
Pre-Existing Hypertension Is Related with Disproportions in T-Lymphocytes in Older Age


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Body Composition
2.3. Blood Sampling
2.4. Flow Cytometry Analysis
2.5. Cytomegalovirus (CMV) IgG
2.6. Haematological Variables
2.7. Biochemical Variables
2.8. Statistical Analysis
3. Results
3.1. Body Composition
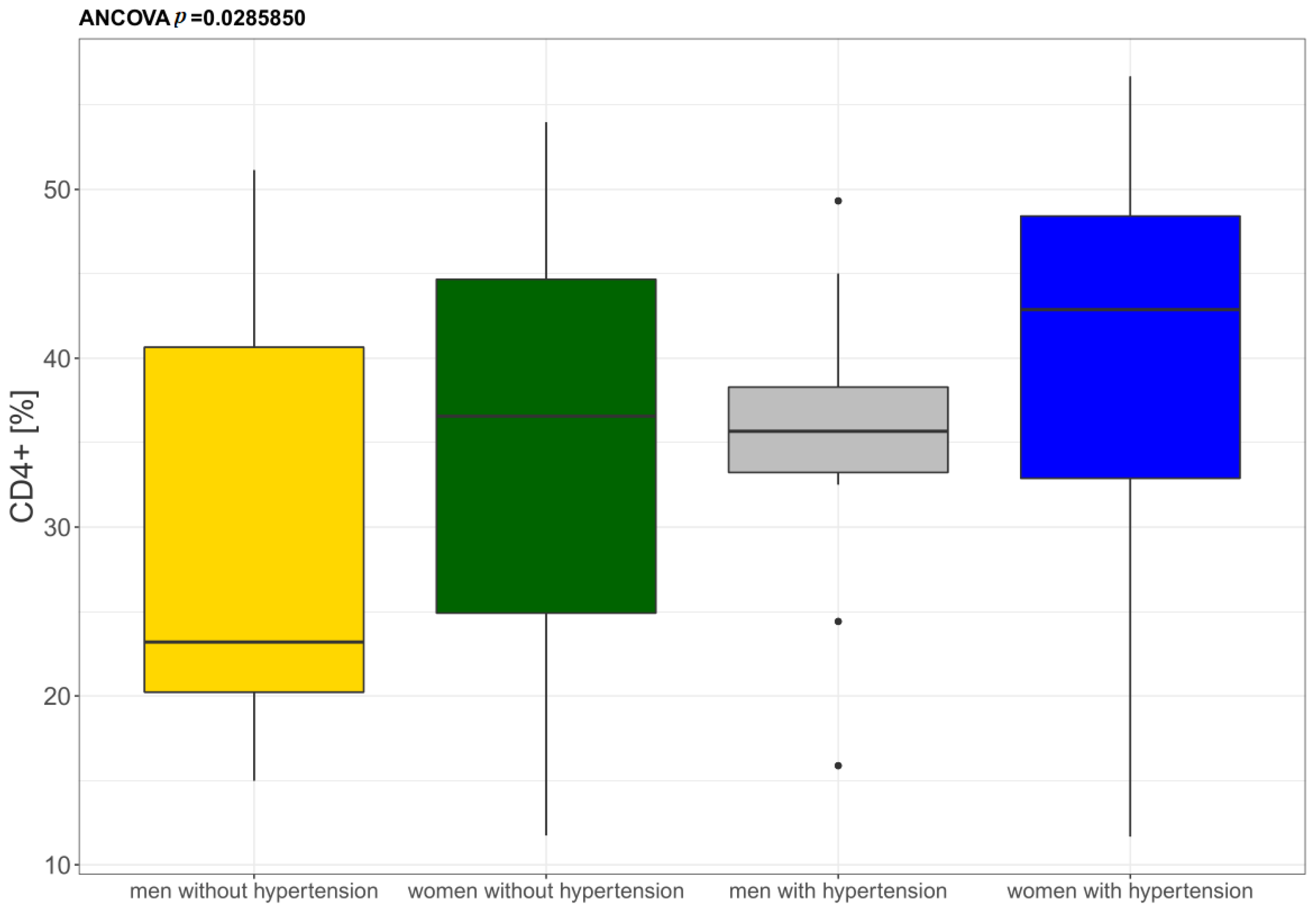
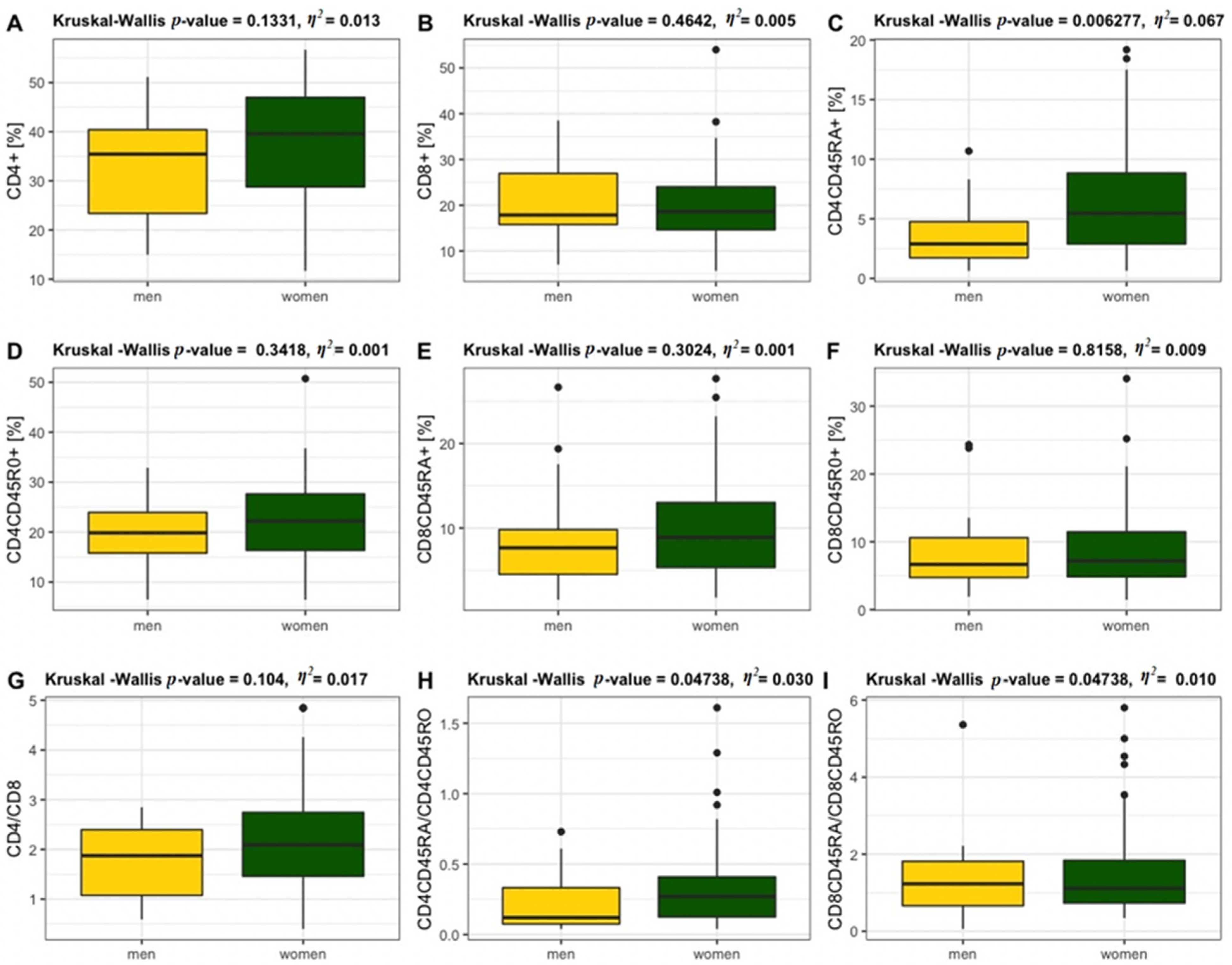
3.2. Flow Cytometry Analysis
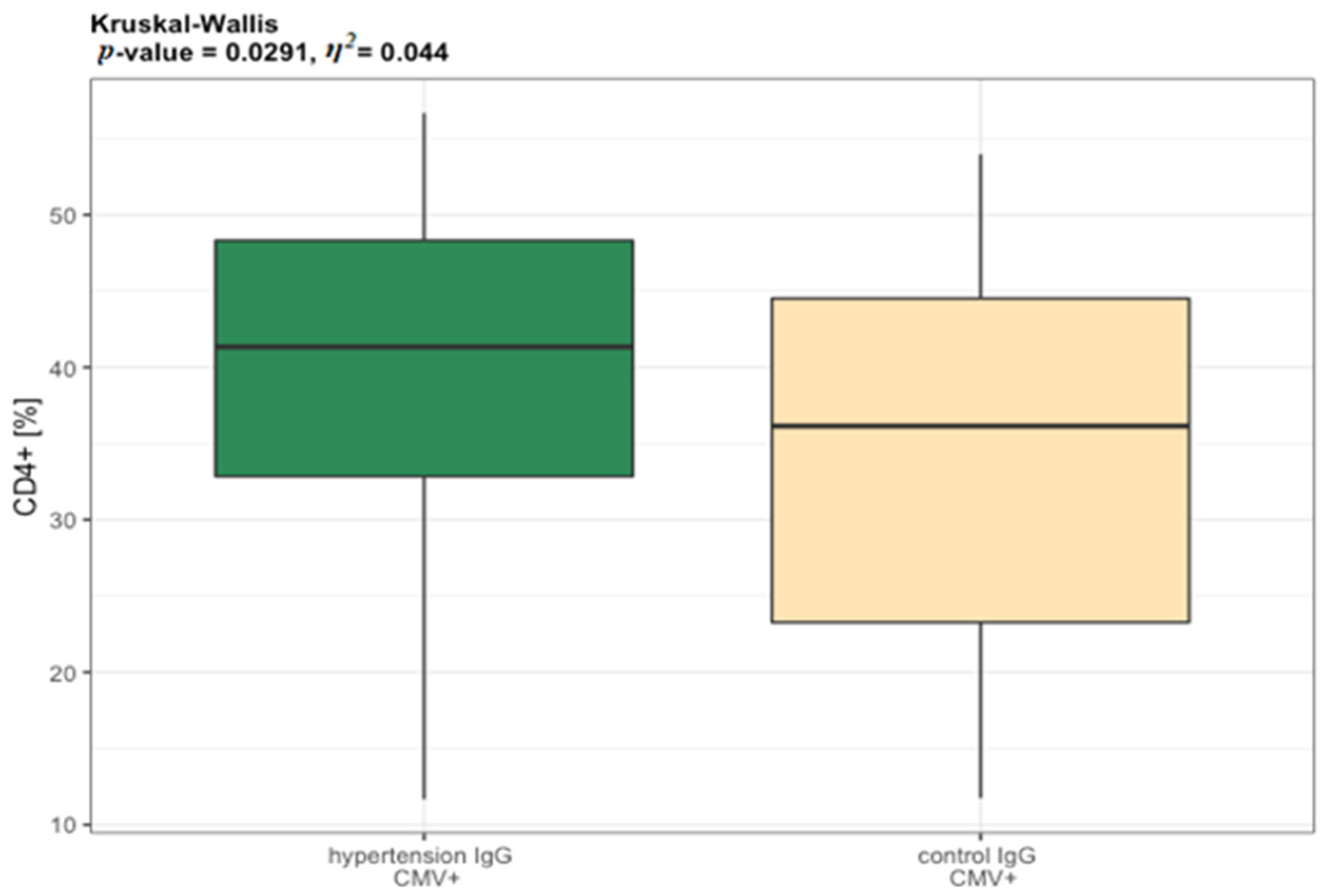
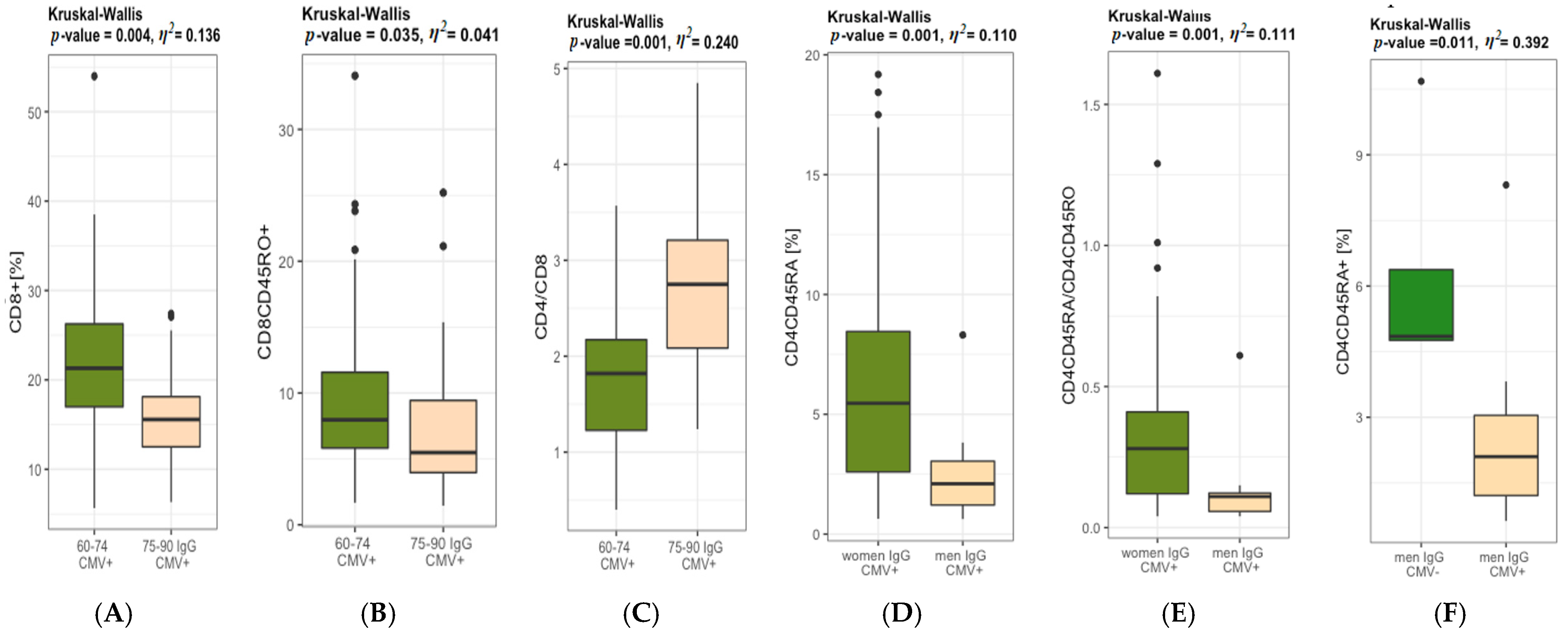
3.3. CMV IgG Status and Immune Cells
3.4. Haematological Variables
3.5. Biochemical Variables
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alam, I.; Goldeck, D.; Larbi, A.; Pawelec, G. Aging affects the proportions of T and B cells in a group of elderly men in a developing country-a pilot study from Pakistan. Age 2012, 35, 1521–1530. [Google Scholar] [CrossRef]
