
Patients with Bicuspid Aortopathy and Aortic Dilatation
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
3. Genetics and Molecular Biology
4. Classification and Nomenclature
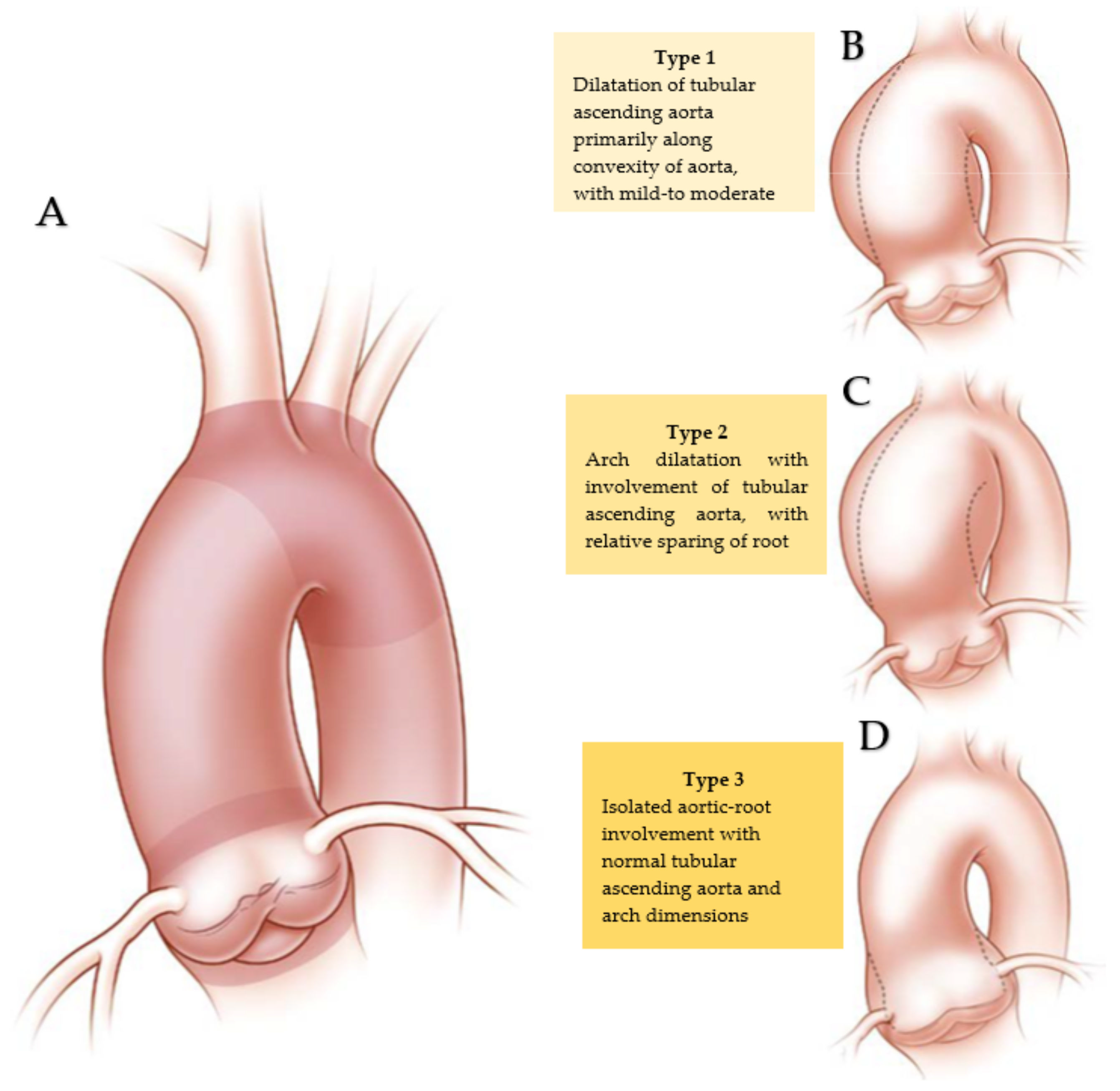
5. BAV Geometry Types and Surgical Implications
6. Pathophysiology
7. Imaging Diagnostic
7.1. Echocardiographic Imaging
7.2. Cardiac Computed Tomography
7.3. Magnetic Resonance
8. Assessment and Treatment
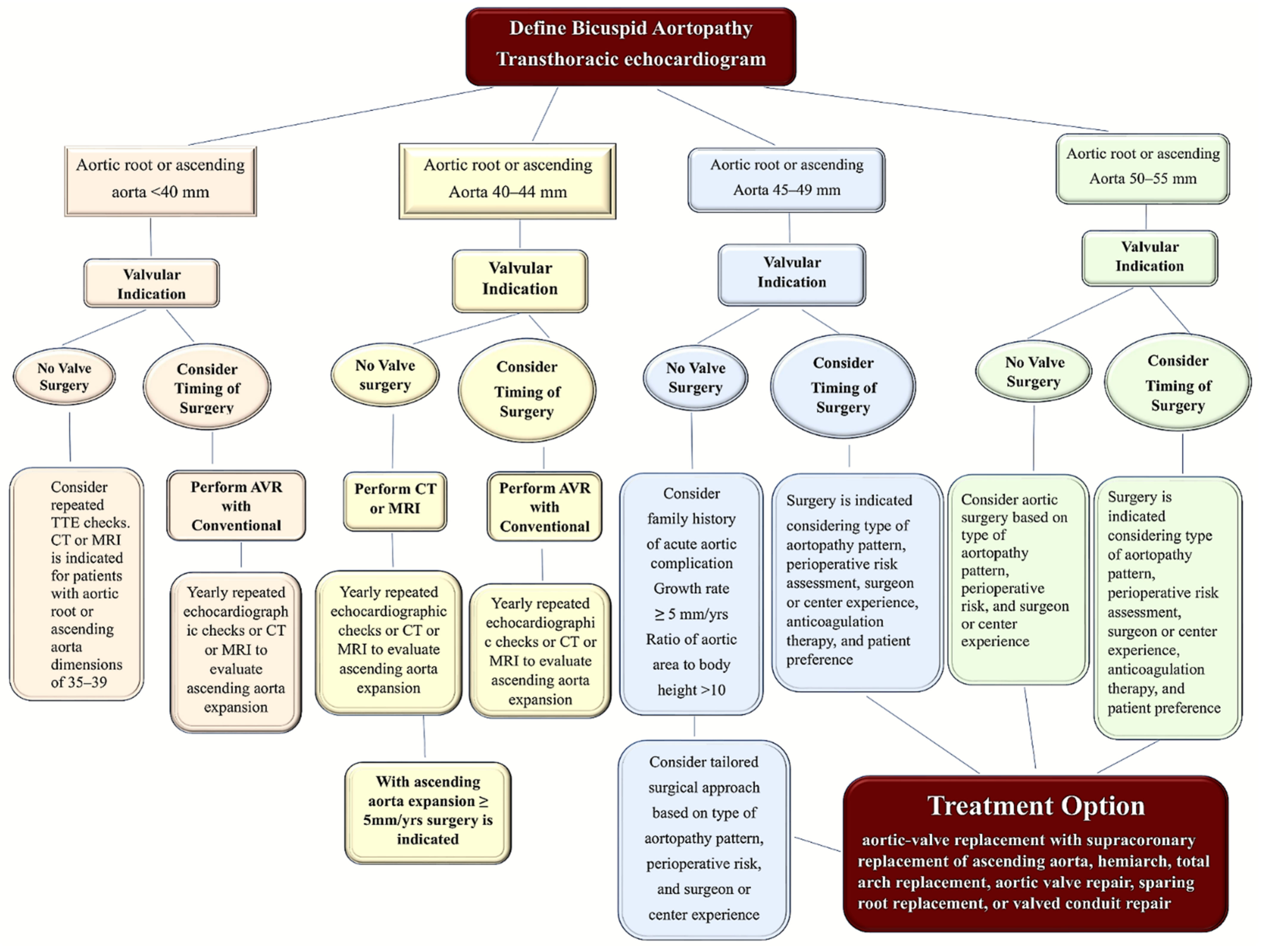
8.1. Decision-Making Algorithm for Treatment Option
8.2. Special Populations
8.3. Surgery in Special Population
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATA | Ascending thoracic aorta |
| ACTA | Alfa actine |
| AS | Aortic stenosis |
| AR | Aortic regurgitation |
| AV | Aortic valve |
| AVK | Anti-vitamin K |
| AVR | Aortic valve replacement |
| AXIN | gene encodes a cytoplasmic protein, which contains a regulation of G-protein signaling (RGS) domain and a disheveled and axin (DIX) domain |
| BAV | Bicuspid aortic valve |
| CABG | Coronary artery bypass grafting |
| CCT | Cardiac computed tomography |
| CineMR | Cine magnetic resonance |
| CMR 4D-flow | Time-resolved three-dimensional phase-contrast cardiovascular magnetic resonance |
| COR | Class of recommendation |
| CT | Computed tomography |
| DA | Descending aorta |
| E | Young’s elastic module |
| EMT | Epithelial–mesenchymal transition |
| EndMT | Endothelial–mesenchymal transition |
| ENG | Endoglin |
| eNOS | Endothelium-derived nitric oxide synthetase |
| Erb | Tyrosine kinase receptor |
| FBN 1 | Fibrillin 1 |
| FJA | flow jet angle |
| GATA | sequence for transcription factors for zinc proteins’ binding DNA sequence |
| IPRF | In-plane rotational flow |
| LOE | Level of evidence |
| LVOT | Left ventricular outflow tract |
| MAPK | Mitogen-activated protein kinase |
| miRNA | Micro-RNA |
| MMP | Metalloproteinases |
| MR | Magnetic resonance |
| MRI | Magnetic resonance Imaging |
| NFD | normalized flow displacement |
| NOTCH1 | gene encoding transmembrane proteins |
| NOS3 | nitric oxide synthase 3 |
| PA | pulmonary autograft |
| PDIA2 | Protein disulfide isomerase family A member 2 |
| PECAM | Platelet endothelial cell adhesion molecule |
| PWV | Pulse wave velocity |
| SFRR | systolic flow reversal ratio |
| SMAD 2 | similar mothers against decapentaplegic Drosophila gene 2 |
| SNP | single nucleotide polymorphism |
| STJ | Sinotubular junction |
| TA | Thoracic aorta |
| TAVR | Transcatheter aortic valve replacement |
| TEE | transesophageal echocardiography |
| TGF | Transforming growth factor |
| TIMP | Tissue inhibitor of matrix metalloproteinases |
| TTE | Transthoracic Echocardiography |
| VSMCs | Vascular smooth muscle cells |
| VBR | Virtual Basal Ring |
| WSS | Wall Shear Stress |
| Γ | circulation |
| ω | vorticity |
References
- Ward, C. Clinical significance of the bicuspid aortic valve. Heart 2000, 83, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Tzemos, N.; Therrien, J.; Yip, J.; Thanassoulis, G.; Tremblay, S.; Jamorski, M.T.; Webb, G.D.; Siu, S.C. Outcomes in adults with bicuspid aortic valves. JAMA 2008, 300, 1317–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tutar, E.; Ekici, F.; Atalay, S.; Nacar, N. The prevalence of bicuspid aortic valve in newborns by echocardiographic screening. Am. Heart J. 2005, 150, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Carro, A.; Teixido-Tura, G.; Evangelista, A. Aortic Dilatation in Bicuspid Aortic Valve Disease. Rev. Esp. Cardiol. 2012, 65, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Fedak, P.; Verma, S.; David, T.E.; Leask, R.; Weisel, R.D.; Butany, J. Clinical and Pathophysiological Implications of a Bicuspid Aortic Valve. Circulation 2002, 106, 900–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girdauskas, E.; Borger, M.; Secknus, M.-A.; Girdauskas, G.; Kuntze, T. Is aortopathy in bicuspid aortic valve disease a congenital defect or a result of abnormal hemodynamics? A critical reappraisal of a one-sided argument. Eur. J. Cardio-Thorac. Surg. 2011, 39, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Siu, S.C.; Silversides, C.K. Bicuspid aortic valve disease. J. Am. Coll. Cardiol. 2010, 55, 2789–2800. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Kang, L.; Ma, Z.; Lu, S.; Huang, B.; Wang, C.; Zou, Y.; Sun, Y. MicroRNAs involve in bicuspid aortic aneurysm: Pathogenesis and biomarkers. J. Cardiothorac. Surg. 2021, 16, 230. [Google Scholar] [CrossRef]
- Nappi, F.; Iervolino, A.; Singh, S.S.A.; Chello, M. MicroRNAs in Valvular Heart Diseases: Biological Regulators, Prognostic Markers and Therapeutical Targets. Int. J. Mol. Sci. 2021, 22, 12132. [Google Scholar] [CrossRef]
- Garg, V.; Muth, A.N.; Ransom, J.F.; Schluterman, M.K.; Barnes, R.; King, I.N.; Grossfeld, P.D.; Srivastava, D. Mutations in NOTCH1 cause aortic valve disease. Nature 2005, 437, 270–274. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Aherrahrou, Z.; Liptau, H.; Erasmi, A.W.; Hagemann, C.; Wrobel, S.; Borzym, K.; Schunkert, H.; Sievers, H.H.; Erdmann, J. Novel missense mutations (p. T596M and p. P1797H) in NOTCH1 in patients with bicuspid aortic valve. Biochem. Biophys. Res. Commun. 2006, 345, 1460–1465. [Google Scholar] [CrossRef]
- Martin, L.; Ramachandran, V.; Cripe, L.H.; Hinton, R.B.; Andelfinger, G.; Tabangin, M.; Shooner, K.; Keddache, M.; Benson, D.W. Evidence in favor of linkage to human chromosomal regions 18q, 5q and 13q for bicuspid aortic valve and associated cardiovascular malformations. Hum. Genet. 2007, 121, 275–284. [Google Scholar] [CrossRef]
- Guo, D.-C.; Pannu, H.; Tran-Fadulu, V.; Papke, C.L.; Yu, R.K.; Avidan, N.; Bourgeois, S.; Estrera, A.L.; Safi, H.J.; Sparks, E.; et al. Mutations in smooth muscle α-actin (ACTA2) lead to thoracic aortic aneurysms and dissections. Nat. Genet. 2007, 39, 1488–1493. [Google Scholar] [CrossRef]
- Higgins, C.B.; Wexler, L. Reversal of dominance of the coronary arterial system in isolated aortic stenosis and bicuspid aortic valve. Circulation 1975, 52, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Hutchins, G.M.; Nazarian, I.H.; Bulkley, B.H. Association of left dominant coronary arterial system with congenital bicuspid aortic valve. Am. J. Cardiol. 1978, 42, 57–59. [Google Scholar] [CrossRef]
