
Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review

 ,
,  ,
,  ,
,  ,
, 
 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration and Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Synthesis
2.4. Quality Assessment and Risk of Bias
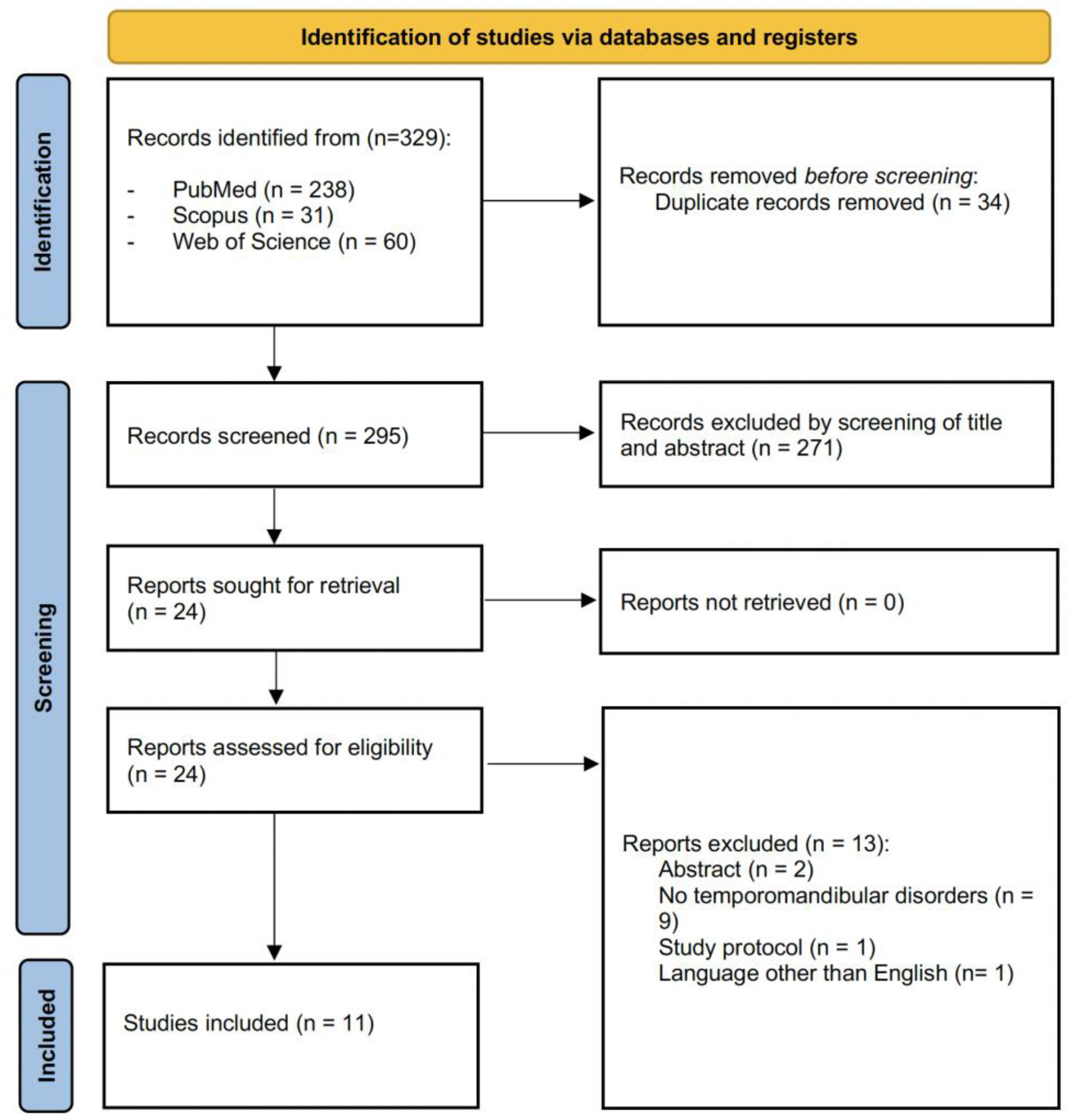
3. Results
3.1. Study Characteristics
3.2. Participants’ Characteristics
3.3. Vitamin D Serum Levels
3.4. Genotype and Frequency of Vitamin D Receptor Polymorphisms
3.5. Vitamin D Serum Levels and Biomarkers Expression
3.6. Vitamin D Serum Level, Physical Impairment, Psychological Impairment, and Quality of Life
3.7. Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the international RDC/TMD consortium network* and orofacial pain special interest group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Okeson, J.P. Bell’s Oral and Facial Pain, 7th ed.; Quintessence Publishing: Hannover, Germany, 2014. [Google Scholar]
- de Souza, R.F.; Lovato da Silva, C.H.; Nasser, M.; Fedorowicz, Z.; Al-Muharraqi, M.A. Interventions for the management of temporomandibular joint osteoarthritis. Cochrane Database Syst. Rev. 2012, 2012, Cd007261. [Google Scholar] [CrossRef]
- Kapos, F.P.; Exposto, F.G.; Oyarzo, J.F.; Durham, J. Temporomandibular disorders: A review of current concepts in aetiology, diagnosis and management. Oral Surg. 2020, 13, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Kavuncu, V.; Sahin, S.; Kamanli, A.; Karan, A.; Aksoy, C. The role of systemic hypermobility and condylar hypermobility in temporomandibular joint dysfunction syndrome. Rheumatol. Int. 2006, 26, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Wongwatana, S.; Kronman, J.H.; Clark, R.E.; Kabani, S.; Mehta, N. Anatomic basis for disk displacement in temporomandibular joint (TMJ) dysfunction. Am. J. Orthod. Dentofac. Orthop. 1994, 105, 257–264. [Google Scholar] [CrossRef]
- American Academy of Orofacial Pain. Orofacial Pain-Guidelinesfor Assessment, Diagnosis, and Management, 4th ed.; Leeuw, R.D., Ed.; Quintessence Publishing: Chicago, IL, USA, 2008. [Google Scholar]
- Ferrillo, M.; Curci, C.; Roccuzzo, A.; Migliario, M.; Invernizzi, M.; de Sire, A. Reliability of cervical vertebral maturation compared to hand-wrist for skeletal maturation assessment in growing subjects: A systematic review. J. Back Musculoskelet. Rehabil. 2021, 34, 925–936. [Google Scholar] [CrossRef]
- Hong, S.W.; Lee, J.K.; Kang, J.H. Skeletal maturation and predicted adult height in adolescents with temporomandibular joint osteoarthritis. J. Oral Rehabil. 2019, 46, 541–548. [Google Scholar] [CrossRef]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef]
- Bueno, C.H.; Pereira, D.D.; Pattussi, M.P.; Grossi, P.K.; Grossi, M.L. Gender differences in temporomandibular disorders in adult populational studies: A systematic review and meta-analysis. J. Oral Rehabil. 2018, 45, 720–729. [Google Scholar] [CrossRef]
