 | 0.01 |
| Surgery time (min.) | 81.3 | 80.0 | 80.4 | 77.0 | −0.74 | 0.461 | 0.00 |
| Pre-op valgus (°) | 21.9 | 21.0 | 20.5 | 20.0 | −0.98 | 0.328 | 0.01 |
| Post-op valgus (°) | 5.8 | 6.0 | 6.6 | 6.0 | −1.27 | 0.204 | 0.01 |
| Angle of correction (°) | 16.2 | 15.0 | 13.9 | 13.0 | −1.44 | 0.151 | 0.01 |
| Complication | Lateral Approach (No./%) | Medial Approach (No./%) |
|---|---|---|
| Peroneal nerve palsy | 1/0.7% | 4/8% |
| Acute, early Periprosthetic Joint Infection [PJI] | 1/0.7% | 1/2% |
| Wound-healing problems | 4/2.8% | 1/2% |
| Persistent patella dislocation | 1/0.7% | 1/2% |
| Medial instability | 2/1.4% | - |
| Aseptic loosening | 1/0.7% | - |
| Total | 10/9% | 7/14% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dudek, P.; Marczak, D.; Okoń, T.; Grzelecki, D.; Szneider, J.; Kowalczewski, J. Lateral or Medial Parapatellar Surgical Approach to the Valgus Osteoarthritic Knee? A Retrospective Single-Center Study. J. Clin. Med. 2022, 11, 5953. https://doi.org/10.3390/jcm11195953
Dudek P, Marczak D, Okoń T, Grzelecki D, Szneider J, Kowalczewski J. Lateral or Medial Parapatellar Surgical Approach to the Valgus Osteoarthritic Knee? A Retrospective Single-Center Study. Journal of Clinical Medicine. 2022; 11(19):5953. https://doi.org/10.3390/jcm11195953
Chicago/Turabian StyleDudek, Piotr, Dariusz Marczak, Tomasz Okoń, Dariusz Grzelecki, Jan Szneider, and Jacek Kowalczewski. 2022. "Lateral or Medial Parapatellar Surgical Approach to the Valgus Osteoarthritic Knee? A Retrospective Single-Center Study" Journal of Clinical Medicine 11, no. 19: 5953. https://doi.org/10.3390/jcm11195953
APA StyleDudek, P., Marczak, D., Okoń, T., Grzelecki, D., Szneider, J., & Kowalczewski, J. (2022). Lateral or Medial Parapatellar Surgical Approach to the Valgus Osteoarthritic Knee? A Retrospective Single-Center Study. Journal of Clinical Medicine, 11(19), 5953. https://doi.org/10.3390/jcm11195953