


A Systematic Review of Treatments of Post-Concussion Symptoms
 , , ,
, , ,
Abstract
:1. Introduction
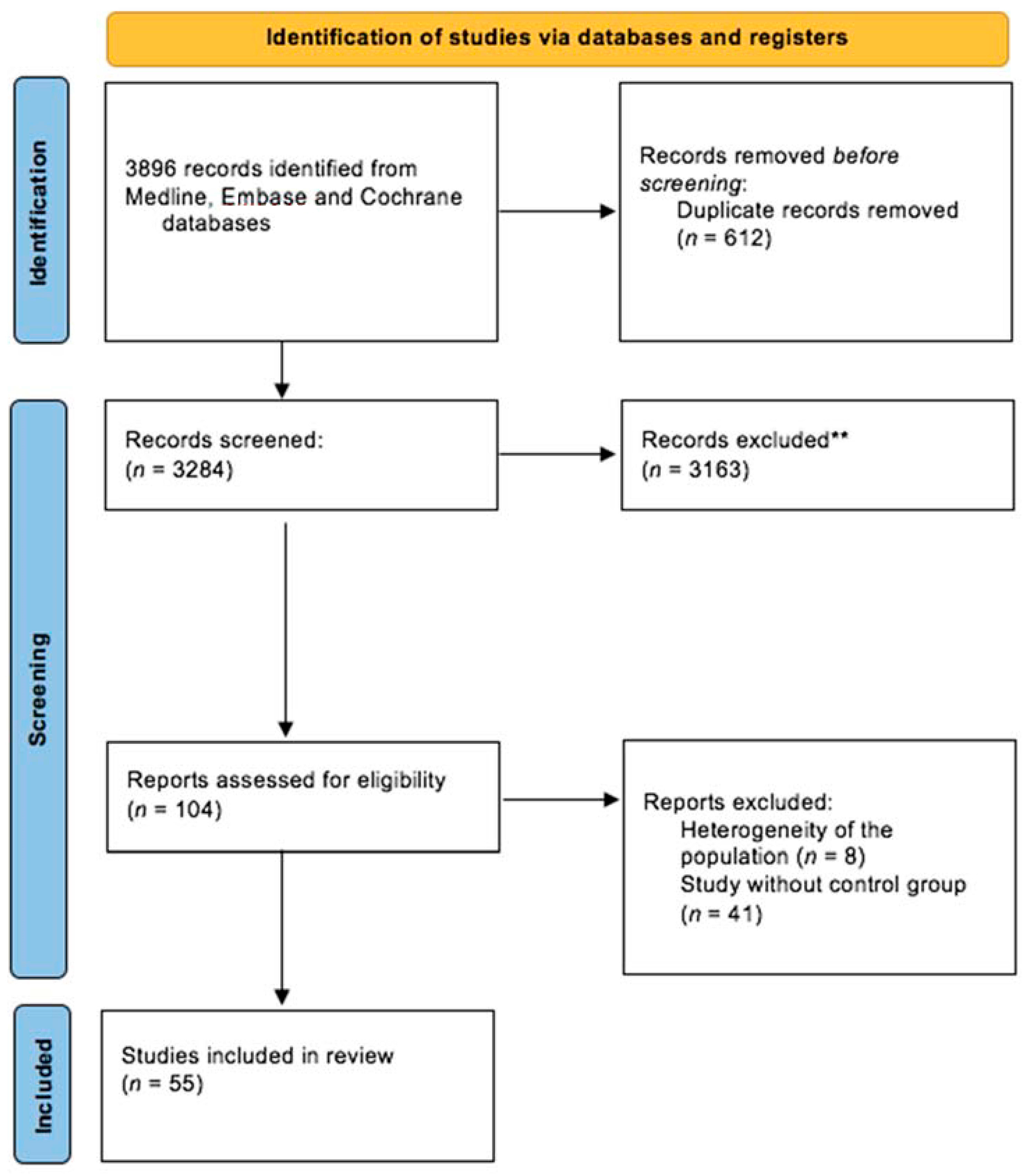
2. Materials and Methods
3. Results
3.1. Treatments Focusing on Cognitive Symptoms and the Reduction of PCS in General
3.1.1. Cognitive Training Programs and Psycho-Education
3.1.2. Pharmacological Treatments
3.1.3. Non-Invasive Brain Stimulation
3.1.4. Hyperbaric Oxygen Therapy
3.1.5. Technology-Assisted Cognitive Rehabilitation
3.1.6. Other Rehabilitation Techniques
3.2. Treatments Focusing on PTSD, Mood, and Sleep Disorders
3.3. Treatment Focusing on Somatic Complaints and Fatigue
3.3.1. Balance Disorders
3.3.2. Headache and Migraine
3.3.3. Oculomotor Disorders
3.3.4. Post-Injury Fatigue
3.4. Early Interventions
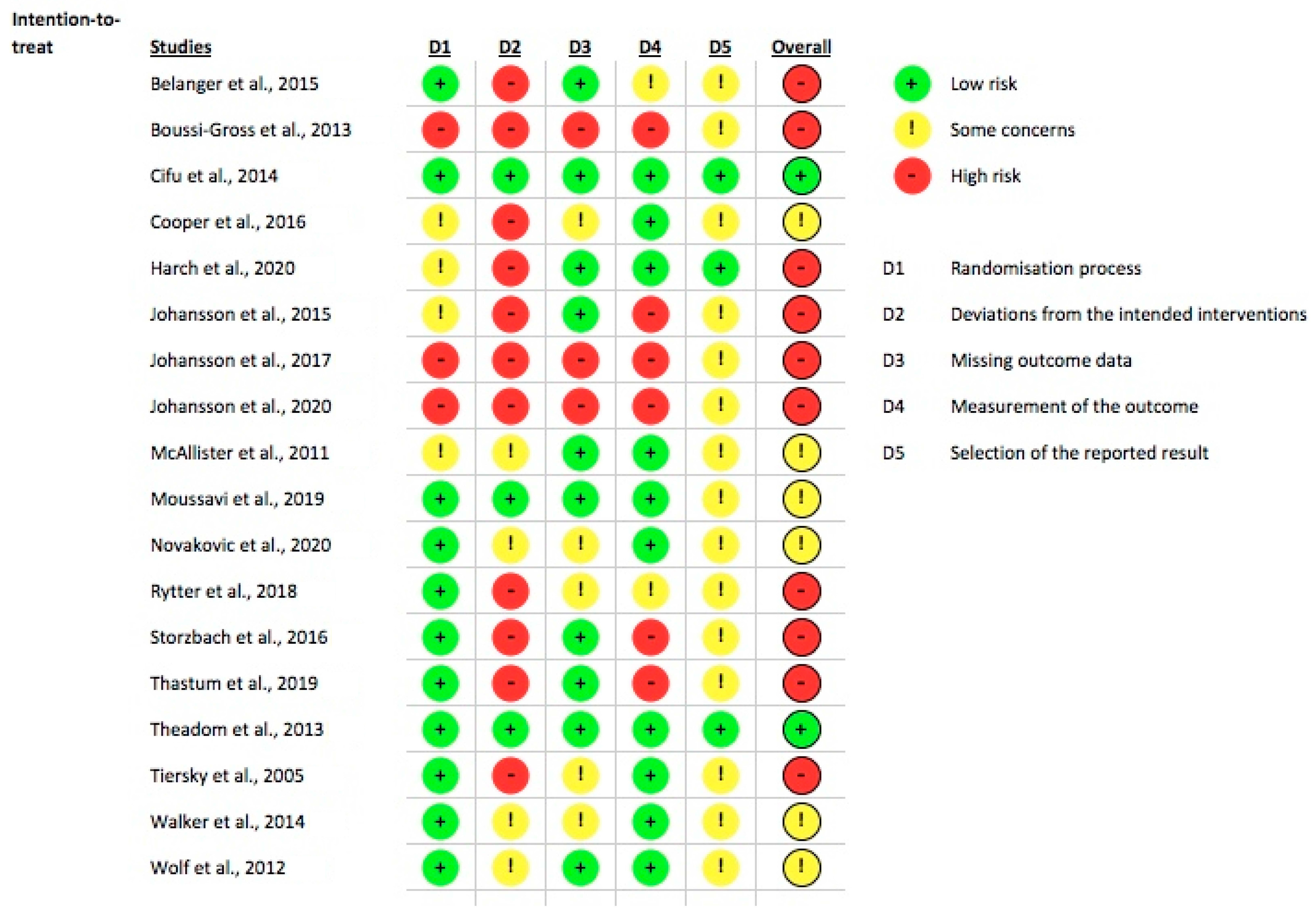
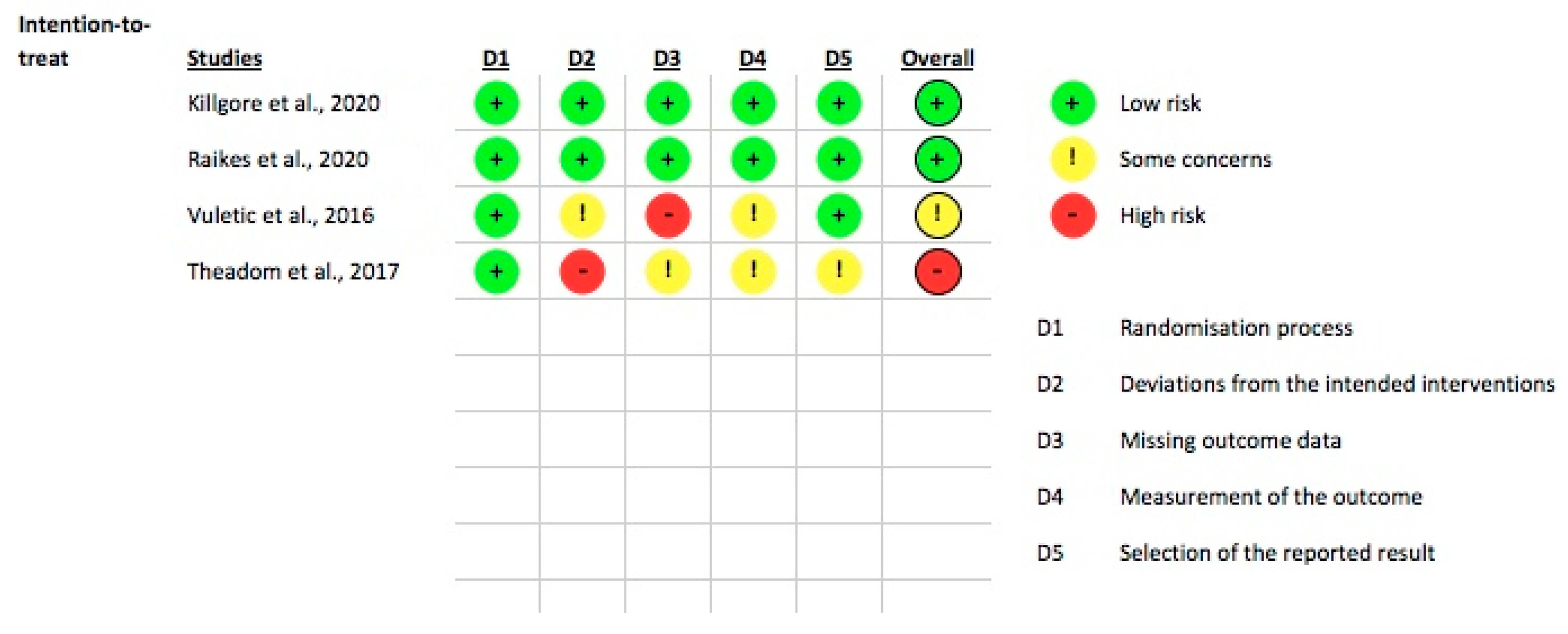
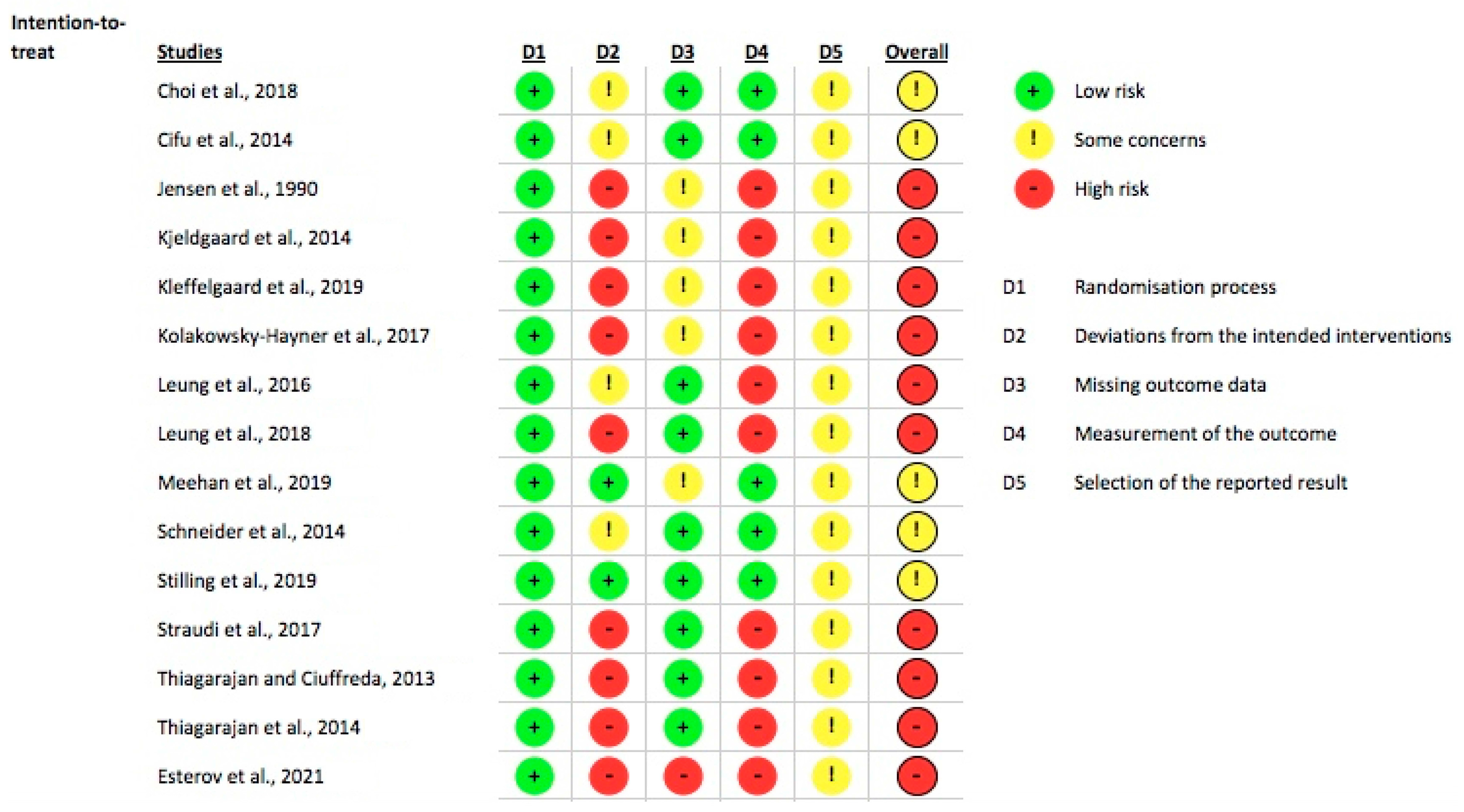
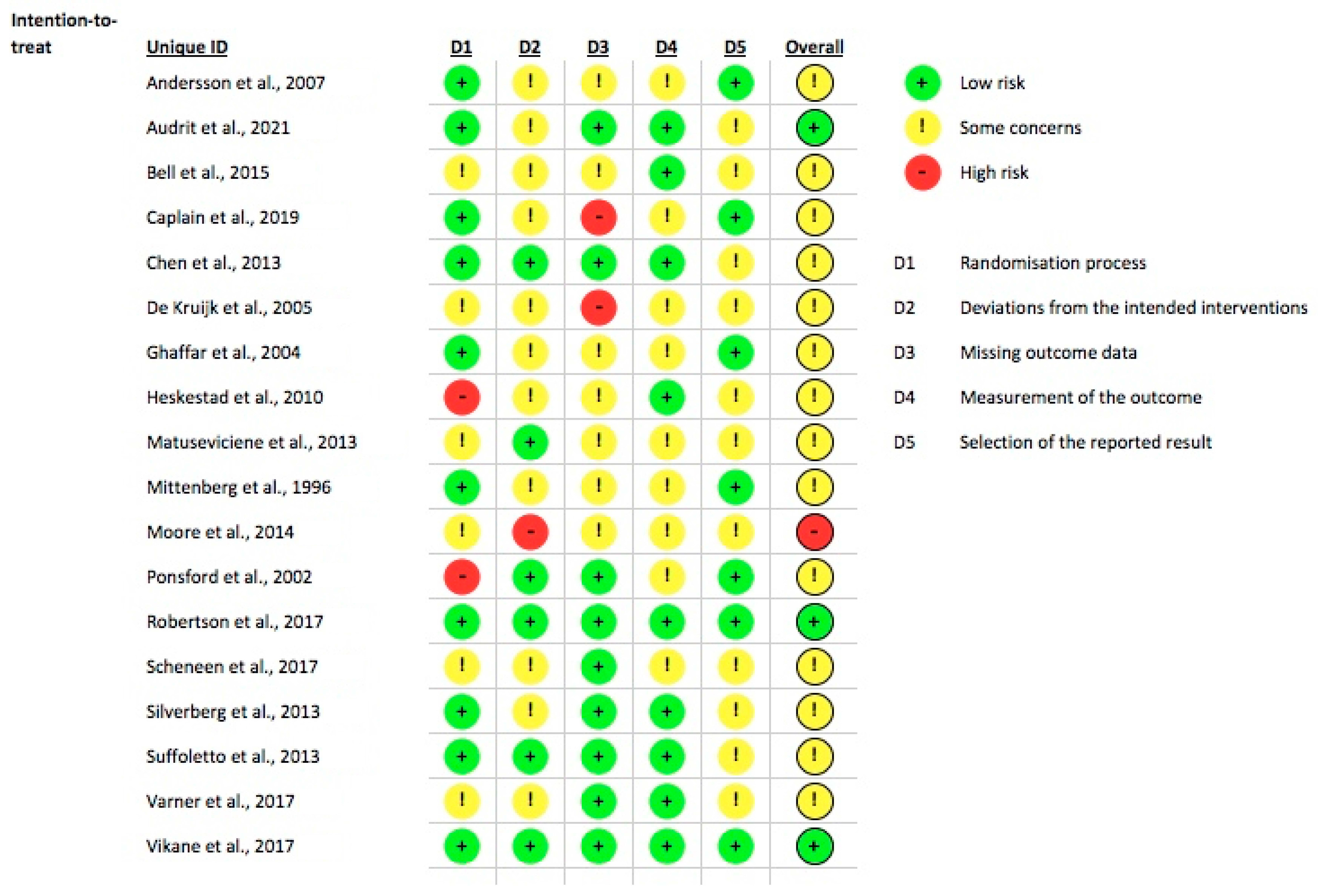
3.5. Risk of Bias Assessment
4. Discussion
4.1. Treatment of Cognitive Symptoms and Reduction of PCS in General
4.2. Treatment of PTSD, Mood, and Sleep Disorders
4.3. Treatment of Somatic Complaints, Headaches, and Fatigue
4.4. Early Interventions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

| First Author, Year of Publication | Study Design | Age (Mean) and Gender of the Participants | Etiology of mTBI | Delay between mTBI and Inclusion | Main Aim | Number of Participants | Outcomes and Tools | Results | + If Main Result Is Significant, − If Not | Incog Recommendation Level |
|---|---|---|---|---|---|---|---|---|---|---|
| Belanger et al., 2015 [36] | RCT | 18–25 y.o. = 14.6% 26–35 y.o. = 39.9% 36–45 y.o. = 36.7% 46–55 y.o. = 8.9% 75% male | Not described | <2 years (37% <1 month, 31.5% = 1 month–1 year, 31.5% > 1 year | To investigate the effectiveness of a web-based educational intervention for reducing post-concussion symptoms. | 158 | -Cognition: Neurobehavioral Symptom Inventory, Brief-Symptom Inventory-18, Self Efficacy for Symptom Management Scale -PTSD: PTSD Checklist Civilian Version -Other: Questionnaire about basic knowledge of mTBI | No effect of the intervention on symptom severity or attributions. Subgroup analyses suggested the benefit of web-based intervention in those receiving concurrent mental health treatment and in those participants with the greatest time since injury (>1 year after mTBI). | - | A |
| Boussi-Gross et al., 2013 [32] | Cross-over | 44 y.o. 57% female | Vehicle accident = 38; falls = 7; object hit = 6; pedestrian accident = 3; assault = 2 | 1–5 years | To test the effectiveness of Hyperbaric Oxygen Therapy (HBOT) in improving brain Function and quality of life in mTBI patients suffering from chronic neurocognitive impairments. | 56 | -Cognition: Information Processing Speed index, attention-related index, memory-related index, executive functions index, Mindstreams battery -Quality of life: EQ-5D -Brain imaging: SPECT | Significant improvements were demonstrated in cognitive function and quality of life in both groups following HBOT. | + | A |
| Cifu et al., 2014 [34] | RCT | 23.2 y.o. 100% male | Military | 3 months–3 years | To evaluate the effects of hyperbaric oxygen therapy (HBOT) on persistent post-concussion symptoms. | 60 | -PCS: RPCSQ -PTSD: Post-traumatic Disorder Checklist-Military version | No effect on post-concussion symptoms after mTBI when compared with a control treatment. | - | A |
| Cooper et al., 2016 [24] | RCT | 31 y.o. 93% male | Military | 3–24 months | To compare different cognitive rehabilitation (CR) interventions (psycho-education, computer-based CR, therapist-directed manualized CR, and integrated therapist-directed CR combined with cognitive-behavioral psychotherapy) for mTBI. | 126 | -Cognition: PASAT -Mood: Symptom Checklist–90 Revised -Other: Key Behaviors Change Inventory | Equivalent improvement on the primary outcome (Paced Auditory Serial Addition Test). Improvements in primary outcome measures during treatment were maintained at follow-up with no differences among arms. | - | A |
| Harch et al., 2020 [31] | Single-blinded Cross-over | 42 y.o. 56% female | 21% Military | >6 months | To assess whether 40 150 kPa HBOT could improve cognitive symptoms of PCS after mTBI. | 63 | -Behavior: Neurobehavioral Symptom Inventory -Substance abuse: Michigan Alcohol Screening Test, Drug Abuse Screening Test -PTSD: Post-Traumatic Stress Disorder Check List-Military or Civilian, Post-Traumatic Stress Disorder Check List-Military or Civilian -Mood: Hamilton Anxiety Scale (HAM-A) -Cognition: Test of Memory Malingering, Green Word Memory Test, Wechsler Test of Adult Reading, Wechsler Adult Intelligence Scale or Wechsler Abbreviated Scale of Intelligence, Wechsler Memory Scale, Rey Auditory Verbal Learning Test Delayed Recall, Benton Visual Retention Test, Stroop Test, Controlled Oral Word Association Test, Category Fluency Test (Animals Test), and Automated Neuropsychological Assessment Metrics -Sleep: Pittsburgh Sleep Quality Index -Quality of life: QOLIBRI | HBOT participants improved significantly in the Neurobehavioral Symptom Inventory, Memory Index, Automated Neuropsychological Assessment Metrics, Hamilton Depression Scale, Hamilton Anxiety Scale, Post-Traumatic Stress Disorder Checklist, Pittsburgh Sleep Quality Index, and Quality of Life after Brain Injury compared to the control group, with the persistence of the improvement at 2 months. | + | A |
| Johansson et al., 2015 [25] | RCT | 41 y.o. 59% female | Not described | >6 months | To assess the effect of Methylphenidate in two different dosages on mental fatigue, pain, and cognition. | 51 (4 with moderate TBI) | -Cognition: Digit Symbol Coding from the WAIS-III; Digit Span; the Trail Making Test A and B | Significant effect on fatigue and processing speed (but not on pain) with a dose-dependent effect. | + | A |
| Johansson et al., 2017 [26] | Follow-up study of RCT | 39.7 y.o. 60% female | Not described | >6 months | Thirty participants who had reported positive effects with methylphenidate during the initial phase of this follow-up study were treated with methylphenidate for a further six months. | 30 (2 moderate TBI) | -Fatigue: Mental Fatigue Scale -Pain: VAS - Depression and anxiety: Comprehensive Psychopathological Rating Scale -Cognition: Digit Symbol Coding, Digit Span, TMT parts A and B | After a six-month follow-up, the effects of determined by the Mental Fatigue Scale, depression, anxiety, and cognitive function (processing speed, attention, working memory), were significantly improved compared to the baseline. | + | B |
| Johansson et al., 2020 [27] | 5.5-year follow-up study of RCT | 46 y.o. 59% female | Not described | >5 year | To assess the long-term effect of Methylphenidate. A comparison was made between those who had continued and those who had discontinued the treatment. The effect was also evaluated after a four-week treatment break. | 17 | -Fatigue: Mental Fatigue Scale -Pain: VAS - Depression and anxiety: Comprehensive Psychopathological Rating Scale -Cognition: Digit Symbol Coding, Digit Span, TMT parts A and B | Significant improvement in mental fatigue, depression, anxiety, and processing speed as compared to patients who discontinued treatment. Withdrawal produced significant deterioration in mental fatigue, depression, and anxiety, and a slower processing speed. | + | B |
| McAllister et al., 2011 [28] | Placebo-controlled double-blind RCT | 27.2 y.o. 46% female | Falls or motor vehicle accidents | >1 month | To assess improvement of working memory by administration of an alpha-2 adrenergic agonist 1 month after injury. | 13 | -Cognition: N-back task in fMRI, WRAT-3, Reading subtest; WAIS-III, Block Design subtest; verbal memory (California Verbal Learning Test or California Verbal Learning Test-II; psychomotor speed (WAIS-III, Digit Symbol-Coding subtest; WM, executive, and attentional functioning (Trail Making Test, Parts A and B or Delis–Kaplan Executive Function System, Trail Making Test Conditions 2 and 4, D-KEFS Color-Word Interference Test, Controlled Oral Word Association Test, Paced Auditory Serial Addition Test, and Gordon Continuous Performance Test | Alterations in working memory after mTBI may be improved with the alpha-2 agonist. | + | B |