- Yan, J.; Greer, J.M.; Hull, R.; O’Sullivan, J.D.; Henderson, R.D.; Read, S.J.; McCombe, P.A. The effect of ageing on human lymphocyte subsets: Comparison of males and females. Immun. Ageing 2010, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Lewkiewicz, S.; Chuang, Y.-L.; Chou, T. A Mathematical Model of the Effects of Aging on Naive T Cell Populations and Diversity. Bull. Math. Biol. 2019, 81, 2783–2817. [Google Scholar] [CrossRef] [PubMed]
- Fagnoni, F.F.; Vescovini, R.; Passeri, G.; Bologna, G.; Pedrazzoni, M.; Lavagetto, G.; Casti, A.; Franceschi, C.; Passeri, M.; Sansoni, P. Shortage of circulating naive CD8+ T cells provides new insights on immunodeficiency in aging. Blood 2000, 95, 2860–2868. [Google Scholar] [CrossRef] [PubMed]
- Globerson, A.; Effros, R.B. Ageing of lymphocytes and lymphocytes in the aged. Immunol. Today 2000, 21, 515–521. [Google Scholar] [CrossRef]
- Hazeldine, J.; Lord, J.M. Immunesenescence: A Predisposing Risk Factor for the Development of COVID-19? Front. Immunol. 2020, 11, 573662. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Ostan, R.; Monti, D.; Gueresi, P.; Bussolotto, M.; Franceschi, C.; Baggio, G. Gender, aging and longevity in humans: An update of an intriguing/neglected scenario paving the way to a gender-specific medicine. Clin. Sci. 2016, 130, 1711–1725. [Google Scholar] [CrossRef] [Green Version]
- Strindhall, J.; Skog, M.; Ernerudh, J.; Bengner, M.; Löfgren, S.; Matussek, A.; Nilsson, B.O.; Wikby, A. The inverted CD4/CD8 ratio and associated parameters in 66-year-old individuals: The Swedish HEXA immune study. Age 2012, 35, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Vasson, M.-P.; Farges, M.-C.; Goncalves-Mendes, N.; Talvas, J.; Ribalta, J.; Winklhofer-Roob, B.; Rock, E.; Rossary, A. Does aging affect the immune status? A comparative analysis in 300 healthy volunteers from France, Austria and Spain. Immun. Ageing 2013, 10, 38. [Google Scholar] [CrossRef]
- Guzik, T.J.; Hoch, N.E.; Brown, K.A.; McCann, L.A.; Rahman, A.; Dikalov, S.; Goronzy, J.; Weyand, C.; Harrison, D.G. Role of the T cell in the genesis of angiotensin II–induced hypertension and vascular dysfunction. J. Exp. Med. 2007, 204, 2449–2460. [Google Scholar] [CrossRef]
- Rai, A.; Narisawa, M.; Li, P.; Piao, L.; Li, Y.; Yang, G.; Cheng, X.W. Adaptive immune disorders in hypertension and heart failure: Focusing on T-cell subset activation and clinical implications. J. Hypertens. 2020, 38, 1878–1889. [Google Scholar] [CrossRef]
- Durstine, J.L.; Moore, G.E. ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- World Health Organization. Document Number: WHO/NMH/NPH/01.2 2001; 55p. Available online: https://apps.who.int/iris/handle/10665/66941 (accessed on 9 October 2021).