- Rashid, A.; Saucedo, J.F.; Hennebry, T.A. Association of Single Coronary Artery and Congenital Bicuspid Aortic Valve with Review of Literature. J. Interv. Cardiol. 2005, 18, 389–391. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Target Recognition and Regulatory Functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Insull, W., Jr. The Pathology of Atherosclerosis: Plaque Development and Plaque Responses to Medical Treatment. Am. J. Med. 2009, 122, S3–S14. [Google Scholar] [CrossRef]
- LeMaire, S.A.; Wang, X.; Wilks, J.A.; Carter, S.A.; Wen, S.; Won, T.; Leonardelli, D.; Anand, G.; Conklin, L.D.; Wang, X.L.; et al. Matrix metalloproteinases in ascending aortic aneurysms: Bicuspid versus trileaflet aortic valves1. J. Surg. Res. 2005, 123, 40–48. [Google Scholar] [CrossRef]
- Wu, J.; Song, H.-F.; Li, S.-H.; Guo, J.; Tsang, K.; Tumiati, L.; Butany, J.; Yau, T.M.; Ouzounian, M.; Fu, S.; et al. Progressive Aortic Dilation Is Regulated by miR-17–Associated miRNAs. J. Am. Coll. Cardiol. 2016, 67, 2965–2977. [Google Scholar] [CrossRef]
- Naito, S.; Petersen, J.; Sequeira-Gross, T.; Neumann, N.; Escobar, J.D.; Zeller, T.; Reichenspurner, H.; Girdauskas, E. Bicuspid aortopathy—Molecular involvement of microRNAs and MMP-TIMP. Biomarkers 2020, 25, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, D.; Zhu, S.; Wang, F.; Sun, X.; Yang, S.; Wang, C. Plasma Exosomal Mir-423-5p Is Involved in the Occurrence and Development of Bicuspid Aortopathy via TGF-beta/SMAD2 Pathway. Front. Physiol. 2021, 12, 759035. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Zhu, P.; Gu, J.; Ni, B.; Sun, H.; He, K.; Bian, J.; Shao, Y.; Du, J. Transcription factor Sp2 promotes TGFB-mediated interstitial cell osteogenic differentiation in bicuspid aortic valves through a SMAD-dependent pathway. Exp. Cell Res. 2022, 411, 112972. [Google Scholar] [CrossRef] [PubMed]
- Naito, S.; Sequeira-Gross, T.; Petersen, J.; Detlef, I.; Sachse, M.; Zeller, T.; Reichenspurner, H.; Girdauskas, E. Circulating microRNAs in the prediction of BAV aortopathy: Do the expression patterns correlate between blood and aortic tissue? Rev. Cardiovasc. Med. 2022, 23, 47. [Google Scholar] [CrossRef]
- Albinsson, S.; Della Corte, A.; Alajbegovic, A.; Krawczyk, K.K.; Bancone, C.; Galderisi, U.; Cipollaro, M.; De Feo, M.; Forte, A. Patients with bicuspid and tricuspid aortic valve exhibit distinct regional microrna signatures in mildly dilated ascending aorta. Heart Vessel. 2017, 32, 750–767. [Google Scholar] [CrossRef]
- Borghini, A.; Foffa, I.; Pulignani, S.; Vecoli, C.; Ait-Ali, L.; Andreassi, M.G. miRNome Profiling in Bicuspid Aortic Valve-Associated Aortopathy by Next-Generation Sequencing. Int. J. Mol. Sci. 2017, 18, 2498. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Micaelo, N.; Beltrán-Debón, R.; Aragonès, G.; Faiges, M.; Alegret, J.M. MicroRNAs Clustered within the 14q32 Locus Are Associated with Endothelial Damage and Microparticle Secretion in Bicuspid Aortic Valve Disease. Front. Physiol. 2017, 8, 648. [Google Scholar] [CrossRef] [Green Version]
- Maleki, S.; Cottrill, K.A.; Poujade, F.-A.; Bhattachariya, A.; Bergman, O.; Gådin, J.R.; Simon, N.; Lundströmer, K.; Franco-Cereceda, A.; Björck, H.M.; et al. The mir-200 family regulates key pathogenic events in ascending aortas of individuals with bicuspid aortic valves. J. Intern. Med. 2019, 285, 102–114. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Micaelo, N.; Beltrán-Debón, R.; Baiges, I.; Faiges, M.; Alegret, J.M. Specific circulating microRNA signature of bicuspid aortic valve disease. J. Transl. Med. 2017, 15, 76. [Google Scholar] [CrossRef] [Green Version]
- Gallo, A.; Agnese, V.; Coronnello, C.; Raffa, G.M.; Bellavia, D.; Conaldi, P.G.; Pilato, M.; Pasta, S. On the prospect of serum exosomal miRNA profiling and protein biomarkers for the diagnosis of ascending aortic dilatation in patients with bicuspid and tricuspid aortic valve. Int. J. Cardiol. 2018, 273, 230–236. [Google Scholar] [CrossRef]
- Giusti, B.; Sticchi, E.; De Cario, R.; Magi, A.; Nistri, S.; Pepe, G. Genetic Bases of Bicuspid Aortic Valve: The Contribution of Traditional and High-Throughput Sequencing Approaches on Research and Diagnosis. Front. Physiol. 2017, 8, 612. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Montes, C.; Martín, M.; Martínez-Arias, L.; Coto, E.; Naves-Díaz, M.; Morís, C.; Cannata-Andía, J.B.; Rodríguez, I. Variants in cardiac GATA genes associated with bicuspid aortic valve. Eur. J. Clin. Investig. 2018, 48, e13027. [Google Scholar] [CrossRef]
- Hill, J.C.; Billaud, M.; Richards, T.D.; Kotlarczyk, M.P.; Shiva, S.; Phillippi, J.A.; Gleason, T.G. Layer-specific Nos3 expression and genotypic distribution in bicuspid aortic valve aortopathy. Eur. J. Cardio-Thorac. Surg. 2022, ezac237. [Google Scholar] [CrossRef]
- Wooten, E.C.; Iyer, L.K.; Montefusco, M.C.; Hedgepeth, A.K.; Payne, D.D.; Kapur, N.K.; Housman, D.E.; Mendelsohn, M.E.; Huggins, G.S. Application of gene network analysis techniques identifies AXIN1/PDIA2 and endoglin haplotypes associated with bicuspid aortic valve. PLoS ONE 2010, 5, e8830. [Google Scholar] [CrossRef]
- Fulmer, D.; Toomer, K.; Guo, L.; Moore, K.; Glover, J.; Moore, R.; Stairley, R.; Lobo, G.; Zuo, X.; Dang, Y.; et al. Defects in the Exocyst-Cilia Machinery Cause Bicuspid Aortic Valve Disease and Aortic Stenosis. Circulation 2019, 140, 1331–1341. [Google Scholar] [CrossRef]
- Roberts, W.C. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am. J. Cardiol. 1970, 26, 72–83. [Google Scholar] [CrossRef]
- Michelena, H.I.; Della Corte, A.; Evangelista, A.; Maleszewski, J.J.; Edwards, W.D.; Roman, M.J.; Devereux, R.B.; Fernández, B.; Asch, F.M.; Barker, A.J.; et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. Eur. J. Cardiothorac. Surg. 2021, 60, 448–476. [Google Scholar] [CrossRef]
- Brandenburg, R.O.; Tajik, A.J.; Edwards, W.D.; Reeder, G.S.; Shub, C.; Seward, J.B. Accuracy of 2-dimensional echocardiographic diagnosis of congenitally bicuspid aortic valve: Echocardiographic-anatomic correlation in 115 patients. Am. J. Cardiol. 1983, 51, 1469–1473. [Google Scholar] [CrossRef]
- Angelini, A.; Ho, S.Y.; Anderson, R.H.; Devine, W.A.; Zuberbuhler, J.R.; Becker, A.E.; Davies, M.J. The morphology of the normal aortic valve as compared with the aortic valve having two leaflets. J. Thorac. Cardiovasc. Surg. 1989, 98, 362–367. [Google Scholar] [CrossRef]
- Sabet, H.Y.; Edwards, W.D.; Tazelaar, H.D.; Daly, R.C. Congenitally Bicuspid Aortic Valves: A Surgical Pathology Study of 542 Cases (1991 Through 1996) and a Literature Review of 2,715 Additional Cases. Mayo Clin. Proc. 1999, 74, 14–26. [Google Scholar] [CrossRef]
