
Micro-Elimination of Hepatitis C among Patients with Kidney Disease by Using Electronic Reminder System—A Hospital-Based Experience

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
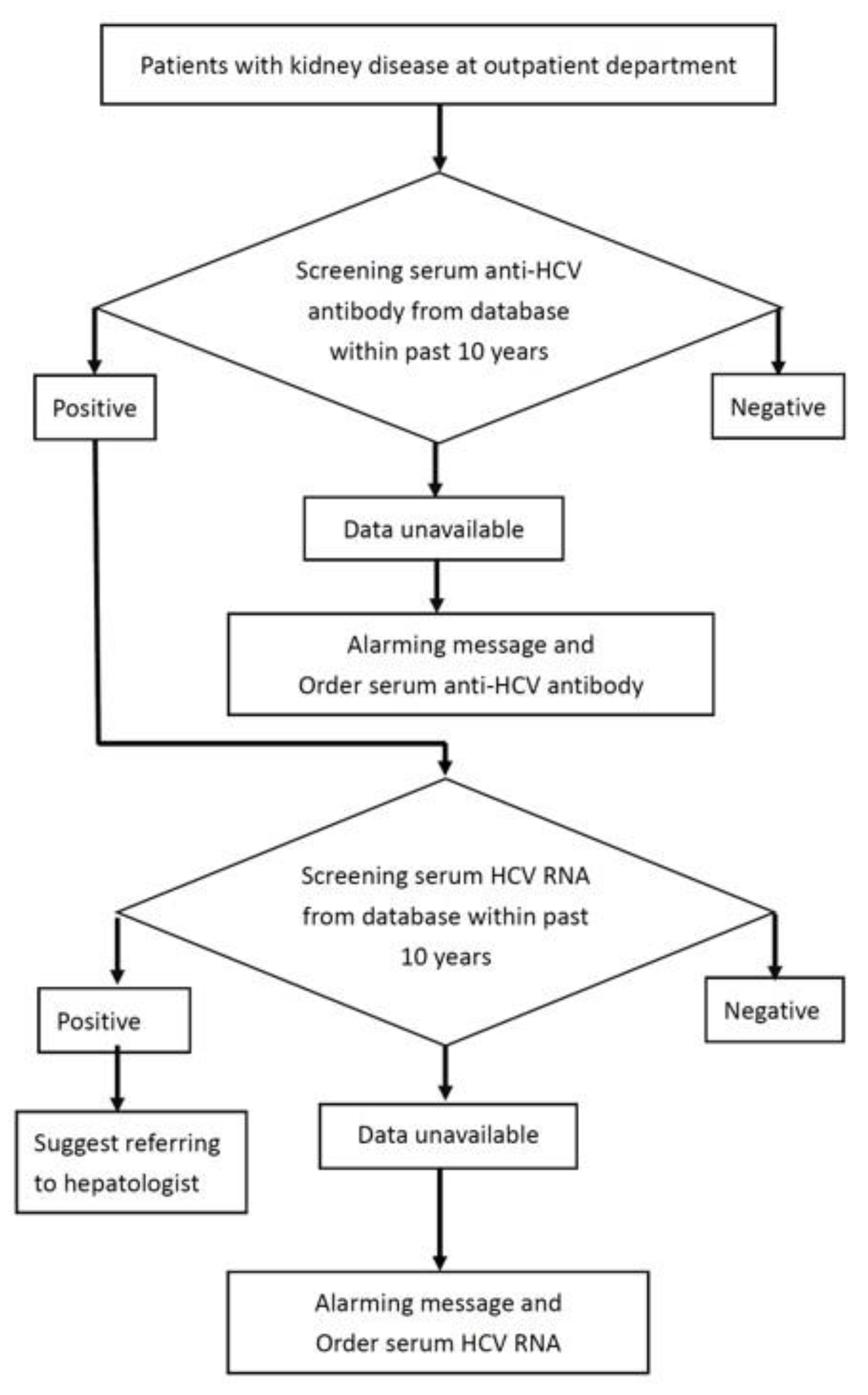
2.2. Alert System Implementation
2.3. HCV Testing
2.4. Statistical Analysis
3. Results
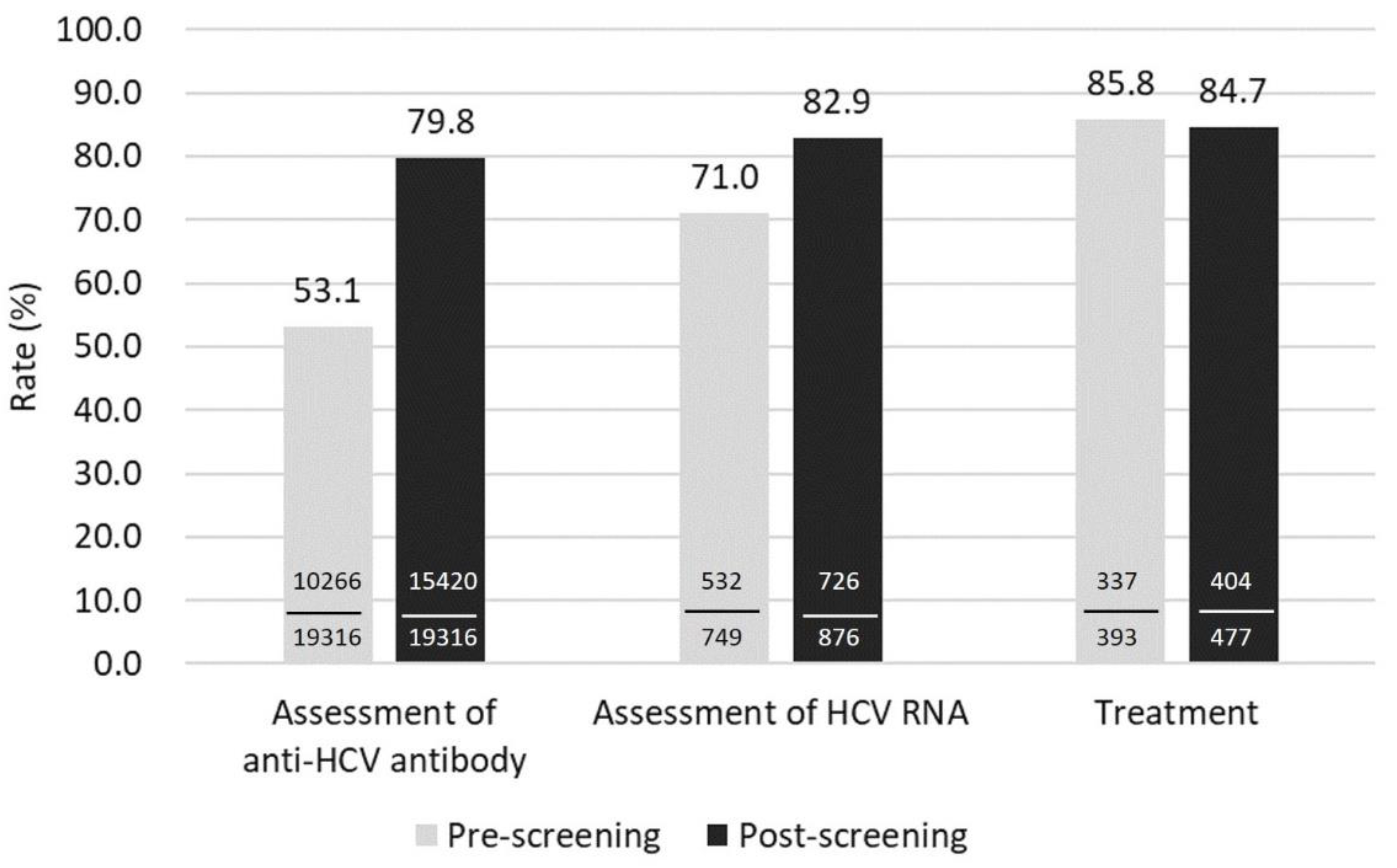
3.1. HCV Screening Rate
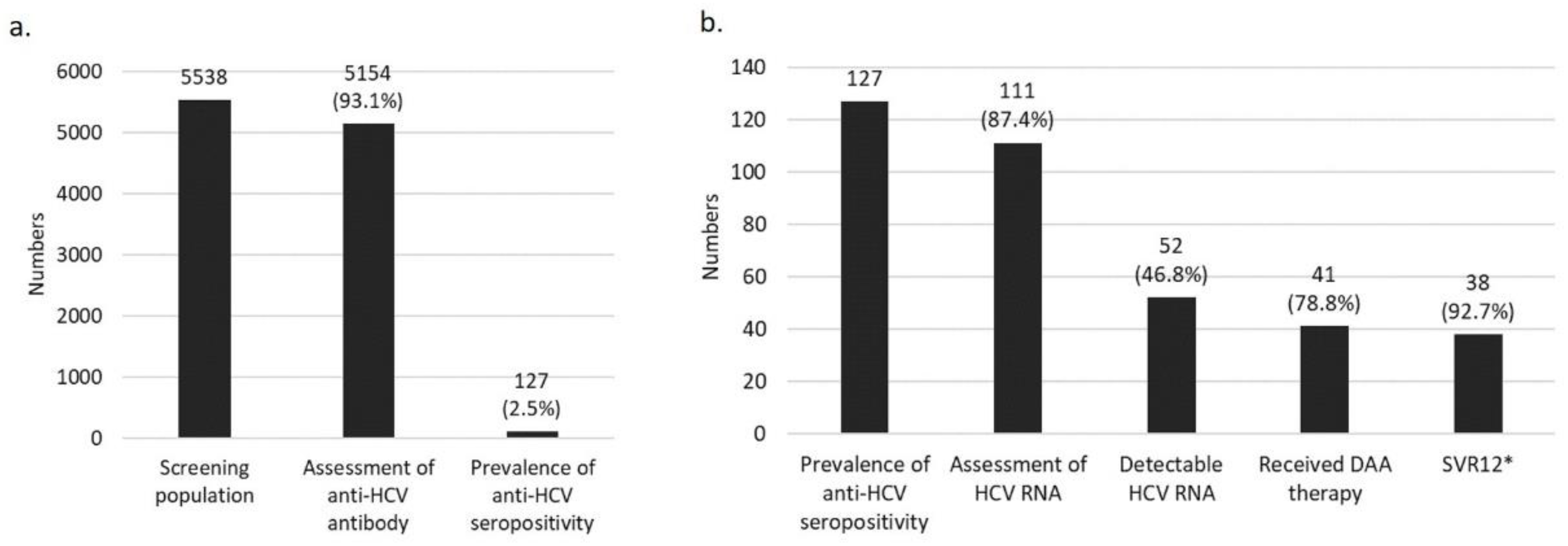
3.2. HCV Cascade of Care
3.3. HCV Testing Results
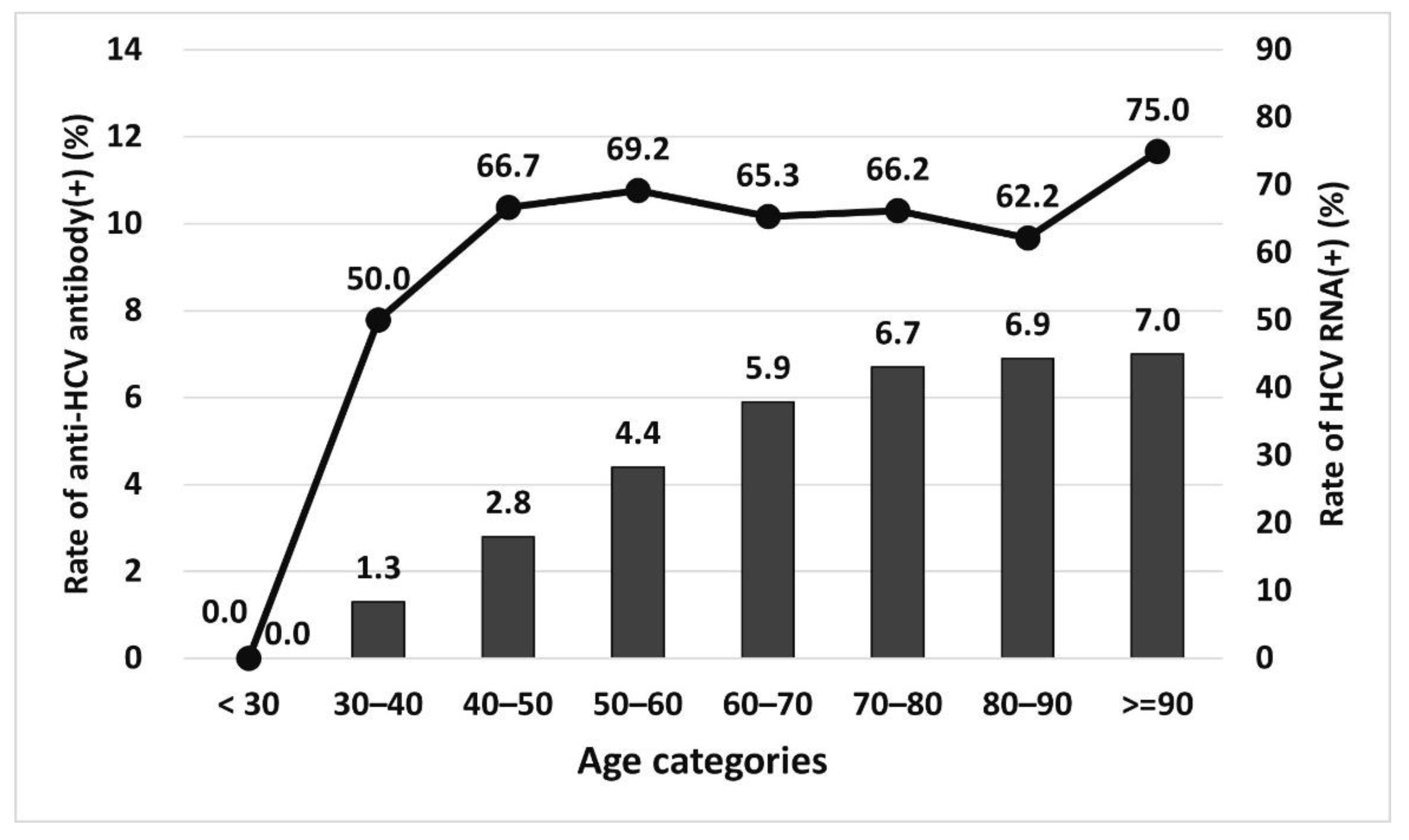
3.4. HCV Prevalence in Different Age Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Negro, F.; Forton, D.; Craxì, A.; Sulkowski, M.S.; Feld, J.J.; Manns, M.P. Extrahepatic Morbidity and Mortality of Chronic Hepatitis C. Gastroenterology 2015, 149, 1345–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pol, S.; Parlati, L.; Jadoul, M. Hepatitis C virus and the kidney. Nat. Rev. Nephrol. 2019, 15, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.-H.; Su, P.-Y.; Liu, I.-L.; Zeng, Y.-Y.; Huang, S.-P.; Hsu, Y.-C.; Yang, C.-W.; Chen, Y.-Y. Direct-acting antiviral treatment for Hepatitis C Virus in geriatric patients: A real-world retrospective comparison between early and late elderly patients. PeerJ 2021, 9, e10944. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.-H.; Su, P.-Y.; Zeng, Y.-H.; Liu, I.-L.; Huang, S.-P.; Hsu, Y.-C.; Chen, Y.-Y.; Yang, C.-W.; Wu, S.-S.; Chou, K.-C. Glecaprevir–pibrentasvir for chronic hepatitis C: Comparing treatment effect in patients with and without end-stage renal disease in a real-world setting. PLoS ONE 2020, 15, e0237582. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.U.; Mahmoud, M.I.; Butt, A.A. Hepatitis c virus and chronic kidney disease. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Hepatitis C Work Group. KDIGO 2018 Clinical Practice Guideline for the Prevention, Diagnosis, Evaluation, and Treatment of Hepatitis C in Chronic Kidney Disease. Kidney Int. Suppl. 2018, 2, S91–S165. [Google Scholar]
- Thomas, D.L. State of the Hepatitis C Virus Care Cascade. Clin. Liver Dis. 2020, 16, 8–11. [Google Scholar] [CrossRef]
- Haridy, J.; Iyngkaran, G.; Nicoll, A.; Hebbard, G.; Tse, E.; Fazio, T. eHealth Technologies for Screening, Diagnosis, and Management of Viral Hepatitis: A Systematic Review. Clin. Gastroenterol. Hepatol. 2021, 19, 1139–1150.e30. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, N.; Okumura, A.; Yamamoto, Y.; Yamaguchi, K.; Kaga, A.; Yamada, K.; Hirosaki, T.; Ishikawa, D.; Kunii, S.; Watanabe, K.; et al. Promoting notification and linkage of HBs antigen and anti-HCV antibody-positive patients through hospital alert system. BMC Infect. Dis. 2017, 17, 330. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.K.; Rich, N.E.; Ahn, C.; Turner, B.J.; Sanders, J.M.; Adamson, B.; Quirk, L.; Perryman, P.; Santini, N.O.; Singal, A.G. Evaluation of a Multifaceted Intervention to Reduce Health Disparities in Hepatitis C Screening: A Pre-Post Analysis. Hepatology 2019, 70, 40–50. [Google Scholar] [CrossRef]