| Moussavi et al., 2019 [30] | Placebo-controlled double-blind RCT | 49.5 y.o. 50% female | Falls, sports, and car accidents | >4.5 months | To assess if 4 sessions of 10 Hz rTMS applied on the dorso-lateral pre-frontal cortex could reduce post-concussion syndrome (assessed using the Rivermead Post Concussion Symptoms Questionnaire) after mTBI compared to sham stimulation. | 22 | -PCS: RPCSQ -Depression: Montgomery–Åsberg Depression Rating Scale -Electrovestibulography recording | Participants who had a more recent injury (<one year) and who received active rTMS showed significant improvements compared to those who received sham and to those with a longer duration of injury (>14 months) who received active rTMS. | + | A |
| Novakovic et al., 2020 [23] | Single-blinded controlled RCT | 45.3 y.o. 12% female | military | >6 months | To assess the efficacy of cognitive rehabilitation of executive functions using Goaloriented attention self-regulation training (GOALS) in veterans with mTBI and PTSD. | 40 | -Cognition: Auditory Consonant Trigrams, the Letter Number Sequencing subtest from the Wechsler Adult Intelligence Scale, Third Edition, Color-Word Interference Test Inhibition task from the Delis-Kaplan Executive Function System, Trail Making Test-Part B, Design Fluency-Switching, Verbal Fluency Switching Total Correct (DKEFS), Color-Word Interference Test Inhibition- Switching (DKEFS), Digit Vigilance Test, Hopkins Verbal Learning Test—Revised, Brief Visual Memory Test—Revised, Goal Processing Scale -Daily and emotional functioning: Mayo-Portland Adaptability Inventory, Goal Processing Questionnaire -Psychology: Profile of Mood States, Beck Depression Inventory-II, PTSD Checklist, Military Version | Participants of the group benefiting from the GOALS rehabilitation improved a composite score of neuropsychological tests assessing executive and attentional functions. | + | A |
| Rytter et al., 2018 [19] | Controlled RCT | 18–29 y.o. = 26.7% 30–43 y.o. = 46.7% >44 y.o. = 26.7% 64% female | Fall = 47%; sports accidents = 33% | >6 months | RCT to compare the effectiveness of a specialized, interdisciplinary rehabilitation (S-REHAB) with standard care (STAND) for people with persistent post-concussive symptoms | 89 | -PCS: RPCSQ -Headache: Headache Impact Test -Depression: Major Depression Inventory -Fatigue: Multidimensional Fatigue Inventory-20 -Quality of life: SF-36 | Significant reduction in symptoms measured by the Rivermead Post-Concussion Symptoms Questionnaire compared to the STAND immediately post-treatment and at 6 months of follow-up. | + | A |
| Storzbach et al., 2016 [20] | RCT | 35 y.o. 6% female | Military | Not indicated | To evaluate the efficacy of group-based Compensatory Cognitive Training (120 min group sessions per week, 10 weeks) in veterans with mTBI compared to usual care. | 119 | -Questionnaires: Prospective-Retrospective Memory Questionnaire, Multiple Sclerosis Neuropsychological Screening Questionnaire—Patient Version, Memory Compensation Questionnaire, Portland Cognitive Strategies Scale 2.0, Neurobehavioral Symptom Inventory, the Wide Range Achievement Test- Reading subtest –Cognition: Hopkins Verbal Memory Test—Revised, Wechsler Adult Intelligence Scale—4th Edition, Digit Span Subtest and Digit Symbol Subtest (WAIS-IV), Delis-Kaplan Executive Function System, Trails Sub-test and Verbal Fluency Subtest -PTSD: PTSD Checklist—Military Version -Depression: Beck Depression Inventory, Second Edition -Quality of Life: Satisfaction with Life Scale -Adaptive Functioning: University of California San Diego (UCSD) Performance-Based Skills Assessment, Brief Version | Training in compensatory cognitive strategies facilitates behavioral change (use of cognitive strategies) as well as both subjective and objective improvements in targeted cognitive domains. | + | A |
| Thastum et al., 2019 [22] | Unmasked RCT | 22.9 y.o. 79% female | Traffic accidents = 32%; falls = 26%; sport = 21% | 2–6 months | To test an interdisciplinary, individually tailored intervention of 8 weeks duration based on a gradual return to activities and principles from cognitive behavioral therapy (GAIN). | 112 | -PCS: RPCSQ -2 subscales from The Behavioral Responses to Illness Questionnaire -Quality of life: The Quality of life after Brain Injury–Overall scale, SF-36 -Psychology: Symptom Checklist-90-Revised, 10-item Perceived Stress Scale -Executive functions: Behavior Rating Inventory of Executive Function–Adult version -Patient Global Impression of Change | Patients treated with GAIN plus enhanced usual care reported a significantly larger reduction in PCS than patients receiving enhanced usual care alone.at 3-month follow-up. | + | A |
| Theadom et al., 2013 [29] | Double-blind placebo-controlled Phase II RCT | 44 y.o. 57% female | Motor vehicle accidents = 33.3%; falls = 33.3%; sports-related injury = 10.0% | 3–12 months | To investigate the safety, compliance, and efficacy of Enzogenol (pine extract) for improving cognitive functioning in people 3–12 months following mild TBI. | 62 | -safety and tolerability -Cognition: CFQ, digit span subtest of the Wechsler Adult Intelligence Scale Version 3, Arithmetic WAIS Version 4, Letter Number Sequencing sub-tests of the WAIS Version 4, California Verbal Learning Test -PCS: RPCSQ -Anxiety and mood: HADS | Administration of Enzogenol during 6 weeks is well-tolerated and may reduce self-perceived cognitive failures in patients 3–12 months post-mild TBI. | + | B |
| Tiersky et al., 2005 [21] | Single-blind randomized, wait-listed controlled trial, with repeated measures and multiple baselines. | 47 y.o. 55% female | Motor-vehicle accidents = 65%; falling objects = 15%; falls = 10%, sports-related accidents = 5% | 1–20 years (mean 6.25 y) | To test the effect of a neuropsychologic rehabilitation program, including psychotherapy and cognitive remediation. Treated patients received both individual cognitive-behavioral psychotherapy and cognitive remediation 3 times a week for 11 weeks. | 20 (including 2 with moderate TBI) | -Cognition: Paced Auditory Serial Addition Task, Rey Auditory Verbal Learning Test, ACFI, the Attention Questionnaire. -Psychosocial and affective functioning: Coping Response Inventory and SCL- 90R. -Community participation: Community Integration Questionnaire. | Significant reduction in anxiety and depression and improvement in divided attention at 1 and 3 months follow-up. However, no significant improvement in community integration scores. | + | A |
| Walker et al., 2014 [33] | Sham-controlled double-blind RCT | 23.2 y.o. 0% female | Military | 3–36 months | To assess the effect of HBOT on persistent post-concussion symptoms. | 60 | -Cognition: D-KEFS letter fluency, Trail Making Test part B, Stroop Color-Word, CPT-II detectability, PASAT, WAIS-III Working Memory Index, CVLT, Benton Visual Memory Test | No immediate post-intervention beneficial effect of exposure to hyperbaric oxygen. | - | B |
| Wolf et al., 2012 [80] | Sham-controlled RCT | 28.3 y.o. 4% female | Military | 3–71 months | To evaluate the effect of HBOT on post-concussive symptoms after mild TBI. | 50 | -Cognition: ImPACT Immediate Post-Concussion Assessment and Cognitive Testing -PTSD: PCL-M | No significant differences in cognitive disabilities (on PCL-M composite score nor on the ImPACT total score). | - | A |
| First Author, Year of Publication | Study Design | Age (Mean ± Standard Deviation) and Gender | Etiology of mTBI | Delay between mTBI and Inclusion | Main Aim | Number of Participants | Outcomes and Tools | Results | + If Main Result Is Significant, − If Not | Incog Recommendation Level |
|---|---|---|---|---|---|---|---|---|---|---|
