
COVID-19 Infections in Adults with Congenital Heart Disease—A Prospective Single-Center Study in an Outpatient Setting

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Analysis
2.2. Positive Rate of Antibodies
2.3. International Physical Activity Questionnaire (IPAQ)
2.4. Cardiovascular Magnetic Resonance
2.5. Statistical Analyses
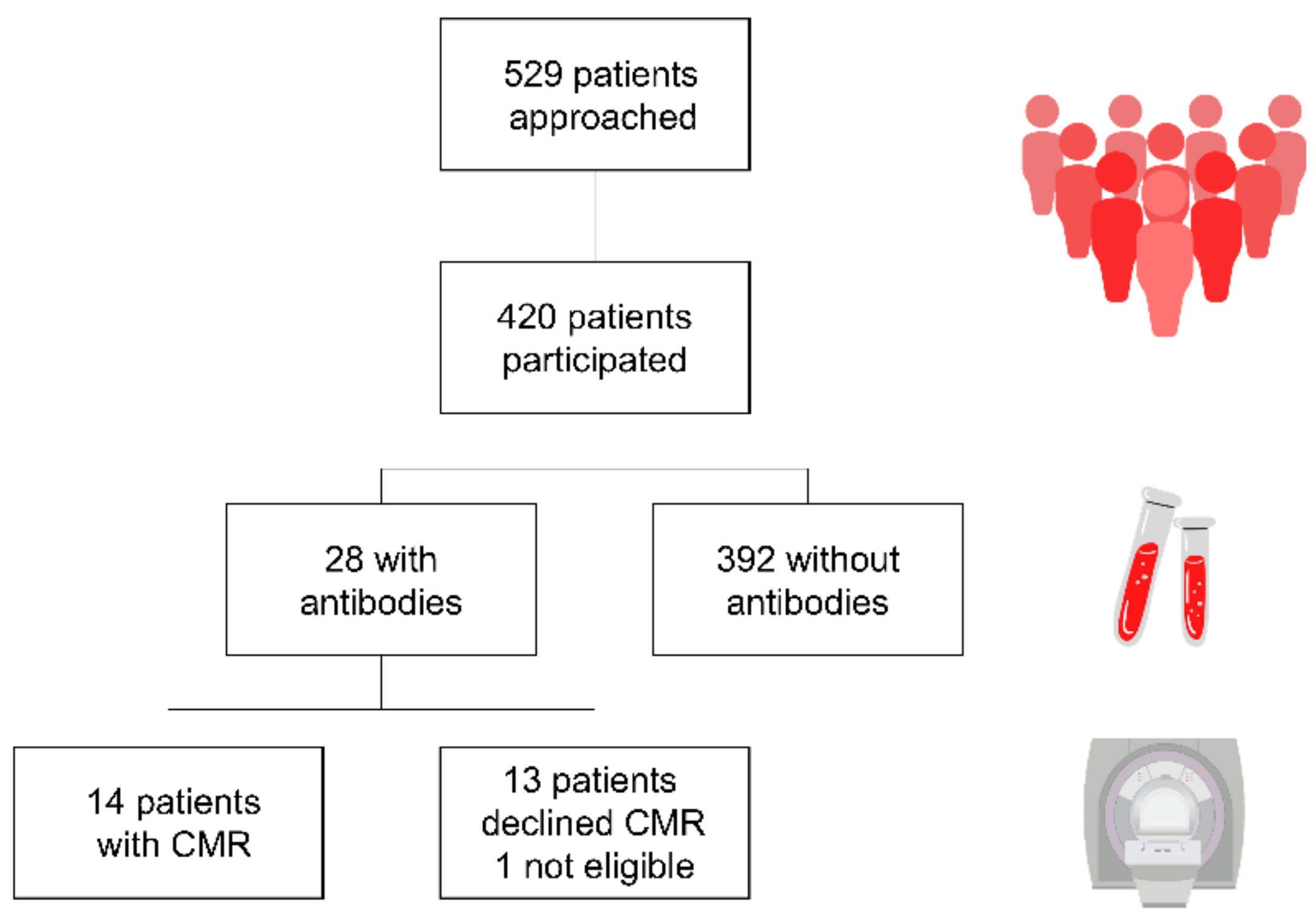
3. Results
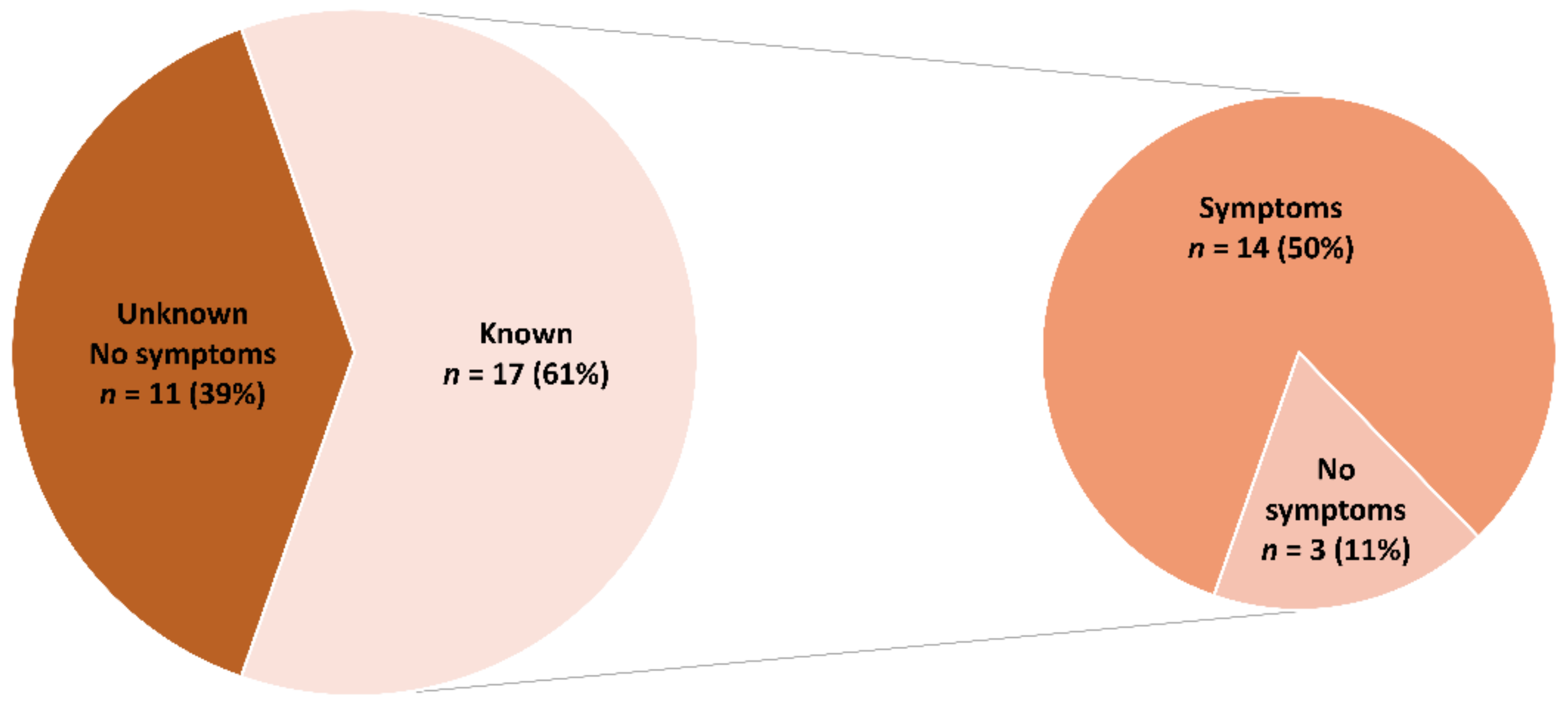
3.1. COVID-19
3.2. Positivity Rate
3.3. Immunization/Vaccination
3.4. Laboratory
3.5. International Physical Activity Questionnaire (IPAQ)
3.6. CMR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Main Congenital Heart Defect | All (n = 420) | COVID-19 Antibodies Neg. (n = 392) | COVID-19 Antibodies Pos. (n = 28) |
|---|---|---|---|
| Atrial septal defect | 31 (7.4) | 30 (7.7) | 1 (3.6) |
| Ventricular septal defect | 38 (9.0) | 34 (8.7) | 4 (14.3) |
| Atrioventricular septal defect | 19 (4.5) | 19 (4.8) | 0 |
| Patent ductus arteriosus | 3 (0.7) | 3 (0.8) | 0 |
| Isolated valve disease excluding PS | 57 (13.6) | 53 (13.5) | 4 (14.3) |
| Pulmonary valve stenosis | 20 (4.8) | 20 (5.1) | 0 |
| Sub- or supravalvular aortic stenosis | 9 (2.1) | 9 (2.3) | 0 |
| Coarctation of the aorta | 43 (10.2) | 41 (10.5) | 2 (7.1) |
| Tetralogy of Fallot | 51 (12.1) | 47 (12.0) | 4 (14.3) |
| Ebstein’s anomaly | 18 (4.3) | 14 (3.6) | 4 (14.3) |
| Transposition of the great arteries | 49 (11.7) | 45 (11.5) | 4 (14.3) |
| Pulmonary atresia | 14 (3.3) | 13 (3.3) | 1 (3.6) |
| Double outlet right ventricle | 14 (3.3) | 13 (3.3) | 1 (3.6) |
| Truncus arteriosus | 3 (0.7) | 3 (0.8) | 0 |
| Anomalous pulmonary venous connection (partial/total) | 6 (1.4) | 6 (1.5) | 0 |
| Single ventricle physiology | 22 (5.2) | 21 (5.4) | 1 (3.6) |
| PAH/Eisenmenger syndrome | 2 (0.5) | 2 (0.5) | 0 |
| Other * | 21 (5.0) | 19 (4.8) | 2 (7.1) |
References
- Warnes, C.A. Adult congenital heart disease: The challenges of a lifetime. Eur. Heart J. 2017, 38, 2041–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marelli, A.J.; Ionescu-Ittu, R.; Mackie, A.S.; Guo, L.; Dendukuri, N.; Kaouache, M. Lifetime Prevalence of Congenital Heart Disease in the General Population From 2000 to 2010. Circulation 2014, 130, 749–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, A.; Thombley, R.; Broberg, C.S.; Harris, I.S.; Foster, E.; Mahadevan, V.S.; John, A.; Vittinghoff, E.; Marcus, G.M.; Dudley, R.A. Age- and Lesion-Related Comorbidity Burden Among US Adults with Congenital Heart Disease: A Population-Based Study. J. Am. Heart Assoc. 2019, 8, e013450. [Google Scholar] [CrossRef]