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Tylutka, A.; Morawin, B.; Gramacki, A.; Zembron-Lacny, A. Lifestyle exercise attenuates immunosenescence; flow cytometry analysis. BMC Geriatr. 2021, 21, 200. [Google Scholar] [CrossRef]
- VanItallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hang, J.; Huang, J.; Zhou, S.; Wu, L.; Zhu, Y.; Zhu, L.; Zhou, H.; Xu, K.; Jiang, H.; Yang, X. The clinical implication of CD45RA+ naïve T cells and CD45RO+ memory T cells in advanced pancreatic cancer: A proxy for tumor biology and outcome prediction. Cancer Med. 2019, 8, 1326–1335. [Google Scholar] [CrossRef] [Green Version]
- McBride, J.A.; Striker, R. Imbalance in the game of T cells: What can the CD4/CD8 T cell ratio tell us about HIV and health. PLoS Pathog. 2017, 13, e1006624. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 9 October 2021).
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Erbaum Press: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Miles, J.; Shevlin, M. Applying Regression and Correlation: A Guide for Students and Researchers; Sage: London, UK, 2001. [Google Scholar]
- Radovanović, D.; Stoickov, V.; Ignjatović, A.; Scanlan, A.T.; Jakovljević, V.; Stojanović, E. A comparison of cardic structure and function between female powerlifters, fitness-oriented athletes, and sedentary controls. Echocardiography 2020, 37, 1566–1573. [Google Scholar] [CrossRef]
- Hu, B.; Jadhav, R.R.; Gustafson, C.E.; Le Saux, S.; Ye, Z.; Li, X.; Tian, L.; Weyand, C.M.; Goronzy, J.J. Distinct age-related epi-genetic eignatures in CD4 and CD8 T cells. Front. Immunol. 2020, 11, 585168. [Google Scholar] [CrossRef]
- Yu, H.T.; Shin, E.-C. T Cell Immunosenescence, Hypertension, and Arterial Stiffness. Epidemiol. Health 2014, 36, e2014005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youn, J.C.; Yu, H.T.; Lim, B.J.; Koh, M.J.; Lee, J.; Chang, D.Y.; Choi, Y.S.; Lee, S.H.; Kang, S.M.; Jang, Y.; et al. Immunosenescent CD8+ T cells and C-X-C chemokine receptor type 3 chemokines are increased in human hypertension. Hypertension 2013, 62, 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, X.; Wang, A.; Zhang, L.; Shan, L.-Y.; Zhang, H.-C.; Li, L.; Si, J.-Q.; Luo, J.; Li, X.-Z.; Ma, K.-T. Up-regulation of gap junction in peripheral blood T lymphocytes contributes to the inflammatory response in essential hypertension. PLoS ONE 2017, 12, e0184773. [Google Scholar] [CrossRef] [Green Version]
- Itani, H.A.; McMaster, W.G., Jr.; Saleh, M.A.; Nazarewicz, R.R.; Mikolajczyk, T.P.; Kaszuba, A.M.; Konior, A.; Prejbisz, A.; Januszewicz, A.; Norlander, A.E.; et al. Activation of human T cells in hypertension: Studies of humanized mice and hypertensive humans. Hypertension 2016, 68, 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso-Fernandez, P.; De la Fuenta, M. Role of the immune system in aging and longevity. Curr. Aging Sci. 2011, 4, 78–100. [Google Scholar] [CrossRef]
