

Expert Clinical Management of Severe Immune-Related Adverse Events: Results from a Multicenter Survey on Hot Topics for Management

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Statistical Analysis
3. Results
3.1. Management of Severe IIH (Grade 3 or 4)
3.1.1. Participants
3.1.2. Diagnosis
3.1.3. Treatment
3.2. Management of Renal irAEs
3.2.1. Participants
3.2.2. Diagnosis
3.2.3. Treatment
3.3. Management of Immune-Related Myositis
3.3.1. Participants
3.3.2. Diagnosis
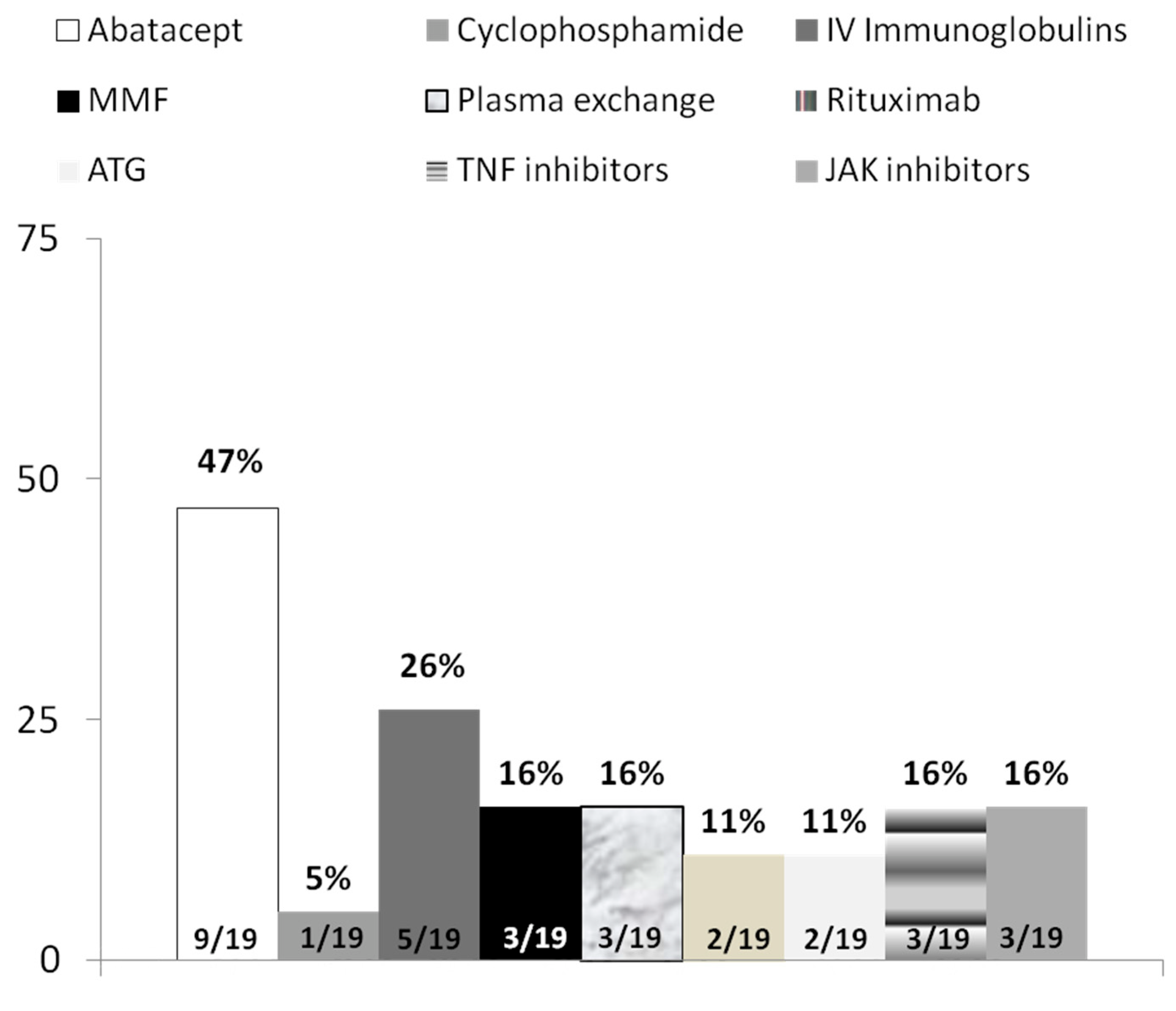
3.3.3. Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- 1.