- Bitiniene, D.; Zamaliauskiene, R.; Kubilius, R.; Leketas, M.; Gailius, T.; Smirnovaite, K. Quality of life in patients with temporomandibular disorders. A systematic review. Stomatologija 2018, 20, 3–9. [Google Scholar]
- Castro-Calderón, A.; Roccuzzo, A.; Ferrillo, M.; Gada, S.; González-Serrano, J.; Fonseca, M.; Molinero-Mourelle, P. Hyaluronic acid injection to restore the lost interproximal papilla: A systematic review. Acta Odontol. Scand. 2022, 80, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; Molinero-Mourelle, P.; Ferrillo, M.; Cobo-Vázquez, C.; Sanchez-Labrador, L.; Ammendolia, A.; Migliario, M.; de Sire, A. Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review. Appl. Sci. 2021, 11, 3927. [Google Scholar] [CrossRef]
- Baad-Hansen, L.; Benoliel, R. Neuropathic orofacial pain: Facts and fiction. Cephalalgia 2017, 37, 670–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolland, M.J.; Grey, A.; Avenell, A. Effects of vitamin D supplementation on musculoskeletal health: A systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018, 6, 847–858. [Google Scholar] [CrossRef] [Green Version]
- Gkekas, N.K.; Anagnostis, P.; Paraschou, V.; Stamiris, D.; Dellis, S.; Kenanidis, E.; Potoupnis, M.; Tsiridis, E.; Goulis, D.G. The effect of vitamin D plus protein supplementation on sarcopenia: A systematic review and meta-analysis of randomized controlled trials. Maturitas 2021, 145, 56–63. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Zittermann, A. The biphasic effect of vitamin D on the musculoskeletal and cardiovascular system. Int. J. Endocrinol. 2017, 2017, 3206240. [Google Scholar] [CrossRef] [Green Version]
- Penner, J.; Ferrand, R.A.; Richards, C.; Ward, K.A.; Burns, J.E.; Gregson, C.L. The impact of vitamin D supplementation on musculoskeletal health outcomes in children, adolescents, and young adults living with HIV: A systematic review. PLoS ONE 2018, 13, e0207022. [Google Scholar] [CrossRef] [Green Version]
- Amirkhizi, F.; Asoudeh, F.; Hamedi-Shahraki, S.; Asghari, S. Vitamin D status is associated with inflammatory biomarkers and clinical symptoms in patients with knee osteoarthritis. Knee 2022, 36, 44–52. [Google Scholar] [CrossRef]
- Calafiore, D.; Fortunato, L.; Migliario, M. Vitamin D for clinical diseases in women: An indispensable factor in medicine and dentistry. J. Clin. Med. 2022, 11, 3104. [Google Scholar] [CrossRef]
- Krasniqi, E.; Boshnjaku, A.; Wagner, K.H.; Wessner, B. Association between polymorphisms in vitamin D pathway-related genes, vitamin D status, muscle mass and function: A systematic review. Nutrients 2021, 13, 3109. [Google Scholar] [CrossRef] [PubMed]