| Killgore et al., 2020 [39] | Double-blind RCT | 23 y.o. 53% female | Not described | 1–18 months (mean 6 months) | To evaluate the effect of blue-wavelength light on cognitive functions at 1–18 months from mTBI. | 32 | -Sleep: duration, circadian phase shift, subjective and objective sleepiness -Cognition: psychomotor vigilance test, RBANS (battery) -Functional Connectivity -White matter axonal integrity. Each of these was assessed at the baseline week or visit and again during the final week or follow-up visit. | Participants of the experimental group significantly improved phase-advanced sleep timing, reduced daytime sleepiness, and improved their processing speed during the Tower of London task compared to the control group (Amber light) but not their results at a brief neurocognitive performance battery (RBANS). | + | A |
| Raikes et al., 2020 [40] | Placebo-and double-blind controlled RCT | 26 y.o. 63% | Motor vehicle accident = 50% | <18 months | To assess the effect of 30 min morning blue light therapy during 6 weeks on sleep in mTBI participants at 1–18 months from TBI. | 35 | -Sleep: Epworth Sleepiness Scale, Pittsburgh Sleep Quality Index, Functional Outcome of Sleep Questionnaire, daily sleep onsets and offsets, total time in bed, total nighttime sleep time, sleep efficiency and normalized wake after sleep onset -Depression: Beck Depression Inventory-II -PCS: RPCSQ | The authors found lower Epworth Sleepiness Scale, Beck Depression Inventory-II, Rivermead Post-Concussion Symptom Questionnaire chronic, and somatic symptoms in the experimental group. These participants had greater total sleep time and better scores on sleep questionnaires. | + | A |
| Theadom et al., 2017 [38] | RCT (pilot study) | 35.9 y.o. 63% female | Motor vehicle accident = 50%; hit by object = 21%; other = 29% | 3–36 months | To explore the feasibility and potential efficacy of online interventions for sleep quality following mTBI. | 24 (1 moderate TBI in each group) | -Sleep: Pittsburgh Sleep Quality Index, record of time taken to fall asleep, sleep efficiency, time spent awake after sleep onset, and number of awakenings -PCS: RPCSQ -Cognition: CNS Vital Signs online neuropsychological assessment -Quality of life: Quality of Life after Brain Injury questionnaire | Significant reductions in sleep disturbance in comparison to controls post-intervention. There were no significant group differences in objective sleep quality, cognitive functioning, post-concussion symptoms, or quality of life. | - | B |
| Vuletic et al., 2016 [37] | Single-blind RCT | 29.3 y.o. 6% female | Military | <2 years | Randomized trial to evaluate the effect of telephone-based problem-solving treatment (PST) on sleep quality in active duty post-deployment service members with mild traumatic brain injury. | 356 | -Sleep: Pittsburgh Sleep Quality Index -PCS: RPCSQ -Psychological symptoms: Behavioral Symptoms Inventory-18, PHQ-9 -PTSD: PTSD Checklist-Military Version -Pain: EQOL4, EQOL4 -Symptoms’ impact: SF-12, Sheehan Disability Scale | PST significantly improved sleep quality at 6 months but not at 12 months. | - | A |
| First Author, Year of Publication | Study Design | Age (Mean ± Standard Deviation) and Gender | Etiology of mTBI | Delay between mTBI and Inclusion | Main Aim | Number of Participants | Outcomes and Tools | Main Result | + If Main Result Is Significant, − If Not | Incog Recommendation Level |
|---|---|---|---|---|---|---|---|---|---|---|
| Choi et al., 2018 [48] | Randomized controlled feasibility study | 42.6 y.o. 50% female | Not described | Chronic (mean 15.7 months) | To assess if 10 sessions of 10 Hz rTMS applied on the primary motor cortex of the affected hemisphere could reduce central pain after mTBI (assessed using a numerical rating scale NRS) compared to sham stimulation. | 12 | -Pain: NRS -Quality of life: SF-36 (Physical and Mental Component Scores) | The NRS score was significantly lower in the experimental group with rTMS than in the control group immediately after treatment, at one, two, and four weeks. | + | B |
| Cifu et al., 2014 [35] | Sham-controlled blinded RCT | 23.3 y.o. 0% female | Military | 3 months–3 years | To evaluate the effects of hyperbaric oxygen on eye-tracking abnormalities in males after mTBI. | 60 | Eye-tracking analyses | No effect on post-concussive eye movement abnormalities after mTBI when compared with a sham-control. | - | A |
| Esterov et al., 2021 [51] | RCT | 44 y.o. 65% female | Motor vehicle accidents = 70%; falls = 20%; sports = 10% | 3–88 months | To assess the effect of osteopathic manipulative treatment on headaches after mTBI. | 26 | -Pain: headache scores on a Visual Analog Scale (VAS) and scores on the six-item Headache Impact Test (HIT-6) | Significant improvement of the VAS in the intervention group but not in the HIT-6. | + | B |
| Jensen et al., 1990 [50] | RCT | 31 y.o. 63% female | Not described | 9–12 months post-injury | To test if manual therapy (two sessions) on the neck could reduce post-traumatic headaches. The control group was treated with cold packs on the neck. | 23 | -Pain: VAS, use of analgesics -Frequency of associated symptoms -Neck motion | Significant reduction of the pain index in the treatment group two weeks after the end of treatment, but this effect was no more statistically significant five weeks later. | - | B |
| Kjeldgaard et al., 2014 [49] | RCT | 34 y.o. gender not described | Traffic accident = 45% | Mean time since injury: 27 months | To evaluate the effect of a group-based Cognitive Behavioral Therapy (CBT) intervention in relation to headache, pain perception, psychological symptoms, and quality of life in patients with CPTH. | 90 | -Headache: diary -PCS: Rivermead Post Concussion Symptoms Questionnaire -Quality of life: SF-36 -Psychology: SCL-90-R | A nine-week CBT had no effect on headache and pressure pain thresholds in comparison to a waiting list group. | - | A |
| Kleffelgaard et al., 2019 [41] | Blinded RCT | 39 y.o. 70% female | Traffic accidents = 23%; falls = 9%; violence = 64%; sport = 9% | Mean 3.5 months | To investigate the effects of 8 weeks of group-based vestibular rehabilitation in patients with dizziness after mild traumatic brain injury. | 65 | -Dizziness-related disability: Dizziness Handicap Inventory, Vertigo Symptom Scale-Short Form -Mobility: High-Level Mobility Assessment Tool for TBI -PCS: RPCSQ -Psychology: HADS -Balance: Balance Error Scoring System | Statistically significant mean differences in Dizziness Handicap Inventory at 2.2 ± 0.8 months compared to control. No significant difference 2 months after the end of rehabilitation. | + | A |
| Kolakowsky-Hayner et al., 2017 [55] | Single-blinded crossover | 42.7 y.o. 61% female | Vehicular trauma = 53.7%; violence = 6.5%; sports = 8.1%; fall/hit = 12.2%; pedestrian = 8.9% | At least 6 months after TBI | To evaluate the impact of a graduated physical activity program on fatigue after TBI. | 123 | -Fatigue: Global Fatigue Index, Barrow Neurological Institute Fatigue Scale Overall Severity Index Score, Multidimensional Fatigue Inventory | Less reported fatigue at the end of the intervention (24 weeks) and after a washout period (36 weeks). | + | B |
| Leung et al., 2016 [45] | RCT | 41 y.o. 12.5% female | Military | Chronic (33–580 months) | A sham-controlled randomized study to assess the effect of repetitive transcranial magnetic stimulation (rTMS, 10 Hz, 2000 pulses, 20 trains, one-sec inter-train interval) at the left motor cortex) in reducing mTBI-related headaches. | 24 | -Headache: diary -Cognition: Conner’s Continuous Performance Test -Mood: Hamilton Rating Scale for Depression -PTSD: Mississippi scale for PTSD -Global Pain: Brief Pain Inventory | There was a significant reduction in persistent headache intensity and debilitating headache exacerbation in the real treatment group at 1 and 4 weeks post-treatment. | + | B |
| Leung et al., 2018 [46] | RCT | 34.1 y.o. 21% female | Military | 21–367 months | To assess if 4 sessions of 10 Hz rTMS applied on the left prefrontal cortex could reduce headaches after mTBI (assessed using a diary) compared to sham stimulation. | 44 | -Headache: diary (sum of headache NRS score or sum of the duration of the HA/number of days) -Cognition: Conner’s Continuous Performance Test, the Wechsler Adult Intelligence Scale (WAIS-IV), Hopkins Verbal Learning Test, Stroop Test, -Mood: Hamilton Rating Scale for Depression -Global pain: Brief Pain Inventory –PTSD: Clinician-Administered PTSD Scale (CAPS) | The group benefiting from rTMS showed a significant decrease in the average NRS at 1 and 4 weeks and a significant decrease in the prevalence of persistent headaches at 1 and 4 weeks. The experimental group showed a significant improvement in the Hamilton Rating Scale for Depression score at 1-week. | + | A |