- Dimopoulos, K.; Diller, G.-P.; Koltsida, E.; Pijuan-Domenech, A.; Papadopoulou, S.A.; Babu-Narayan, S.V.; Salukhe, T.V.; Piepoli, M.F.; Poole-Wilson, P.A.; Best, N.; et al. Prevalence, Predictors, and Prognostic Value of Renal Dysfunction in Adults with Congenital Heart Disease. Circulation 2008, 117, 2320–2328. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Gonzalez, R.; Borgia, F.; Diller, G.-P.; Inuzuka, R.; Kempny, A.; Martinez-Naharro, A.; Tutarel, O.; Marino, P.; Wustmann, K.; Charalambides, M.; et al. Abnormal Lung Function in Adults with Congenital Heart Disease: Prevalence, Relation to Cardiac Anatomy, and Association with Survival. Circulation 2013, 127, 882–890. [Google Scholar] [CrossRef]
- Afilalo, J.; Therrien, J.; Pilote, L.; Ionescu-Ittu, R.; Martucci, G.; Marelli, A.J. Geriatric Congenital Heart Disease: Burden of Disease and Predictors of Mortality. J. Am. Coll. Cardiol. 2011, 58, 1509–1515. [Google Scholar] [CrossRef] [Green Version]
- Tutarel, O.; Kempny, A.; Alonso-Gonzalez, R.; Jabbour, R.; Li, W.; Uebing, A.; Dimopoulos, K.; Swan, L.; Gatzoulis, M.A.; Diller, G.-P. Congenital heart disease beyond the age of 60: Emergence of a new population with high resource utilization, high morbidity, and high mortality. Eur. Heart J. 2014, 35, 725–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, W.; Aboulhosn, J. The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on congenital heart disease. Int. J. Cardiol. 2020, 309, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.-P.; Gatzoulis, M.A.; Broberg, C.S.; Aboulhosn, J.; Brida, M.; Schwerzmann, M.; Chessa, M.; Kovacs, A.H.; Roos-Hesselink, J. Coronavirus disease 2019 in adults with congenital heart disease: A position paper from the ESC working group of adult congenital heart disease, and the International Society for Adult Congenital Heart Disease. Eur. Heart J. 2020, 42, 1858–1865. [Google Scholar] [CrossRef]