- Baldock, P.A.; Thomas, G.P.; Hodge, J.M.; Baker, S.U.; Dressel, U.; O’Loughlin, P.D.; Nicholson, G.C.; Briffa, K.H.; Eisman, J.A.; Gardiner, E.M. Vitamin D action and regulation of bone remodeling: Suppression of osteoclastogenesis by the mature osteoblast. J. Bone Miner. Res. 2006, 21, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Harada, S.; Mizoguchi, T.; Kobayashi, Y.; Nakamichi, Y.; Takeda, S.; Sakai, S.; Takahashi, F.; Saito, H.; Yasuda, H.; Udagawa, N.; et al. Daily administration of eldecalcitol (ED-71), an active vitamin D analog, increases bone mineral density by suppressing RANKL expression in mouse trabecular bone. J. Bone Miner. Res. 2012, 27, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Embree, M.; Ono, M.; Kilts, T.; Walker, D.; Langguth, J.; Mao, J.; Bi, Y.; Barth, J.L.; Young, M. Role of subchondral bone during early-stage experimental TMJ osteoarthritis. J. Dent. Res. 2011, 90, 1331–1338. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Lee, S.; Pan, H.C.; Mohammad, A.; Lin, A.; Guo, W.; Chen, E.; Ahn, A.; Li, J.; Ting, K.; et al. Association of condylar bone quality with TMJ osteoarthritis. J. Dent. Res. 2017, 96, 888–894. [Google Scholar] [CrossRef]
- Behm, C.; Blufstein, A.; Gahn, J.; Kubin, B.; Nemec, M.; Moritz, A.; Rausch-Fan, X.; Andrukhov, O. 1,25(OH)2D3 differently affects immunomodulatory activities of mesenchymal stem cells depending on the presence of TNF-α, IL-1β and IFN-γ. J. Clin. Med. 2019, 8, 2211. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Zhang, Y.; Jia, T.; Sun, Y. Molecular mechanism underlying the tumor-promoting functions of carcinoma-associated fibroblasts. Tumour Biol. 2015, 36, 1385–1394. [Google Scholar] [CrossRef]
- Walawska-Hrycek, A.; Galus, W.; Hrycek, E.; Kaczmarczyk, A.; Krzystanek, E. The impact of vitamin D low doses on its serum level and cytokine profile in multiple sclerosis patients. J. Clin. Med. 2021, 10, 2781. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Roccuzzo, A.; Molinero-Mourelle, P.; Falcicchio, G.; Umano, G.R.; Pezzotti, F.; Foglio Bonda, P.L.; Calafiore, D.; de Sire, A. Periodontal disease and vitamin D deficiency in pregnant women: Which correlation with preterm and low-weight birth? J. Clin. Med. 2021, 10, 4578. [Google Scholar] [CrossRef]
- Agostini, D.; Zeppa Donati, S.; Lucertini, F.; Annibalini, G.; Gervasi, M.; Ferri Marini, C.; Piccoli, G.; Stocchi, V.; Barbieri, E.; Sestili, P. Muscle and bone health in postmenopausal women: Role of protein and vitamin D supplementation combined with exercise training. Nutrients 2018, 10, 1103. [Google Scholar] [CrossRef] [Green Version]
- Gratton, M.P.; Londono, I.; Rompré, P.; Villemure, I.; Moldovan, F.; Nishio, C. Effect of vitamin D on bone morphometry and stability of orthodontic tooth movement in rats. Am. J. Orthod. Dentofac. Orthop. 2022; in press. [Google Scholar] [CrossRef]
- Institute, T.J.B. JBI Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 14 October 2022).