- Sievers, H.-H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, B.M.; Lewin, M.B.; Stout, K.K.; Gill, E.; Prueitt, A.; Byers, P.H.; Otto, C.M. The bicuspid aortic valve: An integrated phenotypic classification of leaflet morphology and aortic root shape. Heart 2008, 94, 1634–1638. [Google Scholar] [CrossRef]
- Kang, J.-W.; Song, H.G.; Yang, D.H.; Baek, S.; Kim, D.-H.; Song, J.-M.; Kang, D.-H.; Lim, T.-H.; Song, J.-K. Association Between Bicuspid Aortic Valve Phenotype and Patterns of Valvular Dysfunction and Bicuspid Aortopathy: Comprehensive Evaluation Using MDCT and Echocardiography. JACC Cardiovasc. Imaging 2013, 6, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Michelena, H.I.; Prakash, S.K.; Della Corte, A.; Bissell, M.M.; Anavekar, N.; Mathieu, P.; Bossé, Y.; Limongelli, G.; Bossone, E.; Benson, D.W.; et al. Bicuspid aortic valve: Identifying knowledge gaps and rising to the challenge from the International Bicuspid Aortic Valve Consortium (BAVCon). Circulation 2014, 129, 2691–2704. [Google Scholar] [CrossRef] [Green Version]
- Jilaihawi, H.; Chen, M.; Webb, J.; Himbert, D.; Ruiz, C.E.; Rodés-Cabau, J.; Pache, G.; Colombo, A.; Nickenig, G.; Lee, M.; et al. A Bicuspid Aortic Valve Imaging Classification for the TAVR Era. JACC Cardiovasc. Imaging 2016, 9, 1145–1158. [Google Scholar] [CrossRef]
- Sun, B.J.; Lee, S.; Jang, J.Y.; Kwon, O.; Bae, J.S.; Lee, J.H.; Kim, D.-H.; Jung, S.-H.; Song, J.-M.; Kang, D.-H.; et al. Performance of a Simplified Dichotomous Phenotypic Classification of Bicuspid Aortic Valve to Predict Type of Valvulopathy and Combined Aortopathy. J. Am. Soc. Echocardiogr. 2017, 30, 1152–1161. [Google Scholar] [CrossRef]
- Murphy, I.G.; Collins, J.; Powell, A.; Markl, M.; McCarthy, P.; Malaisrie, S.C.; Carr, J.C.; Barker, A.J. Comprehensive 4-stage categorization of bicuspid aortic valve leaflet morphology by cardiac MRI in 386 patients. Int. J. Cardiovasc. Imaging 2017, 33, 1213–1221. [Google Scholar] [CrossRef]
- Bernard, C.; Morgant, M.C.; Guillier, D.; Cheynel, N.; Bouchot, O. Point on the Aortic Bicuspid Valve. Life 2022, 12, 518. [Google Scholar] [CrossRef]
- Groenendijk, B.C.; Hierck, B.P.; Gittenberger-De Groot, A.C.; Poelmann, R.E. Development-related changes in the expression of shear stress responsive genes KLF-2, ET-1, and NOS-3 in the developing cardiovascular system of chicken embryos. Dev. Dyn. 2004, 230, 57–68. [Google Scholar] [CrossRef]
- Noiri, E.; Lee, E.; Testa, J.; Quigley, J.; Colflesh, D.; Keese, C.R.; Giaever, I.; Goligorsky, M.S. Podokinesis in endothelial cell migration: Role of nitric oxide. Am. J. Physiol. Physiol. 1998, 274, C236–C244. [Google Scholar] [CrossRef]
- Fernández, B.; Durán, A.C.; Fernández-Gallego, T.; Fernández, M.C.; Such, M.; Arqué, J.M.; Sans-Coma, V. Bicuspid Aortic Valves with Different Spatial Orientations of the Leaflets Are Distinct Etiological Entities. J. Am. Coll. Cardiol. 2009, 54, 2312–2318. [Google Scholar] [CrossRef] [Green Version]
- Fernández, B.; Soto-Navarrete, M.T.; López-García, A.; López-Unzu, M.; Durán, A.C.; Fernández, M.C. Bicuspid Aortic Valve in 2 Model Species and Review of the Literature. Veter. Pathol. 2020, 57, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Phillips, H.M.; Mahendran, P.; Singh, E.; Anderson, R.H.; Chaudhry, B.; Henderson, D.J. Neural crest cells are required for correct positioning of the developing outflow cushions and pattern the arterial valve leaflets. Cardiovasc. Res. 2013, 99, 452–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sans-Coma, V.; Fernández, B.; Durán, A.C.; Thiene, G.; Arqué, J.M.; Muñoz-Chápuli, R.; Cardo, M. Fusion of valve cushions as a key factor in the formation of congenital bicuspid aortic valves in Syrian hamsters. Anat. Rec. 1996, 244, 490–498. [Google Scholar] [CrossRef]
- Soto-Navarrete, M.T.; López-Unzu, M.; Durán, A.C.; Fernández, B. Embryonic development of bicuspid aortic valves. Prog. Cardiovasc. Dis. 2020, 63, 407–418. [Google Scholar] [CrossRef]
- Evangelista, A.; Gallego, P.; Calvo-Iglesias, F.; Bermejo, J.; Robledo-Carmona, J.; Sánchez, V.; Saura, D.; Arnold, R.; Carro, A.; Maldonado, G.; et al. Anatomical and clinical predictors of valve dysfunction and aortic dilation in bicuspid aortic valve disease. Heart 2018, 104, 566–573. [Google Scholar] [CrossRef]
- Kong, W.K.F.; Delgado, V.; Poh, K.K.; Regeer, M.V.; Ng, A.C.; McCormack, L.; Yeo, T.C.; Shanks, M.; Parent, S.; Enache, R.; et al. Prognostic Implications of Raphe in Bicuspid Aortic Valve Anatomy. JAMA Cardiol. 2017, 2, 285–292. [Google Scholar] [CrossRef]
- Kong, W.K.F.; Regeer, M.V.; Poh, K.K.; Yip, J.W.; van Rosendael, P.; Yeo, T.C.; Tay, E.; Kamperidis, V.; Van Der Velde, E.T.; Mertens, B.; et al. Inter-ethnic differences in valve morphology, valvular dysfunction, and aortopathy between Asian and European patients with bicuspid aortic valve. Eur. Heart J. 2018, 39, 1308–1313. [Google Scholar] [CrossRef]
- Niaz, T.; Poterucha, J.T.; Olson, T.M.; Johnson, J.N.; Craviari, C.; Nienaber, T.; Palfreeman, J.; Cetta, F.; Hagler, D.J. Characteristic Morphologies of the Bicuspid Aortic Valve in Patients with Genetic Syndromes. J. Am. Soc. Echocardiogr. 2018, 31, 194–200. [Google Scholar] [CrossRef]
- Sun, B.J.; Jin, X.; Song, J.-K.; Lee, S.; Lee, J.H.; Park, J.-B.; Lee, S.-P.; Kim, D.-H.; Park, S.-J.; Kim, Y.-J.; et al. Clinical Characteristics of Korean Patients with Bicuspid Aortic Valve Who Underwent Aortic Valve Surgery. Korean Circ. J. 2018, 48, 48–58. [Google Scholar] [CrossRef]
- Yang, L.T.; Pellikka, P.A.; Enriquez-Sarano, M.; Maalouf, J.F.; Scott, C.G.; Michelena, H.I. Stage B Aortic Regurgitation in Bicuspid Aortic Valve: New Observations on Progression Rate and Predictors. JACC Cardiovasc. Imaging 2020, 13, 1442–1445. [Google Scholar] [CrossRef]
- Fernandes, S.M.; Khairy, P.; Sanders, S.P.; Colan, S.D. Bicuspid Aortic Valve Morphology and Interventions in the Young. J. Am. Coll. Cardiol. 2007, 49, 2211–2214. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, S.M.; Sanders, S.P.; Khairy, P.; Jenkins, K.J.; Gauvreau, K.; Lang, P.; Simonds, H.; Colan, S.D. Morphology of bicuspid aortic valve in children and adolescents. J. Am. Coll. Cardiol. 2004, 44, 1648–1651. [Google Scholar] [CrossRef] [Green Version]
- Michelena, H.I.; Della Corte, A.; Evangelista, A.; Maleszewski, J.J.; Enriquez-Sarano, M.; Bax, J.J.; Otto, C.M.; Schäfers, H.-J. Speaking a common language: Introduction to a standard terminology for the bicuspid aortic valve and its aortopathy. Prog. Cardiovasc. Dis. 2020, 63, 419–424. [Google Scholar] [CrossRef]