- Immune-mediated hepatitis survey
- Country:
- Years at practice:
- University hospital: Yes/No
- Estimated number of attended patients with immune-related adverse events
- 0.
- <10
- 1.
- 10–20
- 2.
- 20–30
- 3.
- >40
- 1.
- When do you perform a liver biopsy for suspected immune-related hepatitis?
- All grade-3 and grade-4 immune-related hepatitis, prior to the beginning of corticoids
- All cases of immune-related hepatitis without improvement after therapy with corticoids (guidelines recommendation)
- All grade-3 and grade-4 immune-related hepatitis, regardless of prior corticoids therapy
- All grade-3 and grade-4 immune-related hepatitis, except those with severe hepatitis (Bilirubin > 2.5 mg/dL plus INR > 1.5)
- 2.
- Do you systematically rule out acute hepatitis E in all suspected cases of grade-3 and grade-4 immune-related hepatitis?
- 0.
- Yes, by means of anti-HEV IgM
- 1.
- Yes, by means of HEV-RNA
- 2.
- Yes, by means of both anti-HEV IgM and HEV RNA.
- 3.
- No.
- 3.
- Do you recommend an imaging test (liver US or CT scan) in all cases of grade-3 and grade-4 immune-related hepatitis?
- 0.
- Always.
- 1.
- Never.
- 2.
- Just in case of concomitant increase of AP and/or GGT
- 4.
- When do you start corticoids for immune-related hepatitis?
- All grade-3 and grade-4 immune-related hepatitis
- Only grade-3 and grade-4 immune-related hepatitis with severe inflammation at the liver biopsy
- All grade-3 and grade-4 immune-related hepatitis without improvement after temporary discontinuation of ICI.
- All cases of immune-related hepatitis without improvement after temporary discontinuation of ICI, regardless of the CTCAE grade of hepatitis.
- 5.
- Which immunosuppressant do you prefer for steroid-refractory immune-related hepatitis:
- 0.
- Azathioprine
- 1.
- MMF
- 2.
- Tacrolimus
- 3.
- Cyclosporin
- 4.
- Other:
- 6.
- Which therapy do you use for patients with severe immune-related hepatitis (Bilirubin > 2.5 mg/dL plus INR > 1.5):
- 0.
- Corticoids + MMF + Tocilizumab
- 1.
- Corticoids + MMF + Plasma exchange
- 2.
- Corticoids + MMF + Antithymocyte globulin
- 3.
- Corticoids + MMF + Infliximab
- 4.
- Others:
- 2.
- Immune-mediated renal events survey
- Affiliation:
- Country:
- Years at practice:
- University hospital:
- Onconephrology unit or outpatient consult:
- Estimated number of attended patients with immune-related adverse events x Year:
- <10
- 10–20
- 20–30
- >40
- 1.
- When do you perform a kidney biopsy for suspected immune-related AKI?
- All cases of ICI-treated patients who develop AKI unless there is a clear alternative etiology for the disease (dehydration, obstruction…) without improvement after therapy with corticoids
- ICI-treated patients who develop KDIGO stage 2 or 3 AKI unless there is a clear alternative etiology for the AKI, prior to the beginning of corticoids
- ICI-treated patients who develop KDIGO stage 2 or 3 AKI unless there is a clear alternative etiology for the AKI regardless of prior corticoids therapy
- ICI-treated patients who develop KDIGO stage 3 AKI unless there is a clear alternative etiology for the AKI
- 2.
- Do you systematically rule out eosinophiluria (urine eosinophils) in all suspected cases of AKI related ICI?