- Ahmed, S. Biochemical changes related with temporomandibular joint disorders and inflammatory arthritis. Biomed. Pharmacol. J. 2017, 10, 2085–2090. [Google Scholar] [CrossRef]
- Khanna, S.S.; Parulekar, N.R.; Dhaimade, P.A. The influence of vitamin D on the temporomandibular joint and the activities of daily living. J. Clin. Diagn. Res. 2017, 11, 31–34. [Google Scholar] [CrossRef]
- Bashir, S.; Shah, A.A.; Dar, J.I.; Misgar, I.A.; Sabba, A.; Firdous, P.; Hakim, T.; Mir, S.H. Association of VDR gene BsmI polymorphism with temporomandibular joint disorders: A case control study in Kashmiri population. Gene Rep. 2022, 27, 101613. [Google Scholar] [CrossRef]
- Madani, A.; Shamsian, S.A.; Layegh, P.; Abrisham, S.M.; Ravaghi, A.; Najjaran, N.T. Are certain factors involved in calcium metabolism associated with temporomandibular disorders? Cranio 2021, 39, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Nemati, M.; Tabrizi, R.; Rasooli, F.; Ghafari, S. Is the prevalence of vitamin D deficiency in patients with temporomandibular disorder higher than healthy control group? J. Maxillofac. Oral Surg. 2021. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, R.; Gill, S. Effectiveness of vitamin D along with splint therapy in the vit D deficient patients with temporomandibular disorder-A Randomized, double-blind, placebo-controlled clinical trial. J. Indian Prosthodont. Soc. 2022, 22, 65–73. [Google Scholar] [CrossRef]
- Hong, S.W.; Kang, J.H. Bone mineral density, bone microstructure, and bone turnover markers in females with temporomandibular joint osteoarthritis. Clin. Oral Investig. 2021, 25, 6435–6448. [Google Scholar] [CrossRef]
- Staniszewski, K.; Lygre, H.; Berge, T.; Rosén, A. Serum analysis in patients with temporomandibular disorders: A controlled cross-sectional study in Norway. Pain Res. Manag. 2019, 2019, 1360725. [Google Scholar] [CrossRef] [Green Version]
- Demir, C.Y.; Ersoz, M.E. Biochemical changes associated with temporomandibular disorders. J. Int. Med. Res. 2019, 47, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, S.; Tumer, M.K.; Yigit, S.; Nursal, A.F.; Rustemoglu, A.; Balel, Y. Relation of vitamin D and BsmI variant with temporomandibular diseases in the Turkish population. Br. J. Oral Maxillofac. Surg. 2021, 59, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.D.; Yazicioglu, D.; Öncül, A.M.T.; Yilmaz, E.; Ereş, G. Vitamin D receptor gene polymorphisms (Apa1 and Taq1) in temporomandibular joint internal derangement/osteoarthritis in a group of Turkish patients. Mol. Biol. Rep. 2018, 45, 1839–1848. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 35, 921–936. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Marotta, N.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for reducing pro-inflammatory cytokines serum levels in musculoskeletal and temporomandibular disorders: A comprehensive review. Int. J. Mol. Sci. 2022, 23, 2528. [Google Scholar] [CrossRef]
- Marotta, N.; Ferrillo, M.; Demeco, A.; Drago Ferrante, V.; Inzitari, M.T.; Pellegrino, R.; Pino, I.; Russo, I.; de Sire, A.; Ammendolia, A. Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial. Appl. Sci. 2022, 12, 3821. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Pitance, L.; Singh, V.; Neto, F.; Thie, N.; Michelotti, A. Effectiveness of manual therapy and therapeutic exercise for temporomandibular disorders: Systematic review and meta-analysis. Phys. Ther. 2016, 96, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; d’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. Cranio 2022, 1–17. [Google Scholar] [CrossRef]
- Singh, V.; Misra, A.K.; Singh, M.; Kumar, B.; Midha, N.K.; Ambwani, S. A prospective, cross-sectional study on association of serum vitamin D level with musculoskeletal symptoms and blood pressure in adult population. J. Fam. Med. Prim. Care 2020, 9, 1628–1632. [Google Scholar] [CrossRef]
- Helde-Frankling, M.; Björkhem-Bergman, L. Vitamin D in pain management. Int. J. Mol. Sci. 2017, 18, 2170. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. Effect of vitamin D supplementation on pain: A systematic review and meta-analysis. Pain Physician 2016, 19, 415–427. [Google Scholar]