- Sperling, J.S.; Lubat, E. Forme fruste or ‘Incomplete’ bicuspid aortic valves with very small raphes: The prevalence of bicuspid valve and its significance may be underestimated. Int. J. Cardiol. 2015, 184, 1–5. [Google Scholar] [CrossRef]
- American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Echocardiography; American Heart Association; American Society of Nuclear Cardiology; Heart Failure Society of America; Heart Rhythm Society; Society for Cardiovascular Angiography and Interventions; Society of Critical Care Medicine; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. J. Am. Soc. Echocardiogr. 2011, 24, 229–267. [Google Scholar]
- Guala, A.; Rodriguez-Palomares, J.; Galian-Gay, L.; Teixido-Tura, G.; Johnson, K.M.; Wieben, O.; Avilés, A.S.; Evangelista, A. Partial Aortic Valve Leaflet Fusion Is Related to Deleterious Alteration of Proximal Aorta Hemodynamics. Circulation 2019, 139, 2707–2709. [Google Scholar] [CrossRef]
- Michelena, H.I.; Yang, L.-T.; Enriquez-Sarano, M.; Pochettino, A. The elusive ‘forme fruste’ bicuspid aortic valve: 3D transoesophageal echocardiography to the rescue. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1169. [Google Scholar] [CrossRef]
- Borger, M.A.; Fedak, P.W.; Stephens, E.H.; Gleason, T.G.; Girdauskas, E.; Ikonomidis, J.S.; Khoynezhad, A.; Siu, S.C.; Verma, S.; Hope, M.D.; et al. The American Association for Thoracic Surgery consensus guidelines on bicuspid aortic valve–related aortopathy: Full online-only version. J. Thorac. Cardiovasc. Surg. 2018, 156, e41–e74. [Google Scholar] [CrossRef]
- Aicher, D.; Kunihara, T.; Issa, O.A.; Brittner, B.; Gräber, S.; Schäfers, H.-J. Valve Configuration Determines Long-Term Results After Repair of the Bicuspid Aortic Valve. Circulation 2011, 123, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Jahanyar, J.; de Kerchove, L.; El Khoury, G. Bicuspid aortic valve repair: The 180 degrees -Reimplantation technique. Ann. Cardiothorac. Surg. 2022, 11, 473–481. [Google Scholar] [CrossRef]
- Ikonomidis, J.S.; Ruddy, J.M.; Benton, S.M.; Arroyo, J.; Brinsa, T.A.; Stroud, R.E.; Zeeshan, A.; Bavaria, J.E.; Gorman, J.H.; Gorman, R.C.; et al. Aortic Dilatation with Bicuspid Aortic Valves: Cusp Fusion Correlates to Matrix Metalloproteinases and Inhibitors. Ann. Thorac. Surg. 2012, 93, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadros, T.M.; Klein, M.D.; Shapira, O.M. Ascending aortic dilatation associated with bicuspid aortic valve: Pathophysiology, molecular biology, and clinical implications. Circulation 2009, 119, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Siu, S.C. Aortic Dilatation in Patients with Bicuspid Aortic Valve. New Engl. J. Med. 2014, 370, 1920–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Palomares, J.F.; Dux-Santoy, L.; Guala, A.; Kale, R.; Maldonado, G.; Teixidó-Turà, G.; Galian, L.; Huguet, M.; Valente, F.; Gutiérrez, L.; et al. Aortic flow patterns and wall shear stress maps by 4D-flow cardiovascular magnetic resonance in the assessment of aortic dilatation in bicuspid aortic valve disease. J. Cardiovasc. Magn. Reson. 2018, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Barker, A.J.; Markl, M.; Bürk, J.; Lorenz, R.; Bock, J.; Bauer, S.; Schulz-Menger, J.; von Knobelsdorff-Brenkenhoff, F. Bicuspid Aortic Valve Is Associated with Altered Wall Shear Stress in the Ascending Aorta. Circ. Cardiovasc. Imaging 2012, 5, 457–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, G.; Nistri, S.; Giusti, B.; Sticchi, E.; Attanasio, M.; Porciani, C.; Abbate, R.; Bonow, R.O.; Yacoub, M.; Gensini, G.F. Identification of fibrillin 1 gene mutations in patients with bicuspid aortic valve (BAV) without Marfan syndrome. BMC Med. Genet. 2014, 15, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazel, S.S.; Mallidi, H.R.; Lee, R.S.; Sheehan, M.P.; Liang, D.; Fleischmann, D.; Herfkens, R.; Mitchell, R.S.; Miller, D.C. The aortopathy of bicuspid aortic valve disease has distinctive patterns and usually involves the transverse aortic arch. J. Thorac. Cardiovasc. Surg. 2008, 135, 901–907.e2. [Google Scholar] [CrossRef] [Green Version]
- Girdauskas, E.; Disha, K.; Rouman, M.; Espinoza, A.; Borger, M.; Kuntze, T. Aortic events after isolated aortic valve replacement for bicuspid aortic valve root phenotype: Echocardiographic follow-up study. Eur. J. Cardio-Thorac. Surg. 2015, 48, e71–e76. [Google Scholar] [CrossRef] [Green Version]
- Forte, A.; Yin, X.; Fava, M.; Bancone, C.; Cipollaro, M.; De Feo, M.; Mayr, M.; Jahangiri, M.; Della Corte, A. Locally different proteome in aortas from patients with stenotic tricuspid and bicuspid aortic valvesdagger. Eur. J. Cardiothorac. Surg. 2019, 56, 458–469. [Google Scholar] [CrossRef]
- Guzzardi, D.G.; Barker, A.J.; Van Ooij, P.; Malaisrie, S.C.; Puthumana, J.J.; Belke, D.D.; Mewhort, H.E.; Svystonyuk, D.A.; Kang, S.; Verma, S.; et al. Valve-Related Hemodynamics Mediate Human Bicuspid Aortopathy: Insights from Wall Shear Stress Mapping. J. Am. Coll. Cardiol. 2015, 66, 892–900. [Google Scholar] [CrossRef]
- Sigovan, M.; Hope, M.D.; Dyverfeldt, P.; Saloner, D. Comparison of four-dimensional flow parameters for quantification of flow eccentricity in the ascending aorta. J. Magn. Reson. Imaging 2011, 34, 1226–1230. [Google Scholar] [CrossRef]
- Hess, A.T.; Bissell, M.M.; Glaze, S.J.; Pitcher, A.; Myerson, S.; Neubauer, S.; Robson, M.D. Evaluation of Circulation, Γ, as a quantifying metric in 4D flow MRI. J. Cardiovasc. Magn. Reson. 2013, 15, E36. [Google Scholar] [CrossRef] [Green Version]
- Bensalah, M.Z.; Bollache, E.; Kachenoura, N.; Giron, A.; De Cesare, A.; Macron, L.; Lefort, M.; Redheuill, A.; Mousseaux, E. Geometry is a major determinant of flow reversal in proximal aorta. Am. J. Physiol. Circ. Physiol. 2014, 306, H1408–H1416. [Google Scholar] [CrossRef] [Green Version]
- Ayad, R.F.; Grayburn, P.A.; Ko, J.M.; Filardo, G.; Roberts, W.C. Accuracy of Two-Dimensional Echocardiography in Determining Aortic Valve Structure in Patients > 50 Years of Age Having Aortic Valve Replacement for Aortic Stenosis. Am. J. Cardiol. 2011, 108, 1589–1599. [Google Scholar] [CrossRef]
- Michelena, H.I.; Chandrasekaran, K.; Topilsky, Y.; Messika-Zeitoun, D.; Della Corte, A.; Evangelista, A.; Schäfers, H.-J.; Enriquez-Sarano, M. The Bicuspid Aortic Valve Condition: The Critical Role of Echocardiography and the Case for a Standard Nomenclature Consensus. Prog. Cardiovasc. Dis. 2018, 61, 404–415. [Google Scholar] [CrossRef]