- Yes, always.
- Yes, sometimes.
- No.
- 3.
- Do you systematically recommend a renal US or CT scan in all cases of ICI-treated patients who develop AKI?
- Always.
- Never.
- Just in case of stage 2 or 3 AKI.
- 4.
- When do you use corticoids for immune-related AKI?
- ICI related AKI with SCreatinine 2–3× baseline (as recommended by ASCO and NCCN clinical practice guidelines)
- Only KDIGO stage 3 AKI related to ICI with severe inflammation at the kidney biopsy (ATIN)
- KDIGO stage 2 and 3 AKI related to ICI without improvement after temporary discontinuation of ICI.
- All cases of AKI related to ICI with ATIN diagnosis in kidney biopsy.
- 5.
- In case you started steroids how long do you use them?
- Steroids tapering over 2 weeks
- Steroids tapering over 4–6 weeks
- Steroids tapering over 3 weeks
- Steroids tapering over 12 weeks
- Steroids tapering over 24 weeks
- 6.
- Which immunosuppressive therapy do you prefer for steroid-refractory immune-related AKI.
- Azathioprine
- MMF
- Tacrolimus
- Cyclosporin
- Other
- 7.
- When do you recommend ICI rechallenge in immune-related AKI patients with cancer disease progression?
- Never
- Rechallenge in patients with CTCAE grade 1 toxicity.
- Rechallenge in patients with KDIGO stage 1 or 2 AKI with biopsy-proven ICI.
- Rechallenge after kidney function has completely recovered.
- 3.
- Immune-mediated myositis survey
- ☐
- <10
- ☐
- 10–20
- ☐
- 20–30
- ☐
- 30–40
- ☐
- >40
- Would you recommend a muscle biopsy (for clinical purposes, not research)?Yes ____ No____
- What would be your initial recommendation for treatment with glucocorticoids?Route of administration: oral_______ IV_________Dose and glucocorticoid agent:__________
- Would you add any other treatments at this time? Please specify.
- 4.
- What would be your recommendation for management at this time?________________
- Would you recommend a muscle biopsy (for clinical purposes, not research)?Yes ____ No____
- Would you recommend an endomyocardial muscle biopsy (for clinical purposes, not research)?Yes ____ No____
- What would be your initial recommendation for treatment with glucocorticoids?Route of administration: oral_______ IV_________Dose and glucocorticoid agent:__________
- Would you add any other treatments at this time? Please specify.__________________________
- 5.
- What would be your recommendation for management at this time?________________
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Johnson, D.B.; Reynolds, K.L.; Sullivan, R.J.; Balko, J.M.; Patrinely, J.R.; Cappelli, L.C.; Naidoo, J.; Moslehi, J.J. Immune checkpoint inhibitor toxicities: Systems-based approaches to improve patient care and research. Lancet Oncol. 2020, 21, e398–e404. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, iv119–iv142. [Google Scholar] [CrossRef]
- Schneider, B.J.; Naidoo, J.; Santomasso, B.D.; Lacchetti, C.; Adkins, S.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 4073–4126. [Google Scholar] [CrossRef]
- Xu, C.; Chen, Y.P.; Du, X.J.; Liu, J.Q.; Huang, C.L.; Chen, L.; Zhou, G.Q.; Li, W.F.; Mao, Y.P.; Hsu, C.; et al. Comparative safety of immune checkpoint inhibitors in cancer: Systematic review and network meta-analysis. BMJ 2018, 363, k4226. [Google Scholar] [CrossRef]
- Cappelli, L.C.; Gutierrez, A.K.; Bingham, C.O., 3rd; Shah, A.A. Rheumatic and Musculoskeletal Immune-Related Adverse Events Due to Immune Checkpoint Inhibitors: A Systematic Review of the Literature. Arthritis Care Res. 2017, 69, 1751–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendon, J.; Cordoba, J.; Dhawan, A.; Larsen, F.S.; Manns, M.; Samuel, D.; Simpson, K.J.; Yaron, I.; Bernardi, M. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 2017, 66, 1047–1081. [Google Scholar] [CrossRef]
- Thompson, J.A.; Schneider, B.J.; Brahmer, J.; Andrews, S.; Armand, P.; Bhatia, S.; Budde, L.E.; Costa, L.; Davies, M.; Dunnington, D.; et al. NCCN Guidelines Insights: Management of Immunotherapy-Related Toxicities, Version 1.2020. J. Natl. Compr. Cancer Netw. 2020, 18, 230–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OMERECT: Outcome Measures in Rheumatology Immune-Related Adverse Events Special Interest Group. Available online: https:\\omeract.org (accessed on 31 May 2022).