- Furquim, B.D.; Flamengui, L.M.; Conti, P.C. TMD and chronic pain: A current view. Dent. Press J. Orthod. 2015, 20, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Morris, H.A.; Anderson, P.H. Autocrine and paracrine actions of vitamin D. Clin. Biochem. Rev. 2010, 31, 129–138. [Google Scholar] [PubMed]
- Uitterlinden, A.G.; Fang, Y.; Van Meurs, J.B.; Pols, H.A.; Van Leeuwen, J.P. Genetics and biology of vitamin D receptor polymorphisms. Gene 2004, 338, 143–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombini, A.; Brayda-Bruno, M.; Lombardi, G.; Croiset, S.J.; Ceriani, C.; Buligan, C.; Barbina, M.; Banfi, G.; Cauci, S. BsmI, ApaI and TaqI polymorphisms in the vitamin D receptor gene (VDR) and association with lumbar spine pathologies: An Italian case-control study. PLoS ONE 2016, 11, e0155004. [Google Scholar] [CrossRef] [PubMed]
- Azharuddin, A.; Ilmawan, M.; Fajar, J.K.; Fahriani, M.; Mamada, S.S.; Maliga, H.A.; Nainu, F.; Dhama, K.; Harapan, H.; Magetsari, R. The role of single nucleotide polymorphisms of IL-1A-889C>T (rs1800587), TNF-A-238G>A (rs361525), and VDR TaqI (rs731236) on susceptibility to herniated nucleus pulposus: A systematic review and meta-analysis. F1000Research 2021, 10, 419. [Google Scholar] [CrossRef]
- Usategui-Martín, R.; De Luis-Román, D.-A.; Fernández-Gómez, J.M.; Ruiz-Mambrilla, M.; Pérez-Castrillón, J.-L. Vitamin D receptor (VDR) gene polymorphisms modify the response to vitamin D supplementation: A systematic review and meta-analysis. Nutrients 2022, 14, 360. [Google Scholar] [CrossRef]
- Lv, L.; Tan, X.; Peng, X.; Bai, R.; Xiao, Q.; Zou, T.; Tan, J.; Zhang, H.; Wang, C. The relationships of vitamin D, vitamin D receptor gene polymorphisms, and vitamin D supplementation with Parkinson’s disease. Transl. Neurodegener. 2020, 9, 34. [Google Scholar] [CrossRef]


{kind=link}
| PubMed: ((("vitamin d"[MeSH Terms] OR "vitamin d"[All Fields] OR "ergocalciferols"[MeSH Terms] OR "ergocalciferols"[All Fields] OR "calcifediol"[MeSH Terms] OR "calcifediol"[All Fields] OR "25 oh d3"[All Fields])) AND ((("temporomandibular joint disorders"[MeSH Terms]) OR ("temporomandibular"[All Fields] AND "joint"[All Fields] AND "disorders"[All Fields]) OR ("osteoarthritis"[MeSH Terms] OR "osteoarthritis"[All Fields] OR "osteoarthritides"[All Fields]) OR ("masticatory muscles"[MeSH Terms] OR "masticatory"[All Fields] AND "muscles"[All Fields]) OR ("masticatory muscles"[All Fields])) AND (("disease"[MeSH Terms] OR "disease"[All Fields] OR "disorder"[All Fields] OR "disorders"[All Fields] OR "disorder s"[All Fields] OR "disordes"[All Fields]) OR ("bruxism"[MeSH Terms] OR "bruxism"[All Fields])))) |
| Scopus: ((("vitamin d" OR "ergocalciferols" OR "calcifediol" OR "25 oh d3")) AND (("temporomandibular joint" OR "temporomandibular joint disorders" OR "TMD" OR "temporomandibular osteoarthritis") OR ("masticatory muscles" OR "masticatory muscles disease" OR "masticatory muscles disorder") OR ("bruxism"))) |
| Web of Science: ((("vitamin d" OR "ergocalciferols" OR "calcifediol" OR "25 oh d3")) AND (("temporomandibular joint" OR "temporomandibular joint disorders" OR "TMD" OR "temporomandibular osteoarthritis") OR ("masticatory muscles" OR "masticatory muscles disease" OR "masticatory muscles disorder") OR ("bruxism"))) |
| Authors | Journal | Design | Nationality | Population | Age (years) | Intervention | Comparator | Outcome | Time Points | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Ahmed, H.S. et al., 2017 [35] | Biomedical & Pharmacology Journal | Cross-sectional study | Iraq | Total: n = 90; M/F = 37/53 Group 1: n = 45; M/F = 15/30 Group 2: n = 45; M/F = 22/23 | Total: N/A Group 1: 12.60 ± 50.58 Group 2: 8.50 ± 43.02 | Group 1: TMD patients with rheumatoid arthritis | Group 2: healthy subjects | Calcium, total alkaline phosphatase (ALP) activity, and IL-1 serum levels | The vitamin D serum levels were significantly lower in TMD patients (p = 0.001). Moreover, results showed a significant increase in total ALP and IL-1 serum levels in TMD patients (p = 0.01). There was a significant negative correlation between serum vitamin D activity with total ALP activity and IL-1 in temporomandibular disorder patients (p = 0.001) | |