| Meehan et al., 2019 [44] | Sham-controlled double-blind RCT | 32.8 y.o. 1% female | Military | 3 months–5 years | To describe the effect of HBO2 sessions during 3 months on balance function in military service members. | 71 | -Balance: NeuroCom Computerized Dynamic Posturography, Cervical Vestibular Evoked Myogenic Potential, Ocular Vestibular Evoked Myogenic Potential, tandem gait, Romberg, Sharpened Romberg, Berg Balance Scale -Anxiety and Mood: Beck Anxiety Inventory, Center for Epidemiologic Study–Depression Scale -PTSD: PTSD Checklist-Civilian Version, Structured Clinical Interview for the DSM-IV, PTSD Module | Minimal significant trend on balance after HBO2. Those with affective symptoms had the most improvement in postural control and otolith function. | - | A |
| Schneider et al., 2014 [43] | Single-blinded RCT | 15 y.o. 42% female | Sport | 8–276 days (average: 53 and 47 days in the treatment and control group, respectively) | To determine if a combination of vestibular rehabilitation and cervical spine physiotherapy decreased the time until medical clearance in individuals with prolonged PCS (weekly sessions for 8 weeks) | 31 | -Number of days from treatment initiation until medical clearance to return to sport -Pain: 11-point Numeric Pain Rating Scale score -Balance: Activities-specific Balance Confidence Scale, Functional Gait Assessment -Dizziness; Dizziness Handicap Index, Other: SCAT2 Dynamic Visual Acuity, Head Thrust Test, Modified Motion Sensitivity Test, Cervical Flexor Endurance and Joint Position Error test | Treated patients showed a decreased time to medical clearance to return to sport within 8 weeks compared to the control group receiving conventional physiotherapy | + | A |
| Stilling et al., 2019 [47] | RCT | 36.0 y.o. 90% female | Vehicle accidents = 47%; sports = 32%; falls = 11%; other = 11% | 3 months–5 years | To assess the effect of 10 sessions of rTMS (10 Hz, 600 pulses, 70% resting motor threshold amplitude, on the left dorsolateral prefrontal cortex) on headaches at 1 month in participants with mTBI and persistent post-traumatic headaches. | 20 | -Headache: diary, headache impact test–6 -PCS: RPCSQ, British Columbia post-concussion symptom inventory (BC-PSI) -Cognition: Montreal cognitive assessment -Quality of life: quality of life after brain injury questionnaire (QOLIBRI) -Health: participant health questionnaire-9 –Anxiety: generalized anxiety disorder scale-7 –PTSD: post-traumatic stress disorder checklist for DSM-V | The authors found a significant overall time effect for average headache severity and frequency (based on a diary) 1 month after treatment. | + | B |
| Straudi et al., 2017 [42] | RCT | 36 y.o. 19% | Not described | >12 months | A randomized study to test the effects of video game therapy compared with a balance platform therapy on balance, mobility, and selective attention in chronic traumatic brain injury patients. | 21 | -Balance: CB&M, Unified Balance Scale, Timed Up and Go test -Attention: Go/No Go task -Static balance: force plate | Both groups improved in Community Balance and Mobility Scale scores, but only the video game therapy group increased on the Unified Balance Scale and Timed Up and Go test. | + | B |
| Thiagarajan and Ciuffreda, 2013 [52] | Cross-over design | 29 y.o. % of females not described | Not described | 1–10 years | To evaluate the vergence before and after vergence-based OMT in individuals who reported near work-related symptoms of an oculomotor nature after mTBI. | 12 | -Binocular central fixation, saccadic gain, saccadic latency, saccade ratio | Vergence-based oculomotor rehabilitation was effective in individuals with mTBI who reported near work-related symptoms: reduction in the horizontal fixational error, increase in horizontally and vertically saccadic gain, and decrease in the saccade ratio for reading. | + | B |
| Thiagarajan et al., 2014 [53] | Cross-over design | 29 y.o. % of females not described | Not described | 1–10 years | To evaluate the effect of oculomotor-based vision rehabilitation (OBVR) during 6 weeks (2 sessions per week) in mTBI. | 12 | -Near point of convergence, near point of accommodation, reading eye movements, saccade ratio, reading rate, Convergence Insufficiency Symptom Survey -Visual attention: Visual search and Attention test | OBVR had a strong positive effect on oculomotor control, reading rate, and overall reading ability, with an improvement of over 80% of the abnormal parameters. | + | B |
| First Author, Year of Publication | Study Design | Age (Mean ± Standard Deviation) and Gender | Etiology of mTBI | Delay between mTBI and Inclusion | Main Aim | Number of Participants | Outcomes and Tools | Results | + If Main Result Is Significant, − If Not | Incog Recommendation Level |
|---|---|---|---|---|---|---|---|---|---|---|
| Andersson et al., 2007 [65] | RCT | 32 y.o. 41% of females in the intervention group, 33% in the control group | Traffic accidents = 24%; falls = 45%; blow = 25% | 2–8 weeks | To assess if an early individualized, tailored, multidisciplinary outpatient rehabilitation program of selected patients with mTBI may reduce long-term (1 year) outcomes. | 395 | -PCS: Post-Concussion Symptoms Questionnaire -Life satisfaction: Life Satisfaction Questionnaire -Activity, participation and quality of life: Community Integration Questionnaire, Short-Form Health Survey 36 items, Interest Checklist, Role Checklist, Job Satisfaction Checklist | No statistically significant difference between the groups in terms of PCS and quality of life. | - | A |
| Audrit et al., 2021 [71] | Parallel groups (experimental and wait-list control) | 39 y.o. 60% female | Motor vehicle accidents = 16%; sports = 16%; other = 68% | 1–3 months | To assess the effect of a psycho-educative and counseling intervention named SAAM (Sleep/fatigue, Attention, Anxiety/mood, Memory) on PCS assessed using the Rivermead Post-Concussion Symptoms Questionnaire and on anxiety, depression, sleep, fatigue, memory, attention, and participation. | 25 | -PCS: RPCSQ -Sleep: Pittsburgh Sleep Quality Index -Anxiety and mood: Hospital Anxiety and Depression Scale -Fatigue: Multidimensional Fatigue Inventory -Cognition: attention and memory neuropsychological battery -Participation: Community Integration Questionnaire | No significant group x time interaction for the Rivermead Post-Concussion Questionnaire. | - | A |
| Bell et al., 2008 [58] | RCT with blinded assessment | 33 y.o. 35% female | Vehicle accidents = 55%; assault = 14%; sports = 5%; falls = 15%; other = 11% | <3 months | To determine whether focused, scheduled telephone counseling during the first 3 months after MTBI decreases symptoms and improves functioning at 6 months. | 366 | -PCS: Head Injury Symptom Checklist -Quality of life: Short Form Health Survey-12, Modified Perceived Quality of Life -Health, anxiety, mood: Patient Health Questionnaire (PHQ)-Depression and Panic/Anxiety | Significantly better 6-month outcome for symptoms and daily functioning but no difference in general health outcomes. | + | A |
| Caplain et al., 2019 [59] | RCT | 37 y.o. 63% female | Attacks = 33%; falls = 39%; sports = 0%; vehicle accidents = 19% | <1 month | To assess an early multidimensional intervention associating psycho-education and cognitive rehabilitation in patients presenting high-risk factors for persistent PCS. The control group received psycho-education alone. | 80 | -PCS: DSM-IV criteria -Work: cessation, resumption -Cognition: Digit span forward and backward (Wechsler Memory Scale), Mental control (MEM III, Wechsler Memory Scale), Letter-number sequences (MEM III, Wechsler Memory Scale), Trail Making Test, Parts A and B, Stroop test, Paced Auditory Serial Addition Test (PASAT), D2 Test of Attention, categorical and phonemic verbal fluency, Rey 15-item memory test -Quality of life: Quality of Life after Brain Injury (QOLIBRI) questionnaire -Anxiety and mood | At the 6-month follow-up, the proportion of patients with PCS was significantly lower in the treated group compared to the controls. | + | A |