- Tsung, I.; Dolan, R.; Lao, C.D.; Fecher, L.; Riggenbach, K.; Yeboah-Korang, A.; Fontana, R.J. Liver injury is most commonly due to hepatic metastases rather than drug hepatotoxicity during pembrolizumab immunotherapy. Aliment. Pharmacol. Ther. 2019, 50, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.; Iafolla, M.; Kanjanapan, Y.; Cerocchi, O.; Butler, M.; Siu, L.L.; Bedard, P.L.; Ross, K.; Hansen, B.; Spreafico, A.; et al. Evaluation of liver enzyme elevations and hepatotoxicity in patients treated with checkpoint inhibitor immunotherapy. PLoS ONE 2021, 16, e0253070. [Google Scholar] [CrossRef]
- De Martin, E.; Michot, J.M.; Papouin, B.; Champiat, S.; Mateus, C.; Lambotte, O.; Roche, B.; Antonini, T.M.; Coilly, A.; Laghouati, S.; et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef]
- Al-Nattah, S.; Lata Sharma, K.; Caldis, M.; Spengler, E.; Nicholas Rose, W. Plasmapheresis for Pembrolizumab-Induced Hepatitis in a Patient with Squamous Cell Carcinoma and Prior Orthotopic Liver Transplantation. Case Rep. Hepatol. 2022, 2022, 5908411. [Google Scholar] [CrossRef]
- Riveiro-Barciela, M.; Muñoz-Couselo, E.; Fernandez-Sojo, J.; Diaz-Mejia, N.; Parra-López, R.; Buti, M. Acute liver failure due to immune-mediated hepatitis successfully managed with plasma exchange: New settings call for new treatment strategies? J. Hepatol. 2019, 70, 564–566. [Google Scholar] [CrossRef] [Green Version]
- Mir, H.; Alhussein, M.; Alrashidi, S.; Alzayer, H.; Alshatti, A.; Valettas, N.; Mukherjee, S.D.; Nair, V.; Leong, D.P. Cardiac Complications Associated With Checkpoint Inhibition: A Systematic Review of the Literature in an Important Emerging Area. Can. J. Cardiol. 2018, 34, 1059–1068. [Google Scholar] [CrossRef]
- Safa, H.; Johnson, D.H.; Trinh, V.A.; Rodgers, T.E.; Lin, H.; Suarez-Almazor, M.E.; Fa’ak, F.; Saberian, C.; Yee, C.; Davies, M.A.; et al. Immune checkpoint inhibitor related myasthenia gravis: Single center experience and systematic review of the literature. J. Immunother. Cancer 2019, 7, 319. [Google Scholar] [CrossRef]
- Moi, L.; Bouchaab, H.; Mederos, N.; Nguyen-Ngoc, T.; Perreau, M.; Fenwick, C.; Vaucher, J.; Sempoux, C.; Peters, S.; Obeid, M. Personalized Cytokine-Directed Therapy With Tocilizumab for Refractory Immune Checkpoint Inhibitor-Related Cholangiohepatitis. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2021, 16, 318–326. [Google Scholar] [CrossRef]
- Stroud, C.R.; Hegde, A.; Cherry, C.; Naqash, A.R.; Sharma, N.; Addepalli, S.; Cherukuri, S.; Parent, T.; Hardin, J.; Walker, P. Tocilizumab for the management of immune mediated adverse events secondary to PD-1 blockade. J. Oncol. Pharm. Pract. Off. Publ. Int. Soc. Oncol. Pharm. Pract. 2019, 25, 551–557. [Google Scholar] [CrossRef]
- Kim, S.T.; Tayar, J.; Trinh, V.A.; Suarez-Almazor, M.; Garcia, S.; Hwu, P.; Johnson, D.H.; Uemura, M.; Diab, A. Successful treatment of arthritis induced by checkpoint inhibitors with tocilizumab: A case series. Ann. Rheum. Dis. 2017, 76, 2061–2064. [Google Scholar] [CrossRef]