| Bashir, S. et al., 2022 [37] | Gene Reports | Cross-sectional study | India | Total: n = 106; M/F = N/A Group 1: n = 53; M/F = N/A Group 2: n = 53; M/F = N/A | Total: (18–45) Group 1: N/A Group 2: N/A | Group 1: TMD patients with internal derangement (TMD-ID) | Group 2: healthy subjects | Genotype and frequency of VDR gene polymorphisms for BsmI. | BsmI polymorphism was significantly higher for mutant genotype/allele in TMD-ID patients than for controls (OR = 4.1; p = 0.0015). Therefore, there was a significant association between TMJ internal derangement development and allelic and genotypic frequencies of BsmI. | |
| Demir, C.Y. et al., 2018 [43] | Journal of International Medical Research | Prospective observational study | Turkey | Total: n = 100; M/F = 23/77 Group 1: n = 50; M/F = 11/39 Group 2: n = 50; M/F = 12/38 | Total: 27.07 ± 5.44 Group 1: 28.24 ± 10.41 Group 2: 30.90 ± 8.49 | Group 1: TMD patients | Group 2: healthy subjects | Vitamin D, parathyroid hormone, calcitonin, calcium, phosphorus, and magnesium serum levels. | Only parathyroid hormone serum levels were found to be significantly higher in Group 1 versus Group 2 (p < 0.001). | |
| Gupta, A.K. et al., 2022 [40] | The Journal of Indian Prosthodontic Society | Randomized controlled trial | India | Total: n = 36; M/F = N/A Group 1: n = 18; M/F = N/A Group 2: n = 18; M/F = N/A | Total: (18–45) Group 1: N/A Group 2: N/A | Group 1: stabilization splint plus vitamin D supplementation in TMD patients with vitamin D serum levels < 30 ng/mL | Group 2: stabilization splint plus placebo drug in TMD patients with vitamin D serum levels < 30 ng/mL | Comfort mouth opening, VAS, maximum mouth opening, vitamin D serum levels, TMJ tenderness, efficacy of stabilization splint therapy plus vitamin D supplementation. | T0 (baseline), T1 (1 week), T2 (1 month), T3 (2 months), and T4 (3 months) after therapy | By intergroup analysis, a significant difference was only shown in comfort mouth opening, VAS, and maximum mouth opening (p < 0.05). |
| Hong, S.W. et al., 2021 [41] | Clinical Oral Investigations | Prospective observational study | Korea | Total: n = 100; M/F = 0/100 Group 1: n = 59; M/F = 0/59 Group 2: n = 41; M/F = 0/41 | Total: N/A Group 1: 23.4 ± 3.4 Group 2: 57.2 ± 4.6 | Group 1: 43 young females with TMD osteoarthritis Group 2: 29 post-menopausal females with TMD osteoarthritis | Group 1: 16 young, healthy subjects Group 2: 12 post-menopausal, healthy subjects | TMD osteoarthritis progression, Vitamin D serum level, and BMD | T0 (baseline) and T1 (12 months) | The baseline levels of 25-dihydroxyvitamin D were significantly different among the control group in the young females. There was a significant association between progression of the TMJ osteoarthritis and Vitamin D levels in the young and post-menopausal females (p = 0.045). |
| Khanna, S.S. et al., 2017 [36] | Journal of Clinical and Diagnostic Research | Cross-sectional study | India | Total: n = 100; M/F = 39/61 Group 1: n = 50; M/F = 20/30 Group 2: n = 50; M/F = 19/31 | Total: 48.98 (25–70) Group 1: 52.96 Group 2: 45.0 | Group 1: TMD patients with vitamin D serum levels < 30 ng/mL | Group 2: TMD patients with normal vitamin D serum levels | TMD pain and discomfort in the activities of daily living. | Authors showed that low serum vitamin D levels were associated with TMJ pain and/or discomfort, which had a significant (p = NR) negative impact on the various activities of daily living of the participants. | |
| Madani, A. et al., 2019 [38] | The Journal of Craniomandibular & Sleep Practice | Cross-sectional study | Iran | Total: n = 80; M/F = 14/66 Group 1: n = 51; M/F = 5/46 Group 2: n = 29; M/F = 9/20 | Total: N/A Group 1: 27 (21–46) Group 2: 32 (20–48) | Group 1: TMD patients | Group 2: healthy subjects | Serum concentrations of calcium, phosphate, alkaline phosphatase, parathyroid hormone, and vitamin D. | No statistically significant differences were observed between different groups in any of the variables studied (p > 0.05). | |