| Chen et al., 2013 [72] | Double-blind placebo-controlled RCT | 45 y.o. 34% female | Not described | <1 day | To investigate how cerebrolysin therapy enhances cognitive recovery for mTBI patients. | 32 | -Cognition: MiniMental State Examination (MMSE), Cognitive Abilities Screening Instrument (CASI) | Improvement of CASI score at 12 weeks, especially concerning long-term memory and drawing function, but not the MMSE. | + | B |
| De Kruijk et al., 2005 [63] | RCT | 37 y.o. 44% female | Traffic accidents = 48%; work = 18%; violence = 8%; sports = 10% | <10 days | To evaluate the effect of bed rest on the severity of post-traumatic complaints after mTBI. | 107 | -PCS: 16 post-traumatic complaints assessed on a visual analogic scale -Quality of life: SF-36 | No significant differences between bed rest and no bed rest conditions on recovery. | - | A |
| Ghaffar et al., 2004 [64] | RCT | 32 y.o. 33% female | Motor-vehicle accidents = 48% | <one week | To determine whether multidisciplinary treatment of mTBI improves neurobehavioral outcomes at 6 months after injury. | 191 | -PCS: Rivermead Post-Concussion Disorder Questionnaire -Activity: Rivermead Follow-up Questionnaire -Anxiety and mood: 28-item General Health Questionnaire -Cognition: Stroop Color-Word Test, Symbol-Digit Modalities Test, Paced Visual Serial Addition Task, Simple Reaction Time, Choice Reaction Time, Hopkins Verbal Learning Test-Revised, the Vocabulary subtest of the Wechsler Adult Intelligence Scale—Third Edition (WAIS-III), the Letter–Number Sequencing subtest of the WAIS-III, the Matrix-Reasoning subtest of the WAIS-III | At 6 months after injury, there was no difference between the treatment group and control on any of the tests administered. However, in subjects with a psychiatric history, the provision of treatment was associated with significantly less depressive symptoms (GHQ subscale) 6 months after injury compared with untreated individuals. | - | A |
| Heskestad et al., 2010 [66] | RCT | 2 weeks after the injury | To evaluate the effect of an educational intervention on outcome after minimal, mild and moderate head injury (cognitive-oriented counseling, advice, the proposition of coping strategies, information, and reassuring) through one single consultation. Follow-up at 3 and 12 months. Outcome measures: interviews/symptoms, Beck Depression Inventory, Epworth Sleepiness Scale and the Fatigue Severity Scale. | 326 | -Mood: Beck Depression Inventory -Vigilance: Epworth Sleepiness Scale -Fatigue: Fatigue Severity Scale -Quality of life: SF-36 | No statistically significant differences between the intervention group and the control group. However, only 15% of patients completed the study. | - | B (high number of drop-out) | ||
| Matuseviciene et al., 2013 [67] | RCT | 39 y.o. 50% female | Falls = 42%; car or bicycle accidents = 17%; sports = 16%; assault = 5% | Early: 14–21 days | To investigate the effect of an early intervention visit in addition to written information and treatment as usual for patients with an estimated high risk for persisting disability after mTBI. | 97 | -PCS: RPCSQ -Anxiety and mood: HADS | No additional effect on symptom level at 3 months after mTBI compared to the usual treatment group. | - | A |
| Mittenberg et al., 1996 [56] | RCT with blinded 6-month assessment | 46 y.o. 31% female | Motor vehicle accidents = 59%; falls = 21% | Very early intervention (prior to discharge from the hospital) | To test the effectiveness of a structured cognitive-behavioral procedure for the prevention of PCS. Treatment based on a printed manual and consultation prior to discharge (psycho-education, information, techniques for reducing symptoms, and instructions for gradual resumption of premorbid activities). | 58 | -PCS: duration, number of symptoms, frequency of initial symptoms, days per week symptomatic at 6 months, and the severity of average symptoms at 6 months | 6-month outcome: treated patients reported significantly shorter symptom duration, fewer symptoms, fewer symptomatic days, and lower severity levels. | + | A |
| Moore et al., 2014 [62] | Non-randomized quasi-experimental study | 39 y.o. 27% female | Assault = 25%; bicycle or motor vehicle accidents = 38%; falls = 20% | <24 h | To determine the acceptability and effectiveness of Emergency Department Social Work Intervention for mTBI (SWIFT-Acute) on alcohol use, community functioning, depression, anxiety, post-concussive symptoms, post-traumatic stress disorder, and service use. | 64 | -Alcohol Use Disorders Identification Test -Participation: Community Integration Questionnaire -Qualitative acceptability survey -Health: patient Health Questionnaire-4 -PCS: RPCSQ -PTSD: Post-traumatic Stress Disorder Checklist-Civilian | 3-month outcome: Preliminary evidence of effectiveness in reducing alcohol use and preventing functional decline. No statistically significant differences were found in other measures. | + | B |
| Ponsford et al., 2002 [57] | Pseudo-RCT (participants were alternately assigned to one of two groups) | 26 y.o. gender not described | Motor vehicle accidents = 27%; falls = 18%; cycling accidents = 7%; assaults = 18%; sport = 23% | One week | To evaluate the impact of an information booklet outlining the symptoms associated with mTBI and suggestions for coping strategies. | 202 | -PCS: post-concussion syndrome checklist -Psychological adjustment: symptom checklist-90-revised -Stress: Holmes–Rahe survey of recent experiences -Cognition: national adult reading test (NART),13 four-choice reaction times (decision time), the Wechsler adult intelligence scale (reading) (WAIS-R) digit span and digit symbol subtests, the 2.4 and 2.0 s pacings of the paced auditory serial addition task (PASAT), the speed of comprehension subtest from the speed and capacity of language processing test, and the Rey auditory-verbal learning test | Patients in the intervention group reported fewer symptoms and were less stressed three months after the injury. | + | A |
| Robertson et al., 2017 [73] | Placebo-controlled RCT | 29 y.o. 33% female | Not described | <one week | To determine if the administration of atorvastatin 7 days after mTBI would improve neurological recovery. | 52 | -PCS: RPCSQ -adverse effects | No significant differences in neurological recovery after mTBI using atorvastatin versus a placebo at 3 months. | - | B |
| Scheenen et al., 2017 [70] | RCT | 41 y.o. 55% female | Not described | 4–6 weeks | Effectiveness of early cognitive behavioral intervention (CBTi) compared to telephonic counseling (TC) in at-risk mTBI patients. | 91 | -Return-to-work -Functional Outcome: Glasgow Outcome Scale-Extended -PCS: Head Injury Symptom Checklist -Coping: Utrechtse Coping List -Anxiety and mood: Hospital Anxiety and Depression Scale | No difference in return-to-work rate, coping styles and levels of anxiety, and depression at 3, 6, and 12 months. Patients in the TC group presented a more favorable outcome at 12 months and fewer complaints at 3 and 12 months. | + | A |
| Silverberg et al., 2013 [60] | Masked RCT | 39 y.o. 61% female | Motor vehicle accidents = 43%; falls = 32%; bicycle accidents = 21%; sport = 4% | <6 weeks | To assess the effect of early CBT, in addition to treatment as usual, on patients at risk for chronic PCS. | 28 | -PCS: RPCSQ -Daily functioning: Mayo-Portland Participation Index -Illness Perception Questionnaire—Revised -Anxiety and mood: Hospital Anxiety and Depression Scale | Masked outcome assessment was conducted at a 3-month follow-up. Significantly fewer treated participants had a diagnosis of PCS at follow-up compared to the controls. Treatment effect size was moderate for post-concussion symptoms. | + | A |