- Broberg, C.S.; Kovacs, A.H.; Sadeghi, S.; Rosenbaum, M.S.; Lewis, M.J.; Carazo, M.R.; Rodriguez, F.H., 3rd; Halpern, D.G.; Feinberg, J.; Galilea, F.A.; et al. COVID-19 in Adults with Congenital Heart Disease. J. Am. Coll. Cardiol. 2021, 77, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Schwerzmann, M.; Ruperti-Repilado, F.J.; Baumgartner, H.; Bouma, B.; Bouchardy, J.; Budts, W.; Campens, L.; Chessa, M.; Del Cerro Marin, M.J.; Gabriel, H.; et al. Clinical outcome of COVID-19 in patients with adult congenital heart disease. Heart 2021, 107, 1226–1232. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered from Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Warnes, C.A.; Liberthson, R.; Danielson, G.K.; Dore, A.; Harris, L.; Hoffman, J.I.; Somerville, J.; Williams, R.G.; Webb, G.D. Task Force 1: The changing profile of congenital heart disease in adult life. J. Am. Coll. Cardiol. 2001, 37, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Müller, J.; Amberger, T.; Berg, A.; Goeder, D.; Remmele, J.; Oberhoffer, R.; Ewert, P.; Hager, A. Physical activity in adults with congenital heart disease and associations with functional outcomes. Heart 2017, 103, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Das, S.R.; Addison, D.; Gupta, A.; Jneid, H.; Khan, S.S.; Koromia, G.A.; Kulkarni, P.A.; LaPoint, K.; Lewis, E.F.; et al. 2022 AHA/ACC Key Data Elements and Definitions for Cardiovascular and Noncardiovascular Complications of COVID-19: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e000111. [Google Scholar] [CrossRef]
- Yuan, S.; Oechslin, E. Anatomical complexity does not predict outcomes after COVID-19 in adults with congenital heart disease. Heart 2021, 107, 1193–1195. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.J.; Anderson, B.R.; Fremed, M.; Argenio, M.; Krishnan, U.; Weller, R.; Levasseur, S.; Sommer, R.; Lytrivi, I.D.; Bacha, E.A.; et al. Impact of Coronavirus Disease 2019 (COVID-19) on Patients with Congenital Heart Disease Across the Lifespan: The Experience of an Academic Congenital Heart Disease Center in New York City. J. Am. Heart Assoc. 2020, 9, e017580. [Google Scholar] [CrossRef]