- Hu, T.-H.; Su, W.-W.; Yang, C.-C.; Yang, C.-C.; Kuo, W.-H.; Chen, Y.-Y.; Yeh, Y.-H.; Chen, S.-S.; Tsao, Y.-Y.; Chen, K.-M.; et al. Elimination of Hepatitis C Virus in a Dialysis Population: A Collaborative Care Model in Taiwan. Am. J. Kidney Dis. 2021, 78, 511–519.e1. [Google Scholar] [CrossRef]
- Huang, C.-F.; Wu, P.-F.; Yeh, M.-L.; Huang, C.-I.; Liang, P.-C.; Hsu, C.-T.; Hsu, P.-Y.; Liu, H.-Y.; Huang, Y.-C.; Lin, Z.-Y.; et al. Scaling up the in-hospital hepatitis C virus care cascade in Taiwan. Clin. Mol. Hepatol. 2021, 27, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Xu, H.; Hu, Y.; Shang, J.; Jiang, J.; Yu, L.; Zhao, C.; Zhang, D.; Zhang, X.; Li, J.; et al. Hepatitis C screening in hospitals: Find the missing patients. Virol. J. 2019, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Morales-Arraez, D.; Hernandez-Guerra, M. Electronic Alerts as a Simple Method for Amplifying the Yield of Hepatitis C Virus Infection Screening and Diagnosis. Am. J. Gastroenterol. 2020, 115, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Riveiro-Barciela, M.; Gubern, P.; Roade, L.; Abrisqueta, P.; Carreras, M.J.; Farriols, A.; Bosch, F.; Esteban, R.; Buti, M. An electronic alert system increases screening for hepatitis B and C and improves management of patients with haematological disorders. Sci. Rep. 2020, 10, 3038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konerman, M.A.; Thomson, M.; Gray, K.; Moore, M.; Choxi, H.; Seif, E.; Lok, A.S. Impact of an electronic health record alert in primary care on increasing hepatitis c screening and curative treatment for baby boomers. Hepatology 2017, 66, 1805–1813. [Google Scholar] [CrossRef] [Green Version]