- Muriithi, A.K.; Nasr, S.H.; Leung, N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1857–1862. [Google Scholar] [CrossRef]
- Lee, M.D.; Seethapathy, H.; Strohbehn, I.A.; Zhao, S.H.; Boland, G.M.; Fadden, R.; Sullivan, R.; Reynolds, K.L.; Sise, M.E. Rapid corticosteroid taper versus standard of care for immune checkpoint inhibitor induced nephritis: A single-center retrospective cohort study. J. Immunother. Cancer 2021, 9, e002292. [Google Scholar] [CrossRef]
- García-Carro, C.; Bolufer, M.; Bury, R.; Catañeda, Z.; Muñoz, E.; Felip, E.; Lorente, D.; Carreras, M.J.; Gabaldon, A.; Agraz, I.; et al. Acute kidney injury as a risk factor for mortality in oncological patients receiving check-point inhibitors. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 37, 887–894. [Google Scholar] [CrossRef]
- Gupta, S.; Short, S.A.P.; Sise, M.E.; Prosek, J.M.; Madhavan, S.M.; Soler, M.J.; Ostermann, M.; Herrmann, S.M.; Abudayyeh, A.; Anand, S.; et al. Acute kidney injury in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e003467. [Google Scholar] [CrossRef]
- Abdel-Wahab, N.; Suarez-Almazor, M.E. Frequency and distribution of various rheumatic disorders associated with checkpoint inhibitor therapy. Rheumatology 2019, 58, vii40–vii48. [Google Scholar] [CrossRef] [Green Version]
- Aldrich, J.; Pundole, X.; Tummala, S.; Palaskas, N.; Andersen, C.R.; Shoukier, M.; Abdel-Wahab, N.; Deswal, A.; Suarez-Almazor, M.E. Inflammatory Myositis in Cancer Patients Receiving Immune Checkpoint Inhibitors. Arthritis Rheumatol. 2021, 73, 866–874. [Google Scholar] [CrossRef]
- Lehmann, L.H.; Cautela, J.; Palaskas, N.; Baik, A.H.; Meijers, W.C.; Allenbach, Y.; Alexandre, J.; Rassaf, T.; Müller, O.J.; Aras, M.; et al. Clinical Strategy for the Diagnosis and Treatment of Immune Checkpoint Inhibitor-Associated Myocarditis: A Narrative Review. JAMA Cardiol. 2021, 6, 1329–1337. [Google Scholar] [CrossRef]
- Kostine, M.; Finckh, A.; Bingham, C.O.; Visser, K.; Leipe, J.; Schulze-Koops, H.; Choy, E.H.; Benesova, K.; Radstake, T.; Cope, A.P.; et al. EULAR points to consider for the diagnosis and management of rheumatic immune-related adverse events due to cancer immunotherapy with checkpoint inhibitors. Ann. Rheum. Dis. 2021, 80, 36–48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) | |||
|---|---|---|---|
| Characteristic | IIH | Renal irAEs | Myositis |
| (n = 17) | (n = 20) | (n= 19) | |
| Country | |||
| Australia | 0 | 0 | 1 (5) |
| Belgium | 0 | 1 (5) | 0 |
| Canada | 1 (6) | 0 | 2 (11) |
| France | 2 (12) | 1 (5) | 1 (5) |
| Germany | 0 | 0 | 2 (11) |
| Italy | 2 (12) | 1 (5) | 0 |
| Netherlands | 0 | 1 (5) | 1 (5) |
| Poland | 0 | 1 (5) | 0 |
| Japan | 1 (6) | 0 | 0 |
| Spain | 10 (59) | 2 (10) | 0 |
| United Kingdom | 0 | 0 | 1 (5) |
| United States | 1 (6) | 11 (55) | 11 (58) |
| Taiwan | 0 | 1 (5) | 0 |
| Turkey | 0 | 1 (5) | 0 |
| Years in practice | |||