- Gallego, P.; Ruperti-Repilado, F.J.; Schwerzmann, M. Adults with congenital heart disease during the coronavirus disease 2019 (COVID-19) pandemic: Are they at risk? Rev Esp Cardiol Engl. Ed. 2020, 73, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Strah, D.D.; Kowalek, K.A.; Weinberger, K.; Mendelson, J.; Hoyer, A.W.; Klewer, S.E.; Seckeler, M.D. Worse Hospital Outcomes for Children and Adults with COVID-19 and Congenital Heart Disease. Pediatr. Cardiol. 2021, 43, 541–546. [Google Scholar] [CrossRef]
- Anthony, J.M.; Kasargod Prabhakar, C.R.; Clift, P.; Hudsmith, L. UK ACHD response to COVID-19: Which adult patients are being advised to follow shielding by UK centres? Cardiol. Young 2020, 30, 1547–1548. [Google Scholar] [CrossRef] [PubMed]
- Cousino, M.K.; Pasquali, S.K.; Romano, J.C.; Norris, M.D.; Yu, S.; Reichle, G.; Lowery, R.; Viers, S.; Schumacher, K.R. Impact of the COVID-19 pandemic on CHD care and emotional wellbeing. Cardiol. Young 2021, 31, 822–828. [Google Scholar] [CrossRef]
- Frogoudaki, A.A.; Farmakis, D.; Tsounis, D.; Liori, S.; Stamoulis, K.; Ikonomidis, I.; Filippatos, G.; Parissis, J. Telephone based survey in adults with congenital heart disease during COVID-19 pandemic. Cardiol. J. 2020, 27, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.E.; Whitehead, C.A.; Notley, A.S.; Guy, I.A.; Kasargod Prabhakar, C.R.; Clift, P.; Hudsmith, L.E. The impact of the COVID-19 pandemic on application of European Society of Cardiology (ESC) guidelines for exercise in adults with CHD: A data-based questionnaire. Cardiol. Young 2021, 32, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.A.C.; Bluemke, D.A. Cardiac Abnormalities Depicted with MRI in COVID-19: Ongoing Concern for Myocardial Injury. Radiology 2021, 301, E371–E372. [Google Scholar] [CrossRef]
- Zhang, L.; Wei, X.; Wang, H.; Jiang, R.; Tan, Z.; Ouyang, J.; Li, X.; Lei, C.; Liu, H.; Liu, J. Cardiac involvement in patients recovering from Delta Variant of COVID-19: A prospective multi-parametric MRI study. ESC Heart Fail 2022, 2576–2584. [Google Scholar] [CrossRef]
- Seidel, F.; Kuehne, T.; Kelle, S.; Doeblin, P.; Zieschang, V.; Tschoepe, C.; Al-Wakeel-Marquard, N.; Nordmeyer, S. Cardiovascular magnetic resonance findings in non-hospitalized paediatric patients after recovery from COVID-19. ESC Heart Fail. 2021, 8, 5583–5588. [Google Scholar] [CrossRef] [PubMed]