- Morales-Arraez, D.; Alonso-Larruga, A.; Diaz-Flores, F.; Dopico, J.A.G.; De Vera, A.; Quintero, E.; Hernandez-Guerra, M. Predictive factors for not undergoing RNA testing in patients found to have hepatitis C serology and impact of an automatic alert. J. Viral Hepat. 2019, 26, 1117–1123. [Google Scholar] [CrossRef]
- Chen, C.-H.; Yang, P.-M.; Huang, G.-T.; Lee, H.-S.; Sung, J.-L.; Sheu, J.-C. Estimation of Seroprevalence of Hepatitis B Virus and Hepatitis C Virus in Taiwan from a Large-scale Survey of Free Hepatitis Screening Participants. J. Formos. Med Assoc. 2007, 106, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Hsu, P.; Lee, J.; Niu, S.; Huang, J.; Hsu, C.; Jang, T.; Yeh, M.; Huang, C.; Liang, P.; et al. Evolutionary seroepidemiology of viral hepatitis and the gap in hepatitis C care cascades among uraemic patients receiving haemodialysis in Taiwan—The Formosa-Like Group. J. Viral Hepat. 2021, 28, 719–727. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, C.; Chen, J.; Hsu, N.; Wei, S.; Hou, S.; Lu, S.; Chen, P. Secular Trends and Geographic Maps of Hepatitis C Virus Infection among 4 Million Blood Donors in Taiwan from 1999 to 2017. Hepatol. Commun. 2020, 4, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Castrejón, M.; Chew, K.W.; Javanbakht, M.; Humphries, R.; Saab, S.; Klausner, J.D. Implementation of a Large System-Wide Hepatitis C Virus Screening and Linkage to Care Program for Baby Boomers. Open Forum Infect. Dis. 2017, 4, ofx109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLean, C.D.; Berger, C.; Cangiano, M.L.; Ziegelman, D.; Lidofsky, S.D. Impact of electronic reminder systems on hepatitis C screening in primary care. J. Viral Hepat. 