- Ji, H.; Zheng, W.; Li, X.; Liu, J.; Wu, X.; Zhang, M.A.; Umans, J.G.; Hay, M.; Speth, R.C.; Dunn, S.E.; et al. Sex- specific T cells regulation of angiotensin II dependent hypertension RR. Hypertension 2014, 64, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Sandberg, K.; Ji, H.; Einstein, G.; Au, A.; Hay, M. Is immune system-related hypertension associated with ovarian hormone deficiency? Exp. Physiol. 2016, 101, 368–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, J.; Qu, Y.-Y.; Tang, N.; Liu, Y.-M.; Zhong, H.; Wang, L.-M.; Feng, Q.; Li, Z.; He, F. Association of cytomegalovirus infection with hypertension risk: A meta-analysis. Wien. Klin. Wochenschr. 2016, 128, 586–591. [Google Scholar] [CrossRef] [Green Version]
- Arnold, C.R.; Wolf, J.; Brunner, S.; Herndler-Brandstetter, D.; Grubeck-Loebenstein, B. Gain and loss of T cells subset in old age–age related reshaping of the T cells repertoire. J. Clin. Immunol. 2011, 31, 137–146. [Google Scholar] [CrossRef]
- Gupta, S.; Gollapudi, S. TNF-α-induced apoptosis in human naïve and memory CD8+ T cells in aged humans. Exp. Gerontol. 2005, 41, 69–77. [Google Scholar] [CrossRef]
- Goronzy, J.J.; Lee, W.-W.; Weyand, C.M. Aging and T-cell diversity. Exp. Gerontol. 2007, 42, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Moro-García, M.A.; Alonso-Arias, R.; López-Vázquez, A.; Suárez-García, F.M.; Solano-Jaurrieta, J.J.; Baltar, J.; López-Larrea, C. Relationship between functional ability in older people, immune system status, and intensity of response to CMV. Age 2011, 34, 479–495. [Google Scholar] [CrossRef] [PubMed]
- Adriaensen, W.; Derhovanessian, E.; Vaes, B.; van Pottelbergh, G.; Degryse, J.-M.; Pawelec, G.; Hamprecht, K.; Theeten, H.; Matheï, C. CD4:8 Ratio > 5 Is Associated With a Dominant Naive T-Cell Phenotype and Impaired Physical Functioning in CMV–Seropositive Very Elderly People: Results From the BELFRAIL Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikby, A.; Månsson, I.A.; Johansson, B.; Strindhall, J.; Nilsson, S.E. The immune risk profile is associated with age and gender: Findings from three Swedish population studies of individuals 20–100 years of age. Biogerontology 2008, 9, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Hirokawa, K.; Utsuyama, M.; Hayashi, Y.; Kitagawa, M.; Makinodan, T.; Fulop, T. Slower immune system aging in women versus men in the Japanese population. Immun. Ageing 2013, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Dudkowska, M.; Janiszewska, D.; Karpa, A.; Broczek, K.; Dabrowski, M.; Sikora, E. The role of gender and labour status in immunosenescence of 65+ Polish population. Biogerontology 2017, 18, 581–590. [Google Scholar] [CrossRef] [Green Version]
- Barbé-Tuana, F.; Funchal, G.; Schmitz, C.R.R.; Maurmann, R.; Bauer, M.E. The interplay between immunosenescence and age-related diseases. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–13. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hypertension n = 51 | Control n = 48 | Hypertension vs. Control p-Value | η2 | |
|---|---|---|---|---|
| Mean ± SD (Me) | Mean ± SD (Me) | |||
| Age (years) | 72.3 ± 5.9 (72.0) | 70.2 ±5.5 (70.0) | 0.152 | 0.010 |
| Weight (kg) | 72.3 ± 10.6 (70.1) | 67.1± 9.7 (68.0) | 0.014 | 0.061 |
| Height (cm) | 162.1 ± 6.9 (162.1) | 159.4 ± 4.9 (159.0) | 0.038 | 0.034 |