| <5 | 0 | 1 (5) | 5 (26) |
| 10-May | 6 (35) | 6 (30) | 3 (16) |
| 20-October | 4 (24) | 10 (50) | 7 (37) |
| 20–30 | 3 (18) | 1 (5) | 2 (11) |
| >30 | 4 (24) | 2 (10) | 2 (11) |
| Estimated number of new patients with irAEs seen per year * | |||
| <10 | |||
| 19-Oct | |||
| 20–29 | 3 (18) | 2 (10) | 1 (5) * |
| 30–40 | 5 (29) | 4 (20) | 1 (5) |
| >40 | 3 (18) | 3 (15) | 4 (21) |
| 5 (29) | 0 | 5 (26) | |
| 1 (6) | 11 (55) | 7 (37) | |
| University hospital affiliation | 17 (100) | 19 (95) | 19 (100) |
| Recommendation | ||
|---|---|---|
| Biopsy | ASCO [5] | ESMO [4] |
| Liver | Consider in steroid-refractory cases to rule out other entities | Consider in steroid- and mycophenolate-refractory cases |
| Kidney | Kidney biopsy should be discouraged until steroid-based treatment has been attempted | Grade 2: creatinine level >1.5–3.0 times baseline or >1.5–3.0 times ULN; discuss with nephrologist; early consideration of renal biopsy is helpful, which may negate the need for steroids and determine whether renal deterioration is related to ICIs or other pathology |
| Muscle | Myositis: Consider muscle biopsy on an individual basis when diagnosis is uncertain and overlap with neurologic syndromes such as myasthenia gravis is suspected. Myocarditis: Endomyocardial biopsy should be considered for patients who are unstable, failed initial therapy, or in whom the diagnosis is in doubt | Not specifically discussed; general guidance is to consider tissue biopsy in cases with diagnostic doubt about the etiology of the complication and in whom management would be altered by the outcome of the biopsy procedure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riveiro-Barciela, M.; Soler, M.J.; Barreira-Diaz, A.; Bermejo, S.; Bruera, S.; Suarez-Almazor, M.E. Expert Clinical Management of Severe Immune-Related Adverse Events: Results from a Multicenter Survey on Hot Topics for Management. J. Clin. Med. 2022, 11, 5977. https://doi.org/10.3390/jcm11205977
Riveiro-Barciela M, Soler MJ, Barreira-Diaz A, Bermejo S, Bruera S, Suarez-Almazor ME. Expert Clinical Management of Severe Immune-Related Adverse Events: Results from a Multicenter Survey on Hot Topics for Management. Journal of Clinical Medicine. 2022; 11(20):5977. https://doi.org/10.3390/jcm11205977
Chicago/Turabian StyleRiveiro-Barciela, Mar, Maria Jose Soler, Ana Barreira-Diaz, Sheila Bermejo, Sebastian Bruera, and Maria E. Suarez-Almazor. 2022. "Expert Clinical Management of Severe Immune-Related Adverse Events: Results from a Multicenter Survey on Hot Topics for Management" Journal of Clinical Medicine 11, no. 20: 5977. https://doi.org/10.3390/jcm11205977
APA StyleRiveiro-Barciela, M., Soler, M. J., Barreira-Diaz, A., Bermejo, S., Bruera, S., & Suarez-Almazor, M. E. (2022). Expert Clinical Management of Severe Immune-Related Adverse Events: Results from a Multicenter Survey on Hot Topics for Management. Journal of Clinical Medicine, 11(20), 5977. https://doi.org/10.3390/jcm11205977