- Michelena, H.I.; Khanna, A.D.; Mahoney, D.; Margaryan, E.; Topilsky, Y.; Suri, R.M.; Eidem, B.; Edwards, W.D.; Sundt, T.M.; Enriquez-Sarano, M. Incidence of Aortic Complications in Patients with Bicuspid Aortic Valves. JAMA 2011, 306, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Ugur, M.; Schaff, H.V.; Suri, R.M.; Dearani, J.A.; Joyce, L.D.; Greason, K.L.; Connolly, H.M. Late Outcome of Noncoronary Sinus Replacement in Patients with Bicuspid Aortic Valves and Aortopathy. Ann. Thorac. Surg. 2014, 97, 1242–1246. [Google Scholar] [CrossRef]
- Robicsek, F.; Thubrikar, M.J.; Cook, J.W.; Fowler, B. The congenitally bicuspid aortic valve: How does it function? Why does it fail? Ann. Thorac. Surg. 2004, 77, 177–185. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef] [Green Version]
- Niaz, T.; Poterucha, J.T.; Johnson, J.N.; Craviari, C.; Nienaber, T.; Palfreeman, J.; Cetta, F.; Hagler, D.J. Incidence, morphology, and progression of bicuspid aortic valve in pediatric and young adult subjects with coexisting congenital heart defects. Congenit. Heart Dis. 2017, 12, 261–269. [Google Scholar] [CrossRef]
- Park, J.Y.; Foley, T.A.; Bonnichsen, C.R.; Maurer, M.J.; Goergen, K.M.; Nkomo, V.T.; Enriquez-Sarano, M.; Williamson, E.E.; Michelena, H.I. Transthoracic Echocardiography versus Computed Tomography for Ascending Aortic Measurements in Patients with Bicuspid Aortic Valve. J. Am. Soc. Echocardiogr. 2017, 30, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Beyersdorf, F.; Vahanian, A.; Milojevic, M.; Praz, F.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardio-Thorac. Surg. 2021, 60, 727–800. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Budde, R.P.; Bremerich, J.; Dacher, J.N.; Loewe, C.; Wolf, F.; Natale, L.; Pontone, G.; Redheuil, A.; Vliegenthart, R.; et al. CT and MR imaging prior to transcatheter aortic valve implantation: Standardisation of scanning protocols, measurements and reporting-a consensus document by the European Society of Cardiovascular Radiology (ESCR). Eur. Radiol. 2020, 30, 2627–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amoretti, F.; Cerillo, A.G.; Mariani, M.; Stefano, P. A simple method to visualize the bicuspid aortic valve pathology by cardiac computed tomography. J. Cardiovasc. Comput. Tomogr. 2020, 14, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; De Backer, O.; Bieliauskas, G.; Wong, I.; Bajoras, V.; Xiong, T.-Y.; Zhang, Y.; Kofoed, K.F.; Chen, M.; Sondergaard, L. Cusp Symmetry and Coronary Ostial Eccentricity and its Impact on Coronary Access Following TAVR. JACC Cardiovasc. Interv. 2022, 15, 123–134. [Google Scholar] [CrossRef]
- Chirichilli, I.; Irace, F.G.; Weltert, L.P.; Salica, A.; Wolf, L.G.; Fusca, S.; Ricci, A.; De Paulis, R. A direct correlation between commissural orientation and annular shape in bicuspid aortic valves: A new anatomical and computed tomography classification. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Spath, N.B.; Singh, T.; Papanastasiou, G.; Baker, A.; Janiczek, R.J.; McCann, G.P.; Dweck, M.R.; Kershaw, L.; Newby, D.E.; Semple, S. Assessment of stunned and viable myocardium using manganese-enhanced MRI. Open Heart 2021, 8, e001646. [Google Scholar] [CrossRef]
- Bissell, M.; Hess, A.T.; Biasiolli, L.; Glaze, S.J.; Loudon, M.; Pitcher, A.; Davis, A.; Prendergast, B.; Markl, M.; Barker, A.J.; et al. Aortic dilation in bicuspid aortic valve disease: Flow pattern is a major contributor and differs with valve fusion type. Circ. Cardiovasc. Imaging 2013, 6, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Hope, M.D.; Hope, T.A.; Crook, S.E.; Ordovas, K.G.; Urbania, T.H.; Alley, M.T.; Higgins, C.B. 4D Flow CMR in Assessment of Valve-Related Ascending Aortic Disease. JACC Cardiovasc. Imaging 2011, 4, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, R.; Bock, J.; Barker, A.J.; von Knobelsdorff-Brenkenhoff, F.; Wallis, W.; Korvink, J.G.; Bissell, M.M.; Schulz-Menger, J.; Markl, M. 4D flow magnetic resonance imaging in bicuspid aortic valve disease demonstrates altered distribution of aortic blood flow helicity. Magn. Reson. Med. 2014, 71, 1542–1553. [Google Scholar] [CrossRef]
- Meierhofer, C.; Schneider, E.P.; Lyko, C.; Hutter, A.; Martinoff, S.; Markl, M.; Hager, A.; Hess, J.; Stern, H.; Fratz, S. Wall shear stress and flow patterns in the ascending aorta in patients with bicuspid aortic valves differ significantly from tricuspid aortic valves: A prospective study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Trinh, B.; Dubin, I.; Rahman, O.; Botelho, M.P.; Naro, N.; Carr, J.C.; Collins, J.D.; Barker, A.J. Aortic Volumetry at Contrast-Enhanced Magnetic Resonance Angiography: Feasibility as a Sensitive Method for Monitoring Bicuspid Aortic Valve Aortopathy. Investig. Radiol. 2017, 52, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Pascaner, A.F.; Houriez--Gombaud-Saintonge, S.; Craiem, D.; Gencer, U.; Casciaro, M.E.; Charpentier, E.; Bouaou, K.; De Cesare, A.; Dietenbeck, T.; Chenoune, Y.; et al. Comprehensive assessment of local and regional aortic stiffness in patients with tricuspid or bicuspid aortic valve aortopathy using magnetic resonance imaging. Int. J. Cardiol. 2021, 326, 206–212. [Google Scholar] [CrossRef]
- Goldstein, S.A.; Evangelista, A.; Abbara, S.; Arai, A.; Asch, F.M.; Badano, L.P.; Bolen, M.A.; Connolly, H.M.; Cuéllar-Calàbria, H.; Czerny, M.; et al. Multimodality imaging of diseases of the thoracic aorta in adults: From the American Society of Echocardiography and the European Association of Cardiovascular Imaging: Endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2015, 28, 119–182. [Google Scholar]
- Keane, M.G.; Wiegers, S.E.; Plappert, T.; Pochettino, A.; Bavaria, J.E.; Sutton, M.G. Bicuspid aortic valves are associated with aortic dilatation out of proportion to coexistent valvular lesions. Circulation 2000, 102, III35–III39. [Google Scholar] [CrossRef]
- Kerstjens-Frederikse, W.S.; Sarvaas, G.J.; Ruiter, J.S.; Van Den Akker, P.C.; Temmerman, A.M.; Van Melle, J.P.; Hofstra, R.M.; Berger, R.M. Left ventricular outflow tract obstruction: Should cardiac screening be offered to first-degree relatives? Heart 2011, 97, 1228–1232. [Google Scholar] [CrossRef]
- Masri, A.; Svensson, L.G.; Griffin, B.P.; Desai, M.Y. Contemporary natural history of bicuspid aortic valve disease: A systematic review. Heart 2017, 103, 1323–1330. [Google Scholar] [CrossRef]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E., Jr.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: Executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter. Cardiovasc. Interv. 2010, 76, E43–E86. [Google Scholar]