| BMI (kg/m2) | 27.6 ±3.6 (27.1) | 26.4 ± 3.4 (25.8) | 0.090 | 0.019 |
| BMI 18.5–24.9 kg/m2 (%) | 24.0 | 38.8 | ||
| BMI 25–29.9 kg/m2 (%) | 56.0 | 42.8 | ||
| BMI ≥ 30 kg/m2 (%) | 20.0 | 18.4 | ||
| MM (kg) | 44.7 ± 7.8 (4264) | 42.2 ± 6.0 (40.9) | 0.083 | 0.034 |
| FFM (kg) | 47.5 ± 8.1 (45.4) | 44.2 ± 6.2 (43.5) | 0.035 | 0.035 |
| FFMI (kg/m2) | 18.0 ± 2.3 (17.6) | 17.4 ± 1.9 (16.9) | 0.118 | 0.015 |
| FM (kg) | 24.8 ± 5.6 (24.7) | 22.9 ± 5.8 (22.8) | 0.089 | 0.029 |
| FM% | 34.3 ± 5.6 (35.3) | 33.8 ± 5.2 (34.4) | 0.099 | 0.028 |
| FMI (kg/m2) | 9.5 ± 2.4 (9.5) | 9.0 ± 2.3 (8.8) | 0.263 | 0.007 |
| SBP (mmHg) | 150.9 ± 18.5 (149.5) | 142.1 ± 18.6 (144.0) | 0.022 | 0.054 |
| DBP (mmHg) | 81.2 ± 11.9 (82.0) | 82.6 ± 15.8 (78.0) | 0.945 | 0.010 |
| 60–74 Years n = 63 | 75–90 Years n = 36 | 60–74 Years vs. 75–90 Years p-Value | Females n = 83 | Males n = 16 | Females vs. Males p-Value | |
|---|---|---|---|---|---|---|
| Mean ± SD (Me) | Mean ± SD (Me) | Mean ± SD (Me) | Mean ± SD (Me) | |||
| Age (years) | 67.9 ± 3.5 (68.0) | 77.7 ±3.5 (76.5) | 0.001 | 70.8 ± 5.8 (70.0) | 73.6 ± 5.5 (72.0) | 0.087 |
| Weight (kg) | 70.1 ± 9.7 (68.7) | 69.1± 12.1 (68.5) | 0.100 | 68.6 ± 9.5 (68.1) | 75.9 ± 13.4 (74.5) | 0.009 |
| Height (cm) | 161.5 ± 5.9 (161.0) | 159.4 ± 6.4 (159.0) | 0.642 | 159.5 ± 4.9 (159.0) | 167.3 ± 7.7 (169.5) | 0.001 |
| BMI (kg/m2) | 26.9 ± 3.1 (26.7) | 27.3 ± 4.3 (26.7) | 0.754 | 27.0 ± 3.6 (26.7) | 27.2 ± 3.6 (26.6) | 0.665 |
| MM (kg) | 43.8 ± 6.9 (42.2) | 33.9 ± 5.5 (34.7) | 0.319 | 41.0 ± 3.7 (41.0) | 57.6 ± 4.5 (56.0) | 0.001 |
| FFM (kg) | 46.3 ± 7.5 (44.5) | 45.1 ± 7.4 (44.1) | 0.546 | 44.2 ± 5.1 (44.3) | 54.6 ± 11.2 (57.9) | 0.001 |
| FFMI (kg/m2) | 17.2 ± 2.0 (17.2) | 17.7 ± 2.4 (17.4) | 0.785 | 17.4 ± 1.8 (17.1) | 19.4 ± 3.0 (20.2) | 0.004 |
| FM (kg) | 23.8 ± 5.4 (23.3) | 24.0 ± 6.7 (22.6) | 0.870 | 24.4 ± 5.6 (23.4) | 21.3 ± 6.3 (20.0) | 0.055 |
| FM% | 33.9 ± 5.5 (34.7) | 34.3 ± 5.3 (35.0) | 0.683 | 35.2 ± 4.2 (35.1) | 28.2 ± 7.2 (27.7) | 0.001 |
| FMI (kg/m2) | 9.2 ± 2.2 (9.2) | 9.5 ± 2.7 (9.4) | 0.525 | 9.6 ± 2.2 (9.4) | 7.7 ± 2.5 (7.0) | 0.003 |
| SBP (mmHg) | 143.2 ± 18.7 (143.5) | 153.2 ± 17.9 (151.0) | 0.013 | 146.3 ± 18.7 (147.0) | 148.3 ± 20.8 (147.0) | 0.713 |
| DBP (mmHg) | 82.6 ± 14.8 (78.5) | 80.8 ± 10.7 (82.0) | 0.816 | 81.7 ± 13.7 (79.0) | 83.7 ± 12.5 (83.0) | 0.500 |
| T Lymphocytes | Hypertension n = 51 | Control n = 48 | Hypertension vs. Control p-Value | η2 |
|---|---|---|---|---|
| (%) | Mean ± SD (Me) | Mean ± SD (Me) | ||
| CD4+ | 39.4 ± 10.7 (40.2) | 34.3 ± 11.7 (36.4) | 0.041 | 0.033 |
| CD8+ | 19.9 ± 6.5 (18.4) | 19.2 ± 9.3 (18.9) | 0.446 | 0.004 |
| CD4CD45RA+ | 6.3 ± 4.1 (5.3) | 5.7 ± 4.5 (4.1) | 0.245 | 0.003 |
| CD4CD45RO+ | 22.7 ± 7.3 (22.7) | 20.4 ± 8.2 (19.3) | 0.086 | 0.020 |
| CD8CD45RA+ | 9.4 ± 5.0 (8.6) | 10.3 ± 6.7 (8.7) | 0.897 | 0.010 |
| CD8CD45RO+ | 8.9 ± 5.1 (7.5) | 8.8 ± 6.4 (6.5) | 0.456 | 0.005 |
| CD4/CD8 | 2.2 ± 0.9 (2.0) | 2.1 ± 0.9 (2.1) | 0.766 | 0.009 |
| <1 | 4.0 | 12.2 | ||
| ≥1 or ≤2.5 | 62.0 | 59.2 | ||
| >2.5 | 34.0 | 28.6 | ||
| CD4CD45RA/CD4CD45RO | 0.3 ± 0.3 (0.2) | 0.3 ± 0.2 (0.2) | 0.698 | 0.009 |