| Suffoletto et al., 2013 [61] | RCT | 30 y.o. 56% female | Not described | Early < 14 days | Randomized controlled study with 14-day follow-up to assess the efficacy of text messaging-based education and behavioral support on severe post-concussive symptoms. | 43 | -PCS: RPCSQ, DSM-IV criteria -PTSD: PTSD screen -Anxiety and mood: PHQ-4 -self-medication for pain -perception of the text messaging program | A trend toward lower reports of headaches, concentration difficulty, irritability, and anxiety in the group receiving text messages. | + | B |
| Varner et al. (2017) [69] | RCT | 35.2 y.o. 64% female | Assault = 7%; sport = 9%; bicyle or motor vehicle accidents = 26%; falls = 41% | <24 h | To determine if patients receiving cognitive rest and graduated return to usual activity discharge instructions had a decrease in PCS 2 weeks after injury. | 118 | -PCS: Post-Concussion Symptom Score -Number of missed days of school or work -Repeat visits to a healthcare provider | No significant group difference at 2- and 4-week assessment regarding post-commotional symptoms. | - | A |
| Vikane et al., 2017 [68] | RCT | 32 y.o. 39% female | Traffic accidents = 29%; falls = 37%; assault = 18%; sport = 16% | 6–8 weeks after mTBI | To evaluate the efficacy of a multidisciplinary outpatient follow-up program compared to follow-up by a general practitioner for patients being at-risk or sick-listed with persistent post-concussion symptoms two months after a mild traumatic brain injury. | 151 | -Return-to-work: delay -PCS: RPCSQ -Disability: Glasgow Outcome Scale Extended -Patient’s Global Impression of Change -Anxiety and mood: Hospital Anxiety and Depression Scale | No improvement in return-to-work and fewer post-concussion symptoms in the intervention compared to the control Group at 12 months. | - | A |
Appendix B. Risk of Bias Assessment




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- Manitchoko, L.; Bourdin, V.; Azouvi, P.; Hellmann, R.; Josseran, L. Estimating the epidemiology of mild traumatic brain injury in France from case mix of emergency departments. Ann. Phys. Rehabil. Med. 2020, 64, 101367. [Google Scholar] [CrossRef] [PubMed]
- Brazinova, A.; Rehorcikova, V.; Taylor, M.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.L.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef] [Green Version]
- Carroll, L.J.; Cassidy, J.D.; Holm, L.; Kraus, J.; Coronado, V.G.; WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Methodological issues and research recommendations for mild traumatic brain injury: The WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2004, 36, 113–125. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- van der Naalt, J.; Timmerman, M.E.; de Koning, M.E.; van der Horn, H.J.; Scheenen, M.E.; Jacobs, B.; Hageman, G.; Yilmaz, T.; Roks, G.; Spikman, J.M. Early predictors of outcome after mild traumatic brain injury (UPFRONT): An observational cohort study. Lancet Neurol. 2017, 16, 532–540. [Google Scholar] [CrossRef]
- McMahon, P.J.; Hricik, A.; Yue, J.; Puccio, A.M.; Inoue, T.; Lingsma, H.F.; Beers, S.R.; Gordon, W.A.; Valadka, A.B.; Manley, G.T.; et al. Symptomatology and functional outcome in mild traumatic brain injury: Results from the prospective TRACK-TBI study. J. Neurotrauma 2014, 31, 26–33. [Google Scholar] [CrossRef]
- Theadom, A.; Barker-Collo, S.; Jones, K.; Kahan, M.; Ao, B.T.; McPherson, K.; Starkey, N.; Feigin, V.; Kydd, R.; Barber, P.A.; et al. Work Limitations 4 Years After Mild Traumatic Brain Injury: A Cohort Study. Arch. Phys. Med. Rehabil. 2017, 98, 1560–1566. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; De Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: A European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Mikolić, A.; Polinder, S.; Steyerberg, E.W.; Helmrich, M.I.R.A.R.; Giacino, J.T.; Maas, A.I.R.; van der Naalt, J.; Voormolen, M.D.C.; von Steinbuechel, N.; Wilson, L.; et al. Prediction of Global Functional Outcome and Post-Concussive Symptoms after Mild Traumatic Brain Injury: External Validation of Prognostic Models in the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Study. J. Neurotrauma 2021, 38, 196–209. [Google Scholar] [CrossRef]
- van der Horn, H.J.; Out, M.L.; de Koning, M.E.; Mayer, A.R.; Spikman, J.M.; Sommer, I.E.; van der Naalt, J. An integrated perspective linking physiological and psychological consequences of mild traumatic brain injury. J. Neurol. 2019, 267, 2497–2506. [Google Scholar] [CrossRef]
- Stein, M.B.; Jain, S.; Giacino, J.T.; Levin, H.; Dikmen, S.; Nelson, L.D.; Vassar, M.J.; Okonkwo, D.O.; Diaz-Arrastia, R.; Robertson, C.S.; et al. Risk of Posttraumatic Stress Disorder and Major Depression in Civilian Patients After Mild Traumatic Brain Injury: A TRACK-TBI Study. JAMA Psychiatry 2019, 76, 249–258. [Google Scholar] [CrossRef] [PubMed]
- de Koning, M.; Gareb, B.; El Moumni, M.; Scheenen, M.; van der Horn, H.; Timmerman, M.; Spikman, J.; van der Naalt, J. Subacute posttraumatic complaints and psychological distress in trauma patients with or without mild traumatic brain injury. Injury 2016, 47, 2041–2047. [Google Scholar] [CrossRef] [PubMed]
- Mucha, A.; Fedor, S.; DeMarco, D. Vestibular dysfunction and concussion. Handb. Clin. Neurol. 2018, 158, 135–144. [Google Scholar] [CrossRef]
- Lingsma, H.F.; Yue, J.K.; Maas, A.I.R.; Steyerberg, E.W.; Manley, G.T. TRACK-TBI Investigators. Outcome prediction after mild and complicated mild traumatic brain injury: External validation of existing models and identification of new predictors using the TRACK-TBI pilot study. J. Neurotrauma 2015, 32, 83–94. [Google Scholar] [CrossRef]
- Rytter, H.M.; Graff, H.J.; Henriksen, H.K.; Aaen, N.; Hartvigsen, J.; Hoegh, M.; Nisted, I.; Næss-Schmidt, E.T.; Pedersen, L.L.; Schytz, H.W.; et al. Nonpharmacological Treatment of Persistent Post-concussion Symptoms in Adults: A Systematic Review and Meta-analysis and Guideline Recommendation. JAMA Netw. Open 2021, 4, e2132221. [Google Scholar] [CrossRef]
- Bayley, M.T.; Tate, R.; Douglas, J.M.; Turkstra, L.S.; Ponsford, J.; Stergiou-Kita, M.; Kua, A.; Bragge, P. INCOG guidelines for cognitive rehabilitation following traumatic brain injury: Methods and overview. J. Head Trauma Rehabil. 2014, 29, 290–306. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rytter, H.M.; Westenbaek, K.; Henriksen, H.; Christiansen, P.; Humle, F. Specialized interdisciplinary rehabilitation reduces persistent post-concussive symptoms: A randomized clinical trial. Brain Inj. 2019, 33, 266–281. [Google Scholar] [CrossRef]
- Storzbach, D.; Twamley, E.W.; Roost, M.S.; Golshan, S.; Williams, R.M.; O’Neil, M.; Jak, A.J.; Turner, A.P.; Kowalski, H.M.; Pagulayan, K.F.; et al. Compensatory Cognitive Training for Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn Veterans With Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2017, 32, 16–24. [Google Scholar] [CrossRef]
- Tiersky, L.A.; Anselmi, V.; Johnston, M.V.; Kurtyka, J.; Roosen, E.; Schwartz, T.; DeLuca, J. A trial of neuropsychologic rehabilitation in mild-spectrum traumatic brain injury. Arch. Phys. Med. Rehabil. 2005, 86, 1565–1574. [Google Scholar] [CrossRef]
- Thastum, M.M.; Rask, C.U.; Næss-Schmidt, E.T.; Tuborgh, A.; Jensen, J.S.; Svendsen, S.W.; Nielsen, J.F.; Schröder, A. Novel interdisciplinary intervention, GAIN, vs. enhanced usual care to reduce high levels of post-concussion symptoms in adolescents and young adults 2-6 months post-injury: A randomised trial. eClinicalMedicine 2019, 17, 100214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novakovic-Agopian, T.; Posecion, L.; Kornblith, E.S.; Abrams, G.; McQuaid, J.R.; Neylan, T.C.; Burciaga, J.; Joseph, J.; Carlin, G.; Groberio, J.; et al. Goal-Oriented Attention Self-Regulation Training Improves Executive Functioning in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury. J. Neurotrauma 2021, 38, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.B.; Bowles, A.O.; Kennedy, J.E.; Curtiss, G.; French, L.; Tate, D.; Vanderploeg, R.D. Cognitive Rehabilitation for Military Service Members With Mild Traumatic Brain Injury: A Randomized Clinical Trial. J. Head Trauma Rehabil. 2017, 32, E1–E15. [Google Scholar] [CrossRef] [PubMed]