2018, 25, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Sidlow, R.; Msaouel, P. Improving hepatitis C virus screening rates in primary care: A targeted intervention using the electronic health record. J. Healthc. Qual. 2015, 37, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Federman, A.D.; Kil, N.; Kannry, J.; Andreopolous, E.; Toribio, W.; Lyons, J.; Singer, M.; Yartel, A.; Smith, B.D.; Rein, D.B.; et al. An electronic health record-based intervention to promote hepatitis C virus testing among adults born between 1945 and 1965: A cluster-randomized trial. Med. Care 2017, 55, 590–597. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.H.-M.; Yang, W.-W.; Liu, C.-L.; Pwu, R.-F.; Chien, R.-N.; Lee, P.-C.; Chen, S.-C.; Chen, D.-S.; Lu, S.-N. The epidemiological profile of chronic hepatitis C with advanced hepatic fibrosis regarding virus genotype in Taiwan: A nationwide study. J. Formos. Med Assoc. 2021, 120, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.S.; Jung, E.S.; Kim, J.H.; Jung, Y.K.; Kim, J.H.; An, H.; Yim, H.J.; Yeon, J.E.; Byun, K.S.; Kim, C.D.; et al. Significance of Anti-HCV Signal-to-Cutoff Ratio in Predicting Hepatitis C Viremia. Korean J. Intern. Med. 2009, 24, 302–308. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021 towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Baseline | Screening | p Value a | |