- MacKay, E.J.; Zhang, B.; Augoustides, J.G.; Groeneveld, P.W.; Desai, N.D. Association of Intraoperative Transesophageal Echocardiography and Clinical Outcomes After Open Cardiac Valve or Proximal Aortic Surgery. JAMA Netw. Open 2022, 5, e2147820. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 77, 450–500. [Google Scholar] [CrossRef]
- Van Andel, M.M.; Indrakusuma, R.; Jalalzadeh, H.; Balm, R.; Timmermans, J.; Scholte, A.J.; van den Berg, M.P.; Zwinderman, A.H.; Mulder, B.J.; de Waard, V.; et al. Long-term clinical outcomes of losartan in patients with Marfan syndrome: Follow-up of the multicentre randomized controlled COMPARE trial. Eur. Heart J. 2020, 41, 4181–4187. [Google Scholar] [CrossRef] [PubMed]
- Elefteriades, J.A. Natural history of thoracic aortic aneurysms: Indications for surgery, and surgical versus nonsurgical risks. Ann. Thorac. Surg. 2002, 74, S1877–S1880. [Google Scholar] [CrossRef]
- Beckerman, Z.; Kayatta, M.O.; McPherson, L.; Binongo, J.N.; Lasanajak, Y.; Leshnower, B.G.; Chen, E.P. Bicuspid aortic valve repair in the setting of severe aortic insufficiency. J. Vis. Surg. 2018, 4, 101. [Google Scholar] [CrossRef] [PubMed]
- Borger, M.A.; Preston, M.; Ivanov, J.; Fedak, P.W.; Davierwala, P.; Armstrong, S.; David, T.E. Should the ascending aorta be replaced more frequently in patients with bicuspid aortic valve disease? J. Thorac. Cardiovasc. Surg. 2004, 128, 677–683. [Google Scholar] [CrossRef] [Green Version]
- David, T.E.; Feindel, C.M.; David, C.M.; Manlhiot, C. A quarter of a century of experience with aortic valve-sparing operations. J. Thorac. Cardiovasc. Surg. 2014, 148, 872–880. [Google Scholar] [CrossRef] [Green Version]
- Davies, R.; Kaple, R.K.; Mandapati, D.; Gallo, A.; Botta, D.M.; Elefteriades, J.A.; Coady, M.A. Natural History of Ascending Aortic Aneurysms in the Setting of an Unreplaced Bicuspid Aortic Valve. Ann. Thorac. Surg. 2007, 83, 1338–1344. [Google Scholar] [CrossRef]
- Ergin, M.A.; Spielvogel, D.; Apaydin, A.; Lansman, S.L.; McCullough, J.N.; Galla, J.D.; Griepp, R.B. Surgical treatment of the dilated ascending aorta: When and how? Ann. Thorac. Surg. 1999, 67, 1834–1839. [Google Scholar] [CrossRef]
- Svensson, L.G.; Kim, K.-H.; Lytle, B.W.; Cosgrove, D.M. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection in patients with bicuspid aortic valves. J. Thorac. Cardiovasc. Surg. 2003, 126, 892–893. [Google Scholar] [CrossRef] [Green Version]
- Park, C.B.; Greason, K.L.; Suri, R.M.; Michelena, H.I.; Schaff, H.V.; Sundt, T.M. Fate of nonreplaced sinuses of Valsalva in bicuspid aortic valve disease. J. Thorac. Cardiovasc. Surg. 2011, 142, 278–284. [Google Scholar] [CrossRef] [Green Version]
- Schneider, U.; Feldner, S.K.; Hofmann, C.; Schöpe, J.; Wagenpfeil, S.; Giebels, C.; Schäfers, H.-J. Two decades of experience with root remodeling and valve repair for bicuspid aortic valves. J. Thorac. Cardiovasc. Surg. 2017, 153, S65–S71. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, H.; Nakatani, S.; Stugaard, M.; Tsujita-Kuroda, Y.; Bando, K.; Kobayashi, J.; Yamagishi, M.; Kitakaze, M.; Kitamura, S.; Miyatake, K. Failure to Prevent Progressive Dilation of Ascending Aorta by Aortic Valve Replacement in Patients with Bicuspid Aortic Valve: Comparison with Tricuspid Aortic Valve. Circulation 2003, 108 (Suppl. S1), II291–II294. [Google Scholar] [CrossRef] [Green Version]
- Mastrobuoni, S.; de Kerchove, L.; Solari, S.; Astarci, P.; Poncelet, A.; Noirhomme, P.; Rubay, J.; El Khoury, G. The Ross procedure in young adults: Over 20 years of experience in our Institution. Eur. J. Cardio-Thorac. Surg. 2015, 49, 507–513. [Google Scholar] [CrossRef]
- De Meester, C.; Vanovershelde, J.L.; Jahanyar, J.; Tamer, S.; Mastrobuoni, S.; Van Dyck, M.; Navarra, E.; Poncelet, A.; Astarci, P.; El Khoury, G.; et al. Long-term durability of bicuspid aortic valve repair: A comparison of 2 annuloplasty techniques. Eur. J. Cardiothorac. Surg. 2021, 60, 286–294. [Google Scholar] [CrossRef]
- Nazer, R.I.; Elhenawy, A.M.; Fazel, S.S.; Garrido-Olivares, L.E.; Armstrong, S.; David, T.E. The Influence of Operative Techniques on the Outcomes of Bicuspid Aortic Valve Disease and Aortic Dilatation. Ann. Thorac. Surg. 2010, 89, 1918–1924. [Google Scholar] [CrossRef]
- Mazine, A.; El-Hamamsy, I.; Verma, S.; Peterson, M.D.; Bonow, R.O.; Yacoub, M.H.; David, T.E.; Bhatt, D.L. Ross Procedure in Adults for Cardiologists and Cardiac Surgeons: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2761–2777. [Google Scholar] [CrossRef]
- Nappi, F.; Nenna, A.; Spadaccio, C.; Chello, M. Pulmonary autograft in aortic position: Is everything known? Transl. Pediatr. 2017, 6, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Singh, S.S.A.; Bellomo, F.; Nappi, P.; Iervolino, A.; Acar, C. The Choice of Pulmonary Autograft in Aortic Valve Surgery: A State-of-the-Art Primer. BioMed. Res. Int. 2021, 2021, 5547342. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C.; Acar, C.; El-Hamamsy, I. Lights and Shadows on the Ross Procedure: Biological Solutions for Biological Problems. Semin. Thorac. Cardiovasc. Surg. 2020, 32, 815–822. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C.; Chello, M.; Acar, C. The Ross procedure: Underuse or under-comprehension? J. Thorac. Cardiovasc. Surg. 2015, 149, 1463–1464. [Google Scholar] [CrossRef] [Green Version]
- Svensson, L.G.; Kim, K.H.; Blackstone, E.H.; Rajeswaran, J.; Gillinov, A.M.; Mihaljevic, T.; Griffin, B.P.; Grimm, R.; Stewart, W.J.; Hammer, D.F.; et al. Bicuspid aortic valve surgery with proactive ascending aorta repair. J. Thorac. Cardiovasc. Surg. 2011, 142, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Yang, J.; Lu, Y.; Fan, W.; Bai, L.; Nie, Z.; Wang, R.; Yu, J.; Liu, L.; Liu, Y.; et al. Thoracic Aorta Diameter Calculation by Artificial Intelligence Can Predict the Degree of Arterial Stiffness. Front. Cardiovasc. Med. 2021, 8, 737161. [Google Scholar] [CrossRef]
- Davies, R.R.; Goldstein, L.J.; Coady, M.A.; Tittle, S.L.; Rizzo, J.A.; Kopf, G.S.; Elefteriades, J.A. Yearly rupture or dissection rates for thoracic aortic aneurysms: Simple prediction based on size. Ann. Thorac. Surg. 2002, 73, 17–28. [Google Scholar] [CrossRef]
- Russo, C.F.; Mazzetti, S.; Garatti, A.; Ribera, E.; Milazzo, A.; Bruschi, G.; Lanfranconi, M.; Colombo, T.; Vitali, E. Aortic complications after bicuspid aortic valve replacement: Long-term results. Ann. Thorac. Surg. 2002, 74, S1773–S1776. [Google Scholar] [CrossRef]