- Johansson, B.; Wentzel, A.-P.; Andréll, P.; Mannheimer, C.; Rönnbäck, L. Methylphenidate reduces mental fatigue and improves processing speed in persons suffered a traumatic brain injury. Brain Inj. 2015, 29, 758–765. [Google Scholar] [CrossRef]
- Johansson, B.; Wentzel, A.-P.; Andréll, P.; Rönnbäck, L.; Mannheimer, C. Long-term treatment with methylphenidate for fatigue after traumatic brain injury. Acta Neurol. Scand. 2017, 135, 100–107. [Google Scholar] [CrossRef]
- Johansson, B.; Andréll, P.; Rönnbäck, L.; Mannheimer, C. Follow-up after 5.5 years of treatment with methylphenidate for mental fatigue and cognitive function after a mild traumatic brain injury. Brain Inj. 2020, 34, 229–235. [Google Scholar] [CrossRef]
- McAllister, T.W.; McDonald, B.C.; Flashman, L.A.; Ferrell, R.B.; Tosteson, T.D.; Yanofsky, N.N.; Grove, M.R.; Saykin, A.J. Alpha-2 adrenergic challenge with guanfacine one month after mild traumatic brain injury: Altered working memory and BOLD response. Int. J. Psychophysiol. 2011, 82, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Theadom, A.; Mahon, S.; Barker-Collo, S.; McPherson, K.; Rush, E.; Vandal, A.C.; Feigin, V.L. Enzogenol for cognitive functioning in traumatic brain injury: A pilot placebo-controlled RCT. Eur. J. Neurol. 2013, 20, 1135–1144. [Google Scholar] [CrossRef]
- Moussavi, Z.; Suleiman, A.; Rutherford, G.; Pouya, O.R.; Dastgheib, Z.; Zhang, W.; Salter, J.; Wang, X.; Mansouri, B.; Lithgow, B. A Pilot Randomised Double-Blind Study of the Tolerability and efficacy of repetitive Transcranial Magnetic Stimulation on Persistent Post-Concussion Syndrome. Sci. Rep. 2019, 9, 5498. [Google Scholar] [CrossRef] [Green Version]
- Harch, P.G.; Andrews, S.R.; Rowe, C.J.; Lischka, J.R.; Townsend, M.H.; Yu, Q.; Mercante, D.E. Hyperbaric oxygen therapy for mild traumatic brain injury persistent post-concussion syndrome: A randomized controlled trial. Med. Gas Res. 2020, 10, 8–20. [Google Scholar] [CrossRef]
- Boussi-Gross, R.; Golan, H.; Fishlev, G.; Bechor, Y.; Volkov, O.; Bergan, J.; Friedman, M.; Hoofien, D.; Shlamkovitch, N.; Ben-Jacob, E.; et al. Hyperbaric oxygen therapy can improve post concussion syndrome years after mild traumatic brain injury-randomized prospective trial. PLoS ONE 2013, 8, e79995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, W.C.; Franke, L.M.; Cifu, D.X.; Hart, B.B. Randomized, Sham-Controlled, Feasibility Trial of Hyperbaric Oxygen for Service Members With Post-concussion Syndrome: Cognitive and Psychomotor Outcomes 1 Week Postintervention. Neurorehabilit. Neural Repair 2014, 28, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Cifu, D.X.; Hart, B.B.; West, S.L.; Walker, W.; Carne, W. The effect of hyperbaric oxygen on persistent post-concussion symptoms. J. Head Trauma Rehabil. 2014, 29, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cifu, D.X.; Walker, W.C.; West, S.L.; Hart, B.B.; Franke, L.M.; Sima, A.; Graham, C.W.; Carne, W. Hyperbaric oxygen for blast-related post-concussion syndrome: Three-month outcomes. Ann. Neurol. 2014, 75, 277–286. [Google Scholar] [CrossRef]
- Belanger, H.G.; Barwick, F.; Silva, M.A.; Kretzmer, T.; Kip, K.E.; Vanderploeg, R.D. Web-based psychoeducational intervention for post-concussion symptoms: A randomized trial. Mil. Med. 2015, 180, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Vuletic, S.; Bell, K.; Jain, S.; Bush, N.; Temkin, N.; Fann, J.R.; Stanfill, K.E.; Dikmen, S.; Brockway, J.A.; He, F.; et al. Telephone Problem-Solving Treatment Improves Sleep Quality in Service Members With Combat-Related Mild Traumatic Brain Injury: Results From a Randomized Clinical Trial. J. Head Trauma Rehabil. 2016, 31, 147–157. [Google Scholar] [CrossRef]
- Theadom, A.; Barker-Collo, S.; Jones, K.; Dudley, M.; Vincent, N.; Feigin, V. A pilot randomized controlled trial of on-line interventions to improve sleep quality in adults after mild or moderate traumatic brain injury. Clin. Rehabil. 2018, 32, 619–629. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Vanuk, J.R.; Shane, B.R.; Weber, M.; Bajaj, S. A randomized, double-blind, placebo-controlled trial of blue wavelength light exposure on sleep and recovery of brain structure, function, and cognition following mild traumatic brain injury. Neurobiol. Dis. 2020, 134, 104679. [Google Scholar] [CrossRef]
- Raikes, A.C.; Dailey, N.S.; Shane, B.R.; Forbeck, B.; Alkozei, A.; Killgore, W.D.S. Daily Morning Blue Light Therapy Improves Daytime Sleepiness, Sleep Quality, and Quality of Life Following a Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2020, 35, E405–E421. [Google Scholar] [CrossRef]
- Kleffelgaard, I.; Soberg, H.L.; Tamber, A.-L.; Bruusgaard, K.A.; Pripp, A.H.; Sandhaug, M.; Langhammer, B. The effects of vestibular rehabilitation on dizziness and balance problems in patients after traumatic brain injury: A randomized controlled trial. Clin. Rehabil. 2019, 33, 74–84. [Google Scholar] [CrossRef]
- Straudi, S.; Severini, G.; Charabati, A.S.; Pavarelli, C.; Gamberini, G.; Scotti, A.; Basaglia, N. The effects of video game therapy on balance and attention in chronic ambulatory traumatic brain injury: An exploratory study. BMC Neurol. 2017, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.J.; Meeuwisse, W.H.; Nettel-Aguirre, A.; Barlow, K.; Boyd, L.; Kang, J.; Emery, C.A. Cervicovestibular rehabilitation in sport-related concussion: A randomised controlled trial. Br. J. Sports Med. 2014, 48, 1294–1298. [Google Scholar] [CrossRef] [PubMed]
- Meehan, A.; Hebert, D.; Deru, K.; Weaver, L.K. Longitudinal study of hyperbaric oxygen intervention on balance and affective symptoms in military service members with persistent post-concussive symptoms. J. Vestib. Res. 2019, 29, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Shukla, S.; Fallah, A.; Song, D.; Lin, L.; Golshan, S.; Tsai, A.; Jak, A.; Polston, G.; Lee, R. Repetitive Transcranial Magnetic Stimulation in Managing Mild Traumatic Brain Injury-Related Headaches. Neuromodulation 2016, 19, 133–141. [Google Scholar] [CrossRef]
- Leung, A.; Metzger-Smith, V.; He, Y.; Cordero, J.; Ehlert, B.; Song, D.; Lin, L.; Golshan, S.; Tsai, A.; Vaninetti, M.; et al. Left Dorsolateral Prefrontal Cortex rTMS in Alleviating MTBI Related Headaches and Depressive Symptoms. Neuromodulation 2018, 21, 390–401. [Google Scholar] [CrossRef]
- Stilling, J.M.; Paxman, E.; Mercier, L.J.; Gan, L.S.; Wang, M.; Amoozegar, F.; Dukelow, S.P.; Monchi, O.; Debert, C.T. Treatment of Persistent Post-Traumatic Headache and Post-Concussion Symptoms Using Repetitive Transcranial Magnetic Stimulation: A Pilot, Double-Blind, Randomized Controlled Trial. J. Neurotrauma 2020, 37, 312–323. [Google Scholar] [CrossRef]
- Choi, G.-S.; Kwak, S.G.; Lee, H.D.; Chang, M.C. Effect of high-frequency repetitive transcranial magnetic stimulation on chronic central pain after mild traumatic brain injury: A pilot study. J. Rehabil. Med. 2018, 50, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Kjeldgaard, D.; Forchhammer, H.B.; Teasdale, T.W.; Jensen, R.H. Cognitive behavioural treatment for the chronic post-traumatic headache patient: A randomized controlled trial. J. Headache Pain 2014, 15, 81. [Google Scholar] [CrossRef]
- Jensen, O.K.; Nielsen, F.F.; Vosmar, L. An open study comparing manual therapy with the use of cold packs in the treatment of post-traumatic headache. Cephalalgia 1990, 10, 241–250. [Google Scholar] [CrossRef]
- Esterov, D.; Thomas, A.; Weiss, K. Osteopathic manipulative medicine in the management of headaches associated with postconcussion syndrome. J. Osteopath. Med. 2021, 121, 651–656. [Google Scholar] [CrossRef]
- Thiagarajan, P.; Ciuffreda, K.J. Effect of oculomotor rehabilitation on vergence responsivity in mild traumatic brain injury. J. Rehabil. Res. Dev. 2013, 50, 1223–1240. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajan, P.; Ciuffreda, K.J.; Capo-Aponte, J.E.; Ludlam, D.P.; Kapoor, N. Oculomotor neurorehabilitation for reading in mild traumatic brain injury (mTBI): An integrative approach. NeuroRehabilitation 2014, 34, 129–146. [Google Scholar] [CrossRef] [PubMed]