| Nemati, M. et al., 2021 [39] | Journal of Maxillofacial and Oral Surgery | Cross-sectional study | Iran | Total: n = 110; M/F = 39/71 Group 1: n = 55; M/F = 18/37 Group 2: n = 55; M/F = 21/34 | Total: N/A Group 1: 30.05 ± 6.92 Group 2: 29.74 ± 6.91 | Group 1: TMD patients | Group 2: healthy subjects | Serum level of vitamin D | Analysis of the data demonstrated a significant difference in the mean serum levels of vitamin D between the study and control group (p = 0.001), that had an underlying prevalence of vitamin D deficiency in TMD. | |
| Staniszewski, K. et al., 2019 [42] | Pain Research and Management | Cross-sectional study | Norway | Total: n = 120; M/F = 18/102 Group 1: n = 60; M/F = 9/51 Group 2: n = 60; M/F = 9/51 | Total: N/A Group 1: 45 (20–69) Group 2: 46 (23–71) | Group 1: TMD patients | Group 2: healthy subjects | Serum level of hemoglobin, erythrocyte volume fraction (EVF), mean corpuscular volume (MCV), homocysteine, transferrin receptor (TfR), thyroid- stimulating hormone (TSH), free thyroxine (FT4), parathyroid hormone (PTH), cobalamin, folate, C-reactive protein, creatinine, estimated glomerular filtration rate (GFR), sodium, potassium, calcium, gamma-glutamyl transferase (GT), albumin, and 25(OH) vitamin D. | Results revealed that TMD patients had significantly higher values of hemoglobin (p = 0. 036), cobalamin (p = 0.023), albumin (p = 0.005), PTH (p = 0.038), and 25(OH) vitamin D (p = 0.005), and significantly lower values of creatinine (p = 0.006) and potassium (p = 0.011), compared to controls. | |
| Yildiz, S. et al., 2020 [44] | British Journal of Oral & Maxillofacial Surgery | Prospective case-control study | Turkey | Total: n = 206; M/F = 74/132 Group 1: n = 104; M/F = 30/74 Group 2: n = 102; M/F = 44/58 | Total: N/A Group 1: 28.64 ± 10.11 Group 2: 31.48 ± 11.33 | Group 1: TMD patients (disc displacement with reduction) | Group 2: healthy subjects | VDR BsmI variant (after extraction of genomic DNA) and serum level of vitamin D. | Serum vitamin D level was significantly different between the patient and the control group (p = 0.008); particularly, vitamin D serious deficiency was more prevalent in the TMD patients (p = 0.00001). Logistic regression analysis revealed that the bb genotype and b allele carriers of VDR BsmI variant were significantly associated with an increased risk of disc dislocation (p = 0.022 and p = 0.01, respectively). VDR BsmI bb genotype was higher in the control group compared to the patient group (p = 0.045). | |
| Yilmaz, A.D. et al., 2018 [45] | Molecular Biology Reports | Cross-sectional study | Turkey | Total: n = 119; M/F = N/A Group 1: n = 24; M/F = N/A Group 2: n = 25; M/F = N/A Group 3: n = 70; M/F = N/A | Total: N/A Group 1: 31.58 ± 8.25 Group 2: 31.8 ± 7.53 Group 2: 28.22 ± 5.9 | Group 1: TMD patients (anterior disk displacement with reduction) Group 2: TMD patients (anterior disk displacement without reduction) | Group 3: healthy subjects | VDR Apa1 and Taq1 polymorphisms. | When Group 1 and Group 2 were compared to healthy subjects, Apa1 Aa genotype compared to AA genotype had odds ratios of 1.65, 1.79, and 1.64 respectively (p > 0.05). In TMJ-ID women versus healthy women Aa genotype had 2.06- fold (p = 0.15) odds compared to AA genotype. Taq1 results showed that in TMJ-ID patients and anterior disk displacement without reduction cases the Tt genotype had odds ratios of 0.63 and 0.44- fold (p > 0.05) respectively. In TMJ-ID women the Tt and tt genotypes had odds ratios of 0.53 and 0.73 (p > 0.05). Combined VDR genotypes revealed that AATT had a 3.3-fold (p = 1.21) odds ratio while AATt had a 2.0-fold odds ratio (p = 0.29) (OR 0.59, 95% CI 0.23–1.49, p = 0.26) compared to AaTt. |
| Joanna Briggs Institute Critical Appraisal Checklist for randomized controlled trials. | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Total Score |