- Girdauskas, E.; Disha, K.; Borger, M.; Kuntze, T. Long-term prognosis of ascending aortic aneurysm after aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J. Thorac. Cardiovasc. Surg. 2014, 147, 276–282. [Google Scholar] [CrossRef] [Green Version]
- McKellar, S.H.; Michelena, H.I.; Li, Z.; Schaff, H.V.; Sundt, T.M. Long-Term Risk of Aortic Events Following Aortic Valve Replacement in Patients with Bicuspid Aortic Valves. Am. J. Cardiol. 2010, 106, 1626–1633. [Google Scholar] [CrossRef]
- Boodhwani, M.; Andelfinger, G.; Leipsic, J.; Lindsay, T.; McMurtry, M.S.; Therrien, J.; Siu, S.C. Canadian Cardiovascular Society Position Statement on the Management of Thoracic Aortic Disease. Can. J. Cardiol. 2014, 30, 577–589. [Google Scholar] [CrossRef]
- Pacheco, C.; Mullen, K.A.; Coutinho, T.; Jaffer, S.; Parry, M.; van Spall, H.G.C.; Clavel, M.-A.; Clavel Ma Edwards, J.D.; Sedlak, T.; Norris, C.M.; et al. The Canadian Women’s Heart Health Alliance Atlas on the Epidemiology, Diagnosis, and Management of Cardiovascular Disease in Women—Chapter 5: Sex- and Gender-Unique Manifestations of Cardiovascular Disease. CJC Open 2022, 4, 243–262. [Google Scholar] [CrossRef]
- Kanjanahattakij, N.; Horn, B.; Vutthikraivit, W.; Biso, S.M.; Ziccardi, M.R.; Lu, M.L.R.; Rattanawong, P. Comparing outcomes after transcatheter aortic valve replacement in patients with stenotic bicuspid and tricuspid aortic valve: A systematic review and meta-analysis. Clin. Cardiol. 2018, 41, 896–902. [Google Scholar] [CrossRef] [Green Version]
- Makkar, R.R.; Yoon, S.-H.; Leon, M.B.; Chakravarty, T.; Rinaldi, M.; Shah, P.B.; Skipper, E.R.; Thourani, V.H.; Babaliaros, V.; Cheng, W.; et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. JAMA 2019, 321, 2193–2202. [Google Scholar] [CrossRef] [Green Version]
- Takagi, H.; Hari, Y.; Kawai, N.; Kuno, T.; Ando, T. Meta-analysis of transcatheter aortic valve implantation for bicuspid versus tricuspid aortic valves. J. Cardiol. 2019, 74, 40–48. [Google Scholar] [CrossRef]
- Biner, S.; Rafique, A.M.; Ray, I.; Cuk, O.; Siegel, R.J.; Tolstrup, K. Aortopathy Is Prevalent in Relatives of Bicuspid Aortic Valve Patients. J. Am. Coll. Cardiol. 2009, 53, 2288–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, T.E.; Woo, A.; Armstrong, S.; Maganti, M. When is the Ross operation a good option to treat aortic valve disease? J. Thorac. Cardiovasc. Surg. 2010, 139, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Nenna, A.; Larobina, D.; Carotenuto, A.R.; Jarraya, M.; Spadaccio, C.; Fraldi, M.; Chello, M.; Acar, C.; Carrel, T. Simulating the ideal geometrical and biomechanical parameters of the pulmonary autograft to prevent failure in the Ross operation. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Sievers, H.H.; Stierle, U.; Charitos, E.I.; Takkenberg, J.J.; Hoerer, J.; Lange, R.; Franke, U.; Albert, M.; Gorski, A.; Leyh, R.G.; et al. A multicentre evaluation of the autograft procedure for young patients undergoing aortic valve replacement: Update on the German Ross Registrydagger. Eur. J. Cardiothorac. Surg. 2016, 49, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Sievers, H.-H.; Stierle, U.; Petersen, M.; Klotz, S.; Richardt, D.; Diwoky, M.; Charitos, E.I. Valve performance classification in 630 subcoronary Ross patients over 22 years. J. Thorac. Cardiovasc. Surg. 2018, 156, 79–86.e2. [Google Scholar] [CrossRef] [Green Version]
- Andreas, M.; Seebacher, G.; Reida, E.; Wiedemann, D.; Pees, C.; Rosenhek, R.; Heinze, G.; Moritz, A.; Kocher, A.; Laufer, G. A Single-Center Experience with the Ross Procedure Over 20 Years. Ann. Thorac. Surg. 2014, 97, 182–188. [Google Scholar] [CrossRef]
- Da Costa, F.D.; Takkenberg, J.J.; Fornazari, D.; Balbi Filho, E.M.; Colatusso, C.; Mokhles, M.M.; da Costa, A.B.; Sagrado, A.G.; Ferreira, A.D.; Fernandes, T.; et al. Long-term results of the Ross operation: An 18-year single institutional experience. Eur. J. Cardiothorac. Surg. 2014, 46, 415–422. [Google Scholar] [CrossRef] [Green Version]
- David, T.E.; David, C.; Woo, A.; Manlhiot, C. The Ross procedure: Outcomes at 20 years. J. Thorac. Cardiovasc. Surg. 2014, 147, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Martin, E.; Mohammadi, S.; Jacques, F.; Kalavrouziotis, D.; Voisine, P.; Doyle, D.; Perron, J. Clinical Outcomes Following the Ross Procedure in Adults: A 25-Year Longitudinal Study. J. Am. Coll. Cardiol. 2017, 70, 1890–1899. [Google Scholar] [CrossRef]
- Skillington, P.D.; Mokhles, M.M.; Takkenberg, J.; Larobina, M.; O’Keefe, M.; Wynne, R.; Tatoulis, J. The Ross procedure using autologous support of the pulmonary autograft: Techniques and late results. J. Thorac. Cardiovasc. Surg. 2015, 149, S46–S52. [Google Scholar] [CrossRef] [Green Version]
- Spadaccio, C.; Montagnani, S.; Acar, C.; Nappi, F. Introducing bioresorbable scaffolds into the show. A potential adjunct to resuscitate Ross procedure. Int. J. Cardiol. 2015, 190, 50–52. [Google Scholar] [CrossRef]
- Bouhout, I.; Poirier, N.; Mazine, A.; Dore, A.; Mercier, L.-A.; Leduc, L.; El-Hamamsy, I. Cardiac, Obstetric, and Fetal Outcomes During Pregnancy After Biological or Mechanical Aortic Valve Replacement. Can. J. Cardiol. 2014, 30, 801–807. [Google Scholar] [CrossRef]
- Buratto, E.; Shi, W.Y.; Wynne, R.; Poh, C.L.; Larobina, M.; O’Keefe, M.; Goldblatt, J.; Tatoulis, J.; Skillington, P.D. Improved Survival After the Ross Procedure Compared with Mechanical Aortic Valve Replacement. J. Am. Coll. Cardiol. 2018, 71, 1337–1344. [Google Scholar] [CrossRef]
- Mazine, A.; David, T.; Rao, V.; Hickey, E.; Christie, S.; Manlhiot, C.; Ouzounian, M. Long-term outcomes of the ross procedure versus mechanical aortic valve replacement: A propensity-matched cohort study. Can. J. Cardiol. 2016, 32, S234–S235. [Google Scholar] [CrossRef]
- Steinberg, Z.L.; Dominguez-Islas, C.P.; Otto, C.M.; Stout, K.K.; Krieger, E.V. Maternal and Fetal Outcomes of Anticoagulation in Pregnant Women with Mechanical Heart Valves. J. Am. Coll. Cardiol. 2017, 69, 2681–2691. [Google Scholar] [CrossRef]
- Ikonomidis, J.S.; Kratz, J.M.; Crumbley, A.J., III; Stroud, M.R.; Bradley, S.M.; Sade, R.M.; Crawford, F.A., Jr. Twenty-year experience with the St Jude Medical mechanical valve prosthesis. J. Thorac. Cardiovasc. Surg. 2003, 126, 2022–2031. [Google Scholar] [CrossRef] [Green Version]
- Van Nooten, G.J.; Caes, F.; Francois, K.; Van Bellleghem, Y.; Bové, T.; Vandenplas, G.; Taeymans, Y. Twenty years’ single-center experience with mechanical heart valves: A critical review of anticoagulation policy. J. Heart Valve Dis. 2012, 21, 88–98. [Google Scholar]