- Cifu, D.X.; Hoke, K.W.; Wetzel, P.A.; Wares, J.R.; Gitchel, G.; Carne, W. Effects of hyperbaric oxygen on eye tracking abnormalities in males after mild traumatic brain injury. J. Rehabil. Res. Dev. 2014, 51, 1047–1056. [Google Scholar] [CrossRef]
- Kolakowsky-Hayner, S.A.; Bellon, K.; Toda, K.; Bushnik, T.; Wright, J.; Isaac, L.; Englander, J. A randomised control trial of walking to ameliorate brain injury fatigue: A NIDRR TBI model system centre-based study. Neuropsychol. Rehabil. 2017, 27, 1002–1018. [Google Scholar] [CrossRef] [PubMed]
- Mittenberg, W.; Tremont, G.; Zielinski, R.E.; Fichera, S.; Rayls, K.R. Cognitive-behavioural prevention of post-concussion syndrome. Arch. Clin. Neuropsychol. 1996, 11, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Ponsford, J.; Willmott, C.; Rothwell, A.; Cameron, P.; Kelly, A.-M.; Nelms, R.; Curran, C. Impact of early intervention on outcome following mild head injury in adults. J. Neurol. Neurosurg. Psychiatry 2002, 73, 330–332. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.R.; Hoffman, J.M.; Temkin, N.R.; Powell, J.M.; Fraser, R.T.; Esselman, P.C.; Barber, J.K.; Dikmen, S. The effect of telephone counselling on reducing post-traumatic symptoms after mild traumatic brain injury: A randomised trial. J. Neurol. Neurosurg. Psychiatry 2008, 79, 1275–1281. [Google Scholar] [CrossRef]
- Caplain, S.; Chenuc, G.; Blancho, S.; Marque, S.; Aghakhani, N. Efficacy of Psychoeducation and Cognitive Rehabilitation After Mild Traumatic Brain Injury for Preventing Post-concussional Syndrome in Individuals With High Risk of Poor Prognosis: A Randomized Clinical Trial. Front. Neurol. 2019, 10, 929. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Hallam, B.J.; Rose, A.; Underwood, H.; Whitfield, K.; Thornton, A.; Whittal, M.L. Cognitive-behavioural prevention of post-concussion syndrome in at-risk patients: A pilot randomized controlled trial. J. Head Trauma Rehabil. 2013, 28, 313–322. [Google Scholar] [CrossRef]
- Suffoletto, B.; Wagner, A.K.; Arenth, P.M.; Calabria, J.; Kingsley, E.; Kristan, J.; Callaway, C. Mobile phone text messaging to assess symptoms after mild traumatic brain injury and provide self-care support: A pilot study. J. Head Trauma Rehabil. 2013, 28, 302–312. [Google Scholar] [CrossRef]
- Moore, M.; Winkelman, A.; Kwong, S.; Segal, S.P.; Manley, G.T.; Shumway, M. The emergency department social work intervention for mild traumatic brain injury (SWIFT-Acute): A pilot study. Brain Inj. 2014, 28, 448–455. [Google Scholar] [CrossRef] [PubMed]
- de Kruijk, J.R.; Leffers, P.; Meerhoff, S.; Rutten, J.; Twijnstra, A. Effectiveness of bed rest after mild traumatic brain injury: A randomised trial of no versus six days of bed rest. J. Neurol. Neurosurg. Psychiatry 2002, 73, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, O.; McCullagh, S.; Ouchterlony, D.; Feinstein, A. Randomized treatment trial in mild traumatic brain injury. J. Psychosom. Res. 2006, 61, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Elgmark Andersson, E.; Emanuelson, I.; Björklund, R.; Stålhammar, D.A. Mild traumatic brain injuries: The impact of early intervention on late sequelae. A randomized controlled trial. Acta Neurochir. 2007, 149, 151–159, discussion 160. [Google Scholar] [CrossRef] [PubMed]
- Heskestad, B.; Waterloo, K.; Baardsen, R.; Helseth, E.; Romner, B.; Ingebrigtsen, T. No impact of early intervention on late outcome after minimal, mild and moderate head injury. Scand. J. Trauma Resusc. Emerg. Med. 2010, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matuseviciene, G.; Borg, J.; Stålnacke, B.-M.; Ulfarsson, T.; de Boussard, C. Early intervention for patients at risk for persisting disability after mild traumatic brain injury: A randomized, controlled study. Brain Inj. 2013, 27, 318–324. [Google Scholar] [CrossRef]
- Vikane, E.; Hellstrøm, T.; Røe, C.; Bautz-Holter, E.; Aßmus, J.; Skouen, J.S. Multidisciplinary outpatient treatment in patients with mild traumatic brain injury: A randomised controlled intervention study. Brain Inj. 2017, 31, 475–484. [Google Scholar] [CrossRef] [Green Version]
- Varner, C.E.; McLeod, S.; Nahiddi, N.; Lougheed, R.E.; Dear, T.E.; Borgundvaag, B. Cognitive Rest and Graduated Return to Usual Activities Versus Usual Care for Mild Traumatic Brain Injury: A Randomized Controlled Trial of Emergency Department Discharge Instructions. Acad. Emerg. Med. 2017, 24, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Scheenen, M.E.; Visser-Keizer, A.C.; De Koning, M.E.; Van Der Horn, H.J.; Van De Sande, P.; Van Kessel, M.E.; Van Der Naalt, J.; Spikman, J.M. Cognitive behavioural Intervention Compared to Telephone counselling Early after Mild Traumatic Brain Injury: A Randomized Trial. J. Neurotrauma 2017, 34, 2713–2720. [Google Scholar] [CrossRef] [Green Version]
- Audrit, H.; Beauchamp, M.H.; Tinawi, S.; Laguë-Beauvais, M.; Saluja, R.; de Guise, E. Multidimensional Psychoeducative and counselling Intervention (SAAM) for Symptomatic Patients With Mild Traumatic Brain Injury: A Pilot Randomized Controlled Trial. J. Head Trauma Rehabil. 2021, 36, E249–E261. [Google Scholar] [CrossRef]
- Chen, C.-C.; Wei, S.-T.; Tsaia, S.-C.; Chen, X.-X.; Cho, D.-Y. Cerebrolysin enhances cognitive recovery of mild traumatic brain injury patients: Double-blind, placebo-controlled, randomized study. Br. J. Neurosurg. 2013, 27, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.S.; McCarthy, J.J.; Miller, E.R.; Levin, H.; McCauley, S.R.; Swank, P.R. Phase II Clinical Trial of Atorvastatin in Mild Traumatic Brain Injury. J. Neurotrauma 2017. [Google Scholar] [CrossRef]
- Ponsford, J.; Lee, N.K.; Wong, D.; McKay, A.; Haines, K.; Alway, Y.; Downing, M.; Furtado, C.; O’Donnell, M. Efficacy of motivational interviewing and cognitive behavioural therapy for anxiety and depression symptoms following traumatic brain injury. Psychol. Med. 2016, 46, 1079–1090. [Google Scholar] [CrossRef]
- Lal, A.; Kolakowsky-Hayner, S.A.; Ghajar, J.; Balamane, M. The Effect of Physical Exercise After a Concussion: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2018, 46, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.A.; Hills, A.P.; Iverson, G.L. Graded Combined Aerobic Resistance Exercise (CARE) to Prevent or Treat the Persistent Post-concussion Syndrome. Curr. Neurol. Neurosci. Rep. 2018, 18, 75. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.A.; Farbenblum, J.; McLeod, S. Do physical interventions improve outcomes following concussion: A systematic review and meta-analysis? Br. J. Sports Med. 2021, 56, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.N.; Herget, L.; Zafonte, R.D.; Lamm, A.G.; Wong, B.M.; Leddy, J.J. Rehabilitation of Sport-Related Concussion. Clin. Sports Med. 2021, 40, 93–109. [Google Scholar] [CrossRef]
- Mollica, A.; Safavifar, F.; Fralick, M.; Giacobbe, P.; Lipsman, N.; Burke, M.J. Transcranial Magnetic Stimulation for the Treatment of Concussion: A Systematic Review. Neuromodulation 2021, 24, 803–812. [Google Scholar] [CrossRef]
- Wolf, G.; Cifu, D.; Baugh, L.; Carne, W.; Profenna, L. The effect of hyperbaric oxygen on symptoms after mild traumatic brain injury. J. Neurotrauma 2012, 29, 2606–2612. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heslot, C.; Azouvi, P.; Perdrieau, V.; Granger, A.; Lefèvre-Dognin, C.; Cogné, M. A Systematic Review of Treatments of Post-Concussion Symptoms. J. Clin. Med. 2022, 11, 6224. https://doi.org/10.3390/jcm11206224
Heslot C, Azouvi P, Perdrieau V, Granger A, Lefèvre-Dognin C, Cogné M. A Systematic Review of Treatments of Post-Concussion Symptoms. Journal of Clinical Medicine. 2022; 11(20):6224. https://doi.org/10.3390/jcm11206224
Chicago/Turabian StyleHeslot, Camille, Philippe Azouvi, Valérie Perdrieau, Aurélie Granger, Clémence Lefèvre-Dognin, and Mélanie Cogné. 2022. "A Systematic Review of Treatments of Post-Concussion Symptoms" Journal of Clinical Medicine 11, no. 20: 6224. https://doi.org/10.3390/jcm11206224
APA StyleHeslot, C., Azouvi, P., Perdrieau, V., Granger, A., Lefèvre-Dognin, C., & Cogné, M. (2022). A Systematic Review of Treatments of Post-Concussion Symptoms. Journal of Clinical Medicine, 11(20), 6224. https://doi.org/10.3390/jcm11206224