- Modica, G.; Bianco, M.; Sollazzo, F.; Di Murro, E.; Monti, R.; Cammarano, M.; Morra, L.; Nifosì, F.M.; Gervasi, S.F.; Gravina, E.M.; et al. Myocarditis in Athletes Recovering from COVID-19: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4279. [Google Scholar] [CrossRef] [PubMed]


| All, n (%) | COVID-19 Antibodies Neg., n (%) | COVID-19 Antibodies Pos., n (%) | p | |
|---|---|---|---|---|
| N | 420 | 392 | 28 | |
| Mean age in years | 36.4 ± 11.6 | 36.6 ± 11.6 | 33.0 ± 10.0 | 0.103 |
| Female | 188 (44.8) | 174 (44.8) | 14 (50.0) | 0.564 |
| Body mass index (kg/m2) | 27.3 ± 50.7 | 25.0 ± 4.0 | 0.846 | |
| <25 | 236 (56.2) | 220 (59.1) | 16 (57.1) | |
| 25–30 | 120 (28.6) | 112 (28.6) | 8 (28.6) | |
| >30 | 44 (10.5) | 40 (10.2) | 4 (14.3) | |
| missing | 20 (4.8) | 20 (5.1) | 0 | |
| Complexity | 0.822 | |||
| Simple | 96 (22.9) | 91 (23.2) | 5 (17.9) | |
| Moderate | 186 (44.3) | 172 (43.9) | 14 (50.0) | |
| Severe | 117 (27.9) | 110 (28.1) | 7 (25.0) | |
| Miscellaneous | 21 (5.0) | 19 (4.8) | 2 (7.1) | |
| Cyanosis | 22 (5.2) | 20 (5.1) | 2 (7.1) | 0.640 |
| History of arrhythmias | 49 (11.7) | 46 (11.7) | 3 (10.7) | 0.871 |
| Heart rhythm at presentation | ||||
| Sinus rhythm | 371 (88.3) | 344 (87.8) | 27 (96.4) | 0.23 |
| Pacemaker | 34 (8.1) | 33 (8.4) | 1 (3.6) | 0.72 |
| Atrial fibrillation | 2 (0.5) | 2 (0.5) | 0 (0) | 1.00 |
| Other | 3 (0.7) | 3 (0.8) | 0 (0) | 1.00 |
| Not documented | 10 (2.4) | 10 (2.6) | 0 (0) | 1.00 |
| NYHA class | 0.444 | |||
| I | 300 (71.4) | 279 (71.2) | 21 (75.0) | |
| II | 80 (19.0) | 74 (18.9) | 6 (21.4) | |
| III | 21 (5.0) | 21 (5.4) | 0 (0) | |
| Not documented | 19 (4.5) | 18 (4.6) | 1 (3.6) | |
| Vaccination (COVID-19) | 0.358 | |||
| First dose | 66 (15.7) | 62 (15.8) | 4 (14.3) | |
| Second dose | 42 (10.0) | 40 (10.2) | 2 (7.1) | |
| None | 312 (74.3) | 290 (74.0) | 22 (78.6) | |
| Genetic syndrome | 39 (9.3) | 37 (9.2) | 2 (7.1) | 0.686 |
| Comorbidities | ||||
| CVA | 36 (8.6) | 34 (8.7) | 2 (7.1) | 0.780 |
| Arterial hypertension | 52 (12.4) | 49 (12.5) | 3 (10.7) | 0.782 |
| Lung diseases | 41 (9.8) | 39 (9.9) | 2 (7.1) | 0.629 |
| Diabetes | 12 (2.9) | 11 (2.8) | 1 (3.6) | 0.568 |
| Liver diseases | 40 (9.5) | 38 (9.7) | 2 (7.1) | 0.657 |
| Renal diseases | 31 (7.4) | 31 (7.9) | 0 (0) | 0.122 |
| Endocrinologic diseases | 61 (14.5) | 61 (15.6) | 0 (0) | 0.02 |