- Takkenberg, J.J.; Klieverik, L.M.; Schoof, P.H.; van Suylen, R.J.; van Herwerden, L.A.; Zondervan, P.E.; Roos-Hesselink, J.W.; Eijkemans, M.J.; Yacoub, M.H.; Bogers, A.J. The Ross procedure: A systematic review and meta-analysis. Circulation 2009, 119, 222–228. [Google Scholar] [CrossRef] [Green Version]
- El-Hamamsy, I.; Eryigit, Z.; Stevens, L.-M.; Sarang, Z.; George, R.; Clark, L.; Melina, G.; Takkenberg, J.J.; Yacoub, M.H. Long-term outcomes after autograft versus homograft aortic root replacement in adults with aortic valve disease: A randomised controlled trial. Lancet 2010, 376, 524–531. [Google Scholar] [CrossRef]
- Charitos, E.I.; Takkenberg, J.J.; Hanke, T.; Gorski, A.; Botha, C.; Franke, U.; Dodge-Khatami, A.; Hoerer, J.; Lange, R.; Moritz, A.; et al. Reoperations on the pulmonary autograft and pulmonary homograft after the Ross procedure: An update on the German Dutch Ross Registry. J. Thorac. Cardiovasc. Surg. 2012, 144, 813–823. [Google Scholar] [CrossRef] [Green Version]
- Mokhles, M.M.; Rizopoulos, D.; Andrinopoulou, E.R.; Bekkers, J.A.; Roos-Hesselink, J.W.; Lesaffre, E.; Bogers, A.J.; Takkenberg, J.J. Autograft and pulmonary allograft performance in the second post-operative decade after the Ross procedure: Insights from the Rotterdam Prospective Cohort Study. Eur. Heart J. 2012, 33, 2213–2224. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Spadaccio, C.; Fraldi, M. Reply: Papillary Muscle Approximation Is an Anatomically Correct Repair for Ischemic Mitral Regurgitation. J. Am. Coll. Cardiol. 2016, 68, 1147–1148. [Google Scholar] [CrossRef]
- Nappi, F.; Nenna, A.; Petitti, T.; Spadaccio, C.; Gambardella, I.; Lusini, M.; Chello, M.; Acar, C. Long-term outcome of cryopreserved allograft for aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2018, 156, 1357–1365. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Specification |
|---|---|
| Date of Search (specified to date, month and year) | From January 2022 to May 2022 |
| Databases and other sources searched | PubMed |
| Search terms used (including MeSH and free text search terms and filters) | (BAV OR bicuspid aortopathy OR bicuspid aortic valve) AND (ultrasound OR computed tomography OR magnetic resonance OR US OR CT or MR) |
| Time frame | Up to May 2022 |
| Inclusion and exclusion criteria (study type, language restrictions, etc.) | English language |
| Selection process | Two authors independently selected articles after screening for duplicates. |
| Gene Expression | Pathology |
|---|---|
| miR-146-5p | BAV, aortic aneuurysm (convex region) |
| miR-21-5p | BAV, aortic aneuurysm (convex region) |
| miR-17 | Aoritc anurysm |
| miR 21 | Aortic aneurysm |
| miR-34 a | Aortic aneurysm |
| miR-122 | BAV |
| miR 130 a | BAV |
| miR-133a | TIMP1,TIMP2, aortic aneurysm |
| mi-R 143 | Aortic aneurysm |
| mi-R 145 | Aortic aneurysm |
| miR 146-5p | Aortic aneurysm |
| miR-200 | Endothelial-mesenchimal/epithelial mesenchimal |
| miR-423-5p | BAV, aortic aneurysm |
| miR-424-3p downregulation | Cell proliferation, apoptosis, endothelial cells alterations, aortic anuerysm |
| miR-486 | BAV |
| miR-494 | PECAM |
| miR-712 | Atherosclerosis, aortic aneurysm |
| miR-718 | Aortic aneurysm |
| ACTA2 | BAV. Aortic aneurysm |
| AXIN1-PDIA2 | BAV |
| ENG | BAV |
| FBN 1 | BAV |
| GATA4/GATA5/GATA6 | BAV |
| NOS3 | BAV |
| NOTCH1 (9q34.3) | BAV, outflow tract malformation |
| TGFb1/TGFb2 | Sporadic BAV, Loeys-Dietz syndrome |
| 18q | BAV |
| 5q | BAV |
| 13q | BAV |
| Author | Nomenclature |
|---|---|
| Roberts [36] 1970 | Anterior–posterior cusps Right–left cusps Presence of raphe |
| Brandenburg et al. [38] 1983 | Clock-face nomenclature: Commissures at 4–10 o’clock with raphe at 2 o’clock (R-L) Commissures at 1–6 o’clock with raphe at 10 o’clock (RN) Commissures at 3–9 o’clock without raphe (L-N) |
| Angelini et al. [39] 1989 | Anterior–posterior cusps Right–left cusps Presence of raphe |
| Sabet et al. [40] 1999 | RL RN LN Presence of raphe |
| Sievers and Schmidtke [41] 2007 | Type 0 (no raphe): anteroposterior or lateral cusps (true BAV) Type 1 (1 raphe): R-L, RN, L-N Type 2 (2 raphes): L-R, RN |
| Schaefer et al. [42] 2008 | Type 1: RL Type 2: RN Type 3: LN Presence of raphe Aorta: Type N: normal shape Type E: sinus effacement Type A: ascending aorta dilatation |
| Kang et al. [43] 2013 | Anteroposterior orientation: type 1: R-L with raphe type; 2: R-L without raphe Right–left orientation: Type 3: RN with raphe Type 4: L-N with raphe Type 5: symmetrical cusps with 1 coronary artery originating from each cusp Aorta: Type 0: normal Type 1: dilated root Type 2: dilated ascending aorta Type 3: diffuse involvement of the ascending aorta and arch |
| Michelena et al. [44] 2014 | BAVCon nomenclature: Type 1: R-L Type 2: RN Type 3: L-N Presence of raphe |
| Jilaihawi et al. [45] 2016 | Tricommissural: functional or acquired bicuspidity of a trileaflet valve Bicommissural with raphe Bicommissural without raphe |
| Sun et al. [46] 2017 | Dichotomous nomenclature: R-L Mixed: (RN or L-N) |
| Murphy et al. [47] 2017 | Clock-face nomenclature: Type 0: partial fusion/eccentric leaflet? Type 1: RN, RL, LN partial fusion/eccentric leaflet? Type 2: RL and RN, RL and LN, RN and LN partial fusion/eccentric leaflet? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, F.; Giacinto, O.; Lusini, M.; Garo, M.; Caponio, C.; Nenna, A.; Nappi, P.; Rousseau, J.; Spadaccio, C.; Chello, M. Patients with Bicuspid Aortopathy and Aortic Dilatation. J. Clin. Med. 2022, 11, 6002. https://doi.org/10.3390/jcm11206002
Nappi F, Giacinto O, Lusini M, Garo M, Caponio C, Nenna A, Nappi P, Rousseau J, Spadaccio C, Chello M. Patients with Bicuspid Aortopathy and Aortic Dilatation. Journal of Clinical Medicine. 2022; 11(20):6002. https://doi.org/10.3390/jcm11206002
Chicago/Turabian StyleNappi, Francesco, Omar Giacinto, Mario Lusini, Marialuisa Garo, Claudio Caponio, Antonio Nenna, Pierluigi Nappi, Juliette Rousseau, Cristiano Spadaccio, and Massimo Chello. 2022. "Patients with Bicuspid Aortopathy and Aortic Dilatation" Journal of Clinical Medicine 11, no. 20: 6002. https://doi.org/10.3390/jcm11206002
APA StyleNappi, F., Giacinto, O., Lusini, M., Garo, M., Caponio, C., Nenna, A., Nappi, P., Rousseau, J., Spadaccio, C., & Chello, M. (2022). Patients with Bicuspid Aortopathy and Aortic Dilatation. Journal of Clinical Medicine, 11(20), 6002. https://doi.org/10.3390/jcm11206002