| CD8CD45RA/CD8CD45RO | 1.4 ± 1.1 (1.1) | 1.5 ± 1.1 (1.2) | 0.437 | 0.004 |
| Reference Values | Hypertension n = 51 | Control n = 48 | Hypertension vs. Control p-Value | η2 | |
|---|---|---|---|---|---|
| Mean ± SD (Me) | Mean ± SD (Me) | ||||
| Leukocytes (103/µL) | 5.0–11.6 | 6.9 ± 2.0 (6.6) | 6.2 ± 1.5 (6.1) | 0.081 | 0.021 |
| Lymphocytes (103/µL) | 1.3–4.0 | 2.2 ± 0.7 (2.2) | 2.2 ± 0.7 (2.1) | 0.351 | 0.001 |
| Granulocytes (103/µL) | 2.4–7.6 | 4.2 ± 1.6 (3.9) | 3.6 ± 1.2 (3.5) | 0.124 | 0.014 |
| LYM% | 19.1–48.5 | 33.3 ± 9.0 (33.2) | 35.2 ± 9.0 (35.0) | 0.303 | 0.002 |
| GRA% | 43.6–73.4 | 59.3 ± 9.5 (58.7) | 56.4 ± 10.1 (56.6) | 0.153 | 0.014 |
| RBC (103/µL) | F 4.0–5.5 M 4.5–6.6 | 4.8 ± 0.3 (4.8) | 4.8 ± 0.3 (4.8) | 0.916 | 0.000 |
| HB (g/dL) | F 12.5–16.0 M 13.5–18.0 | 13.8 ± 0.7 (13.7) | 13.9 ± 0.8 (13.9) | 0.439 | 0.006 |
| HCT (%) | F 37–47 M 40.0–51.0 | 39.4 ± 2.3 (39.1) | 39.8 ± 2.4 (39.5) | 0.470 | 0.005 |
| MCV (fL) | F 80–95 M 80–97 | 81.6 ± 2.5 (82.0) | 82.3 ± 3.5 (82.0) | 0.346 | 0.001 |
| MCH (pg) | F 27.0–32.0 M 26.0–32.0 | 28.6 ± 1.0 (28.5) | 28.8 ± 1.4 28.7) | 0.412 | 0.007 |
| MCHC (g/dL) | F 32.0–36.0 M 31.0–36.0 | 35.0 ± 0.8 (35.2) | 35.0 ± 0.7 (35.0) | 0.604 | 0.007 |
| PLT (103/µL) | 150–400 | 265.9 ± 57.4 (257.5) | 236.8 ± 65.1(247.0) | 0.293 | 0.001 |
| Reference Values | Hypertension n = 51 | Control n = 48 | Hypertension vs. Control p-Value | η2 | |
|---|---|---|---|---|---|
| Mean ± SD (Me) | Mean ± SD (Me) | ||||
| Glucose (mg/dL) | 60–115 | 96.6 ± 13.7 (93.0) | 95.4 ± 13.5 (92.8) | 0.592 | 0.007 |
| TC (mg/dL) | <200 | 237.6 ± 56.3 (234.0) | 250.4 ± 50.1 (245.0) | 0.240 | 0.014 |
| TG (mg/dL) | <150 | 120.3 ± 51.5 (115.8) | 124.5 ± 65.1 (119.5) | 0.933 | 0.010 |
| HDL (mg/dL) | desirable >60 | 80.1 ± 15.8 (80.1) | 79.3 ± 12.0 (81.0) | 0.980 | 0.010 |
| LDL (mg/dL) | <130 | 129.7 ± 49.8 (125.3) | 140.1 ± 41.7 (136.8) | 0.267 | 0.013 |
| non-HDL (mg/dL) | <130 | 157.5 ± 60.7 (60.7) | 171.1 ± 48.1 (165.9) | 0.226 | 0.006 |
| oxLDL | - | 413.5 ± 424.2 (127.9) | 531.7 ± 455.8 (381.8) | 0.567 | 0.007 |
| CRP (mg/L) | 0.068–8.2 | 2.6 ± 2.4 (1.9) | 2.6 ± 2.4 (1.9) | 0.972 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tylutka, A.; Morawin, B.; Gramacki, A.; Zembron-Lacny, A. Pre-Existing Hypertension Is Related with Disproportions in T-Lymphocytes in Older Age. J. Clin. Med. 2022, 11, 291. https://doi.org/10.3390/jcm11020291
Tylutka A, Morawin B, Gramacki A, Zembron-Lacny A. Pre-Existing Hypertension Is Related with Disproportions in T-Lymphocytes in Older Age. Journal of Clinical Medicine. 2022; 11(2):291. https://doi.org/10.3390/jcm11020291
Chicago/Turabian StyleTylutka, Anna, Barbara Morawin, Artur Gramacki, and Agnieszka Zembron-Lacny. 2022. "Pre-Existing Hypertension Is Related with Disproportions in T-Lymphocytes in Older Age" Journal of Clinical Medicine 11, no. 2: 291. https://doi.org/10.3390/jcm11020291
APA StyleTylutka, A., Morawin, B., Gramacki, A., & Zembron-Lacny, A. (2022). Pre-Existing Hypertension Is Related with Disproportions in T-Lymphocytes in Older Age. Journal of Clinical Medicine, 11(2), 291. https://doi.org/10.3390/jcm11020291