| Gastrointestinal disorders | 25 (6.0) | 22 (5.6) | 3 (10.7) | 0.270 |
| Rheumatological disorders | 8 (1.9) | 8 (2.0) | 0 (0) | 0.445 |
| COVID-19 Antibodies Neg. (n = 392) | COVID-19 Antibodies Pos. (n = 28) | p | |
|---|---|---|---|
| Haemoglobin, g/dL | 14.7 ± 1.9 | 15.0 ± 2.0 | 0.592 |
| Haematocrit, % | 43.4 ± 6 | 44.0 ± 6 | 0.618 |
| Thrombocytes, /µL | 229,690 ± 57,533 | 222,070 ± 74,510 | 0.316 |
| Leukocytes, /µL | 6594 ± 1867 | 6505 ± 1768 | 0.954 |
| Potassium, mmol/L | 4.0 ± 0.3 | 4.1 ± 0.3 | 0.859 |
| Sodium, mmol/L | 138 ± 2 | 138 ± 2 | 0.509 |
| Creatinine, mg/dL | 0.89 ± 0.36 | 0.86 ± 0.13 | 0.833 |
| GFR, mL/min | 99 ± 22 | 106 ± 17 | 0.169 |
| Troponin T, ng/L | 6.4 ± 4.9 | 5.8 ± 3.7 | 0.574 |
| AST, U/L | 25.4 ± 16.8 | 25.5 ± 11.0 | 0.691 |
| Bilirubin, mg/dL | 0.74 ± 0.60 | 0.86 ± 0.87 | 0.825 |
| CRP, mg/L | 2.3 ± 5.1 | 1.8 ± 1.8 | 0.316 |
| NT-proBNP, ng/L | 265 ± 470 | 171 ± 181 | 0.391 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Langes, N.; Meierhofer, C.; Nagdyman, N.; Maurer, S.J.; Bourier, F.; Halle, M.; Holdenrieder, S.; Ewert, P.; Tutarel, O. COVID-19 Infections in Adults with Congenital Heart Disease—A Prospective Single-Center Study in an Outpatient Setting. J. Clin. Med. 2022, 11, 6105. https://doi.org/10.3390/jcm11206105
Langes N, Meierhofer C, Nagdyman N, Maurer SJ, Bourier F, Halle M, Holdenrieder S, Ewert P, Tutarel O. COVID-19 Infections in Adults with Congenital Heart Disease—A Prospective Single-Center Study in an Outpatient Setting. Journal of Clinical Medicine. 2022; 11(20):6105. https://doi.org/10.3390/jcm11206105
Chicago/Turabian StyleLanges, Nora, Christian Meierhofer, Nicole Nagdyman, Susanne J. Maurer, Felix Bourier, Martin Halle, Stefan Holdenrieder, Peter Ewert, and Oktay Tutarel. 2022. "COVID-19 Infections in Adults with Congenital Heart Disease—A Prospective Single-Center Study in an Outpatient Setting" Journal of Clinical Medicine 11, no. 20: 6105. https://doi.org/10.3390/jcm11206105
APA StyleLanges, N., Meierhofer, C., Nagdyman, N., Maurer, S. J., Bourier, F., Halle, M., Holdenrieder, S., Ewert, P., & Tutarel, O. (2022). COVID-19 Infections in Adults with Congenital Heart Disease—A Prospective Single-Center Study in an Outpatient Setting. Journal of Clinical Medicine, 11(20), 6105. https://doi.org/10.3390/jcm11206105