| Gupta et al., 2022 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 13 |
| Legend: Q1—Was true randomization used for assignment of participants to treatment groups?; Q2—Was allocation to treatment groups concealed?; Q3—Were treatment groups similar at the baseline?; Q4— Were participants blind to treatment assignment?; Q5—Were those delivering treatment blind to treatment assignment?; Q6—Were outcome assessors blind to treatment assignment?; Q7—Were treatment groups treated identically, other than the intervention of interest?; Q8—Was follow up complete and, if not, were differences between groups, in terms of their follow up, adequately described and analyzed?; Q9— Were participants analyzed in the groups to which they were randomized?; Q10—Were outcomes measured in the same way for treatment groups?; Q11—Were outcomes measured in a reliable way?; Q12—Was an appropriate statistical analysis used?; Q13—Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization and parallel groups) accounted for in the conduct and analysis of the trial?; N—no; Y—yes; and N/A—not applicable. | ||||||||||||||
| Joanna Briggs Institute Critical Appraisal for Quasi-Experimental Studies | ||||||||||||||
| Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Total Score | ||||
| Ahmed et al., 2017 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Bashir et al., 2022 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Demir et al., 2018 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Hong et al., 2021 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Khanna et al., 2017 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Madani et al., 2019 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Nemati et al., 2021 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Staniszewski et al., 2019 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Yildiz et al., 2020 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Yilmaz et al., 2018 | Y | Y | N | Y | N | Y | Y | Y | Y | 7 | ||||
| Joanna Briggs Institute Critical Appraisal Checklist for Case Control Studies: Q1—Is it clear in the study what is the ’cause’ and what is the ‘effect’ (i.e., there is no confusion about which variable comes first)?; Q2—Were the participants included in any comparisons similar?; Q3—Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest?; Q4—Was there a control group?; Q5—Were there multiple measurements of the outcome, both pre and post the intervention/exposure?; Q6—Was follow up complete and, if not, were differences between groups in terms of their follow up adequately described and analyzed?; Q7—Were the outcomes of the participants included in any of the comparisons measured in the same way?; Q8—Were outcomes measured in a reliable way?; Q9—Was an appropriate statistical analysis used?; N—no, Y—yes; and N/A—not applicable. | ||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrillo, M.; Lippi, L.; Giudice, A.; Calafiore, D.; Paolucci, T.; Renò, F.; Migliario, M.; Fortunato, L.; Invernizzi, M.; Sire, A.d. Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review. J. Clin. Med. 2022, 11, 6231. https://doi.org/10.3390/jcm11216231
Ferrillo M, Lippi L, Giudice A, Calafiore D, Paolucci T, Renò F, Migliario M, Fortunato L, Invernizzi M, Sire Ad. Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review. Journal of Clinical Medicine. 2022; 11(21):6231. https://doi.org/10.3390/jcm11216231
Chicago/Turabian StyleFerrillo, Martina, Lorenzo Lippi, Amerigo Giudice, Dario Calafiore, Teresa Paolucci, Filippo Renò, Mario Migliario, Leonzio Fortunato, Marco Invernizzi, and Alessandro de Sire. 2022. "Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review" Journal of Clinical Medicine 11, no. 21: 6231. https://doi.org/10.3390/jcm11216231
APA StyleFerrillo, M., Lippi, L., Giudice, A., Calafiore, D., Paolucci, T., Renò, F., Migliario, M., Fortunato, L., Invernizzi, M., & Sire, A. d. (2022). Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review. Journal of Clinical Medicine, 11(21), 6231. https://doi.org/10.3390/jcm11216231