|---|---|---|---|---|
| Age | 67.1 ± 14.1 | 67.1 ± 14.3 | 67.0 ± 13.7 | 0.744 |
| Sex (male) | 54.90% | 56.70% | 51.40% | <0.001 |
| Anti-HCV seropositive | 876/15,420 (5.7%) | 749/10,266 (7.3%) | 127/5154 (2.5%) | <0.001 |
| Detectable HCV RNA | 477/726 (65.7%) | 426/615 (69.1%) | 52/111 (46.8%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, P.-Y.; Su, W.-W.; Hsu, Y.-C.; Wang, S.-Y.; Chiu, P.-F.; Yen, H.-H. Micro-Elimination of Hepatitis C among Patients with Kidney Disease by Using Electronic Reminder System—A Hospital-Based Experience. J. Clin. Med. 2022, 11, 423. https://doi.org/10.3390/jcm11020423
Su P-Y, Su W-W, Hsu Y-C, Wang S-Y, Chiu P-F, Yen H-H. Micro-Elimination of Hepatitis C among Patients with Kidney Disease by Using Electronic Reminder System—A Hospital-Based Experience. Journal of Clinical Medicine. 2022; 11(2):423. https://doi.org/10.3390/jcm11020423
Chicago/Turabian StyleSu, Pei-Yuan, Wei-Wen Su, Yu-Chun Hsu, Shu-Yi Wang, Ping-Fang Chiu, and Hsu-Heng Yen. 2022. "Micro-Elimination of Hepatitis C among Patients with Kidney Disease by Using Electronic Reminder System—A Hospital-Based Experience" Journal of Clinical Medicine 11, no. 2: 423. https://doi.org/10.3390/jcm11020423
APA StyleSu, P. -Y., Su, W. -W., Hsu, Y. -C., Wang, S. -Y., Chiu, P. -F., & Yen, H. -H. (2022). Micro-Elimination of Hepatitis C among Patients with Kidney Disease by Using Electronic Reminder System—A Hospital-Based Experience. Journal of Clinical Medicine, 11(2), 423. https://doi.org/10.3390